
Heterogeneity in Utilization of Optical Imaging Guided Surgery for Identifying or Preserving the Parathyroid Glands—A Meta-Narrative Review

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
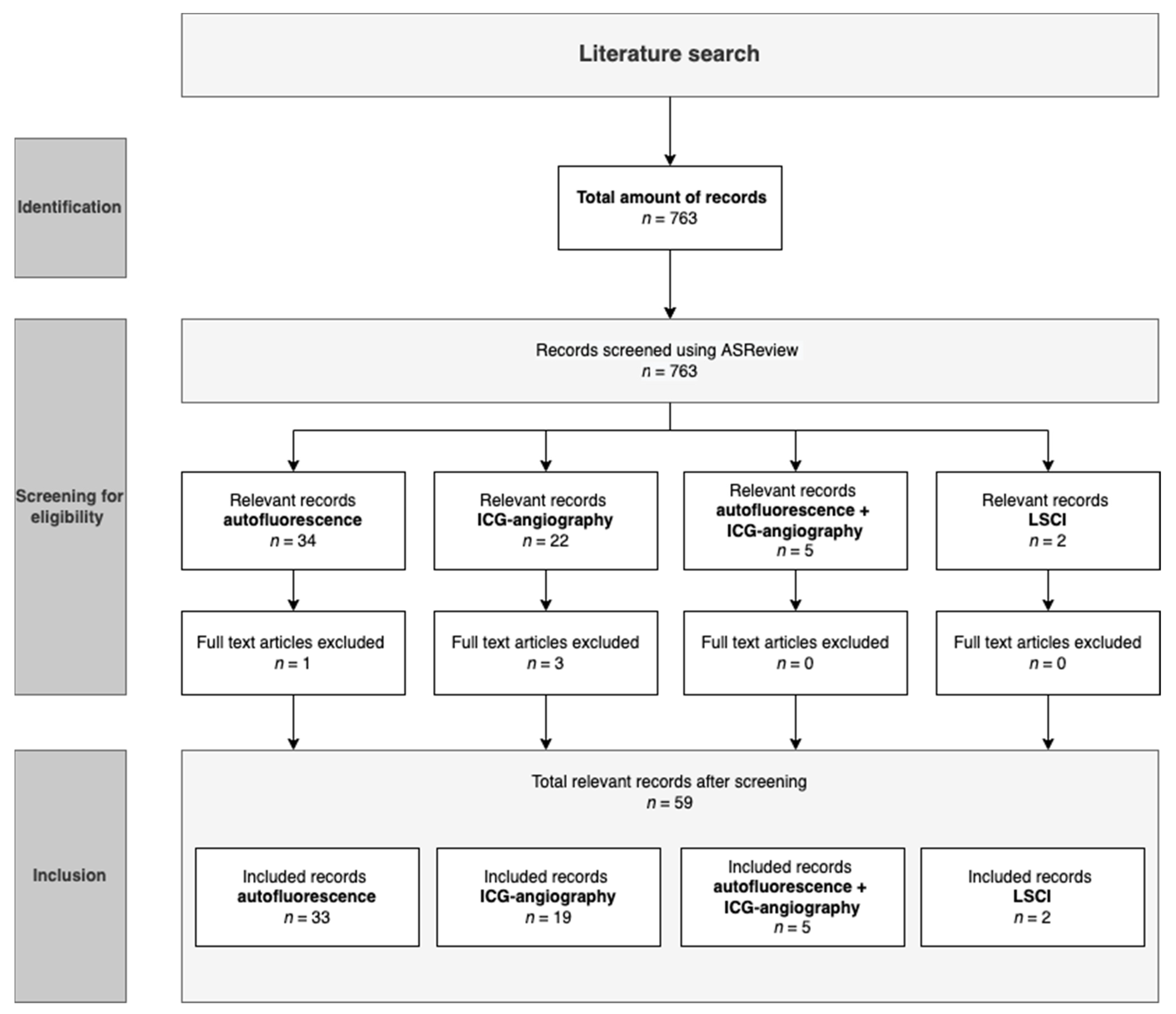
2.2. Search Strategy
2.3. Inclusion Criteria
2.4. Processing of Data
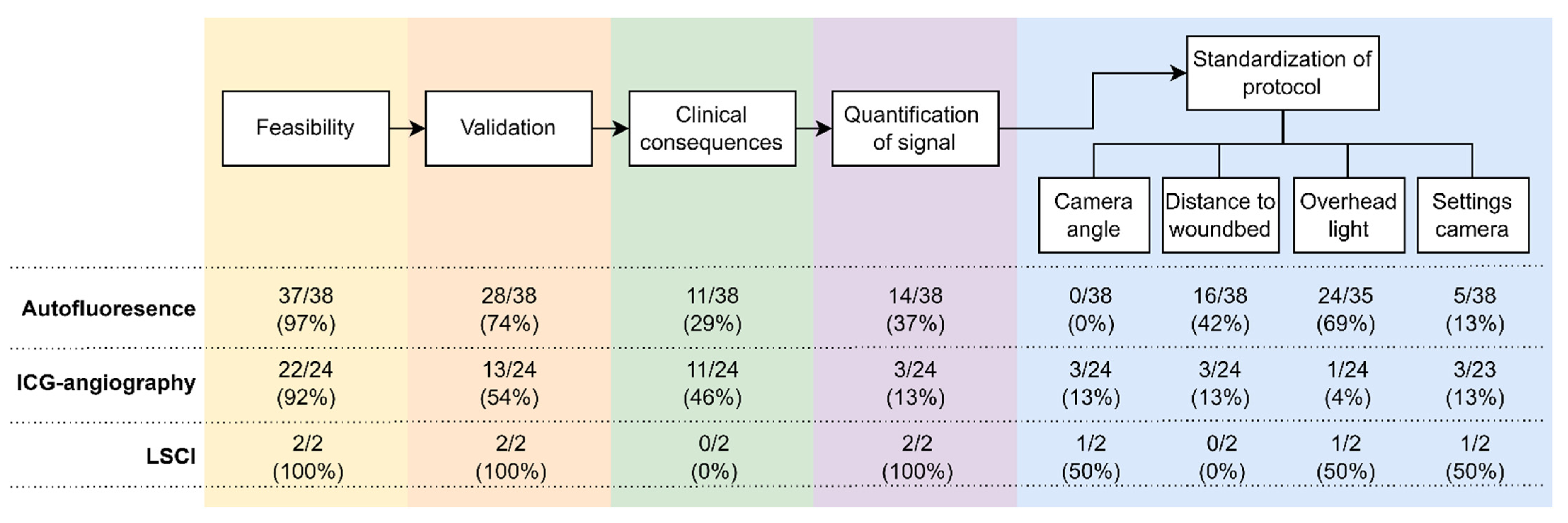
- Feasibility. In this stage, the aim of the study is to examine whether parathyroid glands can be identified or preserved by the technique used.
