

Post Surgical Management of WHO Grade II Meningiomas: Our Experience, the Role of Gamma Knife and a Literature Review

 ,
,  and
and
Abstract
:1. Background
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Exclusion Criteria
- (a)
- Age under 16 years
- (b)
- Type II neurofibromatosis (NF-2)
- (c)
- Sheath meningiomas of the optic nerve
- (d)
- Pregnant or breastfeeding women
2.3. Data Collection and Definitions
2.3.1. Baseline Characteristics
2.3.2. Post-Surgical Management
- -
- Wait and see;
- -
- Conventional adjuvant radiotherapy;
- -
- Stereotactic GKRS radiosurgery.
2.3.3. Follow-Up
- -
- Stable;
- -
- Local/marginal recurrence: recurrence within 2 cm from the margins of surgical cavity;
- -
- Distant recurrence.
2.3.4. Patient with GKRS Treatment
2.4. Statistical Analysis
3. Results
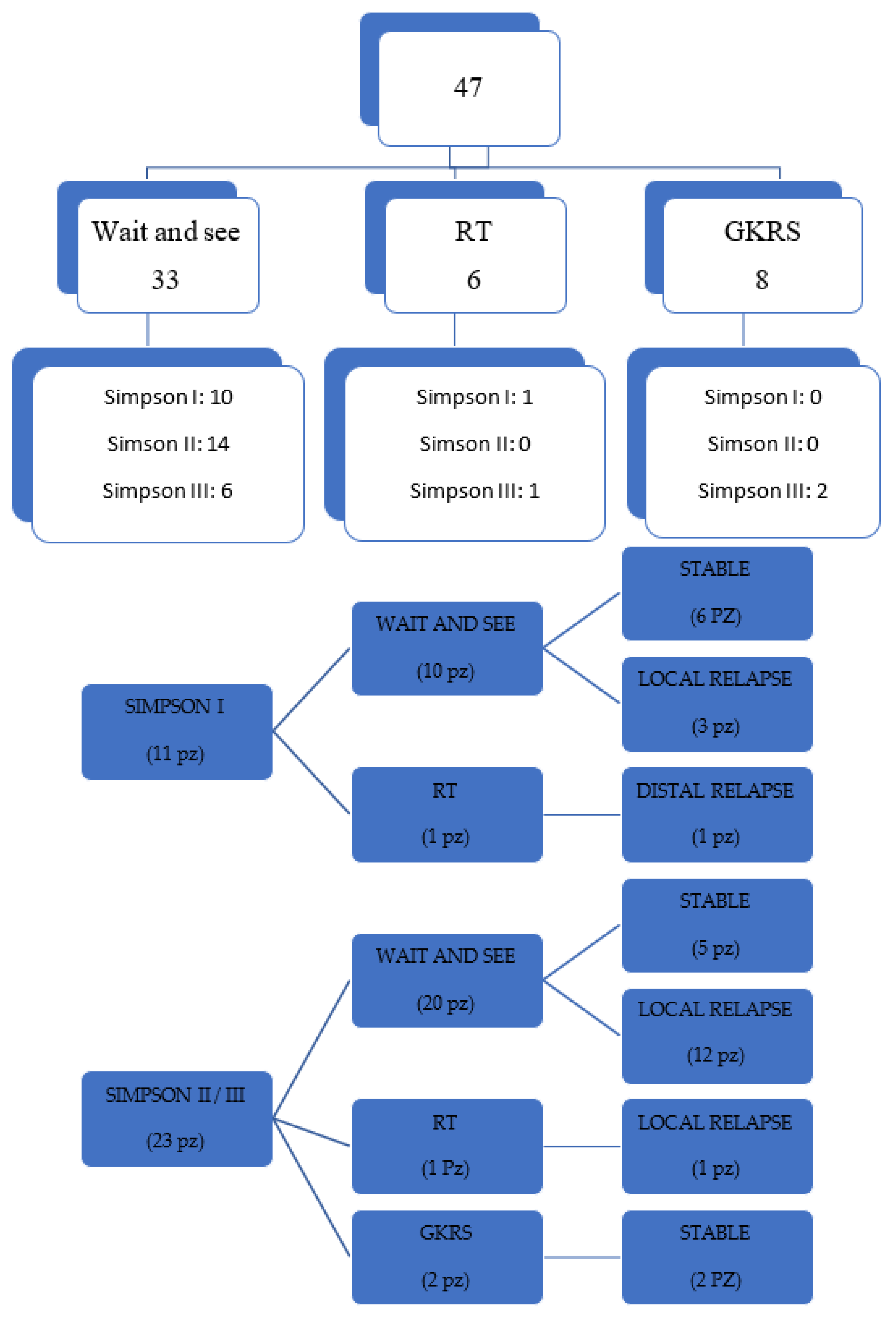
3.1. Post-Surgical Management
3.2. Follow-Up
3.3. Simpson I
3.4. Simpson II and III
3.5. Patients with GKRS Treatment
4. Discussion
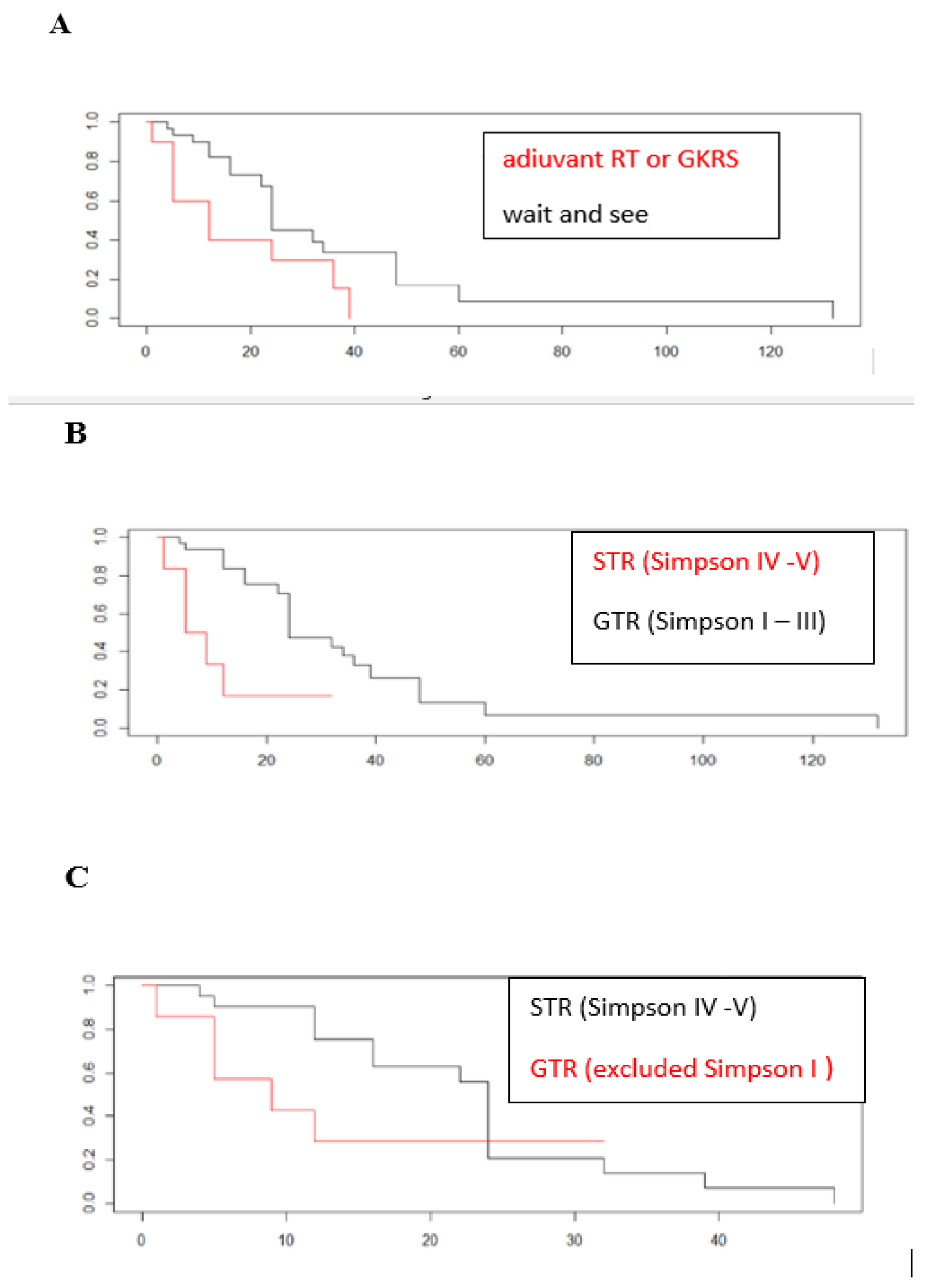
4.1. PFS and Simpson Grade
4.2. GKRS Outcome
4.3. Study Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Rogers, L.; Zhang, P.; Vogelbaum, M.A.; Perry, A.; Ashby, L.S.; Modi, J.M.; Alleman, A.M.; Galvin, J.; Brachman, D.; Jenrette, J.M.; et al. Intermediate-risk meningioma: Initial outcomes from NRG Oncology RTOG 0539. J Neurosurg. 2018, 129, 35–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Louis, D.N.; Perry, A.; Reifenberger, G.; Von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simpson, D. The recurrence of intracranial meningiomas after surgical treatment. J. Neurol. Neurosurg. Psychiatry 1957, 20, 22–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marcus, H.J.; Price, S.J.; Wilby, M.; Santarius, T.; Kirollos, R.W. Radiotherapy as an adjuvant in the management of intracranial meningiomas: Are we practising evidence-based medicine? Br. J. Neurosurg. 2008, 22, 520–528. [Google Scholar] [CrossRef] [PubMed]
- Simon, M.; Boström, J.; Koch, P.; Schramm, J. Interinstitutional variance of postoperative radiotherapy and follow up for meningiomas in Germany: Impact of changes of the WHO classification. J. Neurol. Neurosurg. Psychiatry 2006, 77, 767–773. [Google Scholar] [CrossRef] [Green Version]
- Apra, C.; Peyre, M.; Kalamarides, M. Current treatment options for meningioma. Expert Rev. Neurother. 2018, 18, 241–249. [Google Scholar] [CrossRef]
