
Circulating miRNA-195-5p and -451a in Patients with Acute Hemorrhagic Stroke in Emergency Department

 , , ,
, , , 
 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Selection of Participants
2.2. Interventions
2.3. miRNA Isolation and Real-Time Reverse Transcription (qRT-PCR)
2.4. Serum VEGF-A ELISA Assay
2.5. Outcomes
2.6. Statistical Analysis
3. Results
3.1. Characteristics of Study Subjects
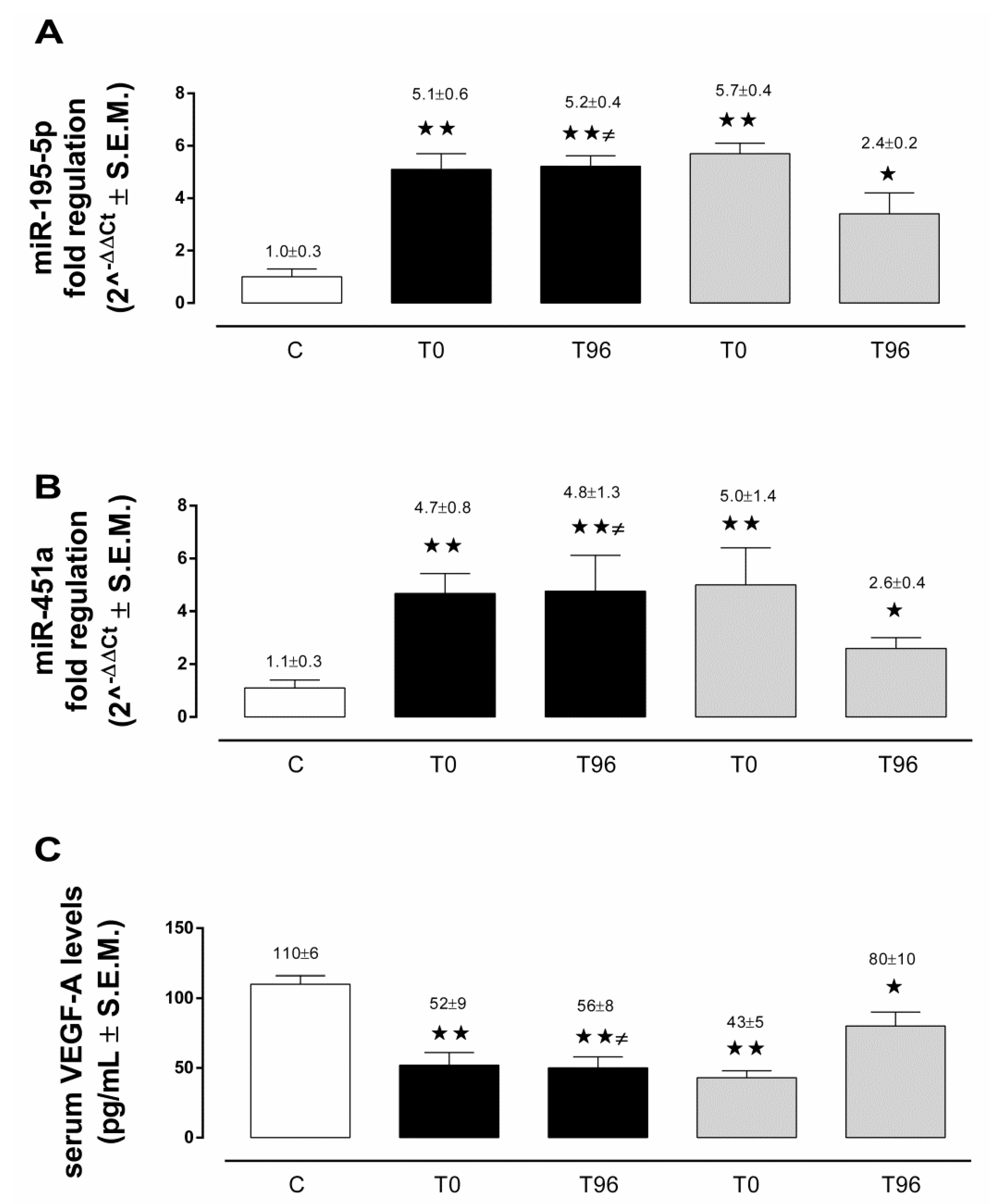
3.2. Circulating miRNA-195-5p in ICH and AIS Patients
3.3. Circulating miRNA-451a in ICH and AIS Patients
3.4. Serum VEGF-A in ICH and AIS Patients
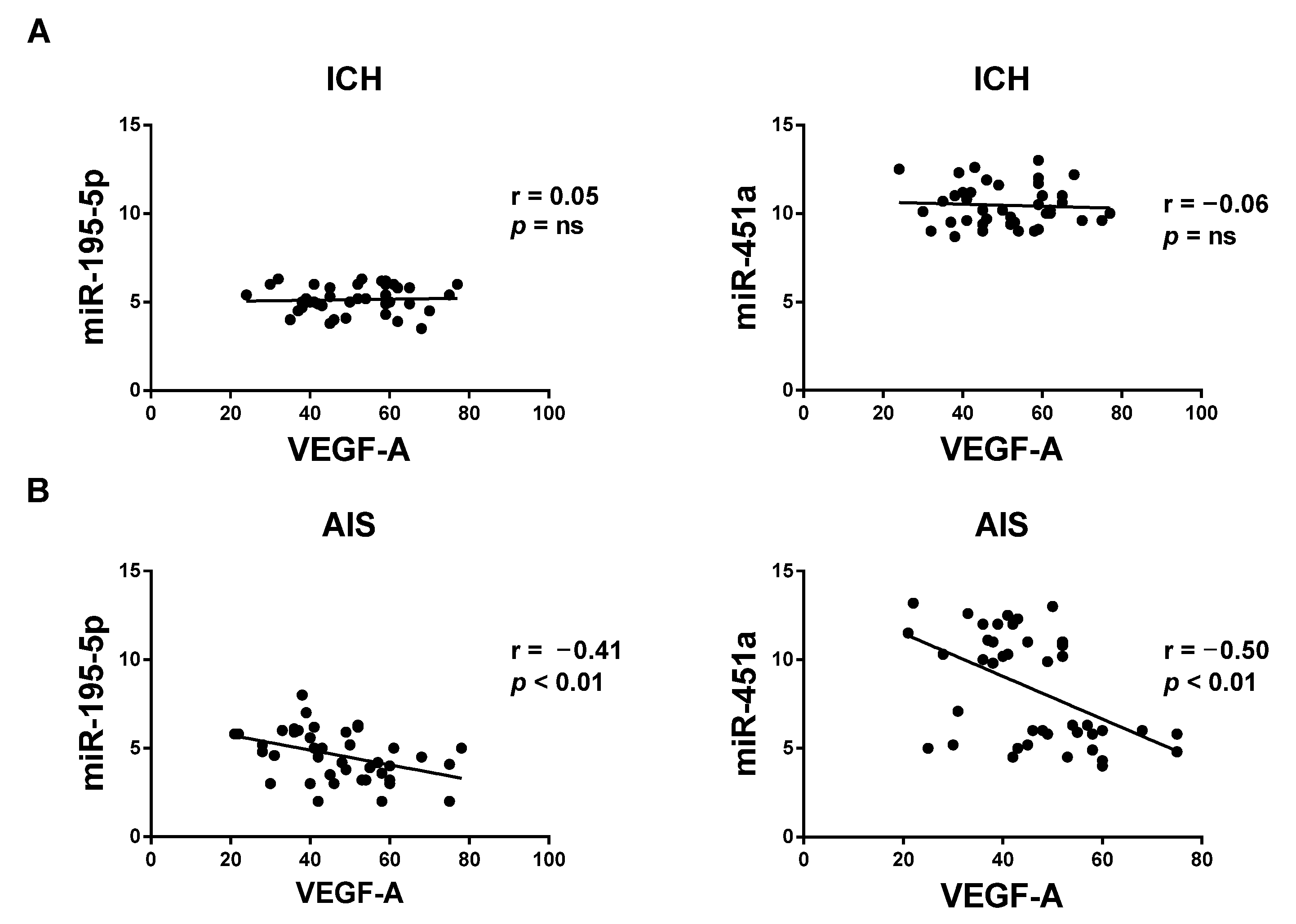
3.5. Correlation between Circulating miRNAs and VEGF-A Serum Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McGurgan, I.J.; Ziai, W.C.; Werring, D.J.; Al-Shahi Salman, R.; Parry-Jones, A.R. Acute Intracerebral Haemorrhage: Diagnosis and Management. Pract. Neurol. 2021, 21, 128–136. [Google Scholar] [CrossRef] [PubMed]
- Hemphill, J.C.; Bonovich, D.C.; Besmertis, L.; Manley, G.T.; Johnston, S.C. The ICH Score: A Simple, Reliable Grading Scale for Intracerebral Hemorrhage. Stroke 2001, 32, 891–897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Asch, C.J.; Luitse, M.J.; Rinkel, G.J.; van der Tweel, I.; Algra, A.; Klijn, C.J. Incidence, Case Fatality, and Functional Outcome of Intracerebral Haemorrhage over Time, According to Age, Sex, and Ethnic Origin: A Systematic Review and Meta-Analysis. Lancet Neurol. 2010, 9, 167–176. [Google Scholar] [CrossRef]
- Krishnamurthi, R.V.; Ikeda, T.; Feigin, V.L. Global, Regional and Country-Specific Burden of Ischaemic Stroke, Intracerebral Haemorrhage and Subarachnoid Haemorrhage: A Systematic Analysis of the Global Burden of Disease Study 2017. Neuroepidemiology 2020, 54, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Balami, J.S.; Buchan, A.M. Complications of Intracerebral Haemorrhage. Lancet Neurol. 2012, 11, 101–118. [Google Scholar] [CrossRef]
- Zeng, Y.; Cheng, H.; Cheng, L.; Huang, G.; Chen, Y.; Tang, W.; He, J. Comparison of Poststroke Depression between Acute Ischemic and Hemorrhagic Stroke Patients. Int. J. Geriatr. Psychiatry 2021, 36, 493–499. [Google Scholar] [CrossRef] [PubMed]
- Morotti, A.; Goldstein, J.N. Diagnosis and Management of Acute Intracerebral Hemorrhage. Emerg. Med. Clin. N. Am. 2016, 34, 883–899. [Google Scholar] [CrossRef] [Green Version]
