

Gamma Knife Radiosurgery as a Salvage Treatment for Nasopharyngeal Carcinoma with Skull Base and Intracranial Invasion (T4b)

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
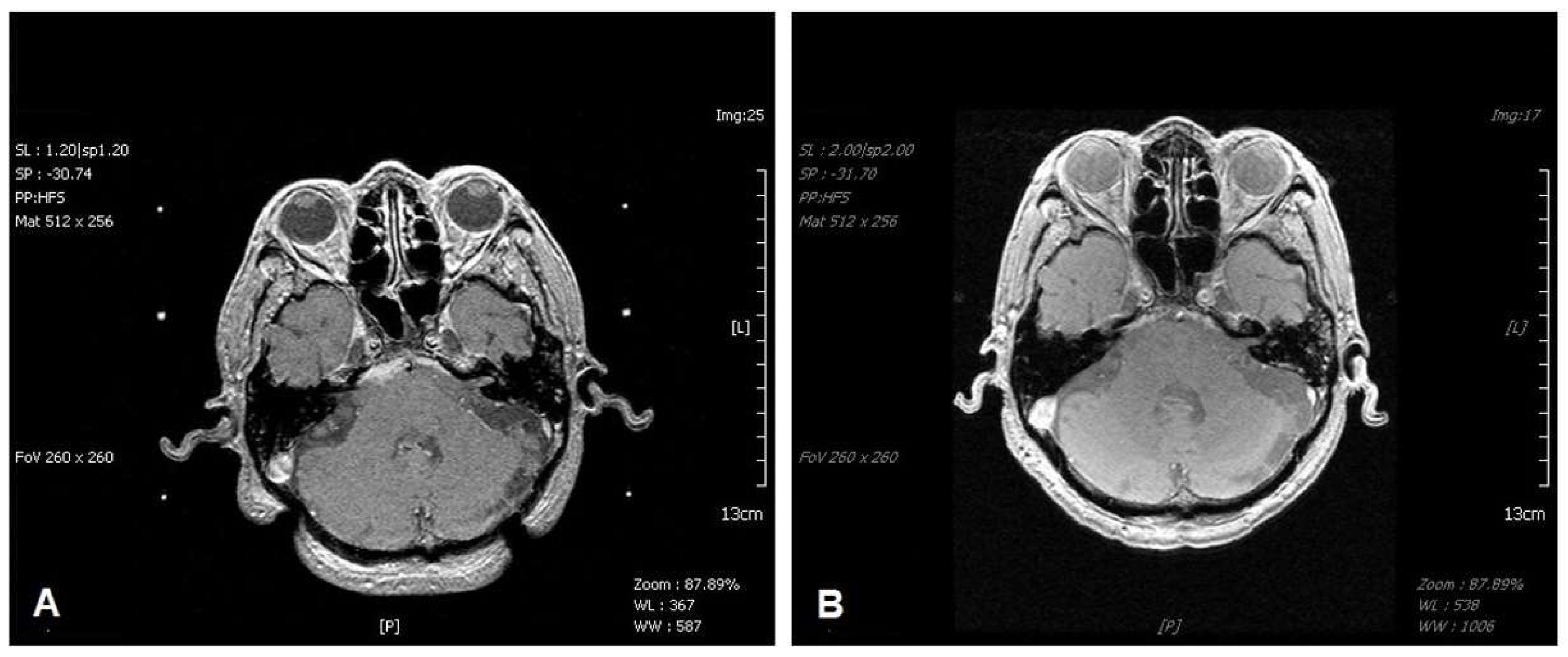
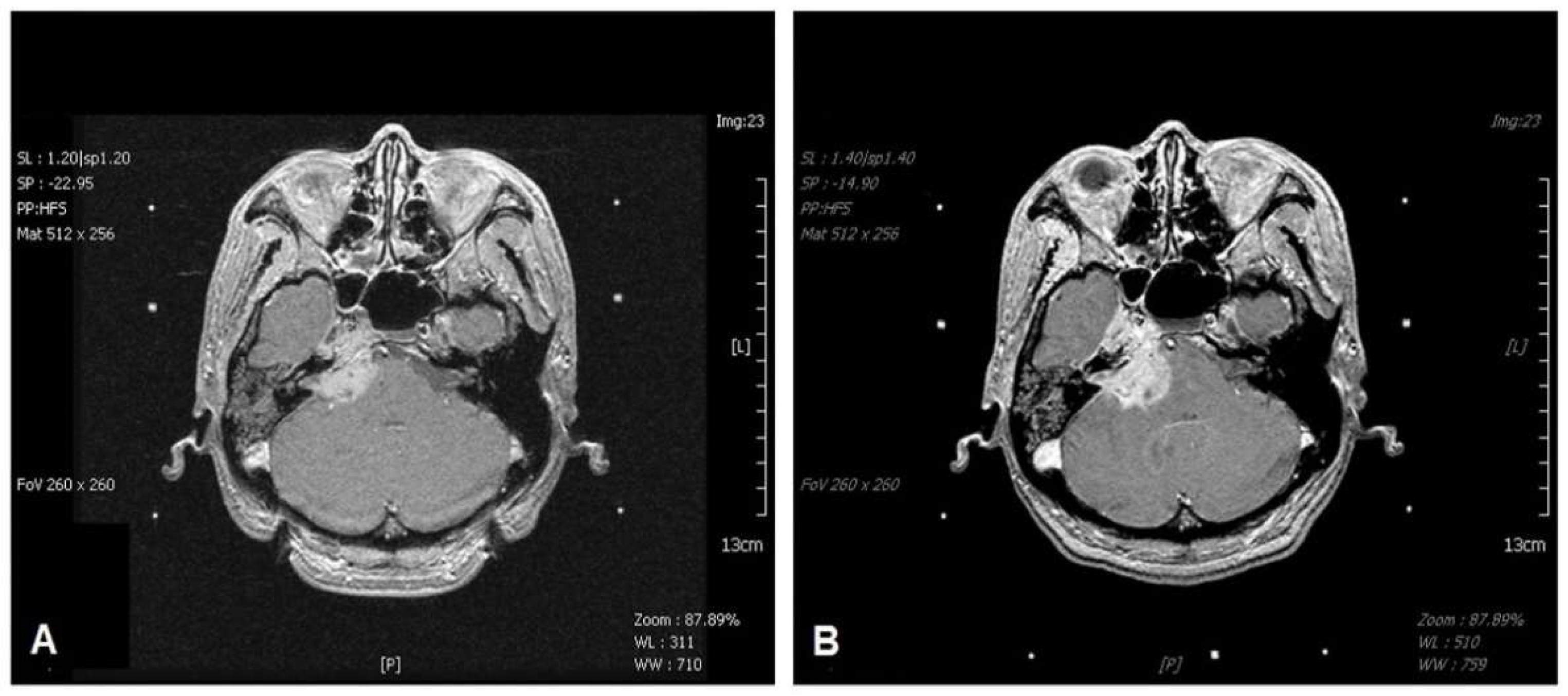
2.2. Magnetic Resonance Imaging Staging of T4b1 and T4b2
2.3. Clinical Data Collection
2.4. Gamma Knife Radiosurgery Technique
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Patients
3.2. Prognostic Significance of Tumor Volume, MRI Staging, KPS, and Other Metastases
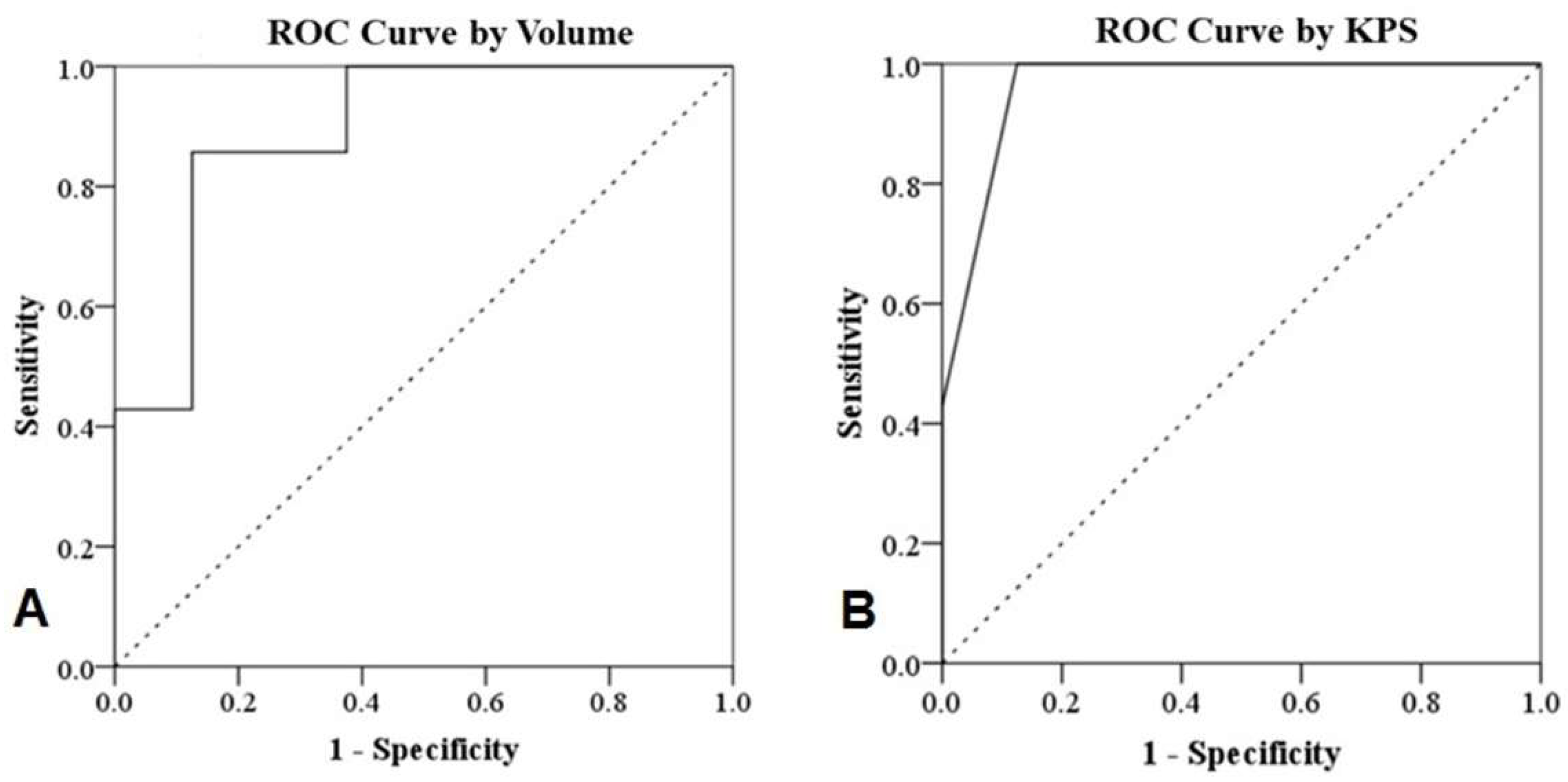
3.3. ROC Analysis
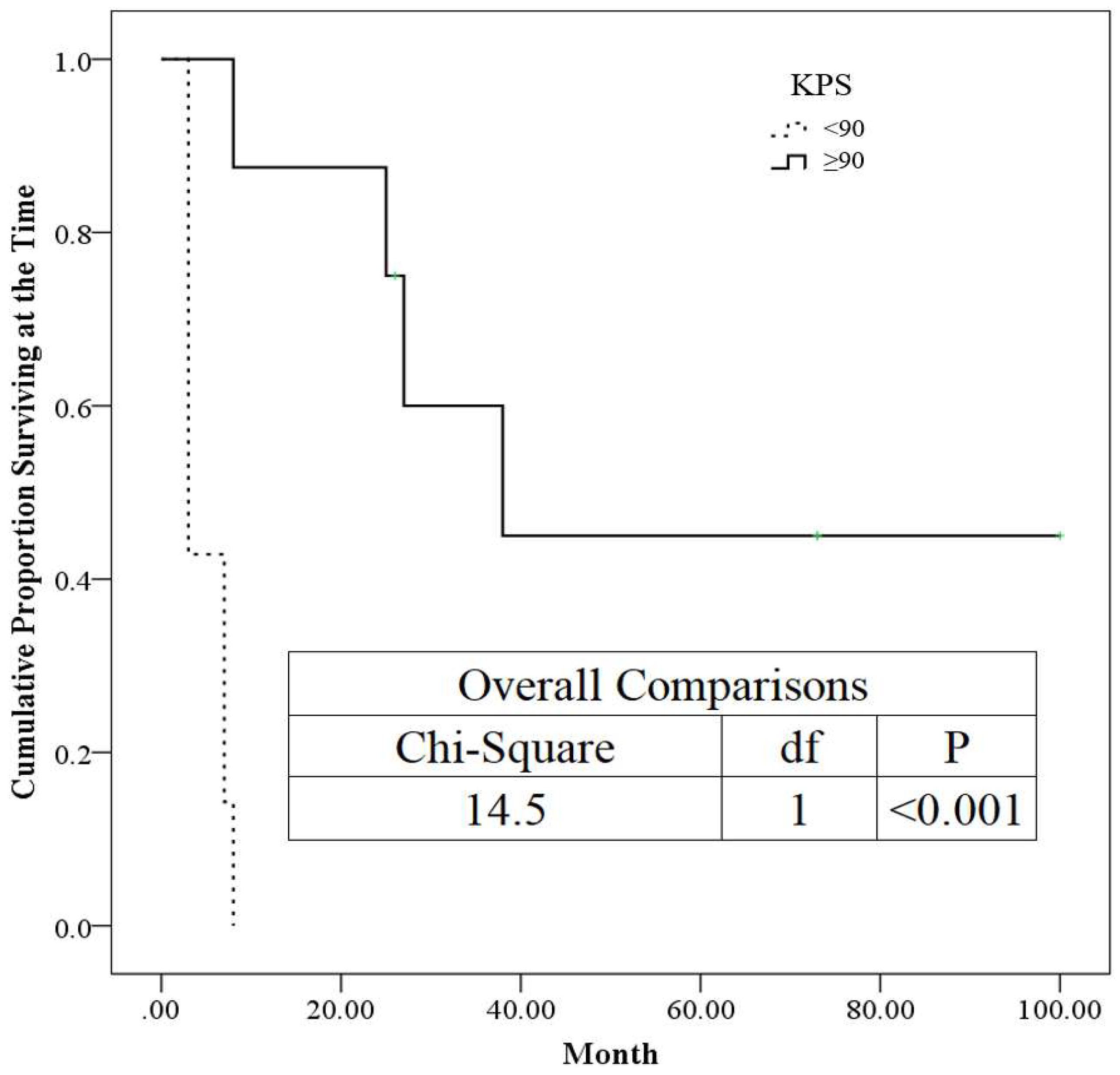
3.4. The Kaplan–Meier Plot for KPS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chang, E.T.; Adami, H.-O. The Enigmatic Epidemiology of Nasopharyngeal Carcinoma. Cancer Epidemiol. Biomark. Prev. 2006, 15, 1765–1777. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The International Agency for Research on Cancer. Pathology and Genetics of Head and Neck Tumors; World Health Organization Classification of Tumours, Barnes, L., Eveson, J.W., Reichart, P., Sidransky, D., Eds.; IARC Press: Lyon, France, 2005. [Google Scholar]
- Chen, Y.-P.; Chan, A.T.C.; Le, Q.-T.; Blanchard, P.; Sun, Y.; Ma, J. Nasopharyngeal carcinoma. Lancet 2019, 394, 64–80. [Google Scholar] [CrossRef]
- Lee, A.W.; Ng, W.T.; Pan, J.J.; Chiang, C.-L.; Poh, S.S.; Choi, H.C.; Ahn, Y.C.; AlHussain, H.; Corry, J.; Grau, C.; et al. International Guideline on Dose Prioritization and Acceptance Criteria in Radiation Therapy Planning for Nasopharyngeal Carcinoma. Int. J. Radiat. Oncol. Boil. Phys. 2019, 105, 567–580. [Google Scholar] [CrossRef] [PubMed]
