
Near-Infrared Fluorescence Tumor-Targeted Imaging in Lung Cancer: A Systematic Review

 , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results and Discussion
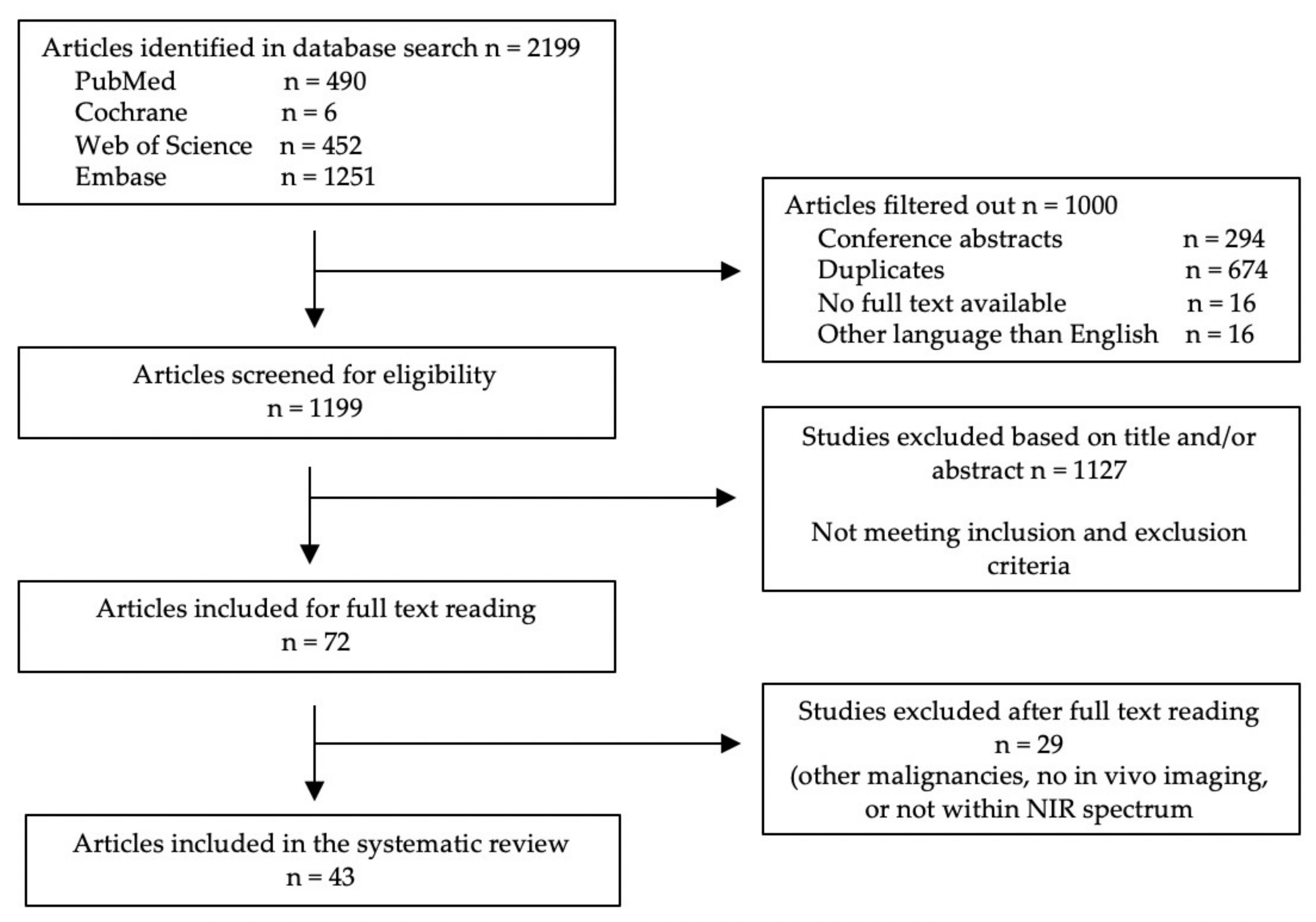
3.1. Literature Search
3.2. Preclinical Studies
3.2.1. Non-Specific Fluorophores
3.2.2. Antibodies
3.2.3. Nanoparticles
3.2.4. Generated Probes
3.2.5. Activatable Probes
3.2.6. Integrin-Targeting Probes
3.2.7. Others

{kind=link}
{kind=link}
{kind=link}
| Fluorescent Probe | Study Population | Doses | Time Interval | Control Group | Results | Toxicity | Ref |
|---|---|---|---|---|---|---|---|
| Non-specific fluorophores | |||||||
| MHI-148 | A549 mice (n = 5 per time interval) | 1.5 nmol IV | 1, 2, 6, 24, 48, 72, 96 and 120 h | Mice not injected with the probe (n = NR) | Tumors start showing fluorescence one hour after injection and reached a peak TBR of 3.62 after 24 h, which remains constant up to 72 h. Control mice did not show fluorescence at the tumor site. | Low cytotoxicity | [36] |
| IR-780 iodide | Chemically induced mouse models (n = NR) | 0.2 mg/kg IV | 14 d | NA | Tumors were detectable with fluorescence imaging. Histological examination confirmed that IR0780 iodide was specifically accumulated in the tumor cells. | NR | [37] |
| 5-ALA | LKR or A549 mouse models (n = 3 per doses) | 0, 10, 20, 40 or 100 mg/kg oral | 1–8 h | NA | In the three highest doses groups fluorescence signals were detectable, with a comparable peak TBR (around 5) 1 hour after administration. The fluorescence intensities in the two highest groups were associated with higher TBRs at later time points. | Nausea | [38] |
| Dogs with primary lung cancer (n = 7) | 20 mg/kg oral | 2–4 h | 6 of 7 cancers were detectable with fluorescence imaging with a median TBR of 2.1. Tumor margins were detectable in two dogs, the others tumors had an unreliable fluorescence pattern. No additional lesions were found. | ||||
| Antibodies | |||||||
| NIR-PD-L1-mAB | NCI-H2444 mouse models (PD-L1+) (n = 3–5) | 22 μg IV | 24, 48, 72, 96 and 120 h | NCI-H1155 (PD-L1 -) mouse models (n = 3–5) | The tumor was detectable after 72 h and was best identified after 120 h. Specific fluorescent uptake in the tumor was higher compared to the control group. | NR | [42] |
| Cy5.5 – mAb109 | A549 mouse models (n = 4) | 0.2 nmol IV | 2, 24, 48 h and 5, 7, 9, 16 d | Mice injected with 0.5 nmol Cy5.5-ICG or co-injected with 500 μg unlabeled mAb109 (n = 4 per group) | Tumors were detectable from 24 h up to 16 days after the administration. The highest tumor to normal tissue ratio was reached after 24 h and was 3.2. Tumor to normal ratios were much lower in the control groups. Fluorescence imaging corresponded to bioluminescence images of co-implanted Luci cells in the tumor. | NR | [43] |
| h173-Cy5.5 | A549 mouse models (n = 5) | 30 μg IV | 6 h, and 1, 2, 3, 4, 7 d | Mice injected with hIgG-Cy5.5 or mice with Axl negative tumors (H249 cells) injected with h173-Cy5.5 or hIgG-Cy5.5 (n = 5 per group) | Tumors were best detectable with fluorescence imaging 2–3 days after administration. The fluorescence intensity was significantly higher compared to the control groups. | NR | [44] |
| Nanoparticles | |||||||
| Anti-EGFR/MB-SHSi | A549 mouse models (n = NR) | NR IV | 1, 3, 6 h | Mice injected with non-targeted MB-SHSi (n = NR) | The tumor was detectable after 1 h and fluorescence intensities were strongest after 6 h. Fluorescence signals were higher compared to the control group. | Negligible cytotoxicity | [45] |
| Cy5.5-CNPs ICG-CNPs | VX2 mouse models (n = 3) | 22.5 mg/kg IV | Up to 96 h | NA | The tumors in the Cy5.5-CNPs group were detectable after 24 h and maximum fluorescence intensities were measured in the tumor between 48 and 96 h. Tumors in the ICG-CNPs group were detectable for up to 96 h. | No cytotoxicity | [46] |
| ICG-CNPs | VX2 rabbit models (n = 3) | 22.5 mg/kg IV | Up to 96 h | Rabbits injected with 2 mg/kg free ICG | Tumors were detectable with fluorescence imaging up to 96 h after injection, with maximum fluorescence intensities after 48 h. Tumor margins were clearly visible. In the control group only 30 min after injection a minimal fluorescence signal was detectable. | No cytotoxicity | [46] |
| rHDL/MB-CCPs | A549 mouse models (n = NR) | NR IV | 2, 4, and 6 h | Mice injected with lipos/MB-CCPs (n = NR) | The tumor was detectable after 2 h and fluorescence signals were highest after 6 h. Fluorescence intensities were higher and tumor targeting was more specific compared to the control group | No significant cytotoxicity | [47] |
| FA–PEG– SPIONs–Cy5.5 | Urethane mouse models (n = 5) | 5 mg/kg IV | 6 and 24 h | Mice injected with non-targeted PEG–SPIONs–Cy5.5 (n = 5) | Fluorescence signals in the lung were higher compared to the control group at both time intervals. | Cy5.5 in high concentration is cytotoxic. | [48] |
| Generated probes | |||||||
| Cy5-S6 | A549 mouse models (n = NR) | 0.5 nmol IV | 5 min and 3, 5 h | Mice injected with control probe Cy5-Lib and mice contralateral injected with Tca8113 tongue carcinoma (n = NR) | Tumors showed fluorescence after five minutes to five hours after the administration. The greatest signal was seen three hours after the injection. Control groups showed limited to no fluorescence uptake at the tumor sites. | NR | [49] |
| Cy5.5-labeled Pep-1 | A549 mouse models (n = 3) | NR IV | 1–11 d | Mice receiving a different phage, free Cy5.5 or mice with different tumor types receiving Cy5.5-labeled Pep-1 (n = 3 per group) | On the 11th-day, high fluorescence signals were detectable in the tumor. Histological examination showed that Pep-1 was strongly detected in tumor tissue. No to minimal fluorescent signals were seen in control groups | NR | [50] |
| Activatable probes | |||||||
| 6QCNIR | KPT mice infected with Lenti-Cre virus (n = NR) | 20 nmol IV | 6 h | Healthy mice injected with the probe (n = NR) | Tumors were detectable with high contrast between tumor and normal tissue. Additional tumor lesions were detectable. Histological examination showed that all fluorescent tissue was malignant. Control mice showed only background fluorescence. | NR | [51] |
| Prosense 680 Prosense 750 | LLC mouse models (n = 5 per probe) | 2 nmol IV | 24 h | Mice not injected with the probe (n = 5) | TBRs of the Prosense 680 and 750 groups were 9.3 and 8.5, respectively. Histological examination showed specific fluorescence uptake in the tumor center, but even higher fluorescence signals in the tumor periphery and immediately adjacent lung parenchyma to this. Lung parenchyma at macroscopic distance from the tumor showed very low fluorescence. TBR in the control was around 1. | Probes appear to be safe | [52] |
| DEATH-CAT-FNIR | krasG12D/+p53−/− adenocarcinoma mouse models (n = NR) | 20 nmol IV | 16 h | NA | Tumors as small as 1 mm were visible with fluorescence imaging. Histological examination showed that only malignant cells showed fluorescence. | NR | [53] |
| HSA-CAPN2 | A549 mouse models (n = 5) | 125 μg IV | 1, 2, 4, 9, and 18 h | Mice injected with HSA–Cy5, CAPN2, or HSA-CAPN2 after IT injection of ALLN, a CAPN2 inhibitor (n = 5 per group) | Tumors were detectable after two hours and fluorescence signals in the tumor were the highest four hours after administration of the probe. Fluorescence signals were significantly higher than in all three control groups. Fluorescence imaging corresponded to bioluminescence images of co-implanted Luc cells in the tumor. | NR | [54] |
| Q-cetuximab | A549 mouse models (n = 3) | 50 μg IV | 8 h | Mice injected with 50 μg ON-Cetuximab or 100 μL PBS (n = 3 per group) | The TBRs in the Q-cetuximab, ON-Cetuximab, and PBS groups were 4.28 ± 1.13, 1.48 ± 0.06, and 1.14 ± 0.08, respectively. Fluorescence imaging corresponded to bioluminescence images of co-implanted Lu2 cells in the tumor. | NR | [55] |