- Manners, J.; Steinberg, A.; Shutter, L. Early Management of Acute Cerebrovascular Accident. Curr. Opin. Crit. Care 2017, 23, 556–560. [Google Scholar] [CrossRef]
- Ehrenreich, H.; Kästner, A.; Weissenborn, K.; Streeter, J.; Sperling, S.; Wang, K.K.; Worthmann, H.; Hayes, R.L.; von Ahsen, N.; Kastrup, A.; et al. Circulating Damage Marker Profiles Support a Neuroprotective Effect of Erythropoietin in Ischemic Stroke Patients. Mol. Med. 2011, 17, 1306–1310. [Google Scholar] [CrossRef]
- Whiteley, W.; Jackson, C.; Lewis, S.; Lowe, G.; Rumley, A.; Sandercock, P.; Wardlaw, J.; Dennis, M.; Sudlow, C. Association of Circulating Inflammatory Markers With Recurrent Vascular Events After Stroke: A Prospective Cohort Study. Stroke 2011, 42, 10–16. [Google Scholar] [CrossRef] [Green Version]
- Faura, J.; Bustamante, A.; Reverté, S.; García-Berrocoso, T.; Millán, M.; Castellanos, M.; Lara-Rodríguez, B.; Zaragoza, J.; Ventura, O.; Hernández-Pérez, M.; et al. Blood Biomarker Panels for the Early Prediction of Stroke-Associated Complications. JAHA 2021, 10, e018946. [Google Scholar] [CrossRef] [PubMed]
- Bustamante, A.; López-Cancio, E.; Pich, S.; Penalba, A.; Giralt, D.; García-Berrocoso, T.; Ferrer-Costa, C.; Gasull, T.; Hernández-Pérez, M.; Millan, M.; et al. Blood Biomarkers for the Early Diagnosis of Stroke: The Stroke-Chip Study. Stroke 2017, 48, 2419–2425. [Google Scholar] [CrossRef] [PubMed]
- Mojtabavi, H.; Shaka, Z.; Momtazmanesh, S.; Ajdari, A.; Rezaei, N. Circulating Brain-Derived Neurotrophic Factor as a Potential Biomarker in Stroke: A Systematic Review and Meta-Analysis. J. Transl. Med. 2022, 20, 126. [Google Scholar] [CrossRef] [PubMed]
- Åberg, N.D.; Wall, A.; Anger, O.; Jood, K.; Andreasson, U.; Blennow, K.; Zetterberg, H.; Isgaard, J.; Jern, C.; Svensson, J. Circulating Levels of Vascular Endothelial Growth Factor and Post-stroke Long-term Functional Outcome. Acta Neurol. Scand. 2020, 141, 405–414. [Google Scholar] [CrossRef]
- Toyoda, K.; Yoshimura, S.; Nakai, M.; Koga, M.; Sasahara, Y.; Sonoda, K.; Kamiyama, K.; Yazawa, Y.; Kawada, S.; Sasaki, M.; et al. Twenty-Year Change in Severity and Outcome of Ischemic and Hemorrhagic Strokes. JAMA Neurol. 2022, 79, 61. [Google Scholar] [CrossRef]
