
Autologous Matrix-Induced Chondrogenesis (AMIC) and Microfractures for Focal Chondral Defects of the Knee: A Medium-Term Comparative Study

 ,
, 
 ,
,  ,
, 
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design
2.2. Surgical Technique
2.3. Outcomes of Interest
2.4. Statistical Analysis
3. Results
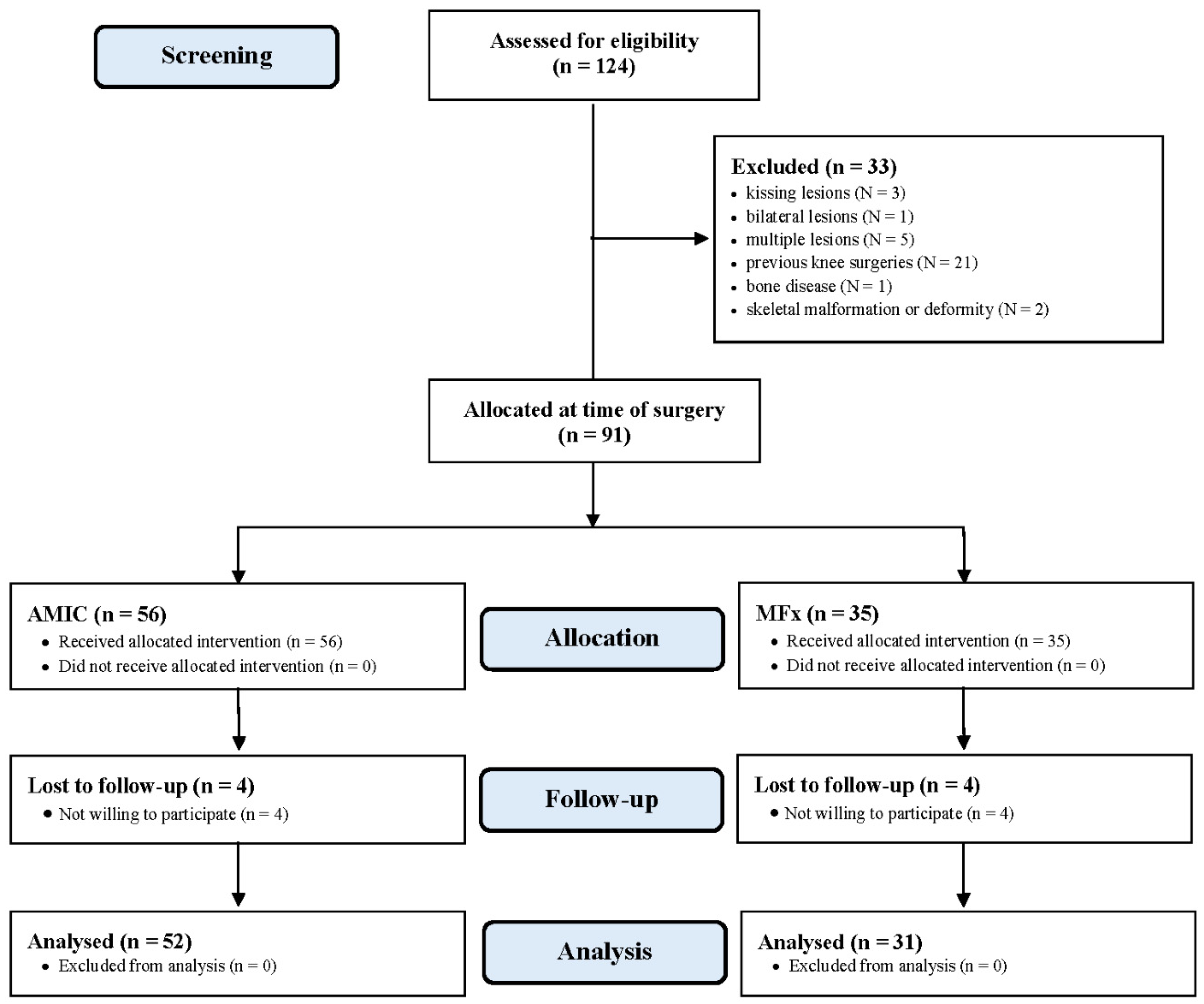
3.1. Recruitment Process
3.2. Patient Demographics
3.3. Outcomes of Interest
3.4. Complications
3.5. Subgroup Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Ethical Approval
References
- Curl, W.W.; Krome, J.; Gordon, E.; Rushing, J.; Smith, B.P.; Poehling, G.G. Cartilage injuries: A review of 31,516 knee arthroscopies. Arthrosc. J. Arthrosc. Relat. Surg. 1997, 13, 456–460. [Google Scholar] [CrossRef]
- Figueroa, D.; Calvo, R.; Vaisman, A.; Carrasco, M.A.; Moraga, C.; Delgado, I. Knee Chondral Lesions: Incidence and Correlation Between Arthroscopic and Magnetic Resonance Findings. Arthrosc. J. Arthrosc. Relat. Surg. 2007, 23, 312–315. [Google Scholar] [CrossRef] [PubMed]
- Heir, S.; Nerhus, T.K.; Røtterud, J.H.; Løken, S.; Ekeland, A.; Engebretsen, L.; Årøen, A. Focal Cartilage Defects in the Knee Impair Quality of Life as Much as Severe Osteoarthritis. Am. J. Sports Med. 2010, 38, 231–237. [Google Scholar] [CrossRef] [Green Version]
- Götze, C.; Nieder, C.; Felder, H.; Migliorini, F. AMIC for Focal Osteochondral Defect of the Talar Shoulder. Life 2020, 10, 328. [Google Scholar] [CrossRef]
- Kreuz, P.; Steinwachs, M.; Erggelet, C.; Krause, S.; Konrad, G.; Uhl, M.; Südkamp, N. Results after microfracture of full-thickness chondral defects in different compartments in the knee. Osteoarthr. Cartil. 2006, 14, 1119–1125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scillia, A.J.; Aune, K.T.; Andrachuk, J.S.; Cain, E.L.; Dugas, J.R.; Fleisig, G.S.; Andrews, J.R. Return to Play after Chondroplasty of the Knee in National Football League Athletes. Am. J. Sports Med. 2015, 43, 663–668. [Google Scholar] [CrossRef]
- Castrodad, I.M.D.; Mease, S.J.; Werheim, E.; McInerney, V.K.; Scillia, A.J. Arthroscopic Chondral Defect Repair with Extracellular Matrix Scaffold and Bone Marrow Aspirate Concentrate. Arthrosc. Tech. 2020, 9, e1241–e1247. [Google Scholar] [CrossRef] [PubMed]
- Atala, A.; Irvine, D.J.; Moses, M.A.; Shaunak, S. Wound Healing Versus Regeneration: Role of the Tissue Environment in Regenerative Medicine. MRS Bull. 2010, 35, 597–606. [Google Scholar] [CrossRef] [Green Version]
- Buckwalter, J.A. Articular Cartilage Injuries. Clin. Orthop. Relat. Res. 2002, 402, 21–37. [Google Scholar] [CrossRef] [PubMed]