- Au, K.; Ngan, R.K.; Ng, A.W.; Poon, D.M.; Ng, W.; Yuen, K.; Lee, V.H.; Tung, S.Y.; Chan, A.T.; Sze, H.C.; et al. Treatment outcomes of nasopharyngeal carcinoma in modern era after intensity modulated radiotherapy (IMRT) in Hong Kong: A report of 3328 patients (HKNPCSG 1301 study). Oral Oncol. 2018, 77, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Li, X.-Y.; Chen, Q.-Y.; Sun, X.-S.; Liu, S.-L.; Yan, J.-J.; Guo, S.-S.; Liu, L.-T.; Xie, H.-J.; Tang, Q.-N.; Liang, Y.-J.; et al. Ten-year outcomes of survival and toxicity for a phase III randomised trial of concurrent chemoradiotherapy versus radiotherapy alone in stage II nasopharyngeal carcinoma. Eur. J. Cancer 2019, 110, 24–31. [Google Scholar] [CrossRef]
- Hui, E.P.; Ma, B.B.; Chan, A.T. The emerging data on choice of optimal therapy for locally advanced nasopharyngeal carcinoma. Curr. Opin. Oncol. 2020, 32, 187–195. [Google Scholar] [CrossRef]
- Chee, J.; Ting, Y.; Ong, Y.K.; Chao, S.S.; Loh, K.S.; Lim, C.M. Relapse status as a prognostic factor in patients receiving salvage surgery for recurrent or residual nasopharyngeal cancer after definitive treatment. Head Neck 2016, 38, 1393–1400. [Google Scholar] [CrossRef]
- Lee, A.W.; Ma, B.; Ng, W.T.; Chan, A.T. Management of Nasopharyngeal Carcinoma: Current Practice and Future Perspective. J. Clin. Oncol. 2015, 33, 3356–3364. [Google Scholar] [CrossRef]
- Qu, W.; Li, S.; Zhang, M.; Qiao, Q. Pattern and prognosis of distant metastases in nasopharyngeal carcinoma: A large-population retrospective analysis. Cancer Med. 2020, 9, 6147–6158. [Google Scholar] [CrossRef]