- Zhou, S.; Bao, J.; Wang, Y.; Pan, S. S100β as a Biomarker for Differential Diagnosis of Intracerebral Hemorrhage and Ischemic Stroke. Neurol. Res. 2016, 38, 327–332. [Google Scholar] [CrossRef]
- Luger, S.; Jæger, H.S.; Dixon, J.; Bohmann, F.O.; Schaefer, J.; Richieri, S.P.; Larsen, K.; Hov, M.R.; Bache, K.G.; Foerch, C.; et al. Diagnostic Accuracy of Glial Fibrillary Acidic Protein and Ubiquitin Carboxy-Terminal Hydrolase-L1 Serum Concentrations for Differentiating Acute Intracerebral Hemorrhage from Ischemic Stroke. Neurocrit. Care 2020, 33, 39–48. [Google Scholar] [CrossRef]
- Foerch, C.; Niessner, M.; Back, T.; Bauerle, M.; De Marchis, G.M.; Ferbert, A.; Grehl, H.; Hamann, G.F.; Jacobs, A.; Kastrup, A.; et al. Diagnostic Accuracy of Plasma Glial Fibrillary Acidic Protein for Differentiating Intracerebral Hemorrhage and Cerebral Ischemia in Patients with Symptoms of Acute Stroke. Clin. Chem. 2012, 58, 237–245. [Google Scholar] [CrossRef] [Green Version]
- Llombart, V.; García-Berrocoso, T.; Bustamante, A.; Giralt, D.; Rodriguez-Luna, D.; Muchada, M.; Penalba, A.; Boada, C.; Hernández-Guillamon, M.; Montaner, J. Plasmatic Retinol-Binding Protein 4 and Glial Fibrillary Acidic Protein as Biomarkers to Differentiate Ischemic Stroke and Intracerebral Hemorrhage. J. Neurochem. 2016, 136, 416–424. [Google Scholar] [CrossRef]
- Montaner, J.; Mendioroz, M.; Delgado, P.; García-Berrocoso, T.; Giralt, D.; Merino, C.; Ribó, M.; Rosell, A.; Penalba, A.; Fernández-Cadenas, I.; et al. Differentiating Ischemic from Hemorrhagic Stroke Using Plasma Biomarkers: The S100B/RAGE Pathway. J. Proteom. 2012, 75, 4758–4765. [Google Scholar] [CrossRef]
- Dias, A.; Silva, I.; Pinto, I.M.; Maia, L.F. Timely and Blood-Based Multiplex Molecular Profiling of Acute Stroke. Life 2021, 11, 816. [Google Scholar] [CrossRef] [PubMed]
- Bejleri, J.; Jirström, E.; Donovan, P.; Williams, D.J.; Pfeiffer, S. Diagnostic and Prognostic Circulating MicroRNA in Acute Stroke: A Systematic and Bioinformatic Analysis of Current Evidence. J. Stroke 2021, 23, 162–182. [Google Scholar] [CrossRef] [PubMed]