| NIR-ASM | A549 mouse models (n = NR) | 5 mg/kg IV | 5, 10, 20, 30 min | Mice were contralaterally injected with MDA-MB-231 cells (NQO1 negative) (n = NR) | Fluorescence signals were detectable in tumors in both mouse models and were the highest 30 min after injection. No fluorescence signals were detectable in NQO1 negative tumors or healthy mice. | No toxicity | [56] |
| LLC mouse models (n = NR) | Healthy mice injected with the probe (n = NR) | ||||||
| pH-AAP | A549 mouse models (n = NR) | 0.24 nmol IT | 2 to 300 min | A549 tumor-bearing mice injected with pH-ALP or SMMC-7721 tumor-bearing mice injected with pH-AAP (n = NR) | The tumors were detectable after 2 min and fluorescence signals were the highest after 120 min. There was a limited background signal. The new probe, pH-AAP, showed less background signal as compared with the previous probe Cy5-S6. Control groups with either a negative control probe or different tumor type showed limited to no fluorescence uptake at the tumor sites. | NR | [57] |
| Integrin-targeting probes | |||||||
| Cyp-GRD | A549 mouse models (n = NR) | 0.3 μmol/kg IV | 2, 8, and 24 h | Mice injected with linear or cyclic RGD conjugated to cypate (n = NR) | Tumor-specific fluorescence uptake was seen 8 h after injection and the tumor was best detectable with fluorescence imaging after 24 h. The fluorescence signals were higher compared to the control groups. | No cytotoxicity | [58] |
| cRGDfK-targeted probe | A549 mouse models (n = 8) | 5 nmol IV | 90 and 180 min | Mice injected with an untargeted probe (n = 8) | The tumors were detectable at both time intervals with comparable fluorescence intensities. The average tumor-to-muscle ratio was 3.6. In the control group, there was only minimal fluorescence visible at the tumor site. | Low phototoxicity | [59] |
| LXY30 | H3255 and PDX human lung squamous cell carcinoma mouse models (n = NR) | 1.8 nmol IV | 6 h | Mice injected with untargeted biotin/streptavidin-Cy5.5 complex (n = NR) | Fluorescence signals were detectable in the tumor in both H3255 and PDX mice. Histopathological examination showed that the probe was specifically taken up in the tumor. Fluorescence signals were higher as compared with the control group. | NR | [60] |
| Endostatin-Cy5.5 | LLC mouse models (n = 3) | 20 mg/kg IV or IP | 1–168 h | Mice injected with alone endostatin or Cy.5.5 and mice not injected at all (n = 3 per group) | Tumors were detectable with fluorescence imaging from 18 to 114 h after intraper injection. The maximum fluorescence intensity was reached after 42 h. After intraveintravenous injection, fluorescence intensity reached the maximum after 3 h and fluorescence signals were detectable up to 72 h. Control groups did not show tumor-specific fluorescence uptake. | NR | [61] |
| Others | |||||||
| HyA-AT-Alexa680 | A549 mouse models (n = 5) | 5 mg/kg IV | 5 min and 1, 8, 24, and 48 h | Mice injected with native Hya – Alexa680 (n = 5) | Till 1 hour after injection, high background signals were detected. After 8 h the tumor was best detectable. The residence time in the tumor was shorter in the control group. | Cytotoxic at incubation time of 72 h and 1 mg/ml nanogel concentration | [62] |
| Dmt-Tic-IR800 | DMS-53 (δOR+) mouse models (n = 4) | 40 nmol/kg IV | 24 h | Mice were contralaterally injected with H1299 (δOR-) cells | The tumors were detectable with fluorescence imaging and had significantly more fluorescent uptake compared to the δOR negative control tumors. | NR | [63] |
| RA-IRDye800CW | A549 mouse models (n = 10) | 10 nmol IV | 1–9 d | NA | The highest fluorescent signals were detected after 72 h. The TBR was 2.15. | Cytotoxicity at doses higher than saturation dose 0.1/mg/kg/week | [64] |
3.3. Clinical Studies
3.3.1. ICG
3.3.2. OTL38
3.4. Metastases
4. Future Perspectives
4.1. Clinical Trials
4.2. Photoacoustic Imaging
4.3. NIR-II Window
4.4. Quantification
4.5. Combination with Targeted Drug Delivery
4.6. Image-Guided Surgery Combined with Photodynamic Therapy
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Search Strategy per Database
- PubMed:
- Cochrane:
- Web of Science:
- Embase:
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemjabbar-Alaoui, H.; Hassan, O.U.; Yang, Y.-W.; Buchanan, P. Lung cancer: Biology and treatment options. Biochim. Biophys. Acta BBA Rev. Cancer 2015, 1856, 189–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snijder, R.J.; de la Rivière, A.B.; Elbers, H.J.; Bosch, J.M.V.D. Survival in Resected Stage I Lung Cancer with Residual Tumor at the Bronchial Resection Margin. Ann. Thorac. Surg. 1998, 65, 212–216. [Google Scholar] [CrossRef]
- Riquet, M.; Achour, K.; Foucault, C.; Barthes, F.L.P.; Dujon, A.; Cazes, A. Microscopic Residual Disease after Resection for Lung Cancer: A Multifaceted but Poor Factor of Prognosis. Ann. Thorac. Surg. 2010, 89, 870–875. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, H.; Taege, C.; Lautenschläger, C.; Neef, H.; Silber, R. Microscopic (R1) and macroscopic (R2) residual disease in patients with resected non-small cell lung cancer. Eur. J. Cardio-Thoracic Surg. 2002, 21, 606–610. [Google Scholar] [CrossRef] [Green Version]
- Şahin, M.; Yenigün, M.B.; Kocaman, G.; Duman, E.; Sakallı, M.A.; Özkan, M.; Yüksel, C.; Cangır, A.K.; Kutlay, H.; Akal, M.; et al. Sublobar resections in early-stage non-small cell lung cancer. Turk. J. Thorac. Cardiovasc. Surg. 2019, 27, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Scott, W.J.; Allen, M.S.; Darling, G.; Meyers, B.; Decker, P.A.; Putnam, J.B.; Mckenna, R.W.; Landrenau, R.J.; Jones, D.R.; Inculet, R.I.; et al. Video-assisted thoracic surgery versus open lobectomy for lung cancer: A secondary analysis of data from the American College of Surgeons Oncology Group Z0030 randomized clinical trial. J. Thorac. Cardiovasc. Surg. 2010, 139, 976–983. [Google Scholar] [CrossRef] [Green Version]
- De Koning, H.J.; van der Aalst, C.M.; de Jong, P.A.; Scholten, E.T.; Nackaerts, K.; Heuvelmans, M.A.; Lammers, J.-W.J.; Weenink, C.; Yousaf-Khan, U.; Horeweg, N.; et al. Reduced Lung-Cancer Mortality with Volume CT Screening in a Randomized Trial. N. Engl. J. Med. 2020, 382, 503–513. [Google Scholar] [CrossRef] [PubMed]
- Bedetti, B.; Bertolaccini, L.; Rocco, R.; Schmidt, J.; Solli, P.; Scarci, M. Segmentectomy versus lobectomy for stage I non-small cell lung cancer: A systematic review and meta-analysis. J. Thorac. Dis. 2017, 9, 1615–1623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ichinose, J.; Kohno, T.; Fujimori, S.; Harano, T.; Suzuki, S. Efficacy and Complications of Computed Tomography-Guided Hook Wire Localization. Ann. Thorac. Surg. 2013, 96, 1203–1208. [Google Scholar] [CrossRef] [PubMed]
- Mayo, J.R.; Clifton, J.C.; Powell, T.I.; English, J.C.; Evans, K.G.; Yee, J.; McWilliams, A.M.; Lam, S.C.; Finley, R.J. Lung Nodules: CT-guided Placement of Microcoils to Direct Video-assisted Thoracoscopic Surgical Resection. Radiology 2009, 250, 576–585. [Google Scholar] [CrossRef] [PubMed]
- Sancheti, M.S.; Lee, R.; Ahmed, S.U.; Pickens, A.; Fernandez, F.G.; Small, W.C.; Nour, S.G.; Force, S.D. Percutaneous Fiducial Localization for Thoracoscopic Wedge Resection of Small Pulmonary Nodules. Ann. Thorac. Surg. 2014, 97, 1914–1919. [Google Scholar] [CrossRef] [PubMed]