- Validation of the parathyroid gland’s identification. In this stage, recognition of the parathyroid glands with optical imaging is either validated by the surgeon, based on naked-eye recognition, or by histopathology. Histopathology was considered to be superior to optical recognition.
- Clinical consequences. Clinical choices are made in this stage based on the optical imaging technique that was used.
- Quantification of the fluorescence signal. The images are quantified in real-time or postoperatively at this stage.
- Standardization of the protocol. In this stage, the protocol is clearly standardized so that it could be performed at any location with roughly the same results. For each article, it was noted whether the following parts were named or standardized: camera-to-wound bed distance, camera angle, whether the overhead lights were turned off, and camera settings. Additionally, for ICG-angiography, the following was noted: the injection protocol, whether a video or an image was recorded, and the dose of injected ICG.
3. Results
3.1. Autofluorescence
3.1.1. Selected Articles
3.1.2. Study Population
3.1.3. Study Design
3.1.4. Imaging Technique
3.1.5. Standardization of Protocol
3.1.6. Study Outcomes

{kind=link}
{kind=link}
{kind=link}
| Application | First Author | Origin | Publicated (MM.YY) | Journal | Study Design | Surgery | Sample Size | Imaging Technique | In/Ex Vivo Imaging |
|---|---|---|---|---|---|---|---|---|---|
| AF | Paras [20] | USA | 06.11 | Journal of Biomedical Optics | Prospective cohort | PTx/Tx | 21 | Spectroscopy | In vivo |
| AF | McWade [9] | USA | 12.13 | Surgery | Prospective cohort | Tx | 45 | Spectroscopy | In vivo |
| AF | McWade [22] | USA | 12.14 | Journal of Clinical Endocrinology and Metabolism | Prospective cohort | PTx/Tx | 116 | Spectroscopy and NIR camera (Karl Storz) | In vivo |
| AF | McWade [21] | USA | 01.16 | Surgery | Prospective cohort | PTx/Tx | 137 | Spectroscopy | In vivo |
| AF | Falco [23] | Argentina | 08.16 | Journal of the American College of Surgeons | Prospective cohort | PTx/Tx | 28 | NIR camera (Fluobeam) | In vivo |
| AF | De Leeuw [24] | France | 09.16 | World Journal of Surgery | Prospective cohort | PTx/Tx | 63 | NIR camera (Fluobeam) | In and ex vivo |
| AF | Kim [50] | South Korea | 12.16 | Journal of Clinical Endocrinology and Metabolism | Prospective cohort | Tx | 8 | Digital camera and NIR diode + illuminator | In vivo |
| AF | Shinden [25] | Japan | 06.17 | World Journal of Surgery | Prospective cohort | PTx/Tx | 17 | NIR camera (PDE-Neo) | In and ex vivo |
| AF | Ladurner [54] | Germany | 08.17 | Surgical Endoscopy | Prospective cohort | Laparoscopic PTx/Tx | 30 | Endoscopy NIR camera (Karl Storz) | in vivo |
| AF | Falco [26] | Argentina | 09.17 | Surgical Endoscopy | Retrospective review of prospective data | PTx/Tx | 74 | NIR camera, unknown system | In vivo |
| ICG + AF | Kahramangil [51] | USA | 12.17 | Gland Surgery | Prospective cohort | Tx | 44 | NIR camera (Pinpoint for ICG, Fluobeam for AF) | In vivo |
| AF | Ladurner [55] | Germany | 01.18 | Annals of the Royal College of Surgeons of England | Prospective cohort | Laparoscopic Tx | 20 | Endoscopy NIR camera (Karl Storz) | In vivo |
| AF | Benmiloud [39] | France | 01.18 | Surgery | Non-randomized controlled study | Tx | 513 | NIR camera (Fluobeam) | In vivo |
| AF | Kim [52] | South Korea | 02.18 | Journal of the American College of Surgeons | Prospective cohort | Tx | 38 | Digital camera and NIR diode + illuminator | In vivo |
| ICG + AF | Alesina [27] | Germany | 03.18 | Langenbeck’s Archives of Surgergy | Prospective cohort | PTx/Tx | 5 | Endoscopy NIR camera (Karl Storz) | In vivo |
| AF | Kahramangil [28] | USA | 04.18 | Annals of Surgical Oncology | International multicenter retrospective cohort | PTx/Tx | 210 | NIR camera (Fluobeam) | In vivo |
| AF | Thomas [29] | USA | 11.18 | Thyroid | Prospective cohort | PTx/Tx | 197 | Spectrometer and Pteye | In vivo |
| AF | Thomas [30] | USA | 01.19 | Surgery | Prospective cohort | PTx/Tx | 41 | Pteye and Overlay Tissue Imaging System | In vivo |
| AF | Dip [40] | Argentina | 05.19 | Journal of the American College of Surgeons | RCT | Tx | 170 | NIR camera (Fluobeam) | In vivo |
| ICG + AF | Ladurner [31] | Germany | 07.19 | Molecules | Prospective cohort | PTx/Tx | 117 | Endoscopy NIR camera (Karl Storz) | In vivo |
| AF | Thomas [33] | USA | 09.19 | Journal of the American College of Surgeons | Prospective cohort | PTx/Tx | 20 | NIR camera (PDE-Neo II) vs. PTeye | In and ex vivo |
| ICG + AF | Lerchenberger [32] | Germany | 09.19 | International Journal of Endocrinology | Prospective cohort | PTx/Tx | 50 | Endoscopy NIR camera (Karl Storz) | In vivo |
| AF | DiMarco [47] | UK | 09.19 | Annals of the Royal College of Surgeons of England | Prospective cohort | Tx | 269 | NIR camera (Fluobeam) | In vivo |
| AF | Liu [48] | China | 01.20 | BMC Surgery | Prospective cohort | Tx | 20 | i-Raman Pro NIR camera | In vivo |