- Giordano, M.; Ciarambino, T.; D’Amico, M.; Trotta, M.C.; Di Sette, A.M.; Marfella, R.; Malatino, L.; Paolisso, G.; Adinolfi, L.E. Circulating miRNA-195-5p and -451a in Transient and Acute Ischemic Stroke Patients in an Emergency Department. J. Clin. Med. 2019, 8, 130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giordano, M.; Trotta, M.C.; Ciarambino, T.; D’Amico, M.; Galdiero, M.; Schettini, F.; Paternosto, D.; Salzillo, M.; Alfano, R.; Andreone, V.; et al. Circulating miRNA-195-5p and -451a in Diabetic Patients with Transient and Acute Ischemic Stroke in the Emergency Department. Int. J. Mol. Sci. 2020, 21, 7615. [Google Scholar] [CrossRef] [PubMed]
- Tiedt, S.; Prestel, M.; Malik, R.; Schieferdecker, N.; Duering, M.; Kautzky, V.; Stoycheva, I.; Böck, J.; Northoff, B.H.; Klein, M.; et al. RNA-Seq Identifies Circulating MiR-125a-5p, MiR-125b-5p, and MiR-143-3p as Potential Biomarkers for Acute Ischemic Stroke. Circ. Res. 2017, 121, 970–980. [Google Scholar] [CrossRef]
- Chen, Y.; Song, Y.; Huang, J.; Qu, M.; Zhang, Y.; Geng, J.; Zhang, Z.; Liu, J.; Yang, G.-Y. Increased Circulating Exosomal miRNA-223 Is Associated with Acute Ischemic Stroke. Front. Neurol. 2017, 8, 57. [Google Scholar] [CrossRef] [Green Version]
- Aldous, E.K.; Toor, S.M.; Parray, A.; Al-Sarraj, Y.; Diboun, I.; Abdelalim, E.M.; Arredouani, A.; El-Agnaf, O.; Thornalley, P.J.; Akhtar, N.; et al. Identification of Novel Circulating miRNAs in Patients with Acute Ischemic Stroke. Int. J. Mol. Sci. 2022, 23, 3387. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, Y.; Huang, J.; Chen, X.; Gu, X.; Wang, Y.; Zeng, L.; Yang, G.-Y. Increase of Circulating MiR-223 and Insulin-like Growth Factor-1 Is Associated with the Pathogenesis of Acute Ischemic Stroke in Patients. BMC Neurol. 2014, 14, 77. [Google Scholar] [CrossRef] [Green Version]
- Jin, F.; Xing, J. Circulating MiR-126 and MiR-130a Levels Correlate with Lower Disease Risk, Disease Severity, and Reduced Inflammatory Cytokine Levels in Acute Ischemic Stroke Patients. Neurol. Sci. 2018, 39, 1757–1765. [Google Scholar] [CrossRef]
- Liu, P.; Han, Z.; Ma, Q.; Liu, T.; Wang, R.; Tao, Z.; Li, G.; Li, F.; Zhang, S.; Li, L.; et al. Upregulation of MicroRNA-128 in the Peripheral Blood of Acute Ischemic Stroke Patients Is Correlated with Stroke Severity Partially through Inhibition of Neuronal Cell Cycle Reentry. Cell Transpl. 2019, 28, 839–850. [Google Scholar] [CrossRef] [Green Version]
