
Transmastoid Ultrasound Detection of Middle Ear Effusion and Its Association with Clinical Audiometric Tests



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subject Enrolment
2.2. Clinical Assessments
2.3. Ultrasound Measurement
2.4. Statistical Analyses
3. Results
3.1. Patients’ Characteristics
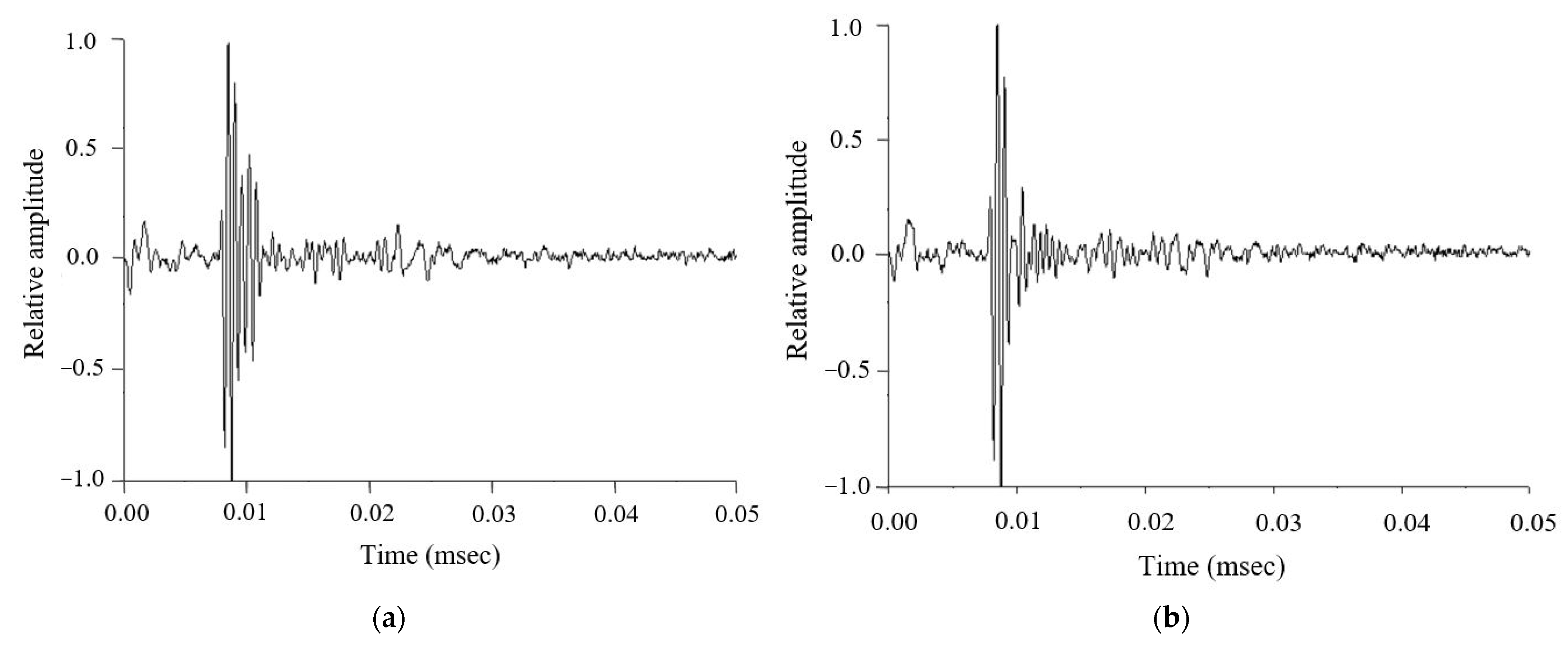
3.2. Ultrasonic Signals in Both Groups
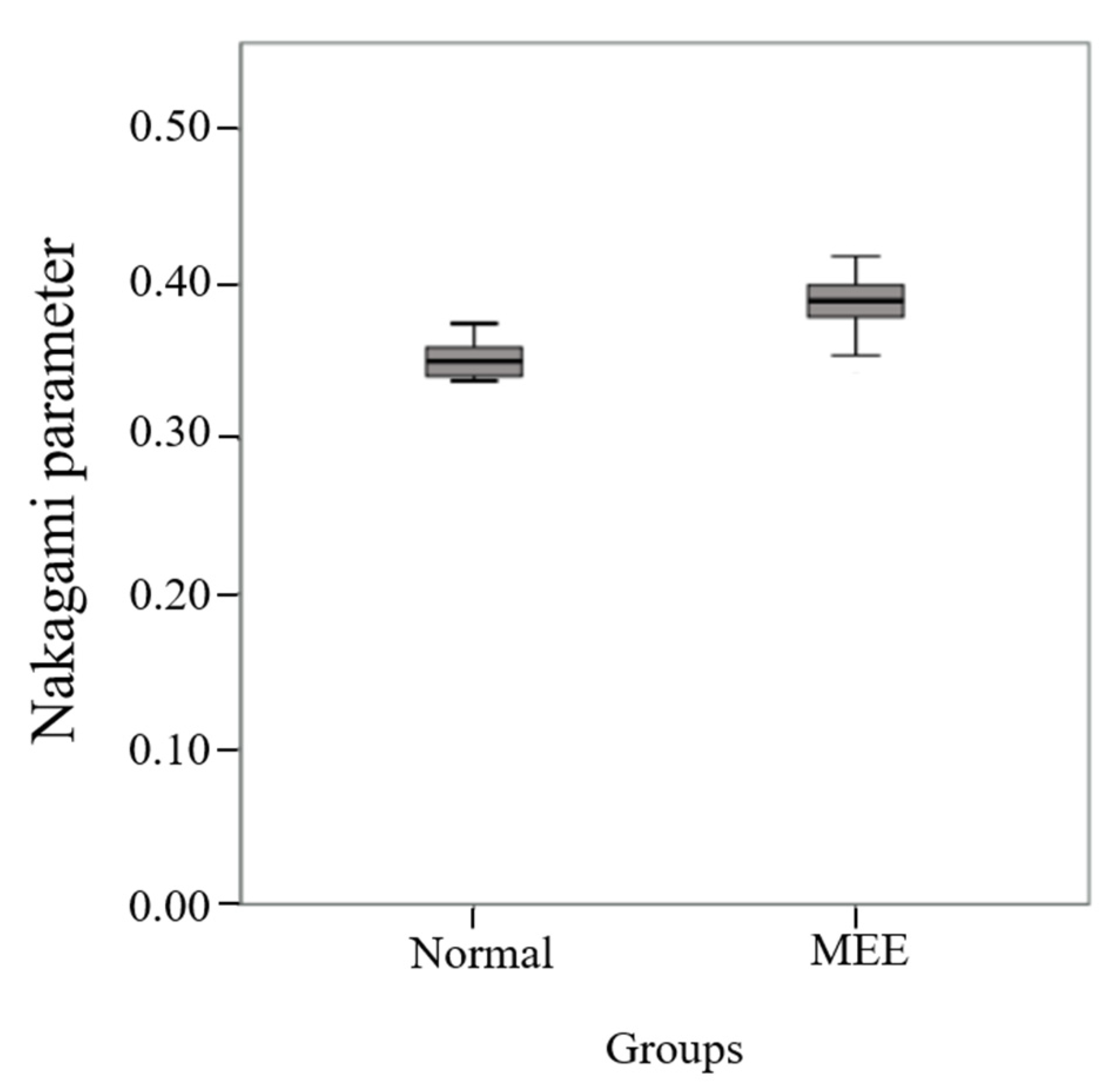
3.3. Nakagami Parameters in the Normal and MEE Groups
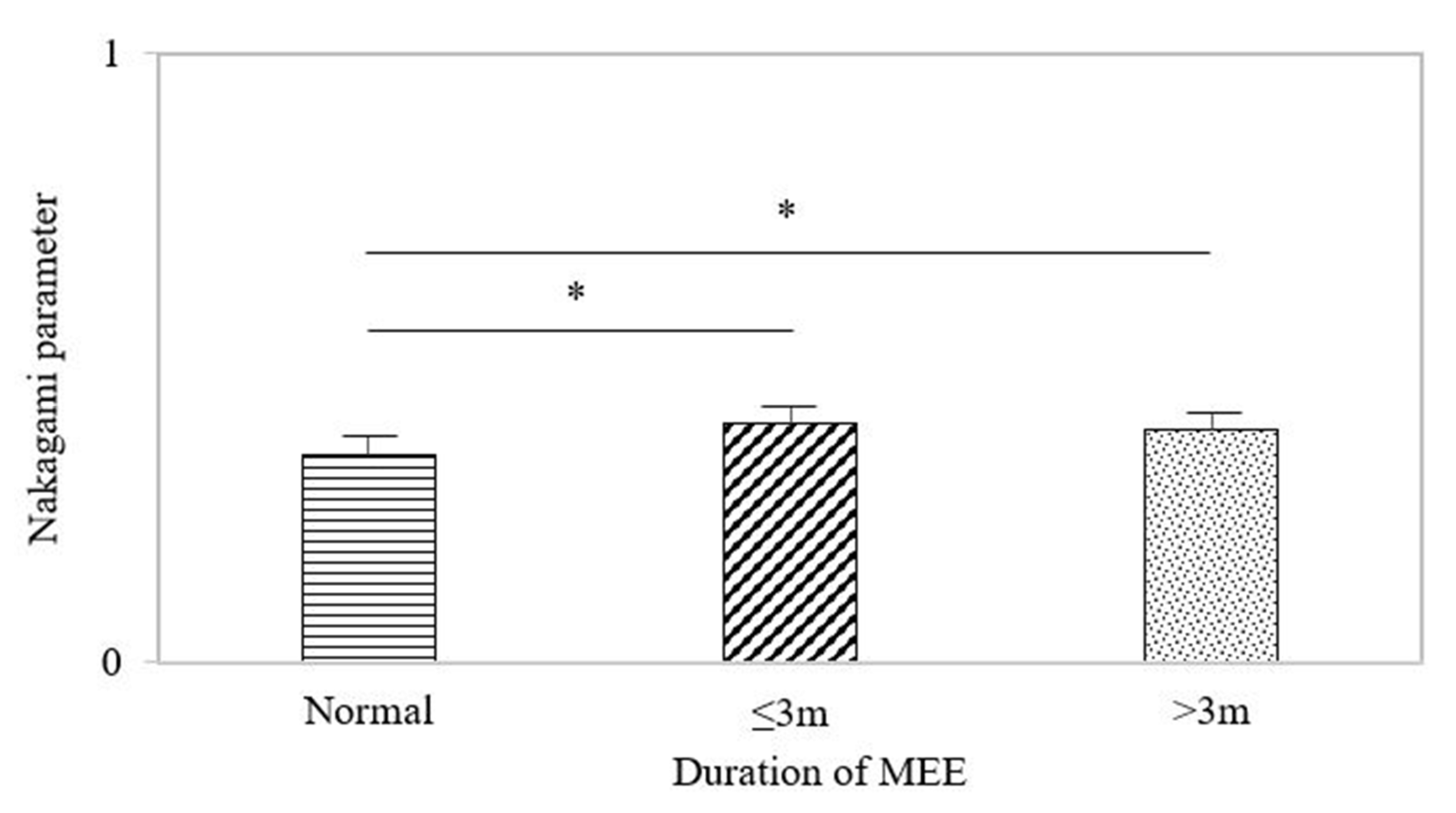
3.4. Nakagami Parameters in MEE within a Period of 3 Months and Longer than 3 Months
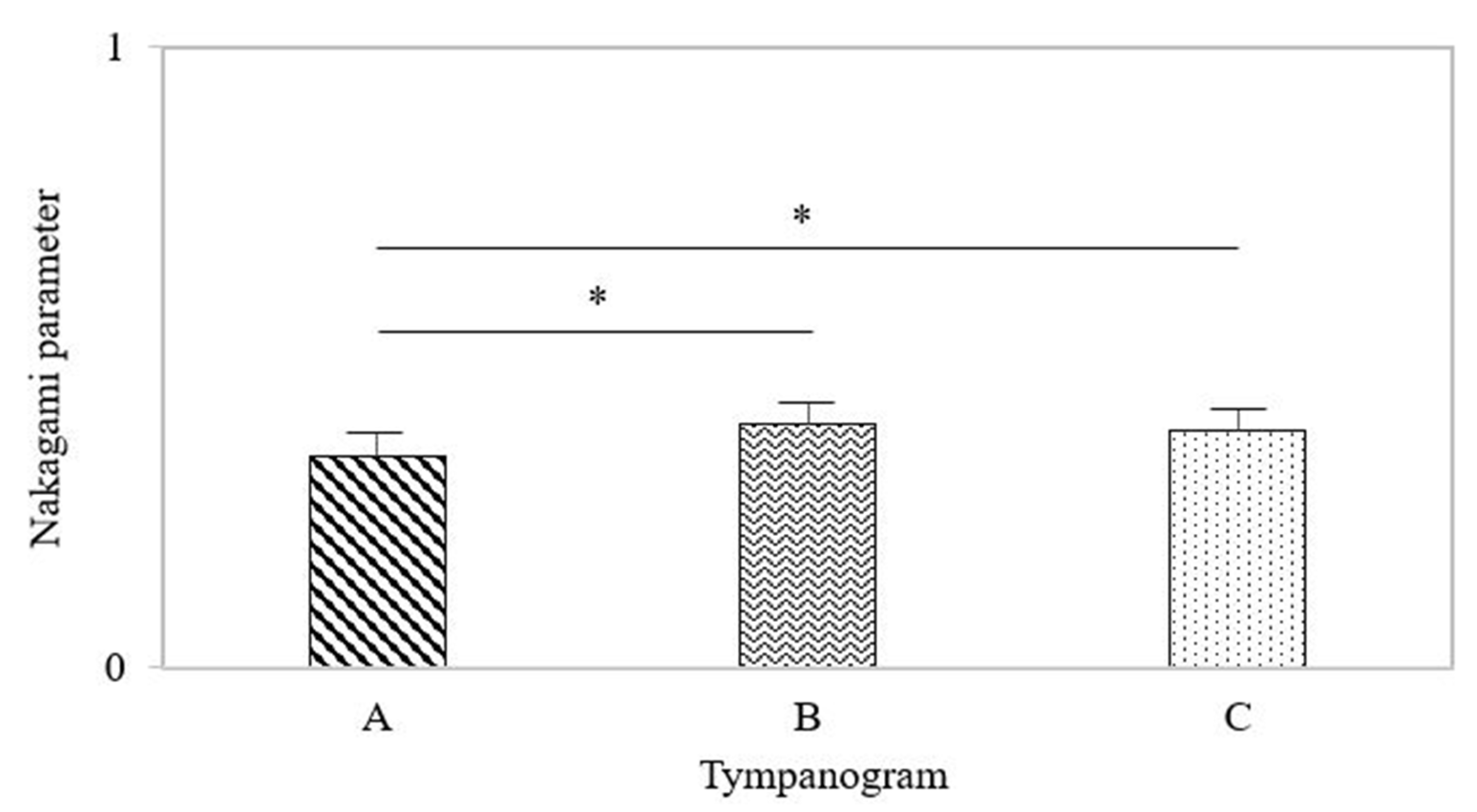
3.5. Nakagami Parameters in the Three Types of Tympanogram
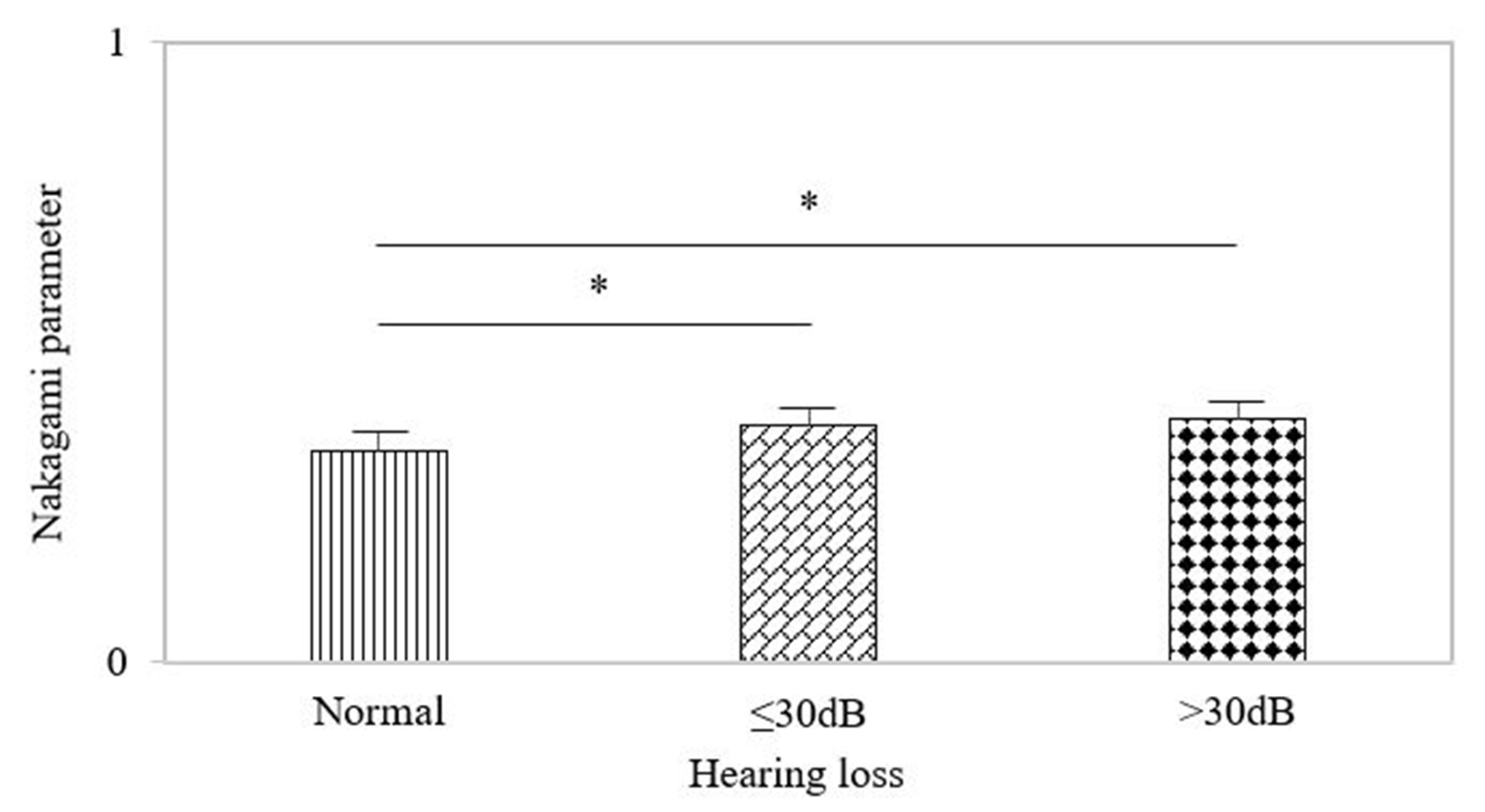
3.6. Nakagami Parameters in the MEE Group with Hearing Loss ≤30 dB and >30 dB
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dagan, R. Treatment of acute otitis media—Challenges in the era of antibiotic resistance. Vaccine 2020, 19, S9–S16. [Google Scholar] [CrossRef]