- Liu, Y.-P.; Wen, Y.-H.; Tang, J.; Wei, Y.; You, R.; Zhu, X.-L.; Li, J.; Chen, L.; Ling, L.; Zhang, N.; et al. Endoscopic surgery compared with intensity-modulated radiotherapy in resectable locally recurrent nasopharyngeal carcinoma: A multicentre, open-label, randomised, controlled, phase 3 trial. Lancet Oncol. 2021, 22, 381–390. [Google Scholar] [CrossRef]
- Kong, L.; Wang, L.; Shen, C.; Hu, C.; Lu, J.J. Salvage Intensity-Modulated Radiation Therapy (IMRT) for Locally Recurrent Nasopharyngeal Cancer after Definitive IMRT: A Novel Scenario of the Modern Era. Sci. Rep. 2016, 6, 32883. [Google Scholar] [CrossRef] [PubMed]
- Smee, R.I.; Meagher, N.S.; Broadley, K.; Ho, T.; Williams, J.R.; Bridger, G.P. Recurrent nasopharyngeal carcinoma: Current management approaches. Am. J. Clin. Oncol. 2010, 33, 469–473. [Google Scholar] [CrossRef] [PubMed]
- Pai, P.-C.; Chuang, C.-C.; Wei, K.-C.; Tsang, N.-M.; Tseng, C.-K.; Chang, C.-N. Stereotactic radiosurgery for locally recurrent nasopharyngeal carcinoma. Head Neck 2002, 24, 748–753. [Google Scholar] [CrossRef] [PubMed]
- Chua, D.T.T.; Sham, J.S.T.; Hung, K.-N.; Leung, L.H.T.; Cheng, P.-W.; Kwong, P.W.K. Salvage treatment for persistent and recurrent T1-2 nasopharyngeal carcinoma by stereotactic radiosurgery. Head Neck 2001, 23, 791–798. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.-J.; Leung, S.W.; Su, C.-Y. Linear Accelerator Based Radiosurgery as a Salvage Treatment for Skull Base and Intracranial Invasion of Recurrent Nasopharyngeal Carcinomas. Am. J. Clin. Oncol. 2001, 24, 255–258. [Google Scholar] [CrossRef]