| AF | Kose [34] | USA | 01.20 | Surgery (United States) | Prospective cohort | PTx/Tx | 310 | NIR camera (Fluobeam) | In and ex vivo |
| AF | Benmiloud [53] | France | 02.20 | JAMA Surgery | RCT | Tx | 241 | NIR camera (Fluobeam) | In vivo |
| AF | Idogawa [35] | Japan | 05.20 | European Archives of Oto-Rhino- Laryngology | Prospective cohort | PTx/Tx | 45 | NIR camera (PDE-Neo) | In vivo |
| AF | Serra [49] | Portugal | 08.20 | Gland Surgery | Prospective cohort | Tx | 40 | NIR camera (different fabricants) | Ex vivo |
| AF | Takahashi [12] | Japan | 10.20 | Laryngoscope | Prospective cohort | Tx | 36 | NIR camera (PDE-Neo) | In and ex vivo |
| AF | Kim [41] | USA | 10.20 | Journal of Surgical Oncology | Retrospective cohort | Tx | 300 | NIR camera (Fluobeam) | In and ex vivo |
| AF | Papavramidis [42] | Greece | 01.21 | Endocrine | RCT (single-blinded) | Tx | 180 | NIR camera (Fluobeam) | In and ex vivo |
| AF | Akbulut [36] | USA | 03.21 | Journal of Surgical Oncology | Prospective cohort | PTx/Tx | 300 | NIR camera (Fluobeam or Fluobeam LX) | - |
| ICG + AF | Barbieri [43] | Italy | 07.21 | Langenbeck’s Archives of Surgery | Prospective cohort | Tx | 20 | NIR camera (Fluobeam) | In vivo |
| AF | Bellier [44] | France | 07.21 | World Journal of Surgery | Prospective cohort | Tx | 70 | NIR camera (Fluobeam) | Ex vivo |
| AF | van Slycke [45] | Belgium | 08.21 | Surgical Innovation | Prospective cohort | Tx | 40 | NIR camera (Fluobeam) | In and ex vivo |
| AF | Kim [46] | South Korea | 09.21 | Thyroid: official journal of the American Thyroid Association | Retrospective cohort | Tx | 542 | NIR camera, unknown system | In and ex vivo |
| AF | Thomas [37] | USA | 11.21 | American Journal of Surgery | Prospective cohort | PTx/Tx | 167 | PTEye | In vivo |
| AF | Berber [38] | USA | 12.21 | Journal of Surgical Oncology | Retrospective cohort | PTx/Tx | 239 | Unknown device | Ex vivo |
3.2. ICG
3.2.1. Study Population
3.2.2. Study Designs
3.2.3. Imaging Technique
3.2.4. Standardization of Protocol
3.2.5. Study Outcomes
| Application | First Author | Origin | Publicated (MM.YY) | Journal | Study Design | Surgery | Sample Size | Imaging Technique |
|---|---|---|---|---|---|---|---|---|
| ICG | Fortuny [57] | Switzerland | 04.16 | British Journal of Surgery | Prospective cohort | Tx | 36 | Laparoscopy NIR camera (Pinpoint) |
| ICG | Zaidi [58] | USA | 06.16 | Journal of Surgical Oncology | Prospective cohort | Tx | 27 | NIR camera (Pinpoint) |
| ICG | Lang [60] | China | 01.17 | Surgery (United States) | Prospective cohort | Tx | 70 | NIR camera (SPY) |
| ICG | Yu [65] | Korea | 07.17 | Surgical Endoscopy | Prospective cohort | Tx | 66 | NIR camera (da Vinci Si robot system) |
| ICG + AF | Kahra-mangil [51] | USA | 12.17 | Gland Surgery | Prospective cohort | Tx | 44 | Pinpoint for ICG, Fluobeam for AF |
| ICG + AF | Alesina [27] | Germany | 03.18 | Langenbeck’s Archives of Surgery | Prospective cohort | PTx/Tx | 5 | Laparoscopy NIR camera (Karl Storz) |
| ICG | Fortuny [62] | Switzerland | 03.18 | British Journal of Surgery | RCT | Tx | 196 | Laparoscopy NIR camera (Pinpoint) |
| ICG | Jin [59] | China | 12.18 | Advances in Therapy | Prospective cohort | Tx | 26 | Digi-MIH-001 imaging system |
| ICG | van den Bos [70] | Netherlands | 02.-19 | Head and Neck | Prospective cohort | Tx | 26 | Laparoscopy NIR camera (Karl Storz) |
| ICG | Jin [67] | China | 03.19 | Clinical Endocrinology | Prospective cohort | Tx | 26 | Digi-MIH-001 imaging system |
| ICG | Rudin [72] | USA | 06.19 | World Journal of Surgery | Retrospective cohort | Tx | 210 | Laparoscopy NIR camera (Pinpoint) |
| ICG + AF | Ladurner [31] | Germany | 07.19 | Molecules | Retrospective cohort | PTx/Tx | 117 | NIR-endoscope (Karl Storz) |
| ICG | Razavi [74] | USA | 09.19 | Head and Neck | Retrospective cohort | Tx | 43 | NIR-endoscope (Karl Storz) |
| ICG + AF | Lerchenberger [32] | Germany | 09.19 | International Journal of Endocrinology | Prospective cohort | PTx/Tx | 50 | Unknown NIR camera + laparoscopy NIR camera (Olympus) |
| ICG | Gálvez-Pastor [61] | Spain | 11.19 | American Journal of Surgery | Prospective cohort | Tx | 39 | Laparoscopy NIR camera (Pinpoint) |
| ICG | Llorente [64] | Spain | 01.20 | JAMA Surgery | Prospective cohort | Tx | 50 | Unknown |
| ICG | Yavuz [68] | Turkey | 04.20 | Archives of Endocrinology and Metabolism | Prospective cohort | Tx | 43 | NIR camera (SPY) |
| ICG | Papavramidis [73] | Greece | 09.20 | Endocrine Practice | Prospective multicenter | Tx | 60 | NIR camera (OPAL) |
| ICG | Turan [56] | Turkey | 10.20 | Photodiagnosis and Photodynamic Therapy | Retrospective cohort | Tx/PTx | 7 | Laparoscopy NIR camera (Olympus) |
| ICG | Jin [69] | China | 12.20 | Endocrine Practice | RCT | Tx | 56 | Digi-MIH-001 imaging system |
| ICG | Llorente [63] | Spain | 04.21 | Cirugia Espanola | Prospective cohort | Tx | 50 | NIR camera (SPY) |
| ICG | Parfentiev [71] | Georgia | 05.21 | Georgian Med News | RCT | Tx | 58 | Laparoscopy NIR camera (Karl Storz) |
| ICG + AF | Barbieri [43] | Italy | 07.21 | Langenbeck’s Archives of Surgery | Prospective cohort | Tx | 20 | NIR camera (Fluobeam) |