- Goldbrunner, R.; Minniti, G.; Preusser, M.; Jenkinson, M.D.; Sallabanda, K.; Houdart, E.; von Deimling, A.; Stavrinou, P.; Lefranc, F.; Lund-Johansen, M.; et al. EANO guidelines for the diagnosis and treatment of meningiomas. Lancet Oncol. 2016, 17, e383–e391. [Google Scholar] [CrossRef] [Green Version]
- Toma-Dasu, I.; Wojcik, A.; Kjellsson Lindblom, E. Risk of second cancer following radiotherapy. Phys. Med. 2017, 42, 211–212. [Google Scholar] [CrossRef]
- Rogers, L.; Barani, I.; Chamberlain, M.; Kaley, T.J.; McDermott, M.; Raizer, J.; Schiff, D.; Weber, D.C.; Wen, P.Y.; Vogelbaum, M.A. Meningiomas: Knowledge base, treatment outcomes, and uncertainties. A RANO review. J. Neurosurg. 2015, 122, 4–23. [Google Scholar] [CrossRef] [Green Version]
- Behling, F.; Fodi, C.; Hoffmann, E.; Renovanz, M.; Skardelly, M.; Tabatabai, G.; Schittenhelm, J.; Honegger, J.; Tatagiba, M. The role of Simpson grading in meningiomas after integration of the updated WHO classification and adjuvant radiotherapy. Neurosurg. Rev. 2021, 44, 2329–2336. [Google Scholar] [CrossRef]
- Soni, P.; Davison, M.A.; Shao, J.; Momin, A.; Lopez, D.; Angelov, L.; Barnett, G.H.; Lee, J.H.; Mohammadi, A.M.; Kshettry, V.R.; et al. Extent of resection and survival outcomes in World Health Organization grade II meningiomas. J. Neurooncol. 2021, 151, 173–179. [Google Scholar] [CrossRef]
- Hasan, S.; Young, M.; Albert, T.; Shah, A.H.; Okoye, C.; Bregy, A.; Lo, S.S.; Ishkanian, F.; Komotar, R.J. The role of adjuvant radiotherapy after gross total resection of atypical meningiomas. World Neurosurg. 2015, 83, 808–815. [Google Scholar] [CrossRef]
- Aghi, M.K.; Carter, B.S.; Cosgrove, G.R.; Ojemann, R.G.; Amin-Hanjani, S.; Martuza, R.L.; Curry, W.T.; Barker, F.G. Long-term recurrence rates of atypical meningiomas after gross total resection with or without postoperative adjuvant radiation. Neurosurgery 2009, 64, 56–60; discussion 60. [Google Scholar] [CrossRef] [PubMed]
- Graffeo, C.S.; Leeper, H.E.; Perry, A.; Uhm, J.H.; Lachance, D.J.; Brown, P.D.; Ma, D.J.; Van Gompel, J.J.; Giannini, C.; Johnson, D.R.; et al. Revisiting Adjuvant Radiotherapy After Gross Total Resection of World Health Organization Grade II Meningioma. World Neurosurg. 2017, 103, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Pasquier, D.; Bijmolt, S.; Veninga, T.; Rezvoy, N.; Villa, S.; Krengli, M.; Weber, D.C.; Baumert, B.G.; Canyilmaz, E.; Yalman, D.; et al. Atypical and malignant meningioma: Outcome and prognostic factors in 119 irradiated patients. A multicenter, retrospective study of the Rare Cancer Network. Int. J. Radiat. Oncol. Biol. Phys. 2008, 71, 1388–1393. [Google Scholar] [CrossRef] [PubMed]