- Jia, L.; Hao, F.; Wang, W.; Qu, Y. Circulating MiR-145 Is Associated with Plasma High-Sensitivity C-Reactive Protein in Acute Ischemic Stroke Patients: Circulating MiR-145 in AIS. Cell Biochem. Funct. 2015, 33, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Cheng, X.; Kan, P.; Ma, Z.; Wang, Y.; Song, W.; Huang, C.; Zhang, B. Exploring the Potential Value of MiR-148b-3p, MiR-151b and MiR-27b-3p as Biomarkers in Acute Ischemic Stroke. Biosci. Rep. 2018, 38, BSR20181033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, B.; Zhu, Z.; Hao, J.; Wan, Z.; Guo, X. Decreased Plasma MiR-335 Expression in Patients with Acute Ischemic Stroke and Its Association with Calmodulin Expression. J. Int. Med. Res. 2016, 44, 1331–1338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sultan, W.; Machado, L.G.D.D.; Ali, M.G.; Tramontana, A.; Bayoumy, A.E.; Baxter, S.G.; Aly, M.R.A.; Bilotta, F. MicroRNAs as Biomarkers in Spontaneous Intracerebral Hemorrhage: A Systematic Review of Recent Clinical Evidence. Clin. Neurol. Neurosurg. 2022, 213, 107130. [Google Scholar] [CrossRef]
- Wang, J.; Zhu, Y.; Jin, F.; Tang, L.; He, Z.; He, Z. Differential Expression of Circulating MicroRNAs in Blood and Haematoma Samples from Patients with Intracerebral Haemorrhage. J. Int. Med. Res. 2016, 44, 419–432. [Google Scholar] [CrossRef] [Green Version]
- Fu, X.; Niu, T.; Li, X. MicroRNA-126-3p Attenuates Intracerebral Hemorrhage-Induced Blood-Brain Barrier Disruption by Regulating VCAM-1 Expression. Front. Neurosci. 2019, 13, 866. [Google Scholar] [CrossRef] [Green Version]
- Leung, L.Y.; Chan, C.P.Y.; Leung, Y.K.; Jiang, H.L.; Abrigo, J.M.; Wang, D.F.; Chung, J.S.H.; Rainer, T.H.; Graham, C.A. Comparison of MiR-124-3p and MiR-16 for Early Diagnosis of Hemorrhagic and Ischemic Stroke. Clin. Chim. Acta 2014, 433, 139–144. [Google Scholar] [CrossRef]
- Martinez, B.; Peplow, P. Blood MicroRNAs as Potential Diagnostic Markers for Hemorrhagic Stroke. Neural Regen. Res. 2017, 12, 13. [Google Scholar] [CrossRef]
- Zhu, Y.; Wang, J.-L.; He, Z.-Y.; Jin, F.; Tang, L. Association of Altered Serum MicroRNAs with Perihematomal Edema after Acute Intracerebral Hemorrhage. PLoS ONE 2015, 10, e0133783. [Google Scholar] [CrossRef]
- Sacco, R.L.; Kasner, S.E.; Broderick, J.P.; Caplan, L.R.; Connors, J.J.B.; Culebras, A.; Elkind, M.S.V.; George, M.G.; Hamdan, A.D.; Higashida, R.T.; et al. An Updated Definition of Stroke for the 21st Century: A Statement for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2013, 44, 2064–2089. [Google Scholar] [CrossRef] [Green Version]