- Cmelak, A.J.; Cox, R.S.; Adler, J.R.; Fee, W.E.; Goffinet, D.R. Radiosurgery for skull base malignancies and nasopharyngeal carcinoma. Int. J. Radiat. Oncol. Boil. Phys. 1997, 37, 997–1003. [Google Scholar] [CrossRef]
- Leung, T.-W.; Wong, V.Y.; Tung, S.Y. Stereotactic Radiotherapy for Locally Recurrent Nasopharyngeal Carcinoma. Int. J. Radiat. Oncol. Boil. Phys. 2009, 75, 734–741. [Google Scholar] [CrossRef]
- Low, J.S.H.; Chua, E.-T.; Gao, F.; Wee, J.T.S. Stereotactic radiosurgery plus intracavitary irradiation in the salvage of nasopharyngeal carcinoma. Head Neck 2006, 28, 321–329. [Google Scholar] [CrossRef]
- Kotecha, R.; Angelov, L.; Barnett, G.H.; Reddy, C.A.; Suh, J.H.; Murphy, E.S.; Neyman, G.; Chao, S.T. Calvarial and skull base metastases: Expanding the clinical utility of Gamma Knife surgery. J. Neurosurg. 2014, 121, 91–101. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.; Park, S.-H.; Yoon, S.-Y.; Park, K.-S.; Hwang, J.-H.; Hwang, S.-K. Gamma Knife Radiosurgery Using Co-Registration with PET-CT and MRI for Recurrent Nasopharyngeal Carcinoma with Previous Radiotherapy: A Single Center 14-Year Experience. J. Korean Neurosurg. Soc. 2020, 63, 397–405. [Google Scholar] [CrossRef]
- Park, S.-H.; Yoon, S.-Y.; Park, K.-S.; Hwang, J.-H.; Hwang, S.-K. Brain Metastasis from Nasopharyngeal Carcinoma Treated with Stereotactic Radiosurgery. World Neurosurg. 2019, 126, 160–163. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Liu, L.-Z.; Chen, M.; Li, W.-F.; Yin, W.-J.; Lin, A.