- Filardo, G.; Kon, E.; Berruto, M.; Di Martino, A.; Patella, S.; Muccioli, G.M.M.; Zaffagnini, S.; Marcacci, M. Arthroscopic second generation autologous chondrocytes implantation associated with bone grafting for the treatment of knee osteochondritis dissecans: Results at 6years. Knee 2012, 19, 658–663. [Google Scholar] [CrossRef]
- Bertho, P.; Pauvert, A.; Pouderoux, T.; Robert, H. Treatment of large deep osteochondritis lesions of the knee by autologous matrix-induced chondrogenesis (AMIC): Preliminary results in 13 patients. Orthop. Traumatol. Surg. Res. 2018, 104, 695–700. [Google Scholar] [CrossRef] [PubMed]
- Gudas, R.; Kalesinskas, R.J.; Kimtys, V.; Stankevicius, E.; Toliusis, V.; Bernotavicius, G.; Smailys, A. A Prospective Randomized Clinical Study of Mosaic Osteochondral Autologous Transplantation Versus Microfracture for the Treatment of Osteochondral Defects in the Knee Joint in Young Athletes. Arthrosc. J. Arthrosc. Relat. Surg. 2005, 21, 1066–1075. [Google Scholar] [CrossRef]
- Richter, D.L.; Schenck, J.R.C.; Wascher, D.C.; Treme, G. Knee Articular Cartilage Repair and Restoration Techniques. Sports Health A Multidiscip. Approach 2016, 8, 153–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, G.D.; Knutsen, G.; Richardson, J.B. A clinical review of cartilage repair techniques. J. Bone Jt. Surg. Br. Vol. 2005, 87, 445–449. [Google Scholar] [CrossRef]
- Steinwachs, M.; Guggi, T.; Kreuz, P. Marrow stimulation techniques. Injury 2008, 39 (Suppl. 1), S26–S31. [Google Scholar] [CrossRef] [PubMed]
- Hoburg, A.; Löer, I.; Körsmeier, K.; Siebold, R.; Niemeyer, P.; Fickert, S.; Ruhnau, K. Matrix-Associated Autologous Chondrocyte Implantation Is an Effective Treatment at Midterm Follow-up in Adolescents and Young Adults. Orthop. J. Sports Med. 2019, 7. [Google Scholar] [CrossRef] [Green Version]
- Migliorini, F.; Berton, A.; Salvatore, G.; Candela, V.; Khan, W.; Longo, U.G.; Denaro, V. Autologous Chondrocyte Implantation and Mesenchymal Stem Cells for the Treatments of Chondral Defects of the Knee- A Systematic Review. Curr. Stem Cell Res. Ther. 2020, 15, 547–556. [Google Scholar] [CrossRef]
- Baltzer, A.; Ostapczuk, M.; Terheiden, H.; Merk, H. Good short- to medium-term results after osteochondral autograft transplantation (OAT) in middle-aged patients with focal, non-traumatic osteochondral lesions of the knee. Orthop. Traumatol. Surg. Res. 2016, 102, 879–884. [Google Scholar] [CrossRef] [PubMed]
- Shimozono, Y.; Hurley, E.T.; Nguyen, J.T.; Deyer, T.W.; Kennedy, J.G. Allograft Compared with Autograft in Osteochondral Transplantation for the Treatment of Osteochondral Lesions of the Talus. J. Bone Jt. Surg. Am. Vol. 2018, 100, 1838–1844. [Google Scholar] [CrossRef]