- Attia, A.; Chan, M.D.; Mott, R.T.; Russell, G.B.; Seif, D.; Bourland, J.D.; Deguzman, A.F.; Ellis, T.L.; McMullen, K.P.; Munley, M.T.; et al. Patterns of failure after treatment of atypical meningioma with gamma knife radiosurgery. J. Neurooncol. 2012, 108, 179–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenkinson, M.D.; Javadpour, M.; Haylock, B.J.; Young, B.; Gillard, H.; Vinten, J.; Bulbeck, H.; Das, K.; Farrell, M.; Looby, S.; et al. The ROAM/EORTC-1308 trial: Radiation versus Observation following surgical resection of Atypical Meningioma: Study protocol for a randomised controlled trial. Trials 2015, 16, 519. [Google Scholar] [CrossRef] [Green Version]
- Weber, D.C.; Ares, C.; Villa, S.; Peerdeman, S.M.; Renard, L.; Baumert, B.G.; Lucas, A.; Veninga, T.; Pica, A.; Jefferies, S.; et al. Adjuvant postoperative high-dose radiotherapy for atypical and malignant meningioma: A phase-II parallel non-randomized and observation study (EORTC 22042-26042). Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2018, 128, 260–265. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.; Cho, Y.H.; Kim, J.H.; Kim, C.J.; Roh, S.W.; Kwon, D.H. Role of gamma knife radiosurgery for recurrent or residual World Health Organization grade II and III intracranial meningiomas. Br. J. Neurosurg. 2020, 34, 239–245. [Google Scholar] [CrossRef]
- Pettersson-Segerlind, J.; Fletcher-Sandersjöö, A.; von Vogelsang, A.-C.; Persson, O.; Linder, L.K.B.; Förander, P.; Mathiesen, T.; Edström, E.; Elmi-Terander, A. Long-Term Follow-Up, Treatment Strategies, Functional Outcome, and Health-Related Quality of Life after Surgery for WHO Grade 2 and 3 Intracranial Meningiomas. Cancers 2022, 14, 5038. [Google Scholar] [CrossRef]
- Nanda, A.; Bir, S.C.; Konar, S.; Maiti, T.; Kalakoti, P.; Jacobsohn, J.A.; Guthikonda, B. Outcome of resection of WHO Grade II meningioma and correlation of pathological and radiological predictive factors for recurrence. J. Clin. Neurosci. Off. J. Neurosurg. Soc. Australas. 2016, 31, 112–121. [Google Scholar] [CrossRef] [PubMed]