-H.; Sun, Y.; Li, L.; Ma, J. Prognostic Value of Subclassification Using MRI in the T4 Classification Nasopharyngeal Carcinoma Intensity-Modulated Radiotherapy Treatment. Int. J. Radiat. Oncol. Boil. Phys. 2012, 84, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Amin, B.; Gress, D.M.; Meyer Vega, L.R.; Edge, S.B. Nasopharynx. In AJCC Cancer Staging Manual, 8th ed.; Amin, M.B., Greene, F.L., Byrd, D.R., Brookland, R.K., Washington, M.K., Compton, C.C., Eds.; Springer: New York, NY, USA, 2017; p. 103. [Google Scholar]
- Pikis, S.; Mantziaris, G.; Peker, S.; Samanci, Y.; Nabeel, A.M.; Reda, W.A.; Tawadros, S.R.; El-Shehaby, A.M.N.; Abdelkarim, K.; Eldin, R.M.E.; et al. Stereotactic radiosurgery for intracranial chordomas: An international multiinstitutional study. J. Neurosurg. 2022, 1–8. [Google Scholar] [CrossRef]
- Hung, Y.C.; Lee, C.C.; Yang, H.C.; Mohammed, N.; Kearns, K.N.; Sun, S.B.; Mathieu, D.; Touchette, C.J.; Atik, A.F.; Grills, I.S.; et al. Stereotactic radiosurgery for central neurocytomas: An international multicenter retrospective cohort study. J. Neurosurg. 2020, 134, 1122–1131. [Google Scholar] [CrossRef]
- Kondziolka, D.; Bernstein, K.; Lee, C.-C.; Yang, H.-C.; Liscak, R.; May, J.; Martínez-Álvarez, R.; Martínez-Moreno, N.; Bunevicius, A.; Sheehan, J.P. Stereotactic radiosurgery for Rathke’s cleft cysts: An international multicenter study. J. Neurosurg. 2022, 1–6. [Google Scholar] [CrossRef]
- Sun, X.; Su, S.; Chen, C.; Han, F.; Zhao, C.; Xiao, W.; Deng, X.; Huang, S.; Lin, C.; Lu, T. Long-term outcomes of intensity-modulated radiotherapy for 868 patients with nasopharyngeal carcinoma: An analysis of survival and treatment toxicities. Radiother. Oncol. 2014, 110, 398–403. [Google Scholar] [CrossRef]
