

Two-Year Follow-Up on Chemosensory Dysfunction and Adaptive Immune Response after Infection with SARS-CoV-2 in a Cohort of 44 Healthcare Workers


 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
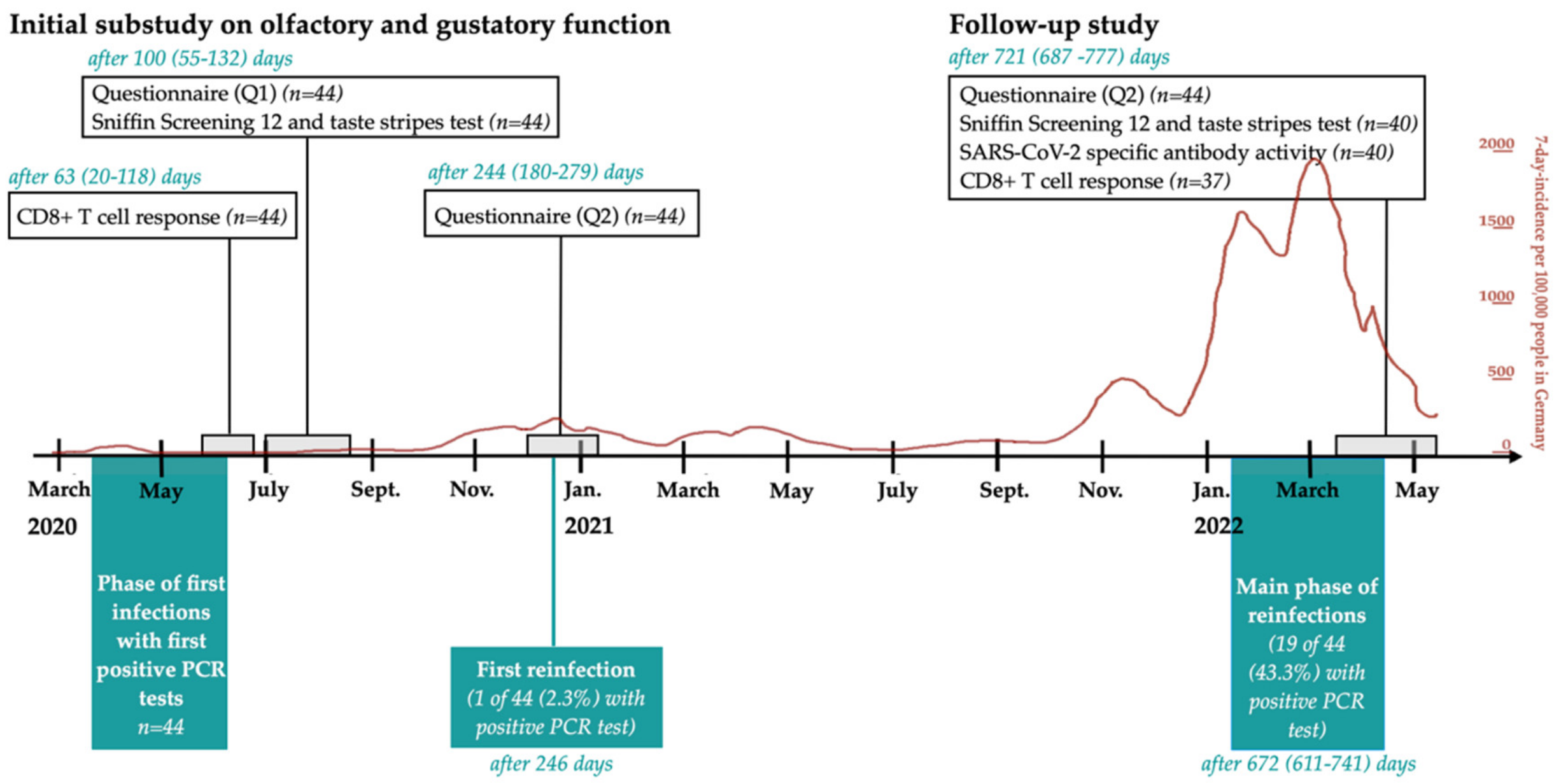
2.2. Study Design
2.3. Questionnaires Q1 and Q2
2.4. Questionnaire Concerning Vaccination, Reinfections with COVID-19, and Quality of Life
2.5. Sniffin’ Sticks Screening 12 Test with Taste Stripes
2.6. Evaluation of SARS-CoV-2 Specific Antibody Levels
2.7. T-Cell Analysis
2.8. Statistical Analysis
3. Results
3.1. Cohort Characteristics
3.2. Self-Reported Chemosensory Dysfunction
3.2.1. Chemosensory Dysfunction over the Course of the Study
3.2.2. Self-Reported Olfactory and Gustatory Dysfunction during Reinfections
3.2.3. Quality of Life and Taste and Smell after 721 Days
3.3. Psychophysical Screening Tests after a Median of 721 and 100 Days
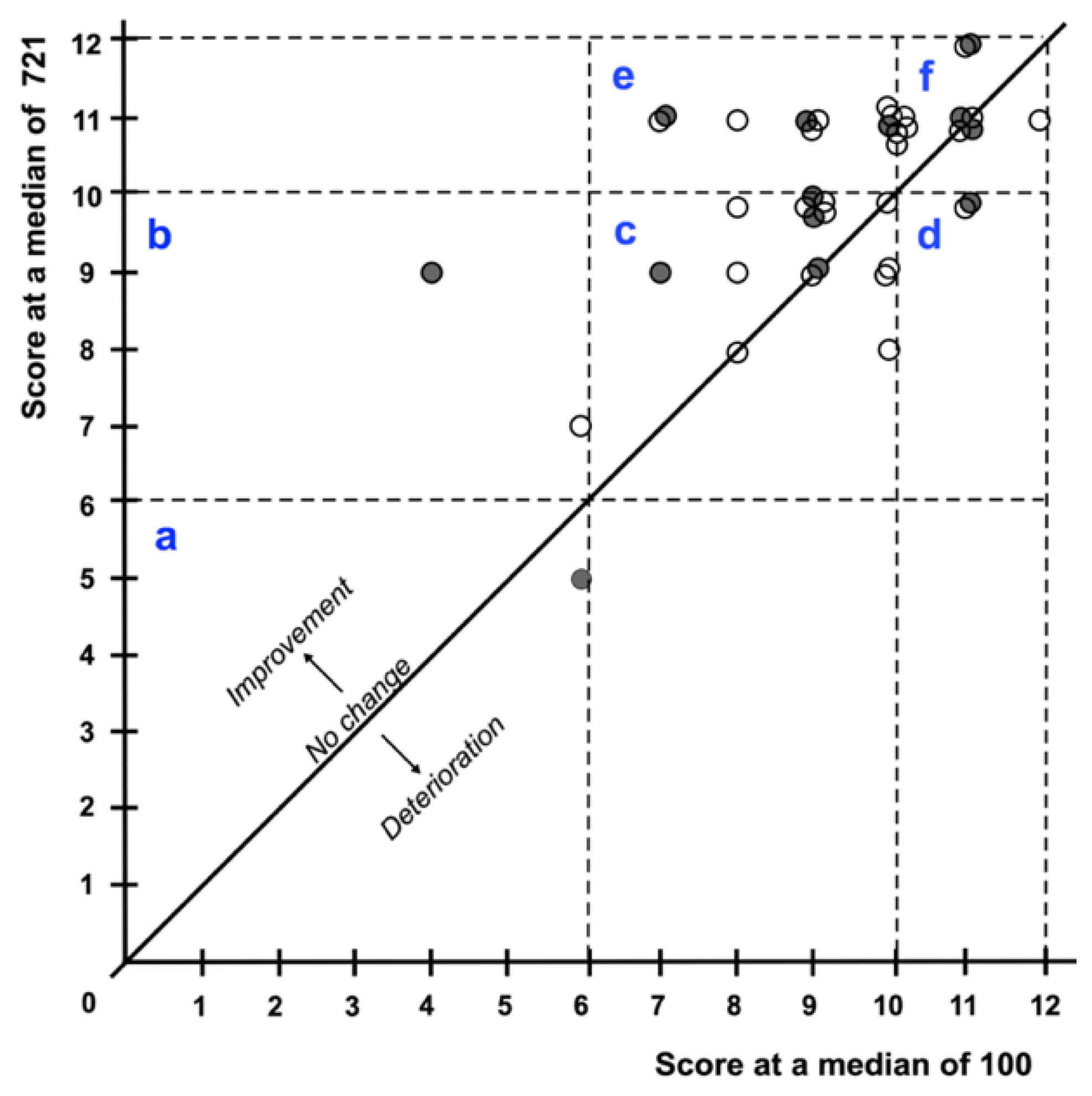
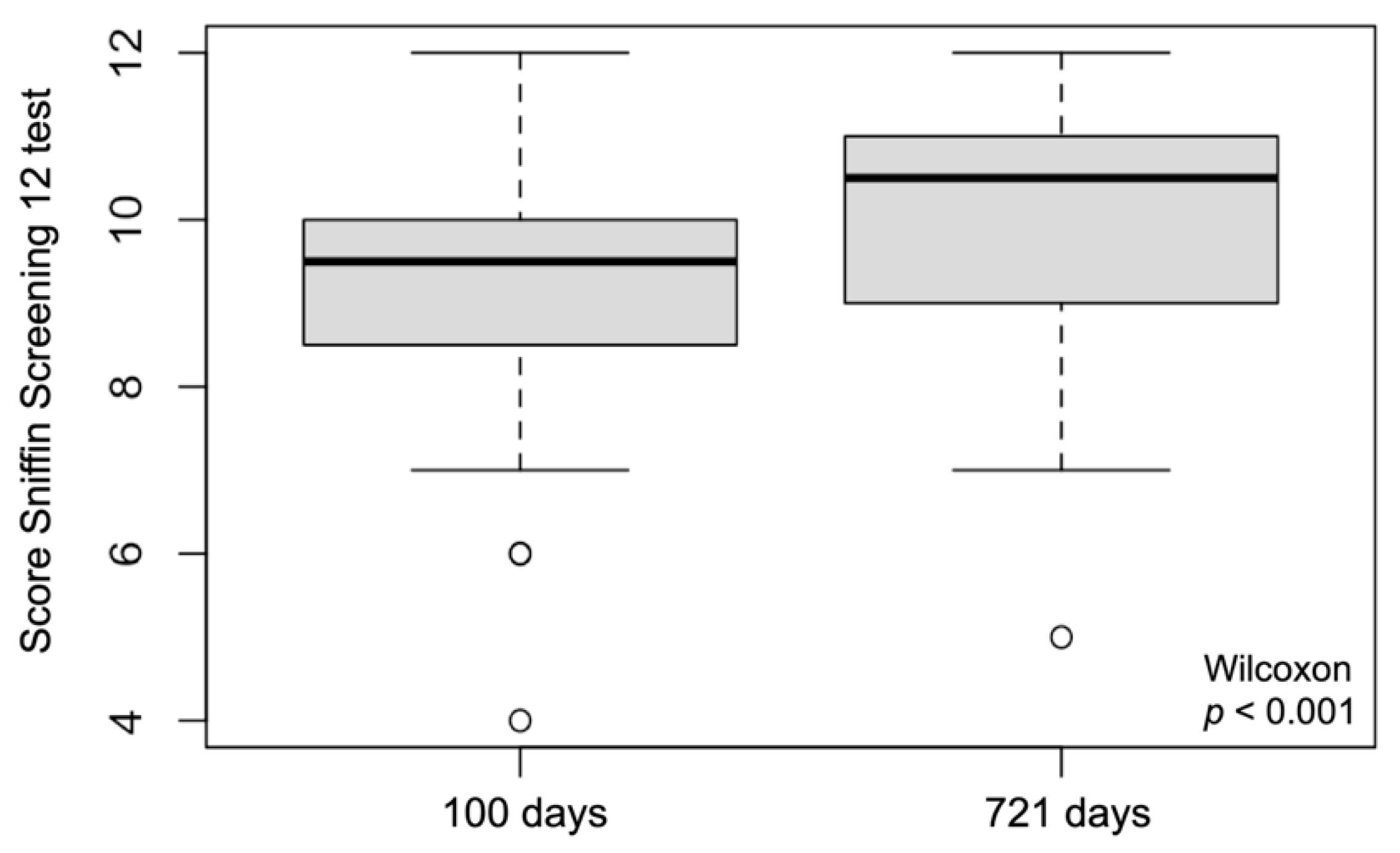
3.3.1. Sniffin’ Screening 12 Test
3.3.2. Taste Stripes Test after 100 and 721 Days
3.4. Comparisons of Self-Report and Psychophysical Screening Tests after 721 Days
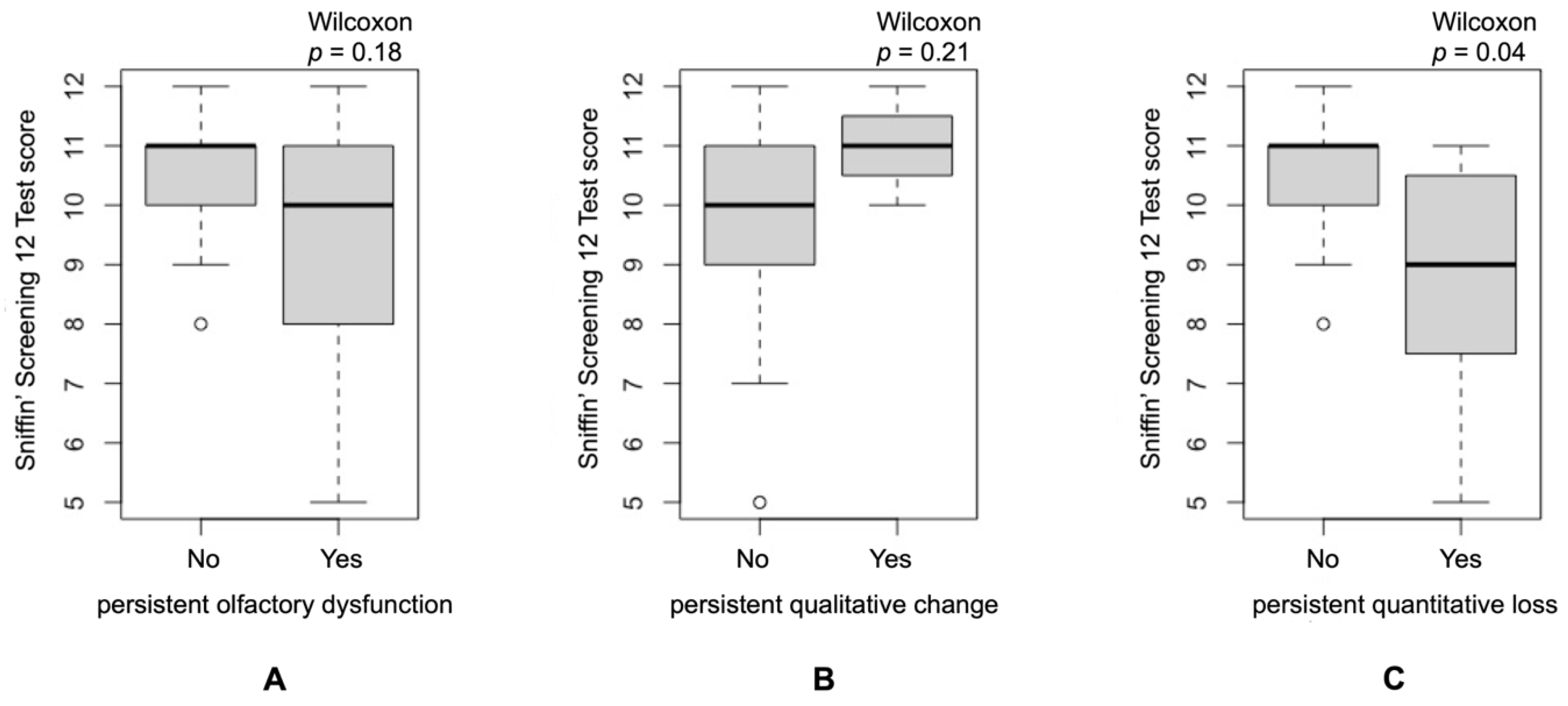
3.4.1. Sniffin’ Screening 12 Test Score and Self-Reported Changes in Olfactory Function
3.4.2. Taste Stripes and Self-Reported Changes in Gustatory Function
3.5. Self-Reported Hyperosmia after 721 Days
3.6. Immune Response and Correlation with Chemosensory Dysfunction
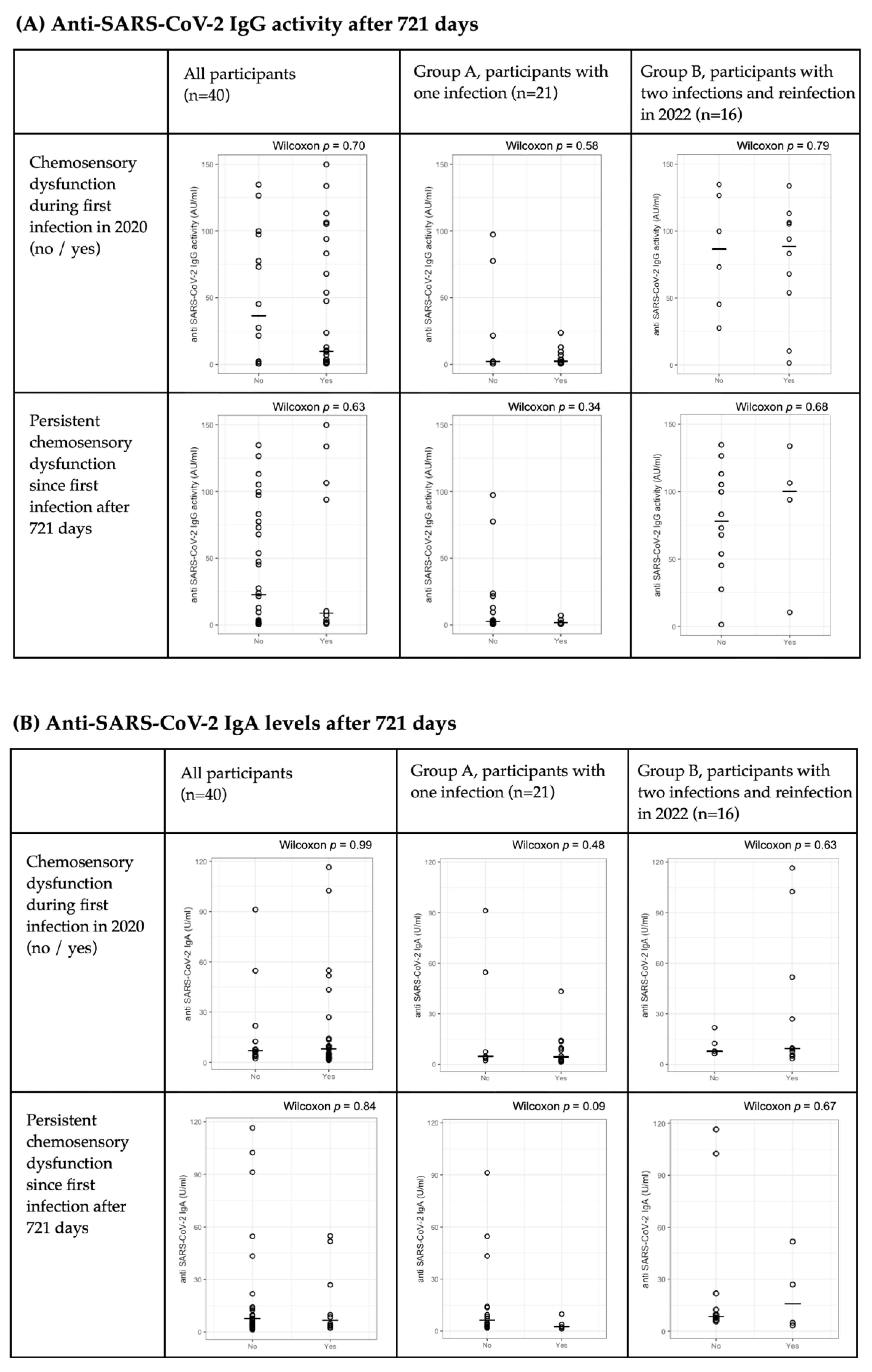
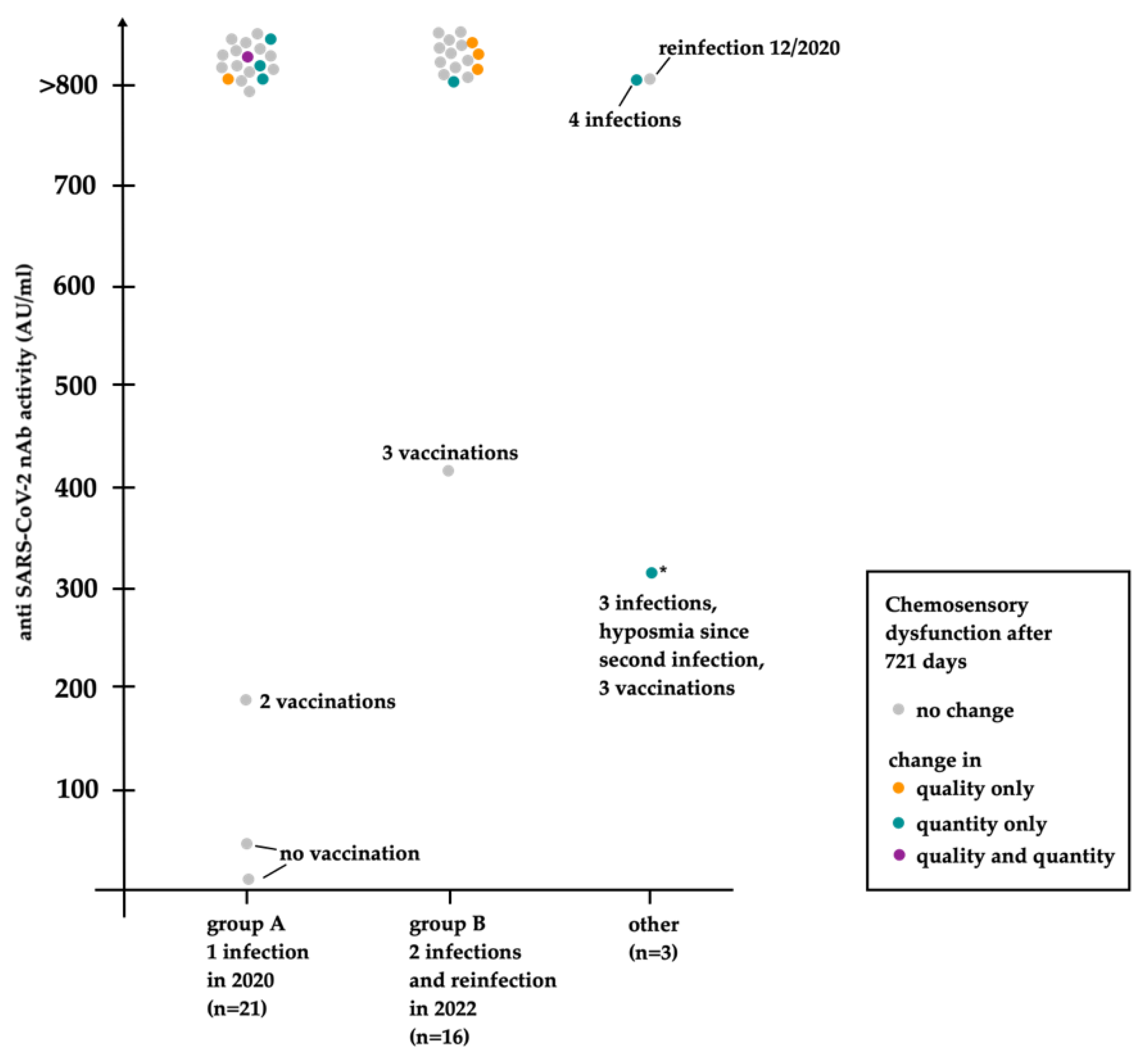
3.6.1. SARS-CoV-2 Specific Antibody Levels after 721 Days
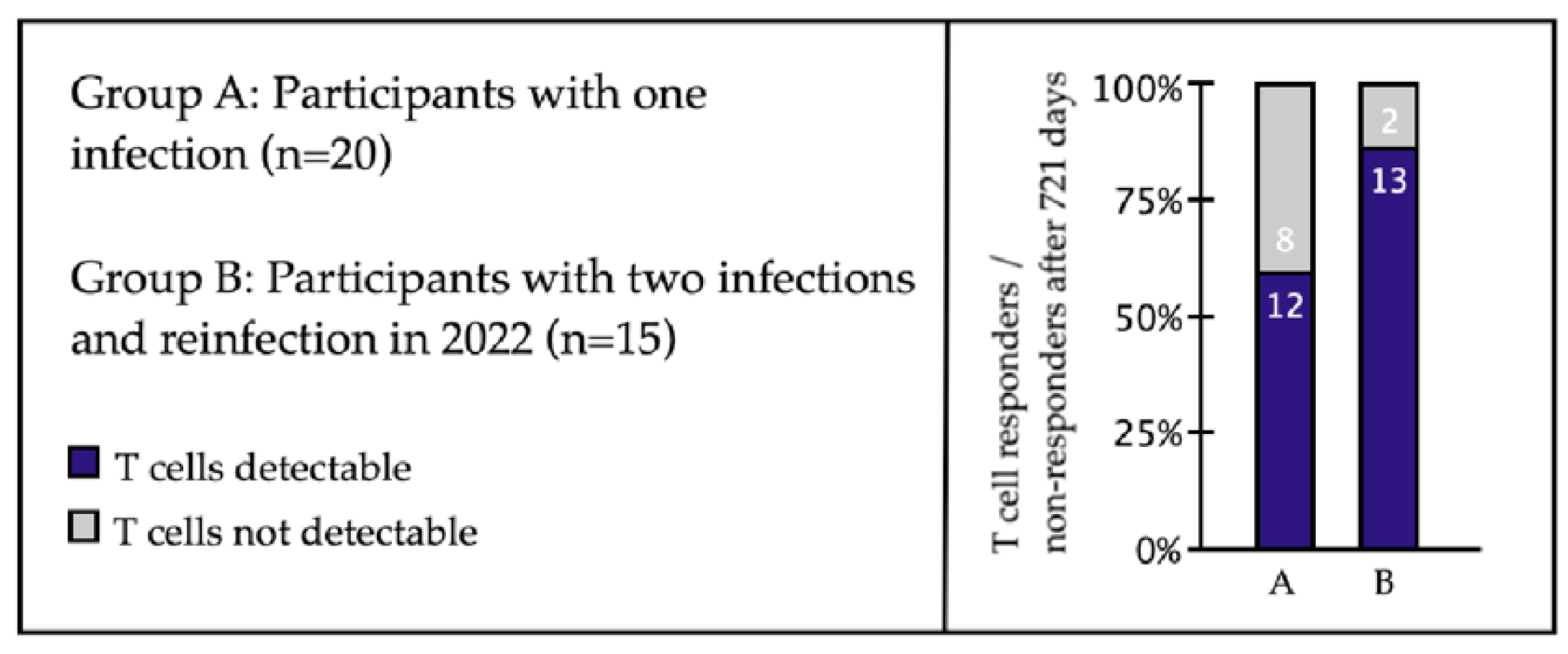
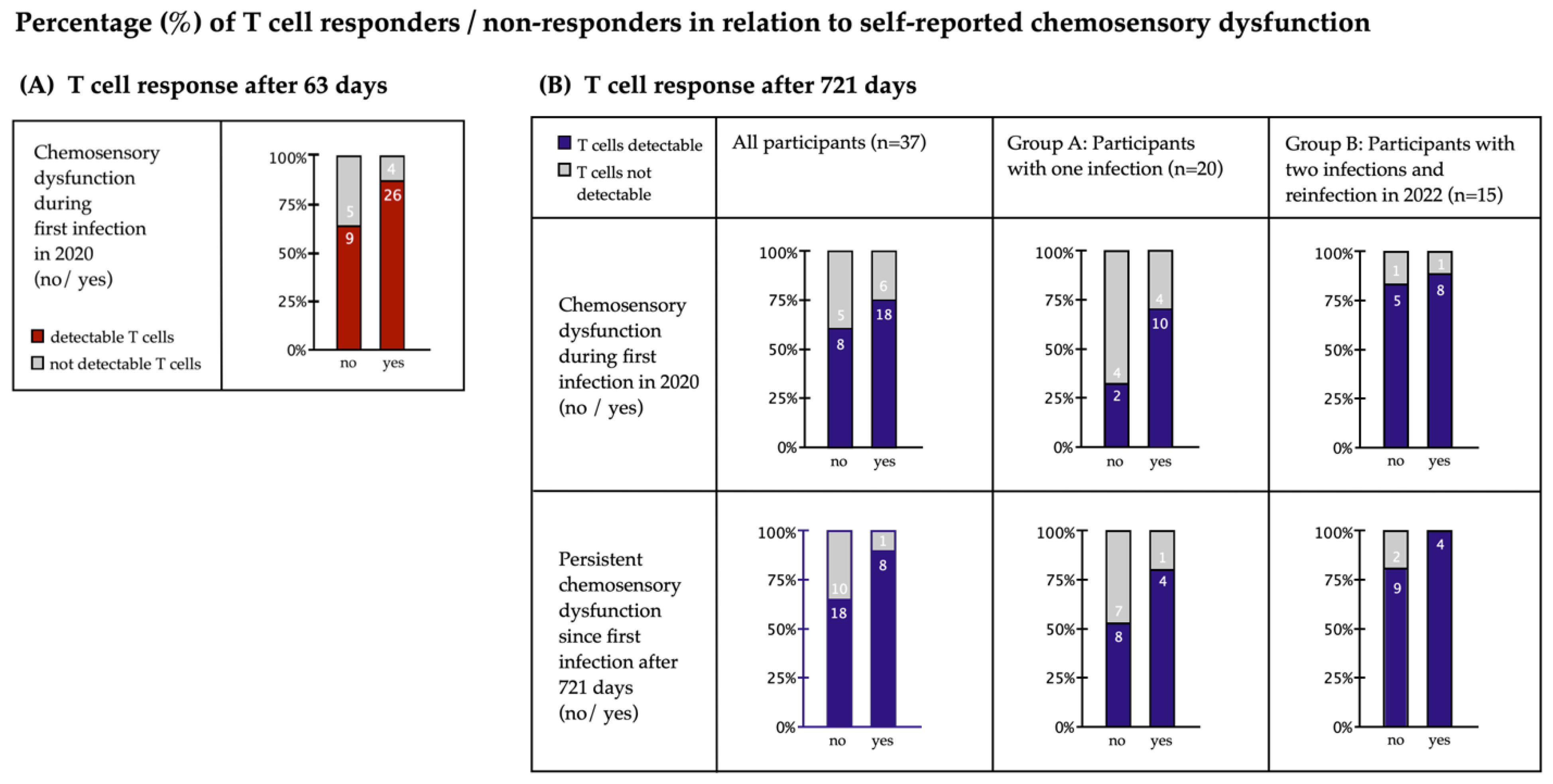
3.6.2. SARS-CoV-2-Specific CD8+ T-Cell Response in Relation to Chemosensory Dysfunctions
4. Discussion
5. Limitations and Strengths
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Description | During COVID-19 | 100 Days | 244 Days | 721 Days |
|---|---|---|---|---|
| Asymptomatic | 14 | 33 | 30 | 32 |
| Alteration of taste or smell | 30 | 11 | 14 | 12 * |
| Quantity only | 14 | 1 | 1 | 7 * |
| Taste only | 1 | 1 | 0 | 0 |
| Ageusia (ag.) | 1 | 0 | 0 | 0 |
| Hypogeusia (hg.) | 0 | 1 | 0 | 0 |
| Smell only | 0 | 0 | 0 | 2 * |
| Taste and smell | 13 | 0 | 1 | 5 |
| Ag. and anosmia (an.) | 13 | 0 | 0 | 0 |
| Hg. and hyposmia (Ho.) | 0 | 0 | 1 | 5 |
| Quality only (total) | 6 | 7 | 10 | 4 |
| Taste only–Dysgeusia (dy.) | 5 | 2 | 2 | 1 |
| Smell only | 0 | 4 | 3 | 1 |
| Parosmia (pa.) | 0 | 2 | 1 | 0 |
| Phantosmia (ph.) | 0 | 1 | 2 | 1 |
| Pa. and ph. | 0 | 1 | 0 | 0 |
| Taste and smell | 1 | 1 | 5 | 2 |
| Dy., pa. and ph. | 1 | 1 | 2 | 0 |
| Dy. and pa. | 0 | 0 | 2 | 1 |