| ICG | Noltes [66] | Netherlands | 12.21 | Annals of Surgery | Prospective multicenter | Tx | 10 | NIR camera (SPY) |
3.3. Laser Speckle Contrast Imaging
3.3.1. Selected Articles and Study Population
3.3.2. Study Design
3.3.3. Imaging Technique
3.3.4. Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lončar, I.; Noltes, M.E.; Dickhoff, C.; Engelsman, A.F.; Schepers, A.; Vriens, M.R.; Bouvy, N.D.; Kruijff, S.; van Ginhoven, T.M. Persistent Postthyroidectomy Hypoparathyroidism in the Netherlands. JAMA Otolaryngol.-Head Neck Surg. 2021, 147, 959–965. [Google Scholar] [CrossRef] [PubMed]
- Edafe, O.; Antakia, R.; Laskar, N.; Uttley, L.; Balasubramanian, S.P. Systematic Review and Meta-Analysis of Predictors of Post-Thyroidectomy Hypocalcaemia. Br. J. Surg. 2014, 101, 307–320. [Google Scholar] [CrossRef] [PubMed]
- Bilezikian, J.P.; Khan, A.; Potts, J.T.; Brandi, M.L.; Clarke, B.L.; Shoback, D.; Jüppner, H.; D’Amour, P.; Fox, J.; Rejnmark, L.; et al. Hypoparathyroidism in the Adult: Epidemiology, Diagnosis, Pathophysiology, Target-Organ Involvement, Treatment, and Challenges for Future Research. J. Bone Miner. Res. 2011, 26, 2317–2337. [Google Scholar] [CrossRef] [PubMed]
- Astor, M.C.; Løvas, K.; Debowska, A.; Eriksen, E.F.; Evang, J.A.; Fossum, C.; Fougner, K.J.; Holte, S.E.; Lima, K.; Moe, R.B.; et al. Epidemiology and Health-Related Quality of Life in Hypoparathyroidism in Norway. J. Clin. Endocrinol. Metab. 2016, 101, 3045–3053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell, D.M.; Regan, S.; Cooley, M.R.; Lauter, K.B.; Vrla, M.C.; Becker, C.B.; Burnett-Bowie, S.A.M.; Mannstadt, M. Long-Term Follow-up of Patients with Hypoparathyroidism. J. Clin. Endocrinol. Metab. 2012, 97, 4507–4514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almquist, M.; Ivarsson, K.; Nordenström, E.; Bergenfelz, A. Mortality in Patients with Permanent Hypoparathyroidism after Total Thyroidectomy. Br. J. Surg. 2018, 105, 1313–1318. [Google Scholar] [CrossRef]
- Dhawan, A.P.; D’Alessandro, B.; Fu, X. Optical Imaging Modalities for Biomedical Applications. IEEE Rev. Biomed. Eng. 2010, 3, 69–92. [Google Scholar] [CrossRef]
- Su, A.; Gong, Y.; Wu, W.; Gong, R.; Li, Z.; Zhu, J. Effect of Autotransplantation of a Parathyroid Gland on Hypoparathyroidism after Total Thyroidectomy. Endocr. Connect. 2018, 7, 286–294. [Google Scholar] [CrossRef] [Green Version]
- McWade, M.A.; Paras, C.; White, L.M.; Phay, J.E.; Mahadevan-Jansen, A.; Broome, J.T. A Novel Optical Approach to Intraoperative Detection of Parathyroid Glands. Surgery 2013, 154, 1371–1377. [Google Scholar] [CrossRef] [Green Version]
- Kose, E.; Kahramangil, B.; Aydin, H.; Donmez, M.; Berber, E. Heterogeneous and Low-Intensity Parathyroid Autofluorescence: Patterns Suggesting Hyperfunction at Parathyroid Exploration. Surgery 2019, 165, 431–437. [Google Scholar] [CrossRef]
- Liu, Z.; Ma, R.; Jia, J.; Wang, T.; Zuo, D.; Yin, D. Evaluation of Autofluorescence in Identifying Parathyroid Glands by Measuring Parathyroid Hormone in Fine-Needle Biopsy Washings. Front. Endocrinol. 2022, 12, 819503. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T.; Yamazaki, K.; Ota, H.; Shodo, R.; Ueki, Y.; Horii, A. Near-Infrared Fluorescence Imaging in the Identification of Parathyroid Glands in Thyroidectomy. Laryngoscope 2021, 131, 1188–1193. [Google Scholar] [CrossRef]
- Cherrick, G.R.; Stein, S.W.; Leevy, C.M.; Davidson, C.S. Indocyanine Green: Observations on Its Physical Properties, Plasma Decay, and Hepatic Extraction. J. Clin. Investig. 1960, 39, 592–600. [Google Scholar] [CrossRef]
- Heeman, W.; Steenbergen, W.; van Dam, G.M.; Boerma, E.C. Clinical Applications of Laser Speckle Contrast Imaging: A Review. J. Biomed. Opt. 2019, 24, 1. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.H.; Lee, S.; Jung, J.; Kim, S.; Kim, S.W.; Hwang, S.H. Near-Infrared Autofluorescence-Based Parathyroid Glands Identification in the Thyroidectomy or Parathyroidectomy: A Systematic Review and Meta-Analysis. Langenbeck’s Arch. Surg. 2021, 406, 1–9. [Google Scholar] [CrossRef]
- Kim, D.H.; Kim, S.W.; Jung, J.; Kim, S.W.; Hwang, S.H. Indocyanine Green Fluorescence for Parathyroid Gland Identification and Function Prediction: Systematic Review and Meta-analysis. Head Neck 2021, 44, 783–791. [Google Scholar] [CrossRef]
- Wong, A.; Wong, J.C.Y.; Pandey, P.U.; Wiseman, S.M. Novel Techniques for Intraoperative Parathyroid Gland Identification: A Comprehensive Review. Expert Rev. Endocrinol. Metab. 2020, 15, 439–457. [Google Scholar] [CrossRef]
- van de Schoot, R.; de Bruin, J.; Schram, R.; Zahedi, P.; de Boer, J.; Weijdema, F.; Kramer, B.; Huijts, M.; Hoogerwerf, M.; Ferdinands, G.; et al. An Open Source Machine Learning Framework for Efficient and Transparent Systematic Reviews. Nat. Mach. Intell. 2021, 3, 125–133. [Google Scholar] [CrossRef]
- Mendeley Ltd. Mendeley: Free Reference Manager and PDF Organizer. Available online: https://www.mendeley.com/ (accessed on 5 March 2022).