- Bellomi, M.; Veronesi, G.; Trifirò, G.; Brambilla, S.; Bonello, L.; Preda, L.; Casiraghi, M.; Borri, A.; Paganelli, G.; Spaggiari, L. Computed Tomography-Guided Preoperative Radiotracer Localization of Nonpalpable Lung Nodules. Ann. Thorac. Surg. 2010, 90, 1759–1764. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, K.-I.; Nomori, H.; Ohtsuka, T.; Kaji, M.; Naruke, T.; Suemasu, K. Usefulness and complications of computed tomography-guided lipiodol marking for fluoroscopy-assisted thoracoscopic resection of small pulmonary nodules: Experience with 174 nodules. J. Thorac. Cardiovasc. Surg. 2006, 132, 320–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchevsky, A.M.; Changsri, C.; Gupta, I.; Fuller, C.; Houck, W.; McKenna, R.J. Frozen Section Diagnoses of Small Pulmonary Nodules: Accuracy and Clinical Implications. Ann. Thorac. Surg. 2004, 78, 1755–1759. [Google Scholar] [CrossRef]
- Gephardt, G.N.; Zarbo, R.J. Interinstitutional comparison of frozen section consultations. A college of American Pathologists Q-Probes study of 90,538 cases in 461 institutions. Arch. Pathol. Lab. Med. 1996, 120, 804–809. [Google Scholar]
- Kondo, R.; Yoshida, K.; Hamanaka, K.; Hashizume, M.; Ushiyama, T.; Hyogotani, A.; Kurai, M.; Kawakami, S.; Fukushima, M.; Amano, J. Intraoperative ultrasonographic localization of pulmonary ground-glass opacities. J. Thorac. Cardiovasc. Surg. 2009, 138, 837–842. [Google Scholar] [CrossRef] [Green Version]
- Chance, B. Near-Infrared Images Using Continuous, Phase-Modulated, and Pulsed Light with Quantitation of Blood and Blood Oxygenationa. Ann. N. Y. Acad. Sci. 1998, 838, 29–45. [Google Scholar] [CrossRef]
- Keereweer, S.; van Driel, P.B.A.A.; Snoeks, T.J.A.; Kerrebijn, J.D.F.; de Jong, R.J.B.; Vahrmeijer, A.L.; Sterenborg, H.J.C.M.; Löwik, C.W.G.M. Optical Image-Guided Cancer Surgery: Challenges and Limitations. Clin. Cancer Res. 2013, 19, 3745–3754. [Google Scholar] [CrossRef] [Green Version]
- Ishizawa, T.; Fukushima, N.; Shibahara, J.; Masuda, K.; Tamura, S.; Aoki, T.; Hasegawa, K.; Beck, Y.; Fukayama, M.; Kokudo, N. Real-time identification of liver cancers by using indocyanine green fluorescent imaging. Cancer 2009, 115, 2491–2504. [Google Scholar] [CrossRef]
- Ishizuka, M.; Kubota, K.; Kita, J.; Shimoda, M.; Kato, M.; Sawada, T. Intraoperative Observation Using a Fluorescence Imaging Instrument during Hepatic Resection for Liver Metastasis from Colorectal Cancer. Hepatogastroenterology 2011, 59, 90–92. [Google Scholar] [CrossRef] [PubMed]
- Van Dam, G.M.; Themelis, G.; Crane, L.M.; Harlaar, N.J.; Pleijhuis, R.G.; Kelder, W.; Sarantopoulos, A.; de Jong, J.S.; Arts, H.J.; van der Zee, A.G.; et al. Intraoperative tumor-specific fluorescence imaging in ovarian cancer by folate receptor-α targeting: First in-human results. Nat. Med. 2011, 17, 1315–1319. [Google Scholar] [CrossRef] [PubMed]
- Keating, J.; Tchou, J.; Okusanya, O.; Fisher, C.; Batiste, R.; Jiang, J.; Kennedy, G.; Nie, S.; Singhal, S. Identification of breast cancer margins using intraoperative near-infrared imaging. J. Surg. Oncol. 2016, 113, 508–514. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Berg, N.S.V.D.; Rosenthal, E.L.; Iv, M.; Zhang, M.; Leonel, J.C.M.V.; Walters, S.; Nishio, N.; Granucci, M.; Raymundo, R.; et al. EGFR-targeted intraoperative fluorescence imaging detects high-grade glioma with panitumumab-IRDye800 in a phase 1 clinical trial. Theranostics 2021, 11, 7130–7143. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, S.-I.; Tokuishi, K.; Miyawaki, M.; Anami, K.; Moroga, T.; Takeno, S.; Chujo, M.; Yamamoto, S.; Kawahara, K. Sentinel Node Navigation Surgery by Thoracoscopic Fluorescence Imaging System and Molecular Examination in Non-Small Cell Lung Cancer. Ann. Surg. Oncol. 2011, 19, 728–733. [Google Scholar] [CrossRef]
- Nomori, H.; Cong, Y.; Sugimura, H. Utility and pitfalls of sentinel node identification using indocyanine green during segmentectomy for cT1N0M0 non-small cell lung cancer. Surg. Today 2016, 46, 908–913. [Google Scholar] [CrossRef]
- Gilmore, D.M.; Khullar, O.V.; Jaklitsch, M.T.; Chirieac, L.R.; Frangioni, J.V.; Colson, Y.L. Identification of metastatic nodal disease in a phase 1 dose-escalation trial of intraoperative sentinel lymph node mapping in non–small cell lung cancer using near-infrared imaging. J. Thorac. Cardiovasc. Surg. 2013, 146, 562–570. [Google Scholar] [CrossRef] [Green Version]
- Yotsukura, M.; Okubo, Y.; Yoshida, Y.; Nakagawa, K.; Watanabe, S.-I. Indocyanine green imaging for pulmonary segmentectomy. JTCVS Tech. 2021, 6, 151–158. [Google Scholar] [CrossRef]
- Bédat, B.; Triponez, F.; Sadowski, S.M.; Ellenberger, C.; Licker, M.; Karenovics, W. Impact of near-infrared angiography on the quality of anatomical resection during video-assisted thoracic surgery segmentectomy. J. Thorac. Dis. 2018, 10, S1229–S1234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsui, T.; Takahashi, Y.; Nakada, T.; Matsushita, H.; Oya, Y.; Sakakura, N.; Kuroda, H. Efficacy of Xenon Light with Indocyanine Green for Intersegmental Visibility in Thoracoscopic Segmentectomy. J. Surg. Res. 2020, 259, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Xu, K.; Cen, R.; Deng, J.; Hao, Z.; Liu, J.; Takizawa, H.; Ng, C.S.H.; Marulli, G.; Kim, M.P.; et al. Preoperative computer tomography-guided indocyanine green injection is associated with successful localization of small pulmonary nodules. Transl. Lung Cancer Res. 2021, 10, 2229–2236. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Li, Z.; Huang, W.; Zhuang, J.; Lin, D.; Zhong, W.; Lan, B. Electromagnetic navigation bronchoscopic localization versus percutaneous CT -guided localization for thoracoscopic resection of small pulmonary nodules. Thorac. Cancer 2021, 12, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Vandoni, R.E.; Cuttat, J.-F.; Wicky, S.; Suter, M. CT-guided methylene-blue labelling before thoracoscopic resection of pulmonary nodules. Eur. J. Cardio-Thoracic Surg. 1998, 14, 265–270. [Google Scholar] [CrossRef] [Green Version]
- Abbas, A.; Kadakia, S.; Ambur, V.; Muro, K.; Kaiser, L. Intraoperative electromagnetic navigational bronchoscopic localization of small, deep, or subsolid pulmonary nodules. J. Thorac. Cardiovasc. Surg. 2017, 153, 1581–1590. [Google Scholar] [CrossRef] [Green Version]
- Geraci, T.C.; Ferrari-Light, D.; Kent, A.; Michaud, G.; Zervos, M.; Pass, H.I.; Cerfolio, R.J. Technique, Outcomes with Navigational Bronchoscopy Using Indocyanine Green for Robotic Segmentectomy. Ann. Thorac. Surg. 2019, 108, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Xia, X.; Gai, Y.; Feng, H.; Qin, C.; Pan, D.; Song, Y.; Zhang, Y.; Lan, X. Florescence Imaging Lung Cancer with a Small Molecule MHI-148. J. Fluoresc. 2020, 30, 1523–1530. [Google Scholar] [CrossRef]
- Zhang, C.; Liu, T.; Su, Y.; Luo, S.; Zhu, Y.; Tan, X.; Fan, S.; Zhang, L.; Zhou, Y.; Cheng, T.; et al. A near-infrared fluorescent heptamethine indocyanine dye with preferential tumor accumulation for in vivo imaging. Biomaterials 2010, 31, 6612–6617. [Google Scholar] [CrossRef] [PubMed]
- Predina, J.D.; Runge, J.; Newton, A.; Mison, M.; Xia, L.; Corbett, C.; Shin, M.; Sulyok, L.F.; Durham, A.; Nie, S.; et al. Evaluation of Aminolevulinic Acid-Derived Tumor Fluorescence Yields Disparate Results in Murine and Spontaneous Large Animal Models of Lung Cancer. Sci. Rep. 2019, 9, 7629. [Google Scholar] [CrossRef]
- Yang, X.; Shi, C.; Tong, R.; Qian, W.; Zhau, H.E.; Wang, R.; Zhu, G.; Cheng, J.; Yang, V.W.; Cheng, T.; et al. Near IR Heptamethine Cyanine Dye–Mediated Cancer Imaging. Clin. Cancer Res. 2010, 16, 2833–2844. [Google Scholar] [CrossRef] [Green Version]
- Charalampaki, P.; Proskynitopoulos, P.J.; Heimann, A.; Nakamura, M. 5-Aminolevulinic Acid Multispectral Imaging for the Fluorescence-Guided Resection of Brain Tumors: A Prospective Observational Study. Front. Oncol. 2020, 10, 1069. [Google Scholar] [CrossRef] [PubMed]