- Siebold, R.; Suezer, F.; Schmitt, B.; Trattnig, S.; Essig, M. Good clinical and MRI outcome after arthroscopic autologous chondrocyte implantation for cartilage repair in the knee. Knee Surg. Sports Traumatol. Arthrosc. 2017, 26, 831–839. [Google Scholar] [CrossRef]
- Niemeyer, P.; Laute, V.; Zinser, W.; Becher, C.; Kolombe, T.; Fay, J.; Pietsch, S.; Kuźma, T.; Widuchowski, W.; Fickert, S. A Prospective, Randomized, Open-Label, Multicenter, Phase III Noninferiority Trial to Compare the Clinical Efficacy of Matrix-Associated Autologous Chondrocyte Implantation with Spheroid Technology Versus Arthroscopic Microfracture for Cartilage Defects of the Knee. Orthop. J. Sports Med. 2019, 7. [Google Scholar] [CrossRef] [Green Version]
- Behrens, P. Matrixgekoppelte Mikrofrakturierung. Arthroskopie 2005, 18, 193–197. [Google Scholar] [CrossRef]
- De Girolamo, L.; Schönhuber, H.; Viganò, M.; Bait, C.; Quaglia, A.; Thiebat, G.; Volpi, P. Autologous Matrix-Induced Chondrogenesis (AMIC) and AMIC Enhanced by Autologous Concentrated Bone Marrow Aspirate (BMAC) Allow for Stable Clinical and Functional Improvements at up to 9 Years Follow-Up: Results from a Randomized Controlled Study. J. Clin. Med. 2019, 8, 392. [Google Scholar] [CrossRef] [Green Version]
- Panni, A.S.; Del Regno, C.; Mazzitelli, G.; D’Apolito, R.; Corona, K.; Vasso, M. Good clinical results with autologous matrix-induced chondrogenesis (Amic) technique in large knee chondral defects. Knee Surg. Sports Traumatol. Arthrosc. 2017, 26, 1–7. [Google Scholar] [CrossRef]
- Schagemann, J.; Behrens, P.; Paech, A.; Riepenhof, H.; Kienast, B.; Mittelstädt, H.; Gille, J. Mid-term outcome of arthroscopic AMIC for the treatment of articular cartilage defects in the knee joint is equivalent to mini-open procedures. Arch. Orthop. Trauma Surg. 2018, 138, 819–825. [Google Scholar] [CrossRef] [PubMed]
- Bark, S.; Piontek, T.; Behrens, P.; Mkalaluh, S.; Varoga, D.; Gille, J. Enhanced microfracture techniques in cartilage knee surgery: Fact or fiction? World J. Orthop. 2014, 5, 444–449. [Google Scholar] [CrossRef]
- Volz, M.; Schaumburger, J.; Frick, H.; Grifka, J.; Anders, S. A randomized controlled trial demonstrating sustained benefit of Autologous Matrix-Induced Chondrogenesis over microfracture at five years. Int. Orthop. 2017, 41, 797–804. [Google Scholar] [CrossRef] [Green Version]
- Anders, S.; Volz, M.; Frick, H.; Gellissen, J. A Randomized, Controlled Trial Comparing Autologous Matrix-Induced Chondrogenesis (AMIC®) to Microfracture: Analysis of 1- and 2-Year Follow-Up Data of 2 Centers. Open Orthop. J. 2013, 7, 133–143. [Google Scholar] [CrossRef] [Green Version]