- Paras, C.; Keller, M.; White, L.; Phay, J.; Mahadevan-Jansen, A. Near-Infrared Autofluorescence for the Detection of Parathyroid Glands. J. Biomed. Opt. 2011, 16, 067012. [Google Scholar] [CrossRef]
- McWade, M.A.; Sanders, M.E.; Broome, J.T.; Solórzano, C.C.; Mahadevan-Jansen, A. Establishing the Clinical Utility of Autofluorescence Spectroscopy for Parathyroid Detection. Surgery 2016, 159, 193–203. [Google Scholar] [CrossRef] [Green Version]
- McWade, M.A.; Paras, C.; White, L.M.; Phay, J.E.; Solórzano, C.C.; Broome, J.T.; Mahadevan-Jansen, A. Label-Free Intraoperative Parathyroid Localization with near-Infrared Autofluorescence Imaging. J. Clin. Endocrinol. Metab. 2014, 99, 4574–4580. [Google Scholar] [CrossRef] [PubMed]
- Falco, J.; Dip, F.; Quadri, P.; de la Fuente, M.; Rosenthal, R. Cutting Edge in Thyroid Surgery: Autofluorescence of Parathyroid Glands. J. Am. Coll. Surg. 2016, 223, 374–380. [Google Scholar] [CrossRef] [PubMed]
- de Leeuw, F.; Breuskin, I.; Abbaci, M.; Casiraghi, O.; Mirghani, H.; ben Lakhdar, A.; Laplace-Builhé, C.; Hartl, D. Intraoperative Near-Infrared Imaging for Parathyroid Gland Identification by Auto-Fluorescence: A Feasibility Study. World J. Surg. 2016, 40, 2131–2138. [Google Scholar] [CrossRef] [PubMed]
- Shinden, Y.; Nakajo, A.; Arima, H.; Tanoue, K.; Hirata, M.; Kijima, Y.; Maemura, K.; Natsugoe, S. Intraoperative Identification of the Parathyroid Gland with a Fluorescence Detection System. World J. Surg. 2017, 41, 1506–1512. [Google Scholar] [CrossRef]
- Falco, J.; Dip, F.; Quadri, P.; de la Fuente, M.; Prunello, M.; Rosenthal, R.J. Increased Identification of Parathyroid Glands Using near Infrared Light during Thyroid and Parathyroid Surgery. Surg. Endosc. 2017, 31, 3737–3742. [Google Scholar] [CrossRef]
- Alesina, P.F.; Meier, B.; Hinrichs, J.; Mohmand, W.; Walz, M.K. Enhanced Visualization of Parathyroid Glands during Video-Assisted Neck Surgery. Langenbeck’s Arch. Surg. 2018, 403, 395–401. [Google Scholar] [CrossRef]
- Kahramangil, B.; Dip, F.; Benmiloud, F.; Falco, J.; de La Fuente, M.; Verna, S.; Rosenthal, R.; Berber, E. Detection of Parathyroid Autofluorescence Using Near-Infrared Imaging: A Multicenter Analysis of Concordance Between Different Surgeons. Ann. Surg. Oncol. 2018, 25, 957–962. [Google Scholar] [CrossRef]
- Thomas, G.; McWade, M.A.; Paras, C.; Mannoh, E.A.; Sanders, M.E.; White, L.M.; Broome, J.T.; Phay, J.E.; Baregamian, N.; Solórzano, C.C.; et al. Developing a Clinical Prototype to Guide Surgeons for Intraoperative Label-Free Identification of Parathyroid Glands in Real Time. Thyroid 2018, 28, 1517–1531. [Google Scholar] [CrossRef]
- Thomas, G.; McWade, M.A.; Nguyen, J.Q.; Sanders, M.E.; Broome, J.T.; Baregamian, N.; Solórzano, C.C.; Mahadevan-Jansen, A. Innovative Surgical Guidance for Label-Free Real-Time Parathyroid Identification. Surgery 2019, 165, 114–123. [Google Scholar] [CrossRef]
- Ladurner, R.; Lerchenberger, M.; al Arabi, N.; Gallwas, J.K.S.; Stepp, H.; Hallfeldt, K.K.J. Parathyroid Autofluorescence—How Does It Affect Parathyroid and Thyroid Surgery? A 5 Year Experience. Molecules 2019, 24, 2560. [Google Scholar] [CrossRef] [Green Version]
- Lerchenberger, M.; al Arabi, N.; Gallwas, J.K.S.; Stepp, H.; Hallfeldt, K.K.J.; Ladurner, R. Intraoperative Near-Infrared Autofluorescence and Indocyanine Green Imaging to Identify Parathyroid Glands: A Comparison. Int. J. Endocrinol. 2019, 2019, 4687951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, G.; Squires, M.H.; Metcalf, T.; Mahadevan-Jansen, A.; Phay, J.E. Imaging or Fiber Probe-Based Approach? Assessing Different Methods to Detect Near Infrared Autofluorescence for Intraoperative Parathyroid Identification. J. Am. Coll. Surg. 2019, 229, 596–608.e3. [Google Scholar] [CrossRef] [PubMed]
- Kose, E.; Rudin, A.V.; Kahramangil, B.; Moore, E.; Aydin, H.; Donmez, M.; Krishnamurthy, V.; Siperstein, A.; Berber, E. Autofluorescence Imaging of Parathyroid Glands: An Assessment of Potential Indications. Surgery 2020, 167, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Idogawa, H.; Sakashita, T.; Homma, A. A Novel Study for Fluorescence Patterns of the Parathyroid Glands during Surgery Using a Fluorescence Spectroscopy System. Eur. Arch. Oto-Rhino-Laryngol. 2020, 277, 1525–1529. [Google Scholar] [CrossRef] [PubMed]
- Akbulut, S.; Erten, O.; Gokceimam, M.; Kim, Y.S.; Krishnamurthy, V.; Heiden, K.; Jin, J.; Siperstein, A.; Berber, E. Intraoperative Near-Infrared Imaging of Parathyroid Glands: A Comparison of First- and Second-Generation Technologies. J. Surg. Oncol. 2021, 123, 866–871. [Google Scholar] [CrossRef] [PubMed]
- Thomas, G.; Solórzano, C.C.; Baregamian, N.; Mannoh, E.A.; Gautam, R.; Irlmeier, R.T.; Ye, F.; Nelson, J.A.; Long, S.E.; Gauger, P.G.; et al. Comparing Intraoperative Parathyroid Identification Based on Surgeon Experience versus near Infrared Autofluorescence Detection—A Surgeon-Blinded Multi-Centric Study. Am. J. Surg. 2021, 222, 944–951. [Google Scholar] [CrossRef]
- Berber, E.; Akbulut, S. Can Near-Infrared Autofluorescence Imaging Be Used for Intraoperative Confirmation of Parathyroid Tissue? J. Surg. Oncol. 2021, 124, 1008–1013. [Google Scholar] [CrossRef]