- Danishyar, A.; Ashurst, J.V. Acute Otitis Media; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Majima, Y.; Hamaguchi, Y.; Hirata, K.; Takeuchi, K.; Morishita, A.; Sakakura, Y. Hearing impairment in relation to viscoelasticity of middle ear effusions in children. Ann. Otol. Rhinol. Laryngol. 1988, 97, 272–274. [Google Scholar] [CrossRef] [PubMed]
- Ravicz, M.E.; Rosowski, J.J.; Merchant, S.N. Mechanisms of hearing loss resulting from middle-ear fluid. Hear Res. 2004, 195, 103–130. [Google Scholar] [CrossRef] [PubMed]
- Fria, T.J.; Cantekin, E.I.; Eichler, J.A. Hearing acuity of children with otitis media with effusion. Arch. Otolaryngol. 1985, 111, 10–16. [Google Scholar] [CrossRef] [PubMed]
- MRC Multi-Centre Otitis Media Study Group. Sensitivity, specificity and predictive value of tympanometry in predicting a hearing impairment in otitis media with effusion. Clin. Otolaryngol. Allied Sci. 1999, 24, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Preciado, D.; Nolan, R.M.; Joshi, R.; Krakovsky, G.M.; Zhang, A.; Pudik, N.A.; Kumar, N.K.; Shelton, R.L.; Boppart, S.A.; Bauman, N.M. Otitis media