- Chung, J.Y.; Lee, D.-H.; Kim, T.H.; Kwack, K.-S.; Yoon, K.H.; Min, B.-H. Cartilage extra-cellular matrix biomembrane for the enhancement of microfractured defects. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 1249–1259. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersson, I.F.; Boegård, T.; Saxne, T.; Silman, A.J.; Svensson, B. Radiographic osteoarthritis of the knee classified by the Ahlback and Kellgren & Lawrence systems for the tibiofemoral joint in people aged 35–54 years with chronic knee pain. Ann. Rheum. Dis. 1997, 56, 493–496. [Google Scholar] [CrossRef] [Green Version]
- Benthien, J.P.; Behrens, P. The treatment of chondral and osteochondral defects of the knee with autologous matrix-induced chondrogenesis (AMIC): Method description and recent developments. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 1316–1319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, E.A.; Verner, A.; Flannery, C.R.; Archer, C.W. Cellular responses of embryonic hyaline cartilage to experimental woundingin vitro. J. Orthop. Res. 2000, 18, 25–34. [Google Scholar] [CrossRef]
- Hunziker, E.B.; Quinn, T.M. Surgical removal of articular cartilage leads to loss of chondrocytes from cartilage bordering the wound edge. J. Bone Jt. Surg. Am. Vol. 2003, 85 (Suppl. 2), 85–92. [Google Scholar] [CrossRef] [PubMed]
- Hunziker, E.B.; Stähli, A. Surgical suturing of articular cartilage induces osteoarthritis-like changes. Osteoarthr. Cartil. 2008, 16, 1067–1073. [Google Scholar] [CrossRef] [Green Version]
- Enea, D.; Cecconi, S.; Calcagno, S.; Busilacchi, A.; Manzotti, S.; Kaps, C.; Gigante, A. Single-stage cartilage repair in the knee with microfracture covered with a resorbable polymer-based matrix and autologous bone marrow concentrate. Knee 2013, 20, 562–569. [Google Scholar] [CrossRef]
- Pipino, G.; Risitano, S.; Alviano, F.; Wu, E.J.; Bonsi, L.; Vaccarisi, D.C.; Indelli, P.F. Microfractures and hydrogel scaffolds in the treatment of osteochondral knee defects: A clinical and histological evaluation. J. Clin. Orthop. Trauma 2019, 10, 67–75. [Google Scholar] [CrossRef]
- Kwan, H.; Chisari, E.; Khan, W.S. Cell-Free Scaffolds as a Monotherapy for Focal Chondral Knee Defects. Materials 2020, 13, 306. [Google Scholar] [CrossRef] [Green Version]