- Nilsson, J.S.; Forslund, O.; Andersson, F.C.; Lindstedt, M.; Greiff, L. Intralesional EBV-DNA load as marker of prognosis for nasopharyngeal cancer. Sci. Rep. 2019, 9, 15432. [Google Scholar] [CrossRef] [Green Version]
- Chua, D.T.; Wei, W.I.; Sham, J.S.; Hung, K.N.; Au, G.K. Stereotactic Radiosurgery Versus Gold Grain Implantation in Salvaging Local Failures of Nasopharyngeal Carcinoma. Int. J. Radiat. Oncol. Boil. Phys. 2007, 69, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Chua, D.T.; Sham, J.S.; Kwong, P.W.; Hung, K.-N.; Leung, L.H. Linear accelerator-based stereotactic radiosurgery for limited, locally persistent, and recurrent nasopharyngeal carcinoma: Efficacy and complications. Int. J. Radiat. Oncol. Boil. Phys. 2003, 56, 177–183. [Google Scholar] [CrossRef]
- Chua, D.T.; Sham, J.S.; Hung, K.-N.; Leung, L.H.; Au, G.K. Predictive factors of tumor control and survival after radiosurgery for local failures of nasopharyngeal carcinoma. Int. J. Radiat. Oncol. Boil. Phys. 2006, 66, 1415–1421. [Google Scholar] [CrossRef]
- Dogan, O.Y.; Yaprak, G.; Ozyurt, H.; Bicakci, B.C.; Demircioglu, F.; Algul, E.; Isik, N. Is fractionated robotic stereotactic body radiosurgery optional salvage treatment for the re-irradiation of locally recurrent nasopharyngeal carcinoma? J. Cancer Res. Ther. 2022, 18, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Liang, S.; Li, L.; Mao, Y.; Tang, L.; Tian, L.; Liao, X.; Cui, C.; Lin, A.; Ma, J. Prognostic impact of magnetic resonance imaging-detected cranial nerve involvement in nasopharyngeal carcinoma. Cancer 2009, 115, 1995–2003. [Google Scholar] [CrossRef] [PubMed]