middle ear effusion identification and characterization using an optical coherence tomography otoscope. Otolaryngol. Head Neck Surg. 2020, 162, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Won, J.; Monroy, G.L.; Huang, P.C.; Hill, M.C.; Novak, M.A.; Porter, R.G.; Spillman, D.R.; Chaney, E.J.; Barkalifa, R.; Boppart, S.A. Assessing the effect of middle ear effusions on wideband acoustic immittance using optical coherence tomography. Ear Hear. 2020, 41, 811–824. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.K.; Wan, Y.L.; Tsui, P.H.; Chiu, W.T.; Jui, F. Using 1 MHz pulse-echo ultrasound externally applied to detect mastoid effusion: Cadaver experiments. Ultrasonics 2012, 52, 663–667. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.K.; Fang, J.; Wan, Y.L.; Tsui, P.H. Ultrasound characterization of the mastoid for detecting middle ear effusion: A preliminary clinical validation. Sci. Rep. 2016, 6, 27777. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenfeld, R.M.; Tunkel, D.E.; Schwartz, S.R.; Anne, S.; Bishop, C.E.; Chelius, D.C.; Hackell, J.; Hunter, L.L.; Keppel, K.L.; Kim, A.H.; et al. Clinical Practice Guideline: Tympanostomy Tubes in Children (Update). Otolaryngol. Head Neck Surg. 2022, 166 (Suppl. S1), S1–S55. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G* Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blomgren, K.; Pitkäranta, A. Is it possible to diagnose acute otitis media accurately in primary health care? Fam. Pract. 2003, 20, 524–527. [Google Scholar] [CrossRef] [PubMed]
- Takata, G.S.; Chan, L.S.; Morphew, T.; Mangione-Smith, R.; Morton, S.C.; Shekelle, P. Evidence assessment of the accuracy of methods of diagnosing middle ear effusion in children with otitis media with effusion. Pediatrics 2003, 112, 1379–1387. [Google Scholar] [CrossRef] [PubMed]
- Anwar, K.; Khan, S.; Rehman, H.U.; Javaid, M.; Shahabi, I. Otitis media with effusion: Accuracy of tympanometry in detecting fluid in the middle ears of children at myringotomies. Pak. J. Med. Sci. 2016, 32, 466–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kashani, R.G.; Młyńczak, M.C.; Zarabanda, D.; Solis-Pazmino, P.; Huland, D.M.; Ahmad, I.N.; Singh, S.P.; Valdez, T.A. Shortwave