- Benmiloud, F.; Rebaudet, S.; Varoquaux, A.; Penaranda, G.; Bannier, M.; Denizot, A. Impact of Autofluorescence-Based Identification of Parathyroids during Total Thyroidectomy on Postoperative Hypocalcemia: A before and after Controlled Study. Surgery 2018, 163, 23–30. [Google Scholar] [CrossRef]
- Dip, F.; Falco, J.; Verna, S.; Prunello, M.; Loccisano, M.; Quadri, P.; White, K.; Rosenthal, R. Randomized Controlled Trial Comparing White Light with Near-Infrared Autofluorescence for Parathyroid Gland Identification during Total Thyroidectomy. J. Am. Coll. Surg. 2019, 228, 744–751. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.S.; Erten, O.; Kahramangil, B.; Aydin, H.; Donmez, M.; Berber, E. The Impact of near Infrared Fluorescence Imaging on Parathyroid Function after Total Thyroidectomy. J. Surg. Oncol. 2020, 122, 973–979. [Google Scholar] [CrossRef]
- Papavramidis, T.S.; Chorti, A.; Tzikos, G.; Anagnostis, P.; Pantelidis, P.; Pliakos, I.; Panidis, S.; Papaioannou, M.; Bakkar, S.; Unal, E.; et al. The Effect of Intraoperative Autofluorescence Monitoring on Unintentional Parathyroid Gland Excision Rates and Postoperative PTH Concentrations—A Single-Blind Randomized-Controlled Trial. Endocrine 2021, 72, 546–552. [Google Scholar] [CrossRef] [PubMed]
- Barbieri, D.; Triponez, F.; Indelicato, P.; Vinciguerra, A.; Trimarchi, M.; Bussi, M. Total Thyroidectomy with Intraoperative Neural Monitoring and Near-Infrared Fluorescence Imaging. Langenbeck’s Arch. Surg. 2021, 1, 3. [Google Scholar] [CrossRef] [PubMed]
- Bellier, A.; Wazne, Y.; Chollier, T.; Sturm, N.; Chaffanjon, P. Spare Parathyroid Glands during Thyroid Surgery with Perioperative Autofluorescence Imaging: A Diagnostic Study. World J. Surg. 2021, 45, 2785–2790. [Google Scholar] [CrossRef] [PubMed]
- Van Slycke, S.; van den Heede, K.; Brusselaers, N.; Vermeersch, H. Feasibility of Autofluorescence for Parathyroid Glands during Thyroid Surgery and the Risk of Hypocalcemia: First Results in Belgium and Review of the Literature. Surg. Innov. 2021, 28, 409–418. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Kim, S.W.; Kang, P.; Choi, J.; Lee, H.S.; Park, S.Y.; Kim, Y.; Ahn, Y.-C.; Lee, K.D. Near-Infrared Autofluorescence Imaging May Reduce Temporary Hypoparathyroidism in Patients Undergoing Total Thyroidectomy and Central Neck Dissection. Thyroid Off. J. Am. Thyroid Assoc. 2021, 31, 1400–1408. [Google Scholar] [CrossRef]
- DiMarco, A.; Chotalia, R.; Bloxham, R.; McIntyre, C.; Tolley, N.; Palazzo, F.F. Does Fluoroscopy Prevent Inadvertent Parathyroidectomy in Thyroid Surgery? Ann. Royal Coll. Surg. Engl. 2019, 101, 508–513. [Google Scholar] [CrossRef]
- Liu, J.; Wang, X.; Wang, R.; Xu, C.; Zhao, R.; Li, H.; Zhang, S.; Yao, X. Near-Infrared Auto-Fluorescence Spectroscopy Combining with Fisher’s Linear Discriminant Analysis Improves Intraoperative Real-Time Identification of Normal Parathyroid in Thyroidectomy. BMC Surg. 2020, 20, 4. [Google Scholar] [CrossRef] [Green Version]
- Serra, C.; Silveira, L.; Canudo, A. Identification of Inadvertently Removed Parathyroid Glands during Thyroid Surgery Using Autofluorescence. Gland Surg. 2020, 9, 893–898. [Google Scholar] [CrossRef]
- Kim, S.W.; Song, S.H.; Lee, H.S.; Noh, W.J.; Oak, C.; Ahn, Y.C.; Lee, K.D. Intraoperative Real-Time Localization of Normal Parathyroid Glands with Autofluorescence Imaging. J. Clin. Endocrinol. Metab. 2016, 101, 4646–4652. [Google Scholar] [CrossRef] [Green Version]
- Kahramangil, B.; Berber, E. Comparison of Indocyanine Green Fluorescence and Parathyroid Autofluorescence Imaging in the Identification of Parathyroid Glands during Thyroidectomy. Gland Surg. 2017, 6, 644–648. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.W.; Lee, H.S.; Ahn, Y.C.; Park, C.W.; Jeon, S.W.; Kim, C.H.; Ko, J.B.; Oak, C.; Kim, Y.; Lee, K.D. Near-Infrared Autofluorescence Image-Guided Parathyroid Gland Mapping in Thyroidectomy. J. Am. Coll. Surg. 2018, 226, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Benmiloud, F.; Godiris-Petit, G.; Gras, R.; Gillot, J.C.; Turrin, N.; Penaranda, G.; Noullet, S.; Chéreau, N.; Gaudart, J.; Chiche, L.; et al. Association of Autofluorescence-Based Detection of the Parathyroid Glands during Total Thyroidectomy with Postoperative Hypocalcemia Risk: Results of the PARAFLUO Multicenter Randomized Clinical Trial. JAMA Surg. 2020, 155, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Ladurner, R.; Sommerey, S.; Arabi, N.A.; Hallfeldt, K.K.J.; Stepp, H.; Gallwas, J.K.S. Intraoperative Near-Infrared Autofluorescence Imaging of Parathyroid Glands. Surg. Endosc. 2017, 31, 3140–3145. [Google Scholar] [CrossRef] [PubMed]
- Ladurner, R.; al Arabi, N.; Guendogar, U.; Hallfeldt, K.K.J.; Stepp, H.; Gallwas, J.K.S. Near-Infrared Autofluorescence Imaging to Detect Parathyroid Glands in Thyroid Surgery. Ann. Royal Coll. Surg. Engl. 2018, 100, 33–36. [Google Scholar] [CrossRef]
- Turan, M.I.; Celik, M.; Ertürk, M.S. Indocyanine Green Fluorescence Angiography-Guided Transoral Endoscopic Thyroidectomy and Parathyroidectomy: First Clinical Report. Photodiagnosis Photodyn. Ther. 2020, 32, 102028. [Google Scholar] [CrossRef]