- Stafford, S.L.; Pollock, B.E.; Foote, R.L.; Link, M.J.; Gorman, D.A.; Schomberg, P.J.; Leavitt, J.A. Meningioma radiosurgery: Tumor control, outcomes, and complications among 190 consecutive patients. Neurosurgery 2001, 49, 1028–1029. [Google Scholar] [CrossRef]
- Harris, A.E.; Lee, J.Y.K.; Omalu, B.; Flickinger, J.C.; Kondziolka, D.; Lunsford, L.D. The effect of radiosurgery during management of aggressive meningiomas. Surg. Neurol. 2003, 60, 298–305; discussion 305. [Google Scholar] [CrossRef] [PubMed]
- Huffmann, B.C.; Reinacher, P.C.; Gilsbach, J.M. Gamma knife surgery for atypical meningiomas. J. Neurosurg. 2005, 283–286. [Google Scholar] [CrossRef]
- Malik, I.; Rowe, J.G.; Walton, L.; Radatz, M.W.R.; Kemeny, A.A. The use of stereotactic radiosurgery in the management of meningiomas. Br. J. Neurosurg. 2005, 19, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Kondziolka, D.; Mathieu, D.; Lunsford, L.D.; Martin, J.J.; Madhok, R.; Niranjan, A.; Flickinger, J.C. Radiosurgery as definitive management of intracranial meningiomas. Neurosurgery 2008, 62, 53–60. [Google Scholar] [CrossRef] [Green Version]
- Pollock, B.E.; Stafford, S.L.; Link, M.J.; Garces, Y.I.; Foote, R.L. Stereotactic radiosurgery of World Health Organization grade II and III intracranial meningiomas: Treatment results on the basis of a 22-year experience. Cancer 2012, 118, 1048–1054. [Google Scholar] [CrossRef] [PubMed]
- Hanakita, S.; Koga, T.; Igaki, H.; Murakami, N.; Oya, S.; Shin, M.; Saito, N. Role of gamma knife surgery for intracranial atypical (WHO grade II) meningiomas. J. Neurosurg. 2013, 119, 1410–1414. [Google Scholar] [CrossRef] [Green Version]
- Mori, Y.; Tsugawa, T.; Hashizume, C.; Kobayashi, T.; Shibamoto, Y. Gamma knife stereotactic radiosurgery for atypical and malignant meningiomas. Acta Neurochir. Suppl. 2013, 116, 85–89. [Google Scholar] [CrossRef]
- Tamura, M.; Kubo, K.; Okita, R.; Ogura, M.; Nakao, N.; Uematsu, Y.; Itakura, T.; Hayashi, M.; Muragaki, Y.; Iseki, H. Management of non-benign meningiomas with Gamma Knife radiosurgery. Acta Neurochir. Suppl. 2013, 116, 91–97. [Google Scholar] [CrossRef]
- Ferraro, D.J.; Funk, R.K.; Blackett, J.W.; Ju, M.R.; DeWees, T.A.; Chicoine, M.R.; Dowling, J.L.; Rich, K.M.; Drzymala, R.E.; Zoberi, I.; et al. A retrospective analysis of survival and prognostic factors after stereotactic radiosurgery for aggressive meningiomas. Radiat. Oncol. 2014, 9, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, W.-H.; Lee, C.-C.; Yang, H.-C.; Liu, K.-D.; Wu, H.-M.; Shiau, C.