- Yin, K.-J.; Hamblin, M.; Chen, Y.E. Angiogenesis-Regulating MicroRNAs and Ischemic Stroke. Curr. Vasc. Pharmacol. 2015, 13, 352–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, G.; Morris-Blanco, K.C.; Lopez, M.S.; Yang, T.; Zhao, H.; Vemuganti, R.; Luo, Y. Impact of MicroRNAs on Ischemic Stroke: From Pre- to Post-Disease. Prog. Neurobiol. 2018, 163–164, 59–78. [Google Scholar] [CrossRef] [PubMed]
- Atif, H.; Hicks, S.D. A Review of MicroRNA Biomarkers in Traumatic Brain Injury. J. Exp. Neurosci. 2019, 13, 1179069519832286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, Y.; Zhang, Z.; Wang, Z.; Liu, J. miRNA-27b Regulates Angiogenesis by Targeting AMPK in Mouse Ischemic Stroke Model. Neuroscience 2019, 398, 12–22. [Google Scholar] [CrossRef]
- Gugliandolo, A.; Silvestro, S.; Sindona, C.; Bramanti, P.; Mazzon, E. miRNA: Involvement of the MAPK Pathway in Ischemic Stroke. A Promising Therapeutic Target. Medicina 2021, 57, 1053. [Google Scholar] [CrossRef]
- Pignataro, G. Emerging Role of MicroRNAs in Stroke Protection Elicited by Remote Postconditioning. Front. Neurol. 2021, 12, 748709. [Google Scholar] [CrossRef]
- Saif, J.; Emanueli, C. miRNAs in Post-Ischaemic Angiogenesis and Vascular Remodelling. Biochem. Soc. Trans. 2014, 42, 1629–1636. [Google Scholar] [CrossRef]
- Dewdney, B.; Trollope, A.; Moxon, J.; Thomas Manapurathe, D.; Biros, E.; Golledge, J. Circulating MicroRNAs as Biomarkers for Acute Ischemic Stroke: A Systematic Review. J. Stroke Cerebrovasc. Dis. 2018, 27, 522–530. [Google Scholar] [CrossRef]
- Sun, S.; Li, L.; Dong, L.; Cheng, J.; Zhao, C.; Bao, C.; Wang, H. Circulating MRNA and MicroRNA Profiling Analysis in Patients with Ischemic Stroke. Mol. Med. Rep. 2020, 22, 792–802. [Google Scholar] [CrossRef]
- Liu, H.M. Neovasculature and Blood-Brain Barrier in Ischemic Brain Infarct. Acta Neuropathol. 1988, 75, 422–426. [Google Scholar] [CrossRef]