| Dy. and ph. | 0 | 0 | 1 | 0 |
| Dy. and Hyperosmia | 0 | 0 | 0 | 1 |
| Quality and quantity (total) | 10 | 3 | 3 | 1 |
| Taste only | 0 | 0 | 0 | 0 |
| Smell only-pa. and ho. | 0 | 1 | 1 | 1 |
| Taste and smell | 10 | 2 | 2 | 0 |
| Dy. and an. | 3 | 0 | 0 | 0 |
| Dy., pa. and ph. | 1 | 0 | 0 | 0 |
| Dy., an., pa. and ph. | 1 | 0 | 0 | 0 |
| Ag., an. and pa. | 1 | 0 | 0 | 0 |
| Ag., an. and ph. | 1 | 0 | 0 | 0 |
| Ag., an., pa. and ph. | 3 | 0 | 0 | 0 |
| Dy., hg. and ho. | 0 | 1 | 1 | 0 |
| Dy., ho., pa. and ph. | 0 | 1 | 0 | 0 |
| Dy. and ho. | 0 | 0 | 1 | 0 |
References
- Dawson, P.; Rabold, E.M.; Laws, R.L.; Conners, E.E.; Gharpure, R.; Yin, S.; Buono, S.A.; Dasu, T.; Bhattacharyya, S.; Westergaard, R.P.; et al. Loss of Taste and Smell as Distinguishing Symptoms of Coronavirus Disease 2019. Clin. Infect. Dis. 2020, 72, 682–685. [Google Scholar] [CrossRef]
- Chua, A.J.; Charn, T.C.; Chan, E.C.; Loh, J. Acute Olfactory Loss Is Specific for COVID-19 at the Emergency Department. Ann. Emerg. Med. 2020, 76, 550–551. [Google Scholar] [CrossRef]
- Gerkin, R.C.; Ohla, K.; Veldhuizen, M.G.; Joseph, P.V.; Kelly, C.E.; Bakke, A.J.; Steele, K.E.; Farruggia, M.C.; Pellegrino, R.; Pepino, M.Y.; et al. The best COVID-19 predictor is recent smell loss: A cross-sectional study. medRxiv 2020. [Google Scholar] [CrossRef]
- Wong, D.K.C.; Gendeh, H.S.; Thong, H.K.; Lum, S.G.; Gendeh, B.S.; Saim, A.; Salina, H. A review of smell and taste dysfunction in COVID-19 patients. Med. J. Malays. 2020, 75, 574–581. [Google Scholar]
- Boscolo-Rizzo, P.; Tirelli, G.; Meloni, P.; Hopkins, C.; Madeddu, G.; De Vito, A.; Gardenal, N.; Valentinotti, R.; Tofanelli, M.; Borsetto, D.; et al. Coronavirus disease 2019 (COVID-19)-related smell and taste impairment with widespread diffusion of severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2) Omicron variant. Int. Forum Allergy Rhinol. 2022, 12, 1273–1281. [Google Scholar] [CrossRef]
- Coelho, D.H.; Reiter, E.R.; French, E.; Costanzo, R.M. Decreasing Incidence of Chemosensory Changes by COVID-19 Variant. Otolaryngol. Head Neck Surg. 2022, 1945998221097656. [Google Scholar] [CrossRef] [PubMed]
- Santos, R.E.A.; da Silva, M.G.; do Monte Silva, M.C.B.; Barbosa, D.A.M.; Gomes, A.; Galindo, L.C.M.; da Silva Aragao, R.; Ferraz-Pereira, K.N. Onset and duration of symptoms of loss of smell/taste in patients with COVID-19: A systematic review. Am. J. Otolaryngol. 2021, 42, 102889. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, C.; Surda, P.; Vaira, L.A.; Lechien, J.R.; Safarian, M.; Saussez, S.; Kumar, N. Six month follow-up of self-reported loss of smell during the COVID-19 pandemic. Rhinology 2021, 59, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Prem, B.; Liu, D.T.; Besser, G.; Sharma, G.; Dultinger, L.E.; Hofer, S.V.; Matiasczyk, M.M.; Renner, B.; Mueller, C.A. Long-lasting olfactory dysfunction in COVID-19 patients. Eur. Arch. Otorhinolaryngol. 2022, 279, 3485–3492. [Google Scholar] [CrossRef]