- Vidal Fortuny, J.; Belfontali, V.; Sadowski, S.M.; Karenovics, W.; Guigard, S.; Triponez, F. Parathyroid Gland Angiography with Indocyanine Green Fluorescence to Predict Parathyroid Function after Thyroid Surgery. Br. J. Surg. 2016, 103, 537–543. [Google Scholar] [CrossRef] [Green Version]
- Zaidi, N.; Bucak, E.; Yazici, P.; Soundararajan, S.; Okoh, A.; Yigitbas, H.; Dural, C.; Berber, E. The Feasibility of Indocyanine Green Fluorescence Imaging for Identifying and Assessing the Perfusion of Parathyroid Glands during Total Thyroidectomy. J. Surg. Oncol. 2016, 113, 775–778. [Google Scholar] [CrossRef]
- Jin, H.; Dong, Q.; He, Z.; Fan, J.; Liao, K.; Cui, M. Application of a Fluorescence Imaging System with Indocyanine Green to Protect the Parathyroid Gland Intraoperatively and to Predict Postoperative Parathyroidism. Adv. Ther. 2018, 35, 2167–2175. [Google Scholar] [CrossRef]
- Lang, B.H.H.; Wong, C.K.H.; Hung, H.T.; Wong, K.P.; Mak, K.L.; Au, K.B. Indocyanine Green Fluorescence Angiography for Quantitative Evaluation of in Situ Parathyroid Gland Perfusion and Function after Total Thyroidectomy. Surgery 2017, 161, 87–95. [Google Scholar] [CrossRef]
- Gálvez-Pastor, S.; Torregrosa, N.M.; Ríos, A.; Febrero, B.; González-Costea, R.; García-López, M.A.; Balsalobre, M.D.; Pastor-Pérez, P.; Moreno, P.; Vázquez-Rojas, J.L.; et al. Prediction of Hypocalcemia after Total Thyroidectomy Using Indocyanine Green Angiography of Parathyroid Glands: A Simple Quantitative Scoring System. Am. J. Surg. 2019, 218, 993–999. [Google Scholar] [CrossRef]
- Vidal Fortuny, J.; Sadowski, S.M.; Belfontali, V.; Guigard, S.; Poncet, A.; Ris, F.; Karenovics, W.; Triponez, F. Randomized Clinical Trial of Intraoperative Parathyroid Gland Angiography with Indocyanine Green Fluorescence Predicting Parathyroid Function after Thyroid Surgery. Br. J. Surg. 2018, 105, 350–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreno Llorente, P.; García Barrasa, A.; Francos Martínez, J.M.; Alberich Prats, M.; Pascua Solé, M. Intraoperative Indocyanine Green (ICG) Angiography of the Parathyroids Glands in Prediction of Post-Thyroidectomy Hypocalcemia: Diagnostic Accuracy of the ICG Score 2 versus the 4-ICG Score. Cirugía Española, 2021; in press. [Google Scholar] [CrossRef]
- Llorente, P.M.; Francos Martínez, J.M.; Barrasa, A.G. Intraoperative Parathyroid Hormone Measurement vs. Indocyanine Green Angiography of Parathyroid Glands in Prediction of Early Postthyroidectomy Hypocalcemia. JAMA Surg. 2020, 155, 84. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.W.; Chung, J.W.; Yi, J.W.; Song, R.Y.; Lee, J.H.; Kwon, H.; Kim, S.J.; Chai, Y.J.; Choi, J.Y.; Lee, K.E. Intraoperative Localization of the Parathyroid Glands with Indocyanine Green and Firefly(R) Technology during BABA Robotic Thyroidectomy. Surg. Endosc. 2017, 31, 3020–3027. [Google Scholar] [CrossRef] [PubMed]
- Noltes, M.E.; Metman, M.J.H.; Heeman, W.; Rotstein, L.; van Ginhoven, T.M.; Vriens, M.R.; Engelsman, A.F.; Boerma, C.E.; Brouwers, A.H.; van Dam, G.M.; et al. A Novel and Generic Workflow of Indocyanine Green Perfusion Assessment Integrating Standardization and Quantification Towards Clinical Implementation. Ann. Surg. 2021, 274, e659–e663. [Google Scholar] [CrossRef]
- Jin, H.; Dong, Q.; He, Z.; Fan, J.; Liao, K.; Cui, M. Research on Indocyanine Green Angiography for Predicting Postoperative Hypoparathyroidism. Clin. Endocrinol. 2019, 90, 487–493. [Google Scholar] [CrossRef]
- Yavuz, E.; Biricik, A.; Karagulle, O.O.; Ercetin, C.; Arici, S.; Yigitbas, H.; Meric, S.; Solmaz, A.; Celik, A.; Gulcicek, O.B. A Comparison of the Quantitative Evaluation of in Situ Parathyroid Gland Perfusion by Indocyanine Green Fluorescence Angiography and by Visual Examination in Thyroid Surgery. Arch. Endocrinol. Metab. 2020, 64, 427–435. [Google Scholar] [CrossRef]
- Jin, H.; Cui, M. Research on Intra-Operative Indocyanine Green Angiography of the Parathyroid for Predicting Postoperative Hypoparathyroidism: A Noninferior Randomized Controlled Trial. Endocr. Pract. 2020, 26, 1469–1476. [Google Scholar] [CrossRef]
- van den Bos, J.; van Kooten, L.; Engelen, S.M.E.; Lubbers, T.; Stassen, L.P.S.; Bouvy, N.D. Feasibility of Indocyanine Green Fluorescence Imaging for Intraoperative Identification of Parathyroid Glands during Thyroid Surgery. Head Neck 2019, 41, 340–348. [Google Scholar] [CrossRef]
- Parfentiev, R.; Grubnik, V.; Bugridze, Z.; Giuashvili, S.; Beselia, L. Study of Intraoperative Indocyanine Green Angiography Effectiveness for Identification of Parathyroid Glands during Total Thyroidectomy. Georgian Med. News 2021, 314, 26–29. [Google Scholar]
- Rudin, A.V.; McKenzie, T.J.; Thompson, G.B.; Farley, D.R.; Lyden, M.L. Evaluation of Parathyroid Glands with Indocyanine Green Fluorescence Angiography After Thyroidectomy. World J. Surg. 2019, 43, 1538–1543. [Google Scholar] [CrossRef]