- Batsakis, J.G. Nerves and Neurotropic Carcinomas. Ann. Otol. Rhinol. Laryngol. 1985, 94, 426–427. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Liu, L.Z.; Mao, Y.P.; Chen, L.; Tang, L.-L.; Zhou, G.-Q.; Sun, Y.; Yue, D.; Lin, A.-H.; Li, L.; et al. Prognostic value of magnetic resonance imaging-detected cranial nerve invasion in nasopharyngeal carcinoma. Br. J. Cancer 2014, 110, 1465–1471. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Predictors | All (N = 15) | Group 1 (Good Outcome) (N = 7) | Group 2 (Poor Outcome) (N = 8) | p-Value |
|---|---|---|---|---|
| Gender (Male) (%) | 12 (80) | 5 (71) | 7 (88) | 0.569 † |
| Age (Mean ± SD) (year) | 51.3 ± 10.3 | 56.4 ± 10.8 | 46.8 ± 7.9 | 0.76 |
| Prescription isodose line | 51.3 ± 1.3 | 50.7 ± 1.9 | 50.0 ± 0 | 0.231 |
| Number of isocenters | 21.7 ± 6.4 | 19.6 ± 6.0 | 23.6 ± 6.5 | 0.302 |
| Tumor volume (Mean ± SD) (cm3) | 12.0 ± 6.2 | 7.9 ± 4.1 | 15.5 ± 5.7 | 0.012 |
| Marginal dose (Mean ± SD) (Gy) | 12.0 ± 2.0 | 12.2 ± 1.5 | 11.8 ± 2.4 | 0.659 |
| Maximal dose (Mean ± SD) (Gy) | 22.9 ± 4.0 | 22.9 ± 2.7 | 23.0 ± 5.0 | 0.956 |
| KPS (Mean (Median) ± SD) | 86.0 (90.0) ± 9.9 | 94.3 (90.0) ± 5.3 | 78.8 (80.0) ± 6.4 | <0.001 |
| Brain MRI | 0.041 † | |||
| Extradural (T4b1) | 8 | 6 | 2 | |
| Intradural (T4b2) | 7 | 1 | 6 | |
| Other metastasis | 0.007 † | |||
| No | 9 | 7 | 2 | |
| Yes | 6 | 0 | 6 | |