-Y.; Guo, W.-Y.; Pan, D.H.-C.; Chung, W.-Y.; Chen, M.-T. Gamma Knife Radiosurgery for Atypical and Anaplastic Meningiomas. World Neurosurg. 2016, 87, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Goldsmith, B.J.; Wara, W.M.; Wilson, C.B.; Larson, D.A. Postoperative irradiation for subtotally resected meningiomas. A retrospective analysis of 140 patients treated from 1967 to 1990. J. Neurosurg. 1994, 80, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, A.; Caccamo, D.V.; Tomecek, F.J.; Malik, G.M. Atypical and malignant meningiomas: A clinicopathological review. Neurosurgery 1993, 33, 955–963. [Google Scholar] [CrossRef] [PubMed]
- Weber, R.G.; Boström, J.; Wolter, M.; Baudis, M.; Collins, V.P.; Reifenberger, G.; Lichter, P. Analysis of genomic alterations in benign, atypical, and anaplastic meningiomas: Toward a genetic model of meningioma progression. Proc. Natl. Acad. Sci. USA 1997, 94, 14719–14724. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N° of Patients or Median (% or Range) | |
|---|---|
| Age | 66.79 (37–82) |
| Male | 18 (48.6%) |
| KPS | |
| ≥80 | 28 (68.3%) |
| <80 | 13 (31.7%) |
| Location | |
| Parasagittal | 11 (23.4%) |
| Convexity | 10 (21.27%) |
| Falx | 10 (21.27%) |
| Lateral and middle sphenoid wing | 7 (14.89) |
| Clinoidal e cavernous sinus | 3 (6.38%) |
| Intraventricular | 1 (2.12%) |
| Planum | 2 (4.24%) |
| Tentorial | 3 (6.38%) |
| Edema | |
| Yes | 37 (76.6%) |
| No | 11 (23.40%) |
| Simpson grade | |
| I | 11 (23.4%) |
| II | 14 (29.78%) |
| III | 9 (19.14%) |
| IV | 9 (19.14%) |
| V | 4 (8.51%) |
| Neurological symptoms | |
| Incidental finding | 3 (6.38%) |
| Headache | 11 (23.4%) |
| Focal deficit | 17 (36.17%) |
| Seizure | 8 (17.02%) |
| Swellings | 1 (2.12%) |
| Behavioral changes | 2 (4.25%) |
| Anatomopathological features | |
| Ki67 | 15 (4–30) |
| N° mitosis | 8.71 (4–20) |
| Brain invasion | 12 (25.53%) |
| Follow up | |
| Present | 43 (91.48%) |
| Months | 28 (6–48) |
| Management post op | |
| Wait and see | 33 (70.21%) |
| Adjuvant RT | 6 (12.76%) |
| Gamma Knife | 8 (17.02%) |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| HR | p Value | HR | p Value | |
| Age | 1.01 | 0.66 | 1.035263 | 0.458939 |
| KPS | 0.999 | 0.99 | 0.942709 | 0.410907 |
| Ki67 | 0.997 | 0.94 | 0.981073 | 0.778205 |
| Mitosis | 1.042 | 0.26 | 1.060144 | 0.444375 |
| Brain Invasion | 0.984 | 0.97 | 1.566417 | 0.217828 |