- Knipps, J.; Fischer, I.; Neumann, L.M.; Rapp, M.; Dibué-Adjei, M.; von Saß, C.F.; Placke, J.-M.; Mijderwijk, H.-J.; Steiger, H.-J.; Sabel, M.; et al. Quantification of PpIX-fluorescence of cerebral metastases: A pilot study. Clin. Exp. Metastasis 2019, 36, 467–475. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, S.; Lesniak, W.G.; Gabrielson, M.; Lisok, A.; Wharram, B.; Sysa-Shah, P.; Azad, B.B.; Pomper, M.G.; Nimmagadda, S. A humanized antibody for imaging immune checkpoint ligand PD-L1 expression in tumors. Oncotarget 2016, 7, 10215–10227. [Google Scholar] [CrossRef] [Green Version]
- Zhu, H.; Liu, T.-L.; Liu, C.-H.; Wang, J.; Zhang, H.; Dong, B.; Shen, J.; Zhao, C.-K.; Li, Z.-F.; Cheng, Z.; et al. Evaluation of a novel monoclonal antibody mAb109 by immuno-PET/fluorescent imaging for noninvasive lung adenocarcinoma diagnosis. Acta Pharmacol. Sin. 2019, 41, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Liu, S.; Liu, R.; Park, R.; Yu, H.; Krasnoperov, V.; Gill, P.S.; Li, Z.; Shan, H.; Conti, P.S. Axl-Targeted Cancer Imaging with Humanized Antibody h173. Mol. Imaging Biol. 2014, 16, 511–518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wan, J.; Wu, W.; Zhang, R.; Liu, S.; Huang, Y. Anti-EGFR antibody conjugated silica nanoparticles as probes for lung cancer detection. Exp. Ther. Med. 2017, 14, 3407–3412. [Google Scholar] [CrossRef] [Green Version]
- On, K.C.; Rho, J.; Yoon, H.Y.; Chang, H.; Yhee, J.Y.; Yoon, J.S.; Jeong, S.Y.; Kim, H.K.; Kim, K. Tumor-Targeting Glycol Chitosan Nanoparticles for Image-Guided Surgery of Rabbit Orthotopic VX2 Lung Cancer. Pharmaceutics 2020, 12, 621. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; Zhang, H.; Zhang, D.; Lu, H.; Ma, D. A Biocompatible Reconstituted High-Density Lipoprotein Nano-System as a Probe for Lung Cancer Detection. Med. Sci. Monit. 2015, 21, 2726–2733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoo, M.-K.; Park, I.-K.; Lim, H.-T.; Lee, S.-J.; Jiang, H.-L.; Kim, Y.-K.; Choi, Y.-J.; Cho, M.-H.; Cho, C.-S. Folate–PEG–superparamagnetic iron oxide nanoparticles for lung cancer imaging. Acta Biomater. 2012, 8, 3005–3013. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.; Cui, W.; He, X.; Guo, Q.; Wang, K.; Ye, X.; Tang, J. Whole Cell-SELEX Aptamers for Highly Specific Fluorescence Molecular Imaging of Carcinomas In Vivo. PLoS ONE 2013, 8, e70476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.J.; Lee, J.H.; Chung, H.K.; Ju, E.J.; Song, S.Y.; Jeong, S.-Y.; Choi, E.K. Application of peptide displaying phage as a novel diagnostic probe for human lung adenocarcinoma. Amino Acids 2016, 48, 1079–1086. [Google Scholar] [CrossRef]
- Ofori, L.O.; Withana, N.P.; Prestwood, T.R.; Verdoes, M.; Brady, J.J.; Winslow, M.M.; Sorger, J.; Bogyo, M. Design of Protease Activated Optical Contrast Agents That Exploit a Latent Lysosomotropic Effect for Use in Fluorescence-Guided Surgery. ACS Chem. Biol. 2015, 10, 1977–1988. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, J.-L.; Alencar, H.; Weissleder, R.; Mahmood, U. Near infrared thoracoscopy of tumoral protease activity for improved detection of peripheral lung cancer. Int. J. Cancer 2006, 118, 2672–2677. [Google Scholar] [CrossRef] [PubMed]
- Widen, J.C.; Tholen, M.; Yim, J.J.; Antaris, A.; Casey, K.M.; Rogalla, S.; Klaassen, A.; Sorger, J.; Bogyo, M. AND-gate contrast agents for enhanced fluorescence-guided surgery. Nat. Biomed. Eng. 2020, 5, 264–277. [Google Scholar] [CrossRef] [PubMed]
- Kwon, S.-H.; Wi, T.; Park, Y.I.; Kim, M.W.; Lee, G.; Higaki, T.; Choi, J.H.; Lee, R. Noninvasive Early Detection of Calpain 2-Enriched Non-Small Cell Lung Cancer Using a Human Serum Albumin-Bounded Calpain 2 Nanosensor. Bioconjugate Chem. 2020, 31, 803–812. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Goh, S.-H.; Choi, Y. Quenched cetuximab conjugate for fast fluorescence imaging of EGFR-positive lung cancers. Biomater. Sci. 2020, 9, 456–462. [Google Scholar] [CrossRef] [PubMed]
- Punganuru, S.R.; Madala, H.R.; Arutla, V.; Zhang, R.; Srivenugopal, K.S. Characterization of a highly specific NQO1-activated near-infrared fluorescent probe and its application for in vivo tumor imaging. Sci. Rep. 2019, 9, 8577. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.; Lei, Y.; Ge, J.; He, X.; Cui, W.; Ye, X.; Liu, J.; Wang, K. A Simple, pH-Activatable Fluorescent Aptamer Probe with Ultralow Background for Bispecific Tumor Imaging. Anal. Chem. 2019, 91, 9154–9160. [Google Scholar] [CrossRef] [PubMed]
- Achilefu, S.; Bloch, S.; Markiewicz, M.A.; Zhong, T.; Ye, Y.; Dorshow, R.B.; Chance, B.; Liang, K. Synergistic effects of light-emitting probes and peptides for targeting and monitoring integrin expression. Proc. Natl. Acad. Sci. USA 2005, 102, 7976–7981. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaw, S.K.; Liu, W.; Duran, C.F.A.G.; Schreiber, C.L.; Mendiola, M.D.L.B.; Zhai, C.; Roland, F.M.; Padanilam, S.J.; Smith, B.D. Non-Covalently Pre-Assembled High-Performance Near-Infrared Fluorescent Molecular Probes for Cancer Imaging. Chem. A Eur. J. 2018, 24, 13821–13829. [Google Scholar] [CrossRef]
- Xiao, W.; Ma, W.; Wei, S.; Li, Q.; Liu, R.; Carney, R.P.; Yang, K.; Lee, J.; Nyugen, A.; Yoneda, K.Y.; et al. High-affinity peptide ligand LXY30 for targeting α3β1 integrin in non-small cell lung cancer. J. Hematol. Oncol. 2019, 12, 56. [Google Scholar] [CrossRef] [Green Version]
- Citrin, D.; Lee, A.K.; Scott, T.; Sproull, M.; Ménard, C.; Tofilon, P.J.; Camphausen, K. In vivo tumor imaging in mice with near-infrared labeled endostatin. Mol. Cancer Ther. 2004, 3, 481–488. [Google Scholar] [PubMed]
- Pedrosa, S.; Pereira, P.; Correia, A.; Gama, F. Targetability of hyaluronic acid nanogel to cancer cells: In vitro and in vivo studies. Eur. J. Pharm. Sci. 2017, 104, 102–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, A.S.; Patek, R.; Enkemann, S.A.; Johnson, J.O.; Chen, T.; Toloza, E.; Vagner, J.; Morse, D.L. Delta-Opioid Receptor (δOR) Targeted Near-Infrared Fluorescent Agent for Imaging of Lung Cancer: Synthesis and Evaluation In Vitro and In Vivo. Bioconjugate Chem. 2015, 27, 427–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, W.; Qiu, X.; Zhang, F.; Sun, J.; Cameron, A.G.; Wendt, J.A.; Mawad, M.E.; Ke, S. An imageable retinoid acid derivative to detect human cancer xenografts and study therapeutic dosing to reduce its toxicity. Contrast Media Mol. Imaging 2010, 6, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.X.; Keating, J.J.; Jesus, E.M.; Judy, R.P.; Madajewski, B.; Venegas, O.; Okusanya, O.T.; Singhal, S. Optimization of the enhanced permeability and retention effect for near-infrared imaging of solid tumors with indocyanine green. Am. J. Nucl. Med. Mol. Imaging 2015, 5, 390–400. [Google Scholar]
- Newton, A.D.; Predina, J.D.; Corbett, C.J.; Frenzel-Sulyok, L.G.; Xia, L.; Petersson, E.J.; Tsourkas, A.; Nie, S.; Delikatny, E.J.; Singhal, S. Optimization of Second Window Indocyanine Green for Intraoperative Near-Infrared Imaging of Thoracic Malignancy. J. Am. Coll. Surg. 2018, 228, 188–197. [Google Scholar] [CrossRef] [PubMed]
- Holt, D.; Okusanya, O.; Judy, R.; Venegas, O.; Jiang, J.; DeJesus, E.; Eruslanov, E.; Quatromoni, J.; Bhojnagarwala, P.; Deshpande, C.; et al. Intraoperative Near-Infrared Imaging Can Distinguish Cancer from Normal Tissue but Not Inflammation. PLoS ONE 2014, 9, e103342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okusanya, O.; Holt, D.; Heitjan, D.; Deshpande, C.; Venegas, O.; Jiang, J.; Judy, R.; DeJesus, E.; Madajewski, B.; Oh, K.; et al. Intraoperative Near-Infrared Imaging Can Identify Pulmonary Nodules. Ann. Thorac. Surg. 2014, 98, 1223–1230. [Google Scholar] [CrossRef] [Green Version]
- Mao, Y.; Chi, C.; Yang, F.; Zhou, J.; He, K.; Li, H.; Chen, X.; Ye, J.; Wang, J.; Tian, J. The identification of sub-centimetre nodules by near-infrared fluorescence thoracoscopic systems in pulmonary resection surgeries. Eur. J. Cardio-Thoracic Surg. 2017, 52, 1190–1196. [Google Scholar] [CrossRef]