- Ohla, K.; Veldhuizen, M.G.; Green, T.; Hannum, M.E.; Bakke, A.J.; Moein, S.T.; Tognetti, A.; Postma, E.M.; Pellegrino, R.; Hwang, D.L.D.; et al. A follow-up on quantitative and qualitative olfactory dysfunction and other symptoms in patients recovering from COVID-19 smell loss. Rhinology 2022. [Google Scholar] [CrossRef]
- Schambeck, S.E.; Crowell, C.S.; Wagner, K.I.; D’Ippolito, E.; Burrell, T.; Mijocevic, H.; Protzer, U.; Busch, D.H.; Gerhard, M.; Poppert, H.; et al. Phantosmia, Parosmia, and Dysgeusia Are Prolonged and Late-Onset Symptoms of COVID-19. J. Clin. Med. 2021, 10, 5266. [Google Scholar] [CrossRef] [PubMed]
- Vaira, L.A.; Gessa, C.; Deiana, G.; Salzano, G.; Maglitto, F.; Lechien, J.R.; Saussez, S.; Piombino, P.; Biglio, A.; Biglioli, F.; et al. The Effects of Persistent Olfactory and Gustatory Dysfunctions on Quality of Life in Long-COVID-19 Patients. Life 2022, 12, 141. [Google Scholar] [CrossRef] [PubMed]
- Boscolo-Rizzo, P.; Fabbris, C.; Polesel, J.; Emanuelli, E.; Tirelli, G.; Spinato, G.; Hopkins, C. Two-Year Prevalence and Recovery Rate of Altered Sense of Smell or Taste in Patients With Mildly Symptomatic COVID-19. JAMA Otolaryngol. Head Neck Surg. 2022, 148, 889–891. [Google Scholar] [CrossRef]
- Burges Watson, D.L.; Campbell, M.; Hopkins, C.; Smith, B.; Kelly, C.; Deary, V. Altered smell and taste: Anosmia, parosmia and the impact of long COVID-19. PLoS ONE 2021, 16, e0256998. [Google Scholar] [CrossRef] [PubMed]
- Croy, I.; Nordin, S.; Hummel, T. Olfactory disorders and quality of life--an updated review. Chem. Senses 2014, 39, 185–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frasnelli, J.; Hummel, T. Olfactory dysfunction and daily life. Eur. Arch. Otorhinolaryngol. 2005, 262, 231–235. [Google Scholar] [CrossRef]
- Veronese, S.; Sbarbati, A. Chemosensory Systems in COVID-19: Evolution of Scientific Research. ACS Chem. Neurosci. 2021, 12, 813–824. [Google Scholar] [CrossRef]
- Xydakis, M.S.; Albers, M.W.; Holbrook, E.H.; Lyon, D.M.; Shih, R.Y.; Frasnelli, J.A.; Pagenstecher, A.; Kupke, A.; Enquist, L.W.; Perlman, S. Post-viral effects of COVID-19 in the olfactory system and their implications. Lancet Neurol. 2021, 20, 753–761. [Google Scholar] [CrossRef]
- Lechien, J.R.; Vaira, L.A.; Saussez, S. Prevalence and 24-month recovery of olfactory dysfunction in COVID-19 patients: A multicentre prospective study. J. Intern. Med. 2022. [Google Scholar] [CrossRef]