infrared otoscopy for diagnosis of middle ear effusions: A machine-learning-based approach. Sci. Rep. 2021, 11, 12509. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Family Physicians; American Academy of Pediatrics Subcommittee on Otitis Media with Effusion. Otitis media with effusion. Pediatrics 2004, 113, 1412–1429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.Y.; Chu, S.Y.; Lin, Y.C.; Tsai, Y.W.; Tai, C.L.; Yang, K.C.; Tsui, P.H. Quantitative imaging of ultrasound backscattered signals with information entropy for bone microstructure characterization. Sci. Rep. 2022, 12, 414. [Google Scholar] [CrossRef] [PubMed]
- John, S.; Turner, J.R.; John, H. Per-Lee. Chapter 120 Auditory Dysfunction: Hearing Loss. In Book Clinical Methods: The History, Physical, and Laboratory Examinations, 3rd ed.; Walker, H.K., Hall, W.D., Hurst, J.W., Eds.; Butterworths: Boston, MA, USA, 1990. [Google Scholar]
- Pereira, N.M.; Maresh, A.; Modi, V.K.; Rosenblatt, S.D. Tympanostomy tubes in the age of quarantine. Int. J. Pediatr. Otorhinolaryngol. 2022, 154, 111047. [Google Scholar] [CrossRef] [PubMed]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.-K.; Wan, Y.-L.; Hsieh, L.-C.; Tsui, P.-H. Transmastoid Ultrasound Detection of Middle Ear Effusion and Its Association with Clinical Audiometric Tests. Life 2022, 12, 599. https://doi.org/10.3390/life12040599
Chen C-K, Wan Y-L, Hsieh L-C, Tsui P-H. Transmastoid Ultrasound Detection of Middle Ear Effusion and Its Association with Clinical Audiometric Tests. Life. 2022; 12(4):599. https://doi.org/10.3390/life12040599
Chicago/Turabian StyleChen, Chin-Kuo, Yung-Liang Wan, Li-Chun Hsieh, and Po-Hsiang Tsui. 2022. "Transmastoid Ultrasound Detection of Middle Ear Effusion and Its Association with Clinical Audiometric Tests" Life 12, no. 4: 599. https://doi.org/10.3390/life12040599
APA StyleChen, C.-K., Wan, Y.-L., Hsieh, L.-C., & Tsui, P.-H. (2022). Transmastoid Ultrasound Detection of Middle Ear Effusion and Its Association with Clinical Audiometric Tests. Life, 12(4), 599. https://doi.org/10.3390/life12040599