- Papavramidis, T.S.; Anagnostis, P.; Chorti, A.; Pliakos, I.; Panidis, S.; Koutsoumparis, D.; Michalopoulos, A. Do Near-Infrared Intra-Operative Findings Obtained Using Indocyanine Green Correlate with Post-Thyroidectomy Parathyroid Function? The Icgpredict Study. Endocr. Pract. 2020, 26, 967–973. [Google Scholar] [CrossRef] [PubMed]
- Razavi, A.C.; Ibraheem, K.; Haddad, A.; Saparova, L.; Shalaby, H.; Abdelgawad, M.; Kandil, E. Efficacy of Indocyanine Green Fluorescence in Predicting Parathyroid Vascularization during Thyroid Surgery. Head Neck 2019, 41, 3276–3281. [Google Scholar] [CrossRef] [PubMed]
- Mannoh, E.A.; Thomas, G.; Solórzano, C.C.; Mahadevan-Jansen, A. Intraoperative Assessment of Parathyroid Viability Using Laser Speckle Contrast Imaging. Sci. Rep. 2017, 7, 14798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mannoh, E.A.; Thomas, G.; Baregamian, N.; Rohde, S.L.; Solórzano, C.C.; Mahadevan-Jansen, A. Assessing Intraoperative Laser Speckle Contrast Imaging of Parathyroid Glands in Relation to Total Thyroidectomy Patient Outcomes. Thyroid 2021, 31, 1558–1565. [Google Scholar] [CrossRef]
- Fleischmann, D.; Kamaya, A. Optimal Vascular and Parenchymal Contrast Enhancement: The Current State of the Art. Radiol. Clin. N. Am. 2009, 47, 13–26. [Google Scholar] [CrossRef]
- Mannoh, E.A.; Parker, L.B.; Thomas, G.; Solórzano, C.C.; Mahadevan-Jansen, A. Development of an Imaging Device for Label-free Parathyroid Gland Identification and Vascularity Assessment. J. Biophotonics 2021, 14, e202100008. [Google Scholar] [CrossRef]
- Solórzano, C.C.; Thomas, G.; Berber, E.; Wang, T.S.; Randolph, G.W.; Duh, Q.Y.; Triponez, F. Current State of Intraoperative Use of near Infrared Fluorescence for Parathyroid Identification and Preservation. Surgery 2021, 169, 868–878. [Google Scholar] [CrossRef]
- Kahramangil, B.; Berber, E. The Use of Near-Infrared Fluorescence Imaging in Endocrine Surgical Procedures. J. Surg. Oncol. 2017, 115, 848–855. [Google Scholar] [CrossRef]
- Demarchi, M.S.; Karenovics, W.; Bédat, B.; Triponez, F. Intraoperative Autofluorescence and Indocyanine Green Angiography for the Detection and Preservation of Parathyroid Glands. J. Clin. Med. 2020, 9, 830. [Google Scholar] [CrossRef] [Green Version]
- Spartalis, E.; Ntokos, G.; Georgiou, K.; Zografos, G.; Tsourouflis, G.; Dimitroulis, D.; Nikiteas, N.I. Intraoperative Indocyanine Green (ICG) Angiography for the Identification of the Parathyroid Glands: Current Evidence and Future Perspectives. In Vivo 2020, 34, 23–32. [Google Scholar] [CrossRef]
- Goncalves, L.N.; van den Hoven, P.; van Schaik, J.; Leeuwenburgh, L.; Hendricks, C.H.F.; Verduijn, P.S.; van der Bogt, K.E.A.; van Rijswijk, C.S.P.; Schepers, A.; Vahrmeijer, A.L.; et al. Perfusion Parameters in Near-Infrared Fluorescence Imaging with Indocyanine Green: A Systematic Review of the Literature. Life 2021, 11, 433. [Google Scholar] [CrossRef] [PubMed]
- Lütken, C.D.; Achiam, M.P.; Svendsen, M.B.; Boni, L.; Nerup, N. Optimizing Quantitative Fluorescence Angiography for Visceral Perfusion Assessment. Surg. Endosc. 2020, 34, 5223–5233. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, A.J.; Wu, M.; LaRochelle, E.P.M.; Gorpas, D.; Ntziachristos, V.; Pfefer, T.J.; Pogue, B.W. Indocyanine Green Matching Phantom for Fluorescence-Guided Surgery Imaging System Characterization and Performance Assessment. J. Biomed. Opt. 2020, 25, 056003. [Google Scholar] [CrossRef] [PubMed]
- di Marco, A.N.; Palazzo, F.F. Near-Infrared Autofluorescence in Thyroid and Parathyroid Surgery. Gland Surg. 2020, 9, S136–S146. [Google Scholar] [CrossRef]



| Application | First Author | Origin | Publicated (MM.YY) | Journal | Study Design | Surgery | Sample Size | Imaging Technique |
|---|---|---|---|---|---|---|---|---|
| LSCI | Mannoh [75] | USA | 11.17 | Scientific Reports | Prospective cohort | PTx/Tx | 7 | LSCI device |
| LSCI | Mannoh [76] | USA | 10.21 | Thyroid | Prospective cohort | Tx | 72 | LSCI device |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feitsma, E.A.; Schouw, H.M.; Noltes, M.E.; Heeman, W.; Kelder, W.; van Dam, G.M.; Kruijff, S. Heterogeneity in Utilization of Optical Imaging Guided Surgery for Identifying or Preserving the Parathyroid Glands—A Meta-Narrative Review. Life 2022, 12, 388. https://doi.org/10.3390/life12030388
Feitsma EA, Schouw HM, Noltes ME, Heeman W, Kelder W, van Dam GM, Kruijff S. Heterogeneity in Utilization of Optical Imaging Guided Surgery for Identifying or Preserving the Parathyroid Glands—A Meta-Narrative Review. Life. 2022; 12(3):388. https://doi.org/10.3390/life12030388
Chicago/Turabian StyleFeitsma, Eline A., Hugo M. Schouw, Milou E. Noltes, Wido Heeman, Wendy Kelder, Gooitzen M. van Dam, and Schelto Kruijff. 2022. "Heterogeneity in Utilization of Optical Imaging Guided Surgery for Identifying or Preserving the Parathyroid Glands—A Meta-Narrative Review" Life 12, no. 3: 388. https://doi.org/10.3390/life12030388
APA StyleFeitsma, E. A., Schouw, H. M., Noltes, M. E., Heeman, W., Kelder, W., van Dam, G. M., & Kruijff, S. (2022). Heterogeneity in Utilization of Optical Imaging Guided Surgery for Identifying or Preserving the Parathyroid Glands—A Meta-Narrative Review. Life, 12(3), 388. https://doi.org/10.3390/life12030388