- Boscolo-Rizzo, P.; Tofanelli, M.; Zanelli, E.; Gardenal, N.; Tirelli, G. COVID-19-Related Quantitative and Qualitative Olfactory and Gustatory Dysfunction: Long-Term Prevalence and Recovery Rate. ORL J. Otorhinolaryngol. Relat. Spec. 2022, 1–5. [Google Scholar] [CrossRef]
- McWilliams, M.P.; Coelho, D.H.; Reiter, E.R.; Costanzo, R.M. Recovery from COVID-19 smell loss: Two-years of follow up. Am. J. Otolaryngol. 2022, 43, 103607. [Google Scholar] [CrossRef] [PubMed]
- Boscolo-Rizzo, P.; Hummel, T.; Hopkins, C.; Dibattista, M.; Menini, A.; Spinato, G.; Fabbris, C.; Emanuelli, E.; D’Alessandro, A.; Marzolino, R.; et al. High prevalence of long-term olfactory, gustatory, and chemesthesis dysfunction in post-COVID-19 patients: A matched case-control study with one-year follow-up using a comprehensive psychophysical evaluation. Rhinology 2021, 59, 517–527. [Google Scholar] [CrossRef] [PubMed]
- Hoang, M.P.; Staibano, P.; McHugh, T.; Sommer, D.D.; Snidvongs, K. Self-reported olfactory and gustatory dysfunction and psychophysical testing in screening for COVID-19: A systematic review and meta-analysis. Int. Forum Allergy Rhinol. 2022, 12, 744–756. [Google Scholar] [CrossRef]
- Wagner, K.I.; Mateyka, L.M.; Jarosch, S.; Grass, V.; Weber, S.; Schober, K.; Hammel, M.; Burrell, T.; Kalali, B.; Poppert, H.; et al. Recruitment of highly cytotoxic CD8(+) T cell receptors in mild SARS-CoV-2 infection. Cell Rep. 2022, 38, 110214. [Google Scholar] [CrossRef]
- Walliczek, U.; Negoias, S.; Hahner, A.; Hummel, T. Assessment of Chemosensory Function Using “Sniffin’ Sticks”, Taste Strips, Taste Sprays, and Retronasal Olfactory Tests. Curr. Pharm. Des. 2016, 22, 2245–2252. [Google Scholar] [CrossRef]
- Stuck, B.A.; Beule, A.; Damm, M.; Gudziol, H.; Huttenbrink, K.B.; Landis, B.N.; Renner, B.; Sommer, J.U.; Uecker, F.C.; Vent, J.; et al. Position paper “Chemosensory testing for expert opinion in smell disorders”. Laryngorhinootologie 2014, 93, 327–329. [Google Scholar] [CrossRef]
- Qian, C.; Zhou, M.; Cheng, F.; Lin, X.; Gong, Y.; Xie, X.; Li, P.; Li, Z.; Zhang, P.; Liu, Z.; et al. Development and multicenter performance evaluation of fully automated SARS-CoV-2 IgM and IgG immunoassays. Clin. Chem. Lab. Med. 2020, 58, 1601–1607. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Fortunato, F.; Martinelli, D.; Iannelli, G.; Milazzo, M.; Farina, U.; Di Matteo, G.; De Nittis, R.; Ascatigno, L.; Cassano, M.; Lopalco, P.L.; et al. Self-reported olfactory and gustatory dysfunctions in COVID-19 patients: A 1-year follow-up study in Foggia district, Italy. BMC Infect. Dis. 2022, 22, 77. [Google Scholar] [CrossRef]