- Chen, H.H.; Chien, C.H.; Liu, H.M. Correlation between Angiogenesis and Basic Fibroblast Growth Factor Expression in Experimental Brain Infarct. Stroke 1994, 25, 1651–1657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krupinski, J.; Kaluza, J.; Kumar, P.; Kumar, S.; Wang, J.M. Role of Angiogenesis in Patients with Cerebral Ischemic Stroke. Stroke 1994, 25, 1794–1798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, M.Y.; Ju, W.K.; Cha, J.H.; Son, B.C.; Chun, M.H.; Kang, J.K.; Park, C.K. Expression of Vascular Endothelial Growth Factor MRNA Following Transient Forebrain Ischemia in Rats. Neurosci. Lett. 1999, 265, 107–110. [Google Scholar] [CrossRef]
- Jin, K.L.; Mao, X.O.; Nagayama, T.; Goldsmith, P.C.; Greenberg, D.A. Induction of Vascular Endothelial Growth Factor and Hypoxia-Inducible Factor-1alpha by Global Ischemia in Rat Brain. Neuroscience 2000, 99, 577–585. [Google Scholar] [CrossRef]
- Gu, W.; Brännström, T.; Jiang, W.; Bergh, A.; Wester, P. Vascular Endothelial Growth Factor-A and -C Protein up-Regulation and Early Angiogenesis in a Rat Photothrombotic Ring Stroke Model with Spontaneous Reperfusion. Acta Neuropathol. 2001, 102, 216–226. [Google Scholar] [CrossRef]
- Xiong, Y.; Mahmood, A.; Chopp, M. Angiogenesis, Neurogenesis and Brain Recovery of Function Following Injury. Curr. Opin. Investig. Drugs 2010, 11, 298–308. [Google Scholar]
- Ergul, A.; Alhusban, A.; Fagan, S.C. Angiogenesis: A Harmonized Target for Recovery after Stroke. Stroke 2012, 43, 2270–2274. [Google Scholar] [CrossRef] [Green Version]
- Greenberg, D.A.; Jin, K. Vascular Endothelial Growth Factors (VEGFs) and Stroke. Cell. Mol. Life Sci. 2013, 70, 1753–1761. [Google Scholar] [CrossRef]
- Liu, J.; Wang, Y.; Akamatsu, Y.; Lee, C.C.; Stetler, R.A.; Lawton, M.T.; Yang, G.-Y. Vascular Remodeling after Ischemic Stroke: Mechanisms and Therapeutic Potentials. Prog. Neurobiol. 2014, 115, 138–156. [Google Scholar] [CrossRef] [Green Version]
- Cosky, E.E.P.; Ding, Y. The Role of Vascular Endothelial Growth Factor in Angiogenesis and Brain Circulation after Stroke. Brain Circ. 2018, 4, 73–75. [Google Scholar] [CrossRef]
- Beck, H.; Plate, K.H. Angiogenesis after Cerebral Ischemia. Acta Neuropathol. 2009, 117, 481–496. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Lawes, C.M.M.; Bennett, D.A.; Barker-Collo, S.L.; Parag, V. Worldwide Stroke Incidence and Early Case Fatality Reported in 56 Population-Based Studies: A Systematic Review. Lancet Neurol. 2009, 8, 355–369. [Google Scholar] [CrossRef]