| Simpson grade I–III (GTR) | 0.249 | 0.0087 | 0.069585 | 0.026726 |
| Edema | 0.794 | 0.59 | 0.337299 | 0.212718 |
| Location | Simpson Grade | GK Adjuvant o Alla Relapse | Volume | Total Dose (Max/Min) | Fractionated GKRS | Follow Up (Months) | Complication | |
|---|---|---|---|---|---|---|---|---|
| 1, 58 y | falx | III | Adjuvant | 10.916 | 13 Gy (9.2–26) | NO | Stable (24) | NO |
| 2, 58 y | falx | III | Adjuvant | 4.729 | 14 Gy (28–12) | NO | Stable (24) | NO |
| 3, 75 y | covexity | II | Relapse (24 m) | 6.594 | 15 Gy (30–10.9) | NO | Stable (22) | NO |
| 4, 91 y | parasaggittal | III | Relapse (22 m) after RT | 21.709 | 22.5 Gy (45–16.8) | SI | Stable (13) | NO |
| 5, 71 y | falx | II | Relapse (16 m) | 9.891 | 15 Gy (30–7.1) | NO | Stable (23) | NO |
| 6, 80 y | falx | III | Relapse (12 m) + RT | 24.411 | 15 Gy (24–7.3) | NO | Stable (25) | NO |
| 7, 78 y | tubercle | IV | Adjuvant | 0.305 | 14 Gy (28–12.4) | NO | Stable (15 m) | NO |
| 8 | tentorial | IV | Adjuvant | 3.155 | 13 Gy (26–11.5) | NO | Stable (15 m) | NO |
| 9, 80 y | covexity | I | Relapse (34 m) | 1.633 | 15 (30–13.5) | NO | / | / |
| 10, 59 y | Falx | III | Relapse (4 m) | 9.25 | 25 (48.8–19.1) | SI | Distal relapse | ┼ |
| 11, 73 y | Sphenoid ridge | III | Adjuvant | 0.437 | 15 Gy (27.3–13.3) | NO | / | / |
| 12, 73 y | falx | IV | Adjuvant | 4.528 | 15 Gy (30–13.4) | NO | / | / |
| 13, 49 y | Sphenoid ridge | II | Relapse (26 m) +RT | 4.257 | 15 Gy (30–12.3) | NO | Stable | NO |
| 14, 67 y | Falx | IV | relapse | 2.607 | 15 Gy (12.9–28.0) | NO | Distal Relapse | ┼ |
| 15, 71 y | Falx | III | Relapse (30 m) | 4.651 | 15 Gy (30–12.6) | NO | Stable (18) | NO |
| 16, 68 y | Parasaggittal | I | Relapse (48) | 0.350 | 15 Gy (30–12.5) | NO | / | / |
| 17, 67 y | Covexity | I | Relapse (48) | 2.616 | 15 Gy (30.3–12.8) | NO | Local relapse | NO |
| 18, 64 y | Tentorial | III | Relapse (24 m) | 10.069 | 21 Gy (42–17.1) | SI | / | / |
| 19, 63 y | Sphenoid ridge | II | Relapse (22 m) | 2.567 | 15 Gy (30–10.6) | NO | Stable (6 m) | NO |
| 20, 62 y 21 | Covexity Covexity | I I | Relapse (12 m) Relapse (12 m) | 5.355 0.357 | 15 Gy (30–11.3) 15 Gy (30–12.6) | NO NO | Stable stable | ┼ (NSCLC) |
| 22, 68 y | Falx | III | Relapse (21 m) | 3.412 | 15 Gy (29.8–13.1) | NO | stable | NO |
| 23, 74 y | Planum | IV | Adjuvant | 2.239 | 25 Gy (50–20.4) | SI | Stable (24 m) | NO |
| 24, 74 y | Sphenoid ridge | IV | Adjuvant | 3.997 | 25 Gy (46.7–18.4) | SI | Stable (24 m) | NO |