- Lechien, J.R.; Journe, F.; Hans, S.; Chiesa-Estomba, C.M.; Mustin, V.; Beckers, E.; Vaira, L.A.; De Riu, G.; Hopkins, C.; Saussez, S. Severity of Anosmia as an Early Symptom of COVID-19 Infection May Predict Lasting Loss of Smell. Front. Med. 2020, 7, 582802. [Google Scholar] [CrossRef]
- Saussez, S.; Sharma, S.; Thiriard, A.; Olislagers, V.; Vu Duc, I.; Le Bon, S.D.; Khalife, M.; Hans, S.; De Riu, G.; Hopkins, C.; et al. Predictive factors of smell recovery in a clinical series of 288 coronavirus disease 2019 patients with olfactory dysfunction. Eur. J. Neurol. 2021, 28, 3702–3711. [Google Scholar] [CrossRef]
- Tan, B.K.J.; Han, R.; Zhao, J.J.; Tan, N.K.W.; Quah, E.S.H.; Tan, C.J.; Chan, Y.H.; Teo, N.W.Y.; Charn, T.C.; See, A.; et al. Prognosis and persistence of smell and taste dysfunction in patients with COVID-19: Meta-analysis with parametric cure modelling of recovery curves. BMJ 2022, 378, e069503. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, I.J.; Molinari, G.; Federici, G.; Silvestri, M.; De Corso, E.; Presutti, L.; Alicandri-Ciufelli, M.; Lucidi, D. Delayed recovery from severe acute respiratory syndrome coronavirus-2 related anosmia predicts incomplete olfactory restoration. J. Laryngol. Otol. 2022, 136, 237–242. [Google Scholar] [CrossRef]
- Almutairi, D.M.; Almalki, A.H.; Mirza, A.A.; Khalifah, M.J.; Aljefri, A.A.; Alsalmi, K.A.; Al-Thaqafy, M.S.; Algarni, M.A. Patterns of self-reported recovery from chemosensory dysfunction following SARS-CoV-2 infection: Insights after 1 year of the pandemic. Acta Otolaryngol. 2022, 142, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Amadu, A.M.; Vaira, L.A.; Lechien, J.R.; Scaglione, M.; Saba, L.; Lampus, M.L.; Profili, S.G.; Le Bon, S.D.; Salzano, G.; Maglitto, F.; et al. Analysis of the correlations between the severity of lung involvement and olfactory psychophysical scores in coronavirus disease 2019 (COVID-19) patients. Int. Forum Allergy Rhinol. 2022, 12, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Vaira, L.A.; De Vito, A.; Deiana, G.; Pes, C.; Giovanditto, F.; Fiore, V.; Lechien, J.R.; Le Bon, S.D.; Saussez, S.; Madeddu, G.; et al. Correlations between IL-6 serum level and olfactory dysfunction severity in COVID-19 patients: A preliminary study. Eur. Arch. Otorhinolaryngol. 2022, 279, 811–816. [Google Scholar] [CrossRef]
- Reden, J.; Maroldt, H.; Fritz, A.; Zahnert, T.; Hummel, T. A study on the prognostic significance of qualitative olfactory dysfunction. Eur. Arch. Otorhinolaryngol. 2007, 264, 139–144. [Google Scholar] [CrossRef]