- Bekkers, J.; Tsuchida, A.; Malda, J.; Creemers, L.; Castelein, R.; Saris, D.; Dhert, W. Quality of scaffold fixation in a human cadaver knee model. Osteoarthr. Cartil. 2010, 18, 266–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, S.S.; Lee, S.; Mithoefer, K. Next-Generation Marrow Stimulation Technology for Cartilage Repair. JBJS Rev. 2021, 9, e20.00090. [Google Scholar] [CrossRef]
- Eglin, D.; Grad, S.; Gogolewski, S.; Alini, M. Farsenol-modified biodegradable polyurethanes for cartilage tissue engineering. J. Biomed. Mater. Res. Part A 2010, 92, 393–408. [Google Scholar] [CrossRef] [PubMed]
- Grad, S.; Kupcsik, L.; Gorna, K.; Gogolewski, S.; Alini, M. The use of biodegradable polyurethane scaffolds for cartilage tissue engineering: Potential and limitations. Biomaterials 2003, 24, 5163–5171. [Google Scholar] [CrossRef]
- Khan, S.N.; Cammisa, F.P.; Sandhu, H.S.; Diwan, A.D.; Girardi, F.P.; Lane, J.M. The Biology of Bone Grafting. J. Am. Acad. Orthop. Surg. 2005, 13, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Sen, M.; Miclau, T. Autologous iliac crest bone graft: Should it still be the gold standard for treating nonunions? Injury 2007, 38 (Suppl. 1), S75–S80. [Google Scholar] [CrossRef] [PubMed]
- ASTM International: West Conshohocken, PA, USA, 2018. Available online: www.astm.org (accessed on 22 October 2020).
- Blackman, A.J.; Smith, M.V.; Flanigan, D.C.; Matava, M.J.; Wright, R.W.; Brophy, R.H. Correlation Between Magnetic Resonance Imaging and Clinical Outcomes After Cartilage Repair Surgery in the Knee. Am. J. Sports Med. 2013, 41, 1426–1434. [Google Scholar] [CrossRef] [PubMed]
- Shive, M.S.; Stanish, W.D.; McCormack, R.; Forriol, F.; Mohtadi, N.; Pelet, S.; Desnoyers, J.; Méthot, S.; Vehik, K.; Restrepo, A. BST-CarGel® Treatment Maintains Cartilage Repair Superiority over Microfracture at 5 Years in a Multicenter Randomized Controlled Trial. Cartilage 2014, 6, 62–72. [Google Scholar] [CrossRef]
- Kaiser, N.; Jakob, R.P.; Pagenstert, G.; Tannast, M.; Petek, D. Stable clinical long term results after AMIC in the aligned knee. Arch. Orthop. Trauma Surg. 2020, 1–10. [Google Scholar] [CrossRef]
- Harris, J.D.; Siston, R.A.; Pan, X.; Flanigan, D.C. Autologous Chondrocyte Implantation. J. Bone Jt. Surg. Am. Vol. 2010, 92, 2220–2233. [Google Scholar] [CrossRef]
- Gille, J.; Behrens, P.; Volpi, P.; De Girolamo, L.; Reiss, E.; Zoch, W.; Anders, S. Outcome of Autologous Matrix Induced Chondrogenesis (AMIC) in cartilage knee surgery: Data of the AMIC Registry. Arch. Orthop. Trauma Surg. 2012, 133, 87–93. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Endpoint | AMIC (n = 52) | MFx (n = 31) | p |
|---|---|---|---|
| Follow-up (months) | 43.7 ± 27.6 | 39.5 ± 19.1 | n.s. |
| Age | 29.5 ± 12.1 | 31.3 ± 9.9 | n.s. |