| HR | p Value | |
|---|---|---|
| Volume | 0.76322 | 0.40663 |
| Medium dose | 3.34565 | 0.47343 |
| Maximum dose | 0.89888 | 0.40663 |
| Minimum dose | 0.4864 | 0.47343 |
| Series | N Patients | N Tumors | Volume (cm3) | Marginal Dose (Gy) | Follow Up (Months) | PFS |
|---|---|---|---|---|---|---|
| Stafford [22] | 22 | 22 | 8.2 | 16 | 40 | 68% at 5 y |
| Harris [23] | 18 | 18 | 13.5 | 15 | 28 | 83% at 5 y |
| Huffmann [24] | 15 | 21 | 5 | 16 | 6 | 93% at 6 months |
| Malik [25] | / | 23 | 7.3 | 20 | 44 | 49% at 5 y |
| Kondziolka [26] | 54 | 54 | 7.4 | 14 | 48 | 50% at 2 y |
| Attia [16] | 24 | 24 | 7.9 | 14 | 43 | 25% at 5 y |
| Kim [19] | 35 | 35 | 3.5 | 16 | 29 | 53% at 2 y |
| Pollock [27] | 50 | 71 | 14.6 | 15 | 38 | 40% at 5 y |
| Hanakita [28] | 22 | 28 | 6 | 18 | 23.5 | 20.4% at 5 y |
| Mori [29] | 19 | 22 | 8.6 | 16.5 | 28 | 34% at 3 y |
| Tamura [30] | 9 | 9 | 7.1 | 18.8 | 37 | / |
| Ferraro [31] | 31 | 31 | 3.9 | 18 | 34.5 | 70.1% at 3 y |
| Wang [32] | 46 | 66 | 11.7 | 12.5 | 32.6 | 20.4% at 5 y |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Migliorati, K.; Spatola, G.; Giudice, L.; de Graaf, N.; Bassetti, C.; Giorgi, C.; Fontanella, M.; Vivaldi, O.; Bignardi, M.; Franzin, A. Post Surgical Management of WHO Grade II Meningiomas: Our Experience, the Role of Gamma Knife and a Literature Review. Life 2023, 13, 37. https://doi.org/10.3390/life13010037
Migliorati K, Spatola G, Giudice L, de Graaf N, Bassetti C, Giorgi C, Fontanella M, Vivaldi O, Bignardi M, Franzin A. Post Surgical Management of WHO Grade II Meningiomas: Our Experience, the Role of Gamma Knife and a Literature Review. Life. 2023; 13(1):37. https://doi.org/10.3390/life13010037
Chicago/Turabian StyleMigliorati, Karol, Giorgio Spatola, Lodoviga Giudice, Nine de Graaf, Chiara Bassetti, Cesare Giorgi, Marco Fontanella, Oscar Vivaldi, Mario Bignardi, and Alberto Franzin. 2023. "Post Surgical Management of WHO Grade II Meningiomas: Our Experience, the Role of Gamma Knife and a Literature Review" Life 13, no. 1: 37. https://doi.org/10.3390/life13010037
APA StyleMigliorati, K., Spatola, G., Giudice, L., de Graaf, N., Bassetti, C., Giorgi, C., Fontanella, M., Vivaldi, O., Bignardi, M., & Franzin, A. (2023). Post Surgical Management of WHO Grade II Meningiomas: Our Experience, the Role of Gamma Knife and a Literature Review. Life, 13(1), 37. https://doi.org/10.3390/life13010037