- Puri, B.K.; Monro, J.A.; Julu, P.O.; Kingston, M.C.; Shah, M. Hyperosmia in Lyme disease. Arq. Neuropsiquiatr. 2014, 72, 596–597. [Google Scholar] [CrossRef] [Green Version]
- Di Stadio, A.; D’Ascanio, L.; De Luca, P.; Roccamatisi, D.; La Mantia, I.; Brenner, M.J. Hyperosmia after COVID-19: Hedonic perception or hypersensitivity? Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 2196–2200. [Google Scholar] [CrossRef]
- Marmura, M.J.; Monteith, T.S.; Anjum, W.; Doty, R.L.; Hegarty, S.E.; Keith, S.W. Olfactory function in migraine both during and between attacks. Cephalalgia 2014, 34, 977–985. [Google Scholar] [CrossRef]
- Sezille, C.; Fournel, A.; Rouby, C.; Rinck, F.; Bensafi, M. Hedonic appreciation and verbal description of pleasant and unpleasant odors in untrained, trainee cooks, flavorists, and perfumers. Front. Psychol. 2014, 5, 12. [Google Scholar] [CrossRef] [Green Version]
- Agyeman, A.A.; Chin, K.L.; Landersdorfer, C.B.; Liew, D.; Ofori-Asenso, R. Smell and Taste Dysfunction in Patients With COVID-19: A Systematic Review and Meta-analysis. Mayo Clin. Proc. 2020, 95, 1621–1631. [Google Scholar] [CrossRef] [PubMed]
- Whitcroft, K.L.; Hummel, T. Olfactory Dysfunction in COVID-19: Diagnosis and Management. JAMA 2020, 323, 2512–2514. [Google Scholar] [CrossRef] [PubMed]
- Ta, N.H.; Gao, J.; Philpott, C. A systematic review to examine the relationship between objective and patient-reported outcome measures in sinonasal disorders: Recommendations for use in research and clinical practice. Int. Forum Allergy Rhinol. 2021, 11, 910–923. [Google Scholar] [CrossRef] [PubMed]
- Duncan, H.J.; Seiden, A.M. Long-term follow-up of olfactory loss secondary to head trauma and upper respiratory tract infection. Arch. Otolaryngol. Head Neck Surg. 1995, 121, 1183–1187. [Google Scholar] [CrossRef]
- Rank, A.; Tzortzini, A.; Kling, E.; Schmid, C.; Claus, R.; Loll, E.; Burger, R.; Rommele, C.; Dhillon, C.; Muller, K.; et al. One Year after Mild COVID-19: The Majority of Patients Maintain Specific Immunity, But One in Four Still Suffer from Long-Term Symptoms. J. Clin. Med. 2021, 10, 3305. [Google Scholar] [CrossRef] [PubMed]
- Vaira, L.A.; Hopkins, C.; Sandison, A.; Manca, A.; Machouchas, N.; Turilli, D.; Lechien, J.R.; Barillari, M.R.; Salzano, G.; Cossu, A.; et al. Olfactory epithelium histopathological findings in long-term coronavirus disease 2019 related anosmia. J. Laryngol. Otol. 2020, 134, 1123–1127. [Google Scholar] [CrossRef]
- Dehgani-Mobaraki, P.; Zaidi, A.K.; Yadav, N.; Floridi, A.; Floridi, E. Longitudinal observation of antibody responses for 14 months after SARS-CoV-2 infection. Clin. Immunol. 2021, 230, 108814. [Google Scholar] [CrossRef]