| Gender (female) | 34.6% | 32.3% | n.s. |
| Side (right leg) | 55.8% | 54.8% | n.s. |
| Side (knee compartment) | |||
| Lateral | 35% | 42% | n.s. |
| Medial | 65% | 58% | n.s. |
| Spongiosa transplantation | 32.7% | - | |
| Membrane | |||
| Cartimaix | 23% | ||
| Chondro-Gide | 77% | ||
| Symptom duration (months) | 48.1 ± 80.7 | 35.3 ± 66.8 | n.s. |
| Length of hospital stay (days) | 4.5 ± 1.6 | 3.1 ± 0.9 | 0.03 |
| Area of defect (cm2) | 2.8 ± 2.5 | 2.6 ± 1.8 | n.s. |
| BMI (kg/m2) | 27.1 ± 4.4 | 26.5 ± 3.9 | n.s. |
| Compartment | |||
| Lateral compartment | 34.6% | 29.0% | n.s. |
| Medial compartment | 65.4% | 71.0%% | n.s. |
| Endpoint | AMIC (n = 52) | MFx (n = 31) | 95% CI | MD | p |
|---|---|---|---|---|---|
| IKCD | 75.9 ± 24.6 | 63.3 ± 6.3 | 3.619, 1.581 | 12.6 | 0.007 |
| Lysholm | 71.2 ± 24.3 | 59.9 ± 12.5 | 1.942, 20.658 | 11.3 | 0.02 |
| MOCART | 70.0 ± 19.4 | 68.4 ± 14.3 | −6.384, 9.584 | 1.6 | 0.7 |
| VAS (0–10) | 2.5 ± 2.1 | 4.1 ± 3.3 | 0.422, 2.778 | 1.6 | 0.008 |
| Tegner | 4.8 ± 1.5 | 3.1 ± 0.9 | 1.108, 2.292 | 1.7 | <0.0001 |
| Endpoint | AMIC (n = 52) | MFx (n = 31) | 95% CI | OR | p |
|---|---|---|---|---|---|
| Failure | 3.8% | 29.0% | 0.0195, 0.4902 | 0.098 | 0.005 |
| Knee arthroplasty | 0 | 6.5% | 0.0054, 2.5005 | 0.116 | 0.2 |
| Revision surgery | 1.9% | 19.4% | 0.0093, 0.7159 | 0.082 | 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Migliorini, F.; Eschweiler, J.; Maffulli, N.; Schenker, H.; Baroncini, A.; Tingart, M.; Rath, B. Autologous Matrix-Induced Chondrogenesis (AMIC) and Microfractures for Focal Chondral Defects of the Knee: A Medium-Term Comparative Study. Life 2021, 11, 183. https://doi.org/10.3390/life11030183
Migliorini F, Eschweiler J, Maffulli N, Schenker H, Baroncini A, Tingart M, Rath B. Autologous Matrix-Induced Chondrogenesis (AMIC) and Microfractures for Focal Chondral Defects of the Knee: A Medium-Term Comparative Study. Life. 2021; 11(3):183. https://doi.org/10.3390/life11030183
Chicago/Turabian StyleMigliorini, Filippo, Jörg Eschweiler, Nicola Maffulli, Hanno Schenker, Alice Baroncini, Markus Tingart, and Björn Rath. 2021. "Autologous Matrix-Induced Chondrogenesis (AMIC) and Microfractures for Focal Chondral Defects of the Knee: A Medium-Term Comparative Study" Life 11, no. 3: 183. https://doi.org/10.3390/life11030183
APA StyleMigliorini, F., Eschweiler, J., Maffulli, N., Schenker, H., Baroncini, A., Tingart, M., & Rath, B. (2021). Autologous Matrix-Induced Chondrogenesis (AMIC) and Microfractures for Focal Chondral Defects of the Knee: A Medium-Term Comparative Study. Life, 11(3), 183. https://doi.org/10.3390/life11030183