| Survival (Mean ± SD) (months) | 26.9 ± 31.1 | 51.7 ± 30.0 | 5.3 ± 2.4 | 0.006 |
| Variable | AUC | 95% Confidence Interval | p-Value | Maximal Yuden Index | Cut-Off * Value | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Volume | 0.893 | 0.725 | 1.000 | 0.011 | 0.536 | 11.750 |
| KPS | 0.964 | 0.873 | 1.000 | 0.003 | 0.875 | 85.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chu, S.-A.; Chen, T.-B.; Chen, H.-J.; Wang, K.-W.; Chen, J.-S.; Chuang, F.-C.; Wang, H.-K.; Liang, C.-L. Gamma Knife Radiosurgery as a Salvage Treatment for Nasopharyngeal Carcinoma with Skull Base and Intracranial Invasion (T4b). Life 2022, 12, 1880. https://doi.org/10.3390/life12111880
Chu S-A, Chen T-B, Chen H-J, Wang K-W, Chen J-S, Chuang F-C, Wang H-K, Liang C-L. Gamma Knife Radiosurgery as a Salvage Treatment for Nasopharyngeal Carcinoma with Skull Base and Intracranial Invasion (T4b). Life. 2022; 12(11):1880. https://doi.org/10.3390/life12111880
Chicago/Turabian StyleChu, Shao-Ang, Tai-Been Chen, Han-Jung Chen, Kuo-Wei Wang, Jui-Sheng Chen, Fu-Cheng Chuang, Hao-Kuang Wang, and Cheng-Loong Liang. 2022. "Gamma Knife Radiosurgery as a Salvage Treatment for Nasopharyngeal Carcinoma with Skull Base and Intracranial Invasion (T4b)" Life 12, no. 11: 1880. https://doi.org/10.3390/life12111880
APA StyleChu, S. -A., Chen, T. -B., Chen, H. -J., Wang, K. -W., Chen, J. -S., Chuang, F. -C., Wang, H. -K., & Liang, C. -L. (2022). Gamma Knife Radiosurgery as a Salvage Treatment for Nasopharyngeal Carcinoma with Skull Base and Intracranial Invasion (T4b). Life, 12(11), 1880. https://doi.org/10.3390/life12111880