- Luo, H.; Camilleri, D.; Garitaonandia, I.; Djumanov, D.; Chen, T.; Lorch, U.; Taubel, J.; Wang, D. Kinetics of anti-SARS-CoV-2 IgG antibody levels and potential influential factors in subjects with COVID-19: A 11-month follow-up study. Diagn. Microbiol. Infect. Dis. 2021, 101, 115537. [Google Scholar] [CrossRef]
- Lechien, J.R.; Diallo, A.O.; Dachy, B.; Le Bon, S.D.; Maniaci, A.; Vaira, L.A.; Saussez, S. COVID-19: Post-vaccine Smell and Taste Disorders: Report of 6 Cases. Ear Nose Throat J. 2021, 1455613211033125. [Google Scholar] [CrossRef]
- Russell, M.W.; Moldoveanu, Z.; Ogra, P.L.; Mestecky, J. Mucosal Immunity in COVID-19: A Neglected but Critical Aspect of SARS-CoV-2 Infection. Front. Immunol. 2020, 11, 611337. [Google Scholar] [CrossRef]
- Sheikh-Mohamed, S.; Sanders, E.C.; Gommerman, J.L.; Tal, M.C. Guardians of the oral and nasopharyngeal galaxy: IgA and protection against SARS-CoV-2 infection. Immunol. Rev. 2022, 309, 75–85. [Google Scholar] [CrossRef] [PubMed]
- Wheatley, A.K.; Juno, J.A.; Wang, J.J.; Selva, K.J.; Reynaldi, A.; Tan, H.X.; Lee, W.S.; Wragg, K.M.; Kelly, H.G.; Esterbauer, R.; et al. Evolution of immune responses to SARS-CoV-2 in mild-moderate COVID-19. Nat. Commun. 2021, 12, 1162. [Google Scholar] [CrossRef] [PubMed]
- Laura, L.; Dalmatin-Dragisic, M.; Martinovic, K.; Tutis, B.; Herceg, I.; Arapovic, M.; Arapovic, J. Does pre-existing immunity determine the course of SARS-CoV-2 infection in health-care workers? Single-center experience. Infection 2022, 1–8. [Google Scholar] [CrossRef]
- Ewer, K.J.; Barrett, J.R.; Belij-Rammerstorfer, S.; Sharpe, H.; Makinson, R.; Morter, R.; Flaxman, A.; Wright, D.; Bellamy, D.; Bittaye, M.; et al. T cell and antibody responses induced by a single dose of ChAdOx1 nCoV-19 (AZD1222) vaccine in a phase 1/2 clinical trial. Nat. Med. 2021, 27, 270–278. [Google Scholar] [CrossRef]
- Lechien, J.R.; Chiesa-Estomba, C.M.; Vaira, L.A.; Saussez, S.; Hans, S. COVID-19 Reinfection and Second Episodes of Olfactory and Gustatory Dysfunctions: Report of First Cases. Ear Nose Throat J. 2020, 145561320970105. [Google Scholar] [CrossRef]
- Lechien, J.R.; Chiesa-Estomba, C.M.; Radulesco, T.; Michel, J.; Vaira, L.A.; Le Bon, S.D.; Horoi, M.; Falanga, C.; Barillari, M.R.; Hans, S.; et al. Clinical features of patients who had two COVID-19 episodes: A European multicentre case series. J. Intern. Med. 2021, 290, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Wöchentlicher Lagebericht des RKI zur Coronavirus-Krankheit-2019 (COVID-19) 14.04.2022—AKTUALISIERTER STAND FÜR DEUTSCHLAND. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/Wochenbericht/Wochenbericht_2022-04-14.pdf?__blob=publicationFile (accessed on 22 July 2022).