- Kim, H.K.; Quan, Y.H.; Choi, B.H.; Park, J.-H.; Han, K.N.; Choi, Y.; Kim, B.-M.; Choi, Y.H. Intraoperative pulmonary neoplasm identification using near-infrared fluorescence imaging. Eur. J. Cardio-Thoracic Surg. 2016, 49, 1497–1502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quan, Y.H.; Oh, C.H.; Jung, D.; Lim, J.-Y.; Choi, B.H.; Rho, J.; Choi, Y.; Han, K.N.; Kim, B.-M.; Kim, C.; et al. Evaluation of Intraoperative Near-Infrared Fluorescence Visualization of the Lung Tumor Margin with Indocyanine Green Inhalation. JAMA Surg. 2020, 155, 732. [Google Scholar] [CrossRef]
- Predina, J.D.; Newton, A.; Corbett, C.; Xia, L.; Sulyok, L.F.; Shin, M.; Deshpande, C.; Litzky, L.; Barbosa, E.; Low, P.S.; et al. Localization of Pulmonary Ground-Glass Opacities with Folate Receptor–Targeted Intraoperative Molecular Imaging. J. Thorac. Oncol. 2018, 13, 1028–1036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Predina, J.D.; Newton, A.D.; Connolly, C.; Dunbar, A.; Baldassari, M.; Deshpande, C.; Cantu, E., 3rd; Stadanlick, J.; Kularatne, S.A.; Low, P.S.; et al. Identification of a Folate Receptor-Targeted Near-Infrared Molecular Contrast Agent to Localize Pulmonary Adenocarcinomas. Mol. Ther. 2017, 26, 390–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Predina, J.D.; Newton, A.D.; Keating, J.; Barbosa, E.M.; Okusanya, O.; Xia, L.; Dunbar, A.; Connolly, C.; Baldassari, M.P.; Mizelle, J.; et al. Intraoperative Molecular Imaging Combined with Positron Emission Tomography Improves Surgical Management of Peripheral Malignant Pulmonary Nodules. Ann. Surg. 2017, 266, 479–488. [Google Scholar] [CrossRef] [PubMed]
- Predina, J.D.; Newton, A.D.; Keating, J.; Dunbar, A.; Connolly, C.; Baldassari, M.; Mizelle, J.; Xia, L.; Deshpande, C.; Kucharczuk, J.; et al. A Phase I Clinical Trial of Targeted Intraoperative Molecular Imaging for Pulmonary Adenocarcinomas. Ann. Thorac. Surg. 2018, 105, 901–908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Predina, J.D.; Newton, A.D.; Xia, L.; Corbett, C.; Connolly, C.; Shin, M.; Sulyok, L.F.; Litzky, L.; Deshpande, C.; Nie, S.; et al. An open label trial of folate receptor-targeted intraoperative molecular imaging to localize pulmonary squamous cell carcinomas. Oncotarget 2018, 9, 13517–13529. [Google Scholar] [CrossRef] [PubMed]
- Gangadharan, S.; Sarkaria, I.N.; Rice, D.; Murthy, S.; Braun, J.; Kucharczuk, J.; Predina, J.; Singhal, S. Multiinstitutional Phase 2 Clinical Trial of Intraoperative Molecular Imaging of Lung Cancer. Ann. Thorac. Surg. 2020, 112, 1150–1159. [Google Scholar] [CrossRef] [PubMed]
- Azari, F.; Kennedy, G.; Bernstein, E.; Delikatny, J.; Lee, J.Y.; Kucharczuk, J.; Low, P.S.; Singhal, S. Evaluation of OTL38-Generated Tumor-to-Background Ratio in Intraoperative Molecular Imaging-Guided Lung Cancer Resections. Mol. Imaging Biol. 2021, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Keating, J.J.; Runge, J.J.; Singhal, S.; Nims, S.; Venegas, O.; Durham, A.C.; Swain, G.; Nie, S.; Low, P.S.; Holt, D.E. Intraoperative near-infrared fluorescence imaging targeting folate receptors identifies lung cancer in a large-animal model. Cancer 2017, 123, 1051–1060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stummer, W.; Pichlmeier, U.; Meinel, T.; Wiestler, O.D.; Zanella, F.; Reulen, H.-J.; ALA-Glioma Study Group. Fluorescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma: A randomised controlled multicentre phase III trial. Lancet Oncol. 2006, 7, 392–401. [Google Scholar] [CrossRef]
- Hernot, S.; van Manen, L.; Debie, P.; Mieog, J.S.D.; Vahrmeijer, A.L. Latest developments in molecular tracers for fluorescence image-guided cancer surgery. Lancet Oncol. 2015, 20, e354–e367. [Google Scholar] [CrossRef]
- Topalian, S.L.; Drake, C.G.; Pardoll, D.M. Immune Checkpoint Blockade: A Common Denominator Approach to Cancer Therapy. Cancer Cell 2015, 27, 450–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gatalica, Z.; Snyder, C.; Maney, T.; Ghazalpour, A.; Holterman, D.A.; Xiao, N.; Overberg, P.; Rose, I.; Basu, G.D.; Vranic, S.; et al. Programmed Cell Death 1 (PD-1) and Its Ligand (PD-L1) in Common Cancers and Their Correlation with Molecular Cancer Type. Cancer Epidemiol. Biomark. Prev. 2014, 23, 2965–2970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorensen, S.F.; Zhou, W.; Dolled-Filhart, M.; Georgsen, J.B.; Wang, Z.; Emancipator, K.; Wu, D.; Busch-Sørensen, M.; Meldgaard, P.; Hager, H. PD-L1 Expression and Survival among Patients with Advanced Non–Small Cell Lung Cancer Treated with Chemotherapy. Transl. Oncol. 2016, 9, 64–69. [Google Scholar] [CrossRef] [Green Version]
- Lehtonen, S.; Svensk, A.-M.; Soini, Y.; Pääkkö, P.; Hirvikoski, P.; Kang, S.W.; Säily, M.; Kinnula, V.L. Peroxiredoxins, a novel protein family in lung cancer. Int. J. Cancer 2004, 111, 514–521. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Lee, T.-H.; Park, E.S.; Suh, J.M.; Park, S.J.; Chung, H.K.; Kwon, O.-Y.; Kim, Y.K.; Ro, H.K.; Shong, M. Role of Peroxiredoxins in Regulating Intracellular Hydrogen Peroxide and Hydrogen Peroxide-induced Apoptosis in Thyroid Cells. J. Biol. Chem. 2000, 275, 18266–18270. [Google Scholar] [CrossRef] [Green Version]
- Egler, R.A.; Fernandes, E.; Rothermund, K.; Sereika, S.; Souza-Pinto, N.; Jaruga, P.; Dizdaroglu, M.; Prochownik, E.V. Regulation of reactive oxygen species, DNA damage and c-Myc function by peroxiredoxin 1. Oncogene 2005, 24, 8038–8050. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.-H.; Bogner, P.N.; Baek, S.-H.; Ramnath, N.; Liang, P.; Kim, H.-R.; Andrews, C.; Park, Y.-M. Up-Regulation of Peroxiredoxin 1 in Lung Cancer and Its Implication as a Prognostic and Therapeutic Target. Clin. Cancer Res. 2008, 14, 2326–2333. [Google Scholar] [CrossRef] [Green Version]
- Linger, R.M.; Keating, A.K.; Earp, H.S.; Graham, D.K. TAM Receptor Tyrosine Kinases: Biologic Functions, Signaling, and Potential Therapeutic Targeting in Human Cancer. Adv. Cancer Res. 2008, 100, 35–83. [Google Scholar] [CrossRef] [Green Version]
- Wimmel, A.; Glitz, D.; Kraus, A.; Roeder, J.; Schuermann, M. Axl receptor tyrosine kinase expression in human lung cancer cell lines correlates with cellular adhesion. Eur. J. Cancer 2001, 37, 2264–2274. [Google Scholar] [CrossRef]
- Shinh, Y.-S.; Lai, C.-Y.; Kao, Y.-R.; Shiah, S.-G.; Chu, Y.-W.; Lee, H.-S.; Wu, C.-W. Expression of Axl in Lung Adenocarcinoma and Correlation with Tumor Progression. Neoplasia 2005, 7, 1058–1064. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salomon, D.S.; Brandt, R.; Ciardiello, F.; Normanno, N. Epidermal growth factor-related peptides and their receptors in human malignancies. Crit. Rev. Oncol. 1995, 19, 183–232. [Google Scholar] [CrossRef]
- Lin, F.; Jia, H.-R.; Wu, F.-G. Glycol Chitosan: A Water-Soluble Polymer for Cell Imaging and Drug Delivery. Molecules 2019, 24, 4371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wadsack, C.; Hirschmugl, B.; Hammer, A.; Levak-Frank, S.; Kozarsky, K.F.; Sattler, W.; Malle, E. Scavenger receptor class B, type I on non-malignant and malignant human epithelial cells mediates cholesteryl ester-uptake from high density lipoproteins. Int. J. Biochem. Cell Biol. 2003, 35, 441–454. [Google Scholar] [CrossRef]
- Mahmoudi, M.; Sant, S.; Wang, B.; Laurent, S.; Sen, T. Superparamagnetic iron oxide nanoparticles (SPIONs): Development, surface modification and applications in chemotherapy. Adv. Drug Deliv. Rev. 2011, 63, 24–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Shannessy, D.J.; Yu, G.; Smale, R.; Fu, Y.-S.; Singhal, S.; Thiel, R.P.; Somers, E.B.; Vachani, A. Folate Receptor Alpha Expression in Lung Cancer: Diagnostic and Prognostic Significance. Oncotarget 2012, 3, 414–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nunez, M.I.; Behrens, C.; Woods, D.M.; Lin, H.; Suraokar, M.; Kadara, H.; Hofstetter, W.; Kalhor, N.; Lee, J.J.; Franklin, W.; et al. High Expression of Folate Receptor Alpha in Lung Cancer Correlates with Adenocarcinoma Histology and Mutation. J. Thorac. Oncol. 2012, 7, 833–840. [Google Scholar] [CrossRef] [Green Version]
- Cagle, P.T.; Zhai, Q.J.; Murphy, L.; Low, P. Folate Receptor in Adenocarcinoma and Squamous Cell Carcinoma of the Lung: Potential Target for Folate-Linked Therapeutic Agents. Arch. Pathol. Lab. Med. 2013, 137, 241–244. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.; Chen, W.-H.; Tian, J.; Cheng, Z. NIRF Nanoprobes for Cancer Molecular Imaging: Approaching Clinic. Trends Mol. Med. 2020, 26, 469–482. [Google Scholar] [CrossRef]
- Wu, X.; Chen, J.; Wu, M.; Zhao, J.X. Aptamers: Active Targeting Ligands for Cancer Diagnosis and Therapy. Theranostics 2015, 5, 322–344. [Google Scholar] [CrossRef] [PubMed]
- Tuerk, C.; Gold, L. Systematic Evolution of Ligands by Exponential Enrichment: RNA Ligands to Bacteriophage T4 DNA Polymerase. Science 1990, 249, 505–510. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Xu, L.; Shi, X.; Tan, W.; Fang, X.; Shangguan, D. Recognition of subtype non-small cell lung cancer by DNA aptamers selected from living cells. Analyst 2009, 134, 1808–1814. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.P. Filamentous fusion phage: Novel expression vectors that display cloned antigens on the virion surface. Science 1985, 228, 1315–1317. [Google Scholar] [CrossRef] [PubMed]
- Keefe, A.D.; Pai, S.; Ellington, A. Aptamers as therapeutics. Nat. Rev. Drug Discov. 2010, 9, 537–550. [Google Scholar] [CrossRef]
- Mieog, J.S.D.; Achterberg, F.B.; Zlitni, A.; Hutteman, M.; Burggraaf, J.; Swijnenburg, R.-J.; Gioux, S.; Vahrmeijer, A.L. Fundamentals and developments in fluorescence-guided cancer surgery. Nat. Rev. Clin. Oncol. 2021, 19, 9–22. [Google Scholar] [CrossRef] [PubMed]
- Gocheva, V.; Wang, H.-W.; Gadea, B.B.; Shree, T.; Hunter, K.E.; Garfall, A.L.; Berman, T.; Joyce, J.A. IL-4 induces cathepsin protease activity in tumor-associated macrophages to promote cancer growth and invasion. Genes Dev. 2010, 24, 241–255. [Google Scholar] [CrossRef] [Green Version]
- Zhang, G.; Fang, T.; Chang, M.; Li, J.; Hong, Q.; Bai, C.; Zhou, J. Calpain 2 knockdown promotes cell apoptosis and restores gefitinib sensitivity through epidermal growth factor receptor/protein kinase B/survivin signaling. Oncol. Rep. 2018, 40, 1937–1946. [Google Scholar] [CrossRef] [PubMed]
- Schlager, J.J.; Powis, G. Cytosolic NAD(P)H:(Quinone-acceptor)oxidoreductase in human normal and tumor tissue: Effects of cigarette smoking and alcohol. Int. J. Cancer 1990, 45, 403–409. [Google Scholar] [CrossRef]
- Oh, E.-T.; Park, H.J. Implications of NQO1 in cancer therapy. BMB Rep. 2015, 48, 609–617. [Google Scholar] [CrossRef] [Green Version]
- Cui, X.; Jin, T.; Wang, X.; Jin, G.; Li, Z.; Lin, L. NAD(P)H:quinone oxidoreductase-1 overexpression predicts poor prognosis in small cell lung cancer. Oncol. Rep. 2014, 32, 2589–2595. [Google Scholar] [CrossRef] [Green Version]
- Gatenby, R.A.; Gillies, R. Why do cancers have high aerobic glycolysis? Nat. Rev. Cancer 2004, 324, 1029–1033. [Google Scholar] [CrossRef] [PubMed]
- Vander Heiden, M.G.; Cantley, L.C.; Thompson, C.B. Understanding the Warburg Effect: The Metabolic Requirements of Cell Proliferation. Science 2009, 324, 1029–1033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conus, S.; Simon, H.-U. Cathepsins: Key modulators of cell death and inflammatory responses. Biochem. Pharmacol. 2008, 76, 1374–1382. [Google Scholar] [CrossRef] [PubMed]
- Desgrosellier, J.S.; Cheresh, D.A. Integrins in cancer: Biological implications and therapeutic opportunities. Nat. Rev. Cancer 2010, 10, 9–22. [Google Scholar] [CrossRef] [Green Version]
- Walia, A.; Yang, J.F.; Huang, Y.-H.; Rosenblatt, M.I.; Chang, J.-H.; Azar, D.T. Endostatin’s emerging roles in angiogenesis, lymphangiogenesis, disease, and clinical applications. Biochim. Biophys. Acta BBA Gen. Subj. 2015, 1850, 2422–2438. [Google Scholar] [CrossRef] [Green Version]
- De Valk, K.S.; Deken, M.M.; Handgraaf, H.J.M.; Bhairosingh, S.S.; Bijlstra, O.D.; van Esdonk, M.J.; van Scheltinga, A.G.T.; Valentijn, A.R.P.; March, T.L.; Vuijk, J.; et al. First-in-Human Assessment of cRGD-ZW800-1, a Zwitterionic, Integrin-Targeted, Near-Infrared Fluorescent Peptide in Colon Carcinoma. Clin. Cancer Res. 2020, 26, 3990–3998. [Google Scholar] [CrossRef]
- Goodarzi, N.; Varshochian, R.; Kamalinia, G.; Atyabi, F.; Dinarvand, R. A review of polysaccharide cytotoxic drug conjugates for cancer therapy. Carbohydr. Polym. 2013, 92, 1280–1293. [Google Scholar] [CrossRef]
- Rudzki, Z.; Jothy, S. CD44 and the adhesion of neoplastic cells. Mol. Pathol. 1997, 50, 57–71. [Google Scholar] [CrossRef] [Green Version]
- Minami, M.; Satoh, M. Molecular biology of the opioid receptors: Structures, functions and distributions. Neurosci. Res. 1995, 23, 121–145. [Google Scholar] [CrossRef]
- Zagon, I.S.; McLaughlin, P.J.; Goodman, S.R.; Rhodes, R.E. Opioid receptors and endogenous opioids in diverse human and animal cancers. J. Natl. Cancer Inst. 1987, 79, 1059–1065. [Google Scholar]
- Schreiber, G.; Campa, M.J.; Prabhakar, S.; O’Briant, K.; Bepler, G.; Patz, E.F., Jr. Molecular characterization of the human delta opioid receptor in lung cancer. Anticancer Res. 1998, 18, 1787–1792. [Google Scholar] [PubMed]
- Hansen, L.A.; Sigman, C.C.; Andreola, F.; Ross, S.A.; Kelloff, G.J.; de Luca, L.M. Retinoids in chemoprevention and differentiation therapy. Carcinogenesis 2000, 21, 1271–1279. [Google Scholar] [CrossRef] [PubMed]
- Freemantle, S.J.; Spinella, M.J.; Dmitrovsky, E. Retinoids in cancer therapy and chemoprevention: Promise meets resistance. Oncogene 2003, 22, 7305–7315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mongan, N.P.; Gudas, L.J. Diverse actions of retinoid receptors in cancer prevention and treatment. Differentiation 2007, 75, 853–870. [Google Scholar] [CrossRef] [PubMed]
- Reinhart, M.B.; Huntington, C.R.; Blair, L.J.; Heniford, B.T.; Augenstein, V.A. Indocyanine Green. Surg. Innov. 2015, 23, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Yoneya, S.; Saito, T.; Komatsu, Y.; Koyama, I.; Takahashi, K.; Duvoll-Young, J. Binding properties of indocyanine green in human blood. Investig. Ophthalmol. Vis. Sci. 1998, 39, 1286–1290. [Google Scholar]
- Mahalingam, S.M.; Kularatne, S.A.; Myers, C.H.; Gagare, P.; Norshi, M.; Liu, X.; Singhal, S.; Low, P.S. Evaluation of Novel Tumor-Targeted Near-Infrared Probe for Fluorescence-Guided Surgery of Cancer. J. Med. Chem. 2018, 61, 9637–9646. [Google Scholar] [CrossRef] [Green Version]
- Frangioni, J.V. Translating in vivo diagnostics into clinical reality. Nat. Biotechnol. 2006, 24, 909–913. [Google Scholar] [CrossRef]
- ClinicalTrials.gov. Evaluation of IRDye800CW-nimotuzumab in Lung Cancer Surgery. Available online: https://www.clinicaltrials.gov/ct2/show/record/NCT04459065 (accessed on 26 November 2021).
- ClinicalTrials.gov. A Phase I/II Study Evaluating the Safety and Pharmacokinetics of Panitumumab-IRDye800 as an Optical Imaging Agent to Detect Lung Cancer During Surgical Procedures. Available online: https://www.clinicaltrials.gov/ct2/show/record/NCT03582124 (accessed on 26 November 2021).
- ClinicalTrials.gov. A Phase 2a, Single-dose, Open-label Study to Evaluate Diagnostic Performance, Safety & Timing of Postdose Imaging of ONM-100, an Intraoperative Fluorescence Imaging Agent for the Detection of Cancer, in Patients with Solid Tumors Undergoing Routine Surgery. Available online: https://www.clinicaltrials.gov/ct2/show/record/NCT03735680 (accessed on 26 November 2021).