- Wöchentlicher Lagebericht des RKI zur Coronavirus-Krankheit-2019 (COVID-19) 21.07.2022—AKTUALISIERTER STAND FÜR DEUTSCHLAND. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/Wochenbericht/Wochenbericht_2022-07-21.pdf?__blob=publicationFile (accessed on 25 July 2022).
- Brandal, L.T.; MacDonald, E.; Veneti, L.; Ravlo, T.; Lange, H.; Naseer, U.; Feruglio, S.; Bragstad, K.; Hungnes, O.; Odeskaug, L.E.; et al. Outbreak caused by the SARS-CoV-2 Omicron variant in Norway, November to December 2021. Euro Surveill 2021, 26, 2101147. [Google Scholar] [CrossRef]
- Meng, B.; Abdullahi, A.; Ferreira, I.; Goonawardane, N.; Saito, A.; Kimura, I.; Yamasoba, D.; Gerber, P.P.; Fatihi, S.; Rathore, S.; et al. Altered TMPRSS2 usage by SARS-CoV-2 Omicron impacts infectivity and fusogenicity. Nature 2022, 603, 706–714. [Google Scholar] [CrossRef]
- Rodriguez-Sevilla, J.J.; Guerri-Fernadez, R.; Bertran Recasens, B. Is There Less Alteration of Smell Sensation in Patients With Omicron SARS-CoV-2 Variant Infection? Front. Med. 2022, 9, 852998. [Google Scholar] [CrossRef]
- Vitale-Cross, L.; Szalayova, I.; Scoggins, A.; Palkovits, M.; Mezey, E. SARS-CoV-2 entry sites are present in all structural elements of the human glossopharyngeal and vagal nerves: Clinical implications. EBioMedicine 2022, 78, 103981. [Google Scholar] [CrossRef] [PubMed]
- Speth, M.M.; Singer-Cornelius, T.; Oberle, M.; Gengler, I.; Brockmeier, S.J.; Sedaghat, A.R. Mood, Anxiety and Olfactory Dysfunction in COVID-19: Evidence of Central Nervous System Involvement? Laryngoscope 2020, 130, 2520–2525. [Google Scholar] [CrossRef] [PubMed]
- Croy, I.; Symmank, A.; Schellong, J.; Hummel, C.; Gerber, J.; Joraschky, P.; Hummel, T. Olfaction as a marker for depression in humans. J. Affect. Disord. 2014, 160, 80–86. [Google Scholar] [CrossRef]
- Yom-Tov, E.; Lekkas, D.; Jacobson, N.C. Association of COVID19-induced anosmia and ageusia with depression and suicidal ideation. J. Affect. Disord. Rep. 2021, 5, 100156. [Google Scholar] [CrossRef]
- Cavazzana, A.; Larsson, M.; Munch, M.; Hahner, A.; Hummel, T. Postinfectious olfactory loss: A retrospective study on 791 patients. Laryngoscope 2018, 128, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Kollndorfer, K.; Kowalczyk, K.; Hoche, E.; Mueller, C.A.; Pollak, M.; Trattnig, S.; Schopf, V. Recovery of olfactory function induces neuroplasticity effects in patients with smell loss. Neural Plast. 2014, 2014, 140419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hummel, T.; Rissom, K.; Reden, J.; Hahner, A.; Weidenbecher, M.; Huttenbrink, K.B. Effects of olfactory training in patients with olfactory loss. Laryngoscope 2009, 119, 496–499. [Google Scholar] [CrossRef]
- Damm, M.; Pikart, L.K.; Reimann, H.; Burkert, S.; Goktas, O.; Haxel, B.; Frey, S.; Charalampakis, I.; Beule, A.; Renner, B.; et al. Olfactory training is helpful in postinfectious olfactory loss: A randomized, controlled, multicenter study. Laryngoscope 2014, 124, 826–831. [Google Scholar] [CrossRef] [PubMed]
- Geissler, K.; Reimann, H.; Gudziol, H.; Bitter, T.; Guntinas-Lichius, O. Olfactory training for patients with olfactory loss after upper respiratory tract infections. Eur. Arch. Otorhinolaryngol. 2014, 271, 1557–1562. [Google Scholar] [CrossRef]
- Pires, I.A.T.; Steffens, S.T.; Mocelin, A.G.; Shibukawa, D.E.; Leahy, L.; Saito, F.L.; Amadeu, N.T.; Lopes, N.M.D.; Garcia, E.C.D.; Albanese, M.L.; et al. Intensive Olfactory Training in Post-COVID-19 Patients: A Multicenter Randomized Clinical Trial. Am. J. Rhinol. Allergy 2022, 19458924221113124. [Google Scholar] [CrossRef] [PubMed]
- Vasconcelos, C.C.F.; Hammerle, M.B.; Sales, D.S.; Rueda Lopes, F.C.; Pinheiro, P.G.; Gouvea, E.G.; Alves, M.; Pereira, T.V.; Schmidt, S.L.; Alvarenga, R.M.P.; et al. Post-COVID-19 olfactory dysfunction: Carbamazepine as a treatment option in a series of cases. J. Neurovirol. 2022, 28, 312–318. [Google Scholar] [CrossRef] [PubMed]



| Parameter | Number of Participants (%) |
|---|---|
| Sample size | 44 (100%) |
| Gender | 29 F (65.9%) |
| Age at date of follow-up after 721 days (median, range) | 43, 24–63 |
| Active smoker | 5 (11.3%) |
| Number of infections with SARS-CoV-2 after 721 days | |
| One time | 24 (54.5%) |
| Two times | 18 (40.9%) |
| Three times | 1 (2.3%) |
| Four times | 1 (2.3%) |
| Received number of vaccinations after 721 days | |
| None | 2 (4.5%) |
| One | 2 (4.5%) |
| Two | 7 (15.9%) |
| Three | 33 (75.0%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schambeck, S.E.; Mateyka, L.M.; Burrell, T.; Graf, N.; Brill, I.; Stark, T.; Protzer, U.; Busch, D.H.; Gerhard, M.; Riehl, H.; et al. Two-Year Follow-Up on Chemosensory Dysfunction and Adaptive Immune Response after Infection with SARS-CoV-2 in a Cohort of 44 Healthcare Workers. Life 2022, 12, 1556. https://doi.org/10.3390/life12101556
Schambeck SE, Mateyka LM, Burrell T, Graf N, Brill I, Stark T, Protzer U, Busch DH, Gerhard M, Riehl H, et al. Two-Year Follow-Up on Chemosensory Dysfunction and Adaptive Immune Response after Infection with SARS-CoV-2 in a Cohort of 44 Healthcare Workers. Life. 2022; 12(10):1556. https://doi.org/10.3390/life12101556
Chicago/Turabian StyleSchambeck, Sophia E., Laura M. Mateyka, Teresa Burrell, Natalia Graf, Ioana Brill, Thomas Stark, Ulrike Protzer, Dirk H. Busch, Markus Gerhard, Henriette Riehl, and et al. 2022. "Two-Year Follow-Up on Chemosensory Dysfunction and Adaptive Immune Response after Infection with SARS-CoV-2 in a Cohort of 44 Healthcare Workers" Life 12, no. 10: 1556. https://doi.org/10.3390/life12101556
APA StyleSchambeck, S. E., Mateyka, L. M., Burrell, T., Graf, N., Brill, I., Stark, T., Protzer, U., Busch, D. H., Gerhard, M., Riehl, H., & Poppert, H. (2022). Two-Year Follow-Up on Chemosensory Dysfunction and Adaptive Immune Response after Infection with SARS-CoV-2 in a Cohort of 44 Healthcare Workers. Life, 12(10), 1556. https://doi.org/10.3390/life12101556