- Voskuil, F.J.; Steinkamp, P.J.; Zhao, T.; van der Vegt, B.; Koller, M.; Doff, J.J.; Jayalakshmi, Y.; Hartung, J.P.; Gao, J.; Sumer, B.D.; et al. Exploiting metabolic acidosis in solid cancers using a tumor-agnostic pH-activatable nanoprobe for fluorescence-guided surgery. Nat. Commun. 2020, 11, 3257. [Google Scholar] [CrossRef]
- ClinicalTrials.gov. Intraoperative Imaging of Pulmonary Nodules by SGM-101. Available online: https://www.clinicaltrials.gov/ct2/show/NCT04315467 (accessed on 26 November 2021).
- Wang, L.V.; Hu, S. Photoacoustic Tomography: In Vivo Imaging from Organelles to Organs. Science 2012, 335, 1458–1462. [Google Scholar] [CrossRef] [Green Version]
- Xia, J.; Yao, J.; Wang, L. Photoacoustic Tomography: Principles and Advances. Prog. Electromagn. Res. 2014, 147, 1–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Attia, A.B.E.; Balasundaram, G.; Moothanchery, M.; Dinish, U.; Bi, R.; Ntziachristos, V.; Olivo, M. A review of clinical photoacoustic imaging: Current and future trends. Photoacoustics 2019, 16, 100144. [Google Scholar] [CrossRef] [PubMed]
- Zou, C.; Wu, B.; Dong, Y.; Song, Z.; Zhao, Y.; Ni, X.; Yang, Y.; Liu, Z. Biomedical photoacoustics: Fundamentals, instrumentation and perspectives on nanomedicine. Int. J. Nanomed. 2016, 12, 179–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, C.Y.; Fujino, K.; Motooka, Y.; Gregor, A.; Bernards, N.; Ujiie, H.; Kinoshita, T.; Chung, K.Y.; Han, S.H.; Yasufuku, K. Photoacoustic imaging to localize indeterminate pulmonary nodules: A preclinical study. PLoS ONE 2020, 15, e0231488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, J.; Zhu, B.; Zheng, K.; He, S.; Meng, L.; Song, J.; Yang, H. Recent Progress in NIR-II Contrast Agent for Biological Imaging. Front. Bioeng. Biotechnol. 2020, 7, 487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, H.; Ji, M. Recent Advances of Organic Near-Infrared II Fluorophores in Optical Properties and Imaging Functions. Mol. Imaging Biol. 2020, 23, 160–172. [Google Scholar] [CrossRef]
- Lim, Y.T.; Kim, S.; Nakayama, A.; Stott, N.E.; Bawendi, M.G.; Frangioni, J.V. Selection of Quantum Dot Wavelengths for Biomedical Assays and Imaging. Mol. Imaging 2003, 2, 50–64. [Google Scholar] [CrossRef]
- Hu, Z.; Fang, C.; Li, B.; Zhang, Z.; Cao, C.; Cai, M.; Su, S.; Sun, X.; Shi, X.; Li, C.; et al. First-in-human liver-tumour surgery guided by multispectral fluorescence imaging in the visible and near-infrared-I/II windows. Nat. Biomed. Eng. 2020, 4, 259–271. [Google Scholar] [CrossRef]
- Bijlstra, O.D.; Achterberg, F.B.; Grosheide, L.; Vahrmeijer, A.L.; Swijnenburg, R.-J. Fluorescence-guided minimally-invasive surgery for colorectal liver metastases, a systematic review. Laparosc. Surg. 2021, 5. [Google Scholar] [CrossRef]
- Wang, S.; Fan, Y.; Li, D.; Sun, C.; Lei, Z.; Lu, L.; Wang, T.; Zhang, F. Anti-quenching NIR-II molecular fluorophores for in vivo high-contrast imaging and pH sensing. Nat. Commun. 2019, 10, 1058. [Google Scholar] [CrossRef]
- Nerup, N.; Andersen, H.S.; Ambrus, R.; Strandby, R.B.; Svendsen, M.B.S.; Madsen, M.H.; Svendsen, L.B.; Achiam, M. Quantification of fluorescence angiography in a porcine model. Langenbeck’s Arch. Surg. 2017, 402, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Son, G.M.; Kwon, M.S.; Kim, Y.; Kim, J.; Kim, S.H.; Lee, J.W. Quantitative analysis of colon perfusion pattern using indocyanine green (ICG) angiography in laparoscopic colorectal surgery. Surg. Endosc. 2018, 33, 1640–1649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lütken, C.D.; Achiam, M.; Svendsen, M.B.S.; Boni, L.; Nerup, N. Optimizing quantitative fluorescence angiography for visceral perfusion assessment. Surg. Endosc. 2015, 34, 5223–5233. [Google Scholar] [CrossRef]
- Chan, M.-H.; Lin, H.-M. Preparation and identification of multifunctional mesoporous silica nanoparticles for in vitro and in vivo dual-mode imaging, theranostics, and targeted tracking. Biomaterials 2015, 46, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Zavvar, T.; Babaei, M.; Abnous, K.; Taghdisi, S.M.; Nekooei, S.; Ramezani, M.; Alibolandi, M. Synthesis of multimodal polymersomes for targeted drug delivery and MR/fluorescence imaging in metastatic breast cancer model. Int. J. Pharm. 2020, 578, 119091. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Zhao, Y.; Mu, X.; Wu, H.; Chen, L.; Liu, W.; Mu, Y.; Liu, J.; Wei, X. A silica–polymer composite nano system for tumor-targeted imaging and p53 gene therapy of lung cancer. J. Biomater. Sci. Polym. Ed. 2015, 26, 384–400. [Google Scholar] [CrossRef]
- Xie, X.; Zhan, C.; Wang, J.; Zeng, F.; Wu, S. An Activatable Nano-Prodrug for Treating Tyrosine-Kinase-Inhibitor-Resistant Non-Small Cell Lung Cancer and for Optoacoustic and Fluorescent Imaging. Small 2020, 16, e2003451. [Google Scholar] [CrossRef]
- Celli, J.P.; Spring, B.Q.; Rizvi, I.; Evans, C.L.; Samkoe, K.S.; Verma, S.; Pogue, B.W.; Hasan, T. Imaging and Photodynamic Therapy: Mechanisms, Monitoring, and Optimization. Chem. Rev. 2010, 80, 156–162. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Ramamurthy, G.; Shirke, A.A.; Walker, E.; Mangadlao, J.; Wang, Z.; Wang, Y.; Shan, L.; Schluchter, M.D.; Dong, Z.; et al. Photodynamic Therapy Is an Effective Adjuvant Therapy for Image-Guided Surgery in Prostate Cancer. Cancer Res. 2020, 80, 156–162. [Google Scholar] [CrossRef]
- Liu, B.; Qiao, G.; Han, Y.; Shen, E.; Alfranca, G.; Tan, H.; Wang, L.; Pan, S.; Ma, L.; Xiong, W.; et al. Targeted theranostics of lung cancer: PD-L1-guided delivery of gold nanoprisms with chlorin e6 for enhanced imaging and photothermal/photodynamic therapy. Acta Biomater. 2020, 117, 361–373. [Google Scholar] [CrossRef]
- Li, W.; Zheng, C.; Pan, Z.; Chen, C.; Hu, D.; Gao, G.; Kang, S.; Cui, H.; Gong, P.; Cai, L. Smart hyaluronidase-actived theranostic micelles for dual-modal imaging guided photodynamic therapy. Biomaterials 2016, 101, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Xia, F.; Niu, J.; Hong, Y.; Li, C.; Cao, W.; Wang, L.; Hou, W.; Liu, Y.; Cui, D. Matrix metallopeptidase 2 targeted delivery of gold nanostars decorated with IR-780 iodide for dual-modal imaging and enhanced photothermal/photodynamic therapy. Acta Biomater. 2019, 89, 289–299. [Google Scholar] [CrossRef] [PubMed]
- Xia, F.; Hou, W.; Zhang, C.; Zhi, X.; Cheng, J.; de la Fuente, J.M.; Song, J.; Cui, D. pH-responsive gold nanoclusters-based nanoprobes for lung cancer targeted near-infrared fluorescence imaging and chemo-photodynamic therapy. Acta Biomater. 2018, 68, 308–319. [Google Scholar] [CrossRef] [PubMed]
- Yue, C.; Zhang, C.; Alfranca, G.; Yang, Y.; Jiang, X.; Yang, Y.; Pan, F.; de la Fuente, J.M.; Cui, D. Near-Infrared Light Triggered ROS-activated Theranostic Platform based on Ce6-CPT-UCNPs for Simultaneous Fluorescence Imaging and Chemo-Photodynamic Combined Therapy. Theranostics 2016, 6, 456–469. [Google Scholar] [CrossRef] [PubMed]



| Fluorescent Probe | Molecular Target | Fluorophore | Peak Excitation Wavelength | Peak Emission Wavelength | Ref. |
|---|---|---|---|---|---|
| Preclinical tested probes | |||||
| Non-specific fluorophores | |||||
| MHI-148 | NA | MHI-148 | 760 | 800 | [36] |
| IR-780 iodide | NA | IR-780 iodide | 780 | 799 | [37] |
| 5-ALA | NA | PpIX | 405/633 | 635/710 | [38,40,41] |
| Antibodies | |||||
| NIR-PD-L1-mAb | PD-L1 | 800CW | 780 | 800 | [42] |
| Cy5.5–mAb109 | Prdx I | Cy5.5 | 675 | 694 | [43] |
| h173-Cy5.5 | Axl | Cy5.5 | 675 | 694 | [44] |
| Nanoparticles | |||||
| Anti-EGFR/MB-SHSi | EGFR | MB | 665 | 686 | [45] |
| Cy5.5-CNPs | NA | Cy5.5 | 675 | 694 | [46] |
| ICG-CNPs | NA | ICG | 780 | 805 | [46] |
| rHDL/MB-CCPs | SR-B1 | MB | 665 | 686 | [47] |
| FA-PEG-SPIONs-Cy5.5 | FA | Cy5.5 | 675 | 694 | [48] |
| Generated probes | |||||
| Cy5-S6 | S6 | Cy5 | 649 | 666 | [49] |
| Cy5.5-labeled Pep-1 | Pep-1 (CAKATCPAC) | Cy5.5 | 675 | 694 | [50] |
| Activatable probes | |||||
| 6QCNIR | Cathepsins | DyLight780-B1 | 783 | 799 | [51] |
| Prosense 680 | Cathepsins | Prosense 680 | 680 | 700 | [52] |
| Prosense 750 | Cathepsins | Prosense 750 | 650 | 780 | [52] |
| DEATH-CAT-FNIR | Cathepsins + caspase 3 | Heptamethine cyanine | 765 | 788 | [53] |
| HSA-CAPN2 | CAPN2 | Cy5 | 649 | 666 | [54] |
| Q-cetuximab | EGFR | ATTO655 | 600 | 684 | [55] |
| NIR-ASM | NQO1 | ASM | 460 | 646 | [56] |
| pH-AAP | S6 | Cy5 | 649 | 666 | [57] |
| Integrin-targeting probe | |||||
| Cyp-GRD | αVβ3 | Cypate | 780 | 830 | [58] |
| cRGDfK-targeted probe | Integrins | H3H | 644 | 668 | [59] |
| LXY30-biotin/streptavidin-Cy5.5 | α3β1 | Cy5.5 | 675 | 694 | [60] |
| Endostatin-Cy5.5 | VEGFR-2, VEGFR-3, α5β1, αVβ3 | Cy5.5 | 675 | 694 | [61] |
| Others | |||||
| HyA-AT-Alexa680 | CD44 | Alexa fluor 680 | 679 | 702 | [62] |
| Dmt-Tic-IR800 | δOR | 800CW | 780 | 800 | [63] |
| RA-IRDye800CW | Retinoids | 800CW | 780 | 800 | [64] |
| Clinical tested probes | |||||
| ICG | NA | ICG | 780 | 805 | [65,66,67,68,69,70,71] |
| OTL38 | FRα | S0456 | 774–776 | 794–796 | [72,73,74,75,76,77,78,79] |
| Author and Year | Study Population | #Patients (Lesions) | Doses | Timing | Highlights |
|---|---|---|---|---|---|
| Jiang 2015 | LLC mouse models | 25 (25) | 0.71, 2.0, 5.0, 7.5, 10.0 mg/kg IV | 1 min–72 h | The optimal doses and timing in mice were 5 mg/kg and 24 h. This was confirmed in patients. TBRs in the 5 mg/kg group were 3.1–3.7. |
| Patients with pulmonary nodules | 6 (6) | 0.71, 2.0, 5.0 mg/kg IV | 1 day | ||
| Newton 2018 | Patients with NSCLC | 18 (18) | 1–3 mg/kg IV (n = 9), 4–5 mg/kg IV | 1 day | In the 4–5 mg/kg group, 8 of 9 tumors were fluorescent, with a mean TBR of 2.70. In the 1–3 mg/kg group, 1 of 9 tumors were fluorescent, with a mean TBR of 1.49. |
| Holt 2014 | Dogs with primary lung cancer | 8 (8) | 5 mg/kg IV | 1 day | All tumors were fluorescent with a mean in situ SBR of 8.8. NIR imaging was able to detect adequate resection margins in 5 tumors. The other 3 tumors had peritumoral inflammation. |
| Patients with pulmonary nodules | 5 (5) | All nodules were fluorescent, with a mean SBR of 8.1. In 4 nodules, NIR imaging was able to detect adequate resection margins, and none of these nodules showed inflammation. The other tumor was surrounded by atelectasis. | |||
| Okusanya 2014 | Patients with pulmonary nodules | 18 (18) | 5 mg/kg IV | 1 day | Of 18 lesions, 14 showed fluorescence in situ. There were 5 additional nodules detected. All fluorescent nodules were malignant, and the mean SBR was 2.2. Of non-fluorescent lesions, 3 of 4 were malignant. The sensitivity was 86.4%. |
| Mao 2017 | Patients with pulmonary nodules | 36 (76) | 5 mg/kg IV | 1 day | Of 76 lesions, 68 were detected with IGS, of which 63 lesions were malignant. All 8 non-fluorescent lesions were malignant. The mean SBR was 3.29. In total, 9 additional lesions were identified. Of these, 5 were false positives. The sensitivity was 89.3%. |
| Kim 2016 | Patients with pulmonary cancer | 11 (11) | 1 mg/kg IV | 1 day | Of 11 lesions, 10 were fluorescent, of which 8 lesions were malignant. The two false-positive lesions had a pathological complete response after neoadjuvant therapy and new obstructive pneumonia. The non-fluorescent lesion was a false negative. The sensitivity was 88.9%. |
| Quan 2020 | LLC mouse models | 32 (32) | 1.0 mg/kg inhalation | 10 min–24 h | The tumor margin could be visualized by fluorescence imaging, as confirmed with histological examination. Tumor margins were visible 10 min to 24 h after inhalation of ICG, with a signal peak after 1 h. Inhalation of ICG had a significantly higher tumor margin detection efficiency as compared with intravenous injection of ICG. |
| VX2 rabbit models | 20 (20) | 0.1, 0.25, 0.5, 1.0 mg/kg inhalation | Tumor margins were visible from a dose of 0.25 mg/kg, and higher doses resulted in higher fluorescence intensity in normal tissue. One rabbit showed a false-positive lesion, which turned out to be atelectasis. | ||
| Human lung specimen | 6 (6) | NR inhalation | NR | All tumor margins were visible, with a mean tumor margin detection efficiency (ratio between signal-to-noise ratio in tumor tissue and that in healthy tissue) of 2.9. |
| Author and Year | Study Population | #Patients (Lesions) | Doses | Timing | TP (%) | FP (%) | TN (%) | FN (%) | #Additional Lesions (%TP) | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Predina 2018 | A549 mice models | 15 (15) | 0.0, 0.0125, 0.025, 0.050 and 0.25 mg/kg IV | Up to 8 days | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| Patients with pulmonary nodules | 10 (10) | 0.025 mg/kg IV | 3–6 h | 8 (80) | 0 (0) | 1 (10) | 1 (10) | 3 (100) | 84.6 | * | * | * | |
| Keating 2017 | Dogs with primary lung cancer | 10 (10) | 0.185 mg/kg IV | 2–3 h | 10 (100) | * | * | 0 (0) | NR | 100 | * | * | * |
| Patients with adenocarcinoma | 3 (3) | 0.025 mg/kg IV | 3 (100) | * | * | 0 (0) | NR | 100 | * | * | * | ||
| Azari 2021 | Patients with pulmonary nodules | 279 (279) | 0.025 mg/kg IV | Mean 7.7 h | 217 (77.8) | 32 (12.9) | 8 (2.9) | 22 (7.9) | NR | 90.8 | 20 | 87.1 | 26.7 |
| Gangadharan 2021 | Patients with pulmonary nodules | 92 (92) | 0.025 mg/kg IV | 2–6 h | NR | NR | NR | NR | 24 (37.5) | NR | NR | NR | NR |
| Predina (2) 2018 | Patients with ground-glass opacity | 20 (21) | 0.025 mg/kg IV | 3–6 h | 15 (71.4) | 1 (4.8) | 0 (0) | 5 (23.8) | NR | 75 | * | * | * |
| Predina (3) 2018 | Patients with squamous cell cancer | 12 (13) | 0.025 mg/kg IV | 3–6 h | 7 (53.8) | * | * | 5 (38.5) | NR | 58.3 | * | * | * |
| Predina (4) 2018 | Patients with adenocarcinoma | 20 (21) | 0.025 mg/kg IV | 3–6 h | 17 (81) | * | * | 4 (19) | 4 (100) | 84 | * | * | * |
| Predina 2017 | Patients with pulmonary nodules | 50 (66) | 0.025 mg/kg IV | 3–6 h | 56 (84.6) | 4 (6.1) | 3 (4.5) | 3 (4.5) | 9 (100) | 95.6 | 42.9 | 94.2 | 50 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neijenhuis, L.K.A.; de Myunck, L.D.A.N.; Bijlstra, O.D.; Kuppen, P.J.K.; Hilling, D.E.; Borm, F.J.; Cohen, D.; Mieog, J.S.D.; Steup, W.H.; Braun, J.; et al. Near-Infrared Fluorescence Tumor-Targeted Imaging in Lung Cancer: A Systematic Review. Life 2022, 12, 446. https://doi.org/10.3390/life12030446
Neijenhuis LKA, de Myunck LDAN, Bijlstra OD, Kuppen PJK, Hilling DE, Borm FJ, Cohen D, Mieog JSD, Steup WH, Braun J, et al. Near-Infrared Fluorescence Tumor-Targeted Imaging in Lung Cancer: A Systematic Review. Life. 2022; 12(3):446. https://doi.org/10.3390/life12030446
Chicago/Turabian StyleNeijenhuis, Lisanne K. A., Lysanne D. A. N. de Myunck, Okker D. Bijlstra, Peter J. K. Kuppen, Denise E. Hilling, Frank J. Borm, Danielle Cohen, J. Sven D. Mieog, Willem H. Steup, Jerry Braun, and et al. 2022. "Near-Infrared Fluorescence Tumor-Targeted Imaging in Lung Cancer: A Systematic Review" Life 12, no. 3: 446. https://doi.org/10.3390/life12030446
APA StyleNeijenhuis, L. K. A., de Myunck, L. D. A. N., Bijlstra, O. D., Kuppen, P. J. K., Hilling, D. E., Borm, F. J., Cohen, D., Mieog, J. S. D., Steup, W. H., Braun, J., Burggraaf, J., Vahrmeijer, A. L., & Hutteman, M. (2022). Near-Infrared Fluorescence Tumor-Targeted Imaging in Lung Cancer: A Systematic Review. Life, 12(3), 446. https://doi.org/10.3390/life12030446