- Hemphill, J.C.; Greenberg, S.M.; Anderson, C.S.; Becker, K.; Bendok, B.R.; Cushman, M.; Fung, G.L.; Goldstein, J.N.; Macdonald, R.L.; Mitchell, P.H.; et al. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2015, 46, 2032–2060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toyoda, K.; Koga, M.; Iguchi, Y.; Itabashi, R.; Inoue, M.; Okada, Y.; Ogasawara, K.; Tsujino, A.; Hasegawa, Y.; Hatano, T.; et al. Guidelines for Intravenous Thrombolysis (Recombinant Tissue-Type Plasminogen Activator), the Third Edition, March 2019: A Guideline from the Japan Stroke Society. Neurol. Med. Chir. 2019, 59, 449–491. [Google Scholar] [CrossRef] [Green Version]
- Broderick, J.P.; Adeoye, O.; Elm, J. Evolution of the Modified Rankin Scale and Its Use in Future Stroke Trials. Stroke 2017, 48, 2007–2012. [Google Scholar] [CrossRef]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. 2018 Guidelines for the Early Management of Patients With Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2018, 49, e46–e110. [Google Scholar] [CrossRef]
- Cheng, H.-Y.; Wang, Y.-S.; Hsu, P.-Y.; Chen, C.-Y.; Liao, Y.-C.; Juo, S.-H.H. MiR-195 Has a Potential to Treat Ischemic and Hemorrhagic Stroke through Neurovascular Protection and Neurogenesis. Mol. Ther. Methods Clin. Dev. 2019, 13, 121–132. [Google Scholar] [CrossRef] [Green Version]
- Stylli, S.S.; Adamides, A.A.; Koldej, R.M.; Luwor, R.B.; Ritchie, D.S.; Ziogas, J.; Kaye, A.H. miRNA Expression Profiling of Cerebrospinal Fluid in Patients with Aneurysmal Subarachnoid Hemorrhage. J. Neurosurg. 2017, 126, 1131–1139. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Zhang, A.; Xiang, J.; Lv, Y.; Zhang, X. MiR-451 Acts as a Suppressor of Angiogenesis in Hepatocellular Carcinoma by Targeting the IL-6R-STAT3 Pathway. Oncol. Rep. 2016, 36, 1385–1392. [Google Scholar] [CrossRef]
- Zhao, W.-J.; Zhang, H.-F.; Su, J.-Y. Downregulation of MicroRNA-195 Promotes Angiogenesis Induced by Cerebral Infarction via Targeting VEGFA. Mol. Med. Rep. 2017, 16, 5434–5440. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| C | ICH | AIS | p Value | |
|---|---|---|---|---|
| N (M) | 21 (10) | 21 (11) | 20 (9) | ns |
| Age (years) | 69 ± 2 | 68 ± 3 | 73 ± 5 | ns |
| BMI (kg/m2) | 27 ± 2 | 25 ± 5 | 26 ± 4 | ns |
| SBP (mmHg) | 142 ± 6 | 141 ± 7 | 139 ± 5 | ns |
| DBP (mmHg) | 81 ± 2 | 85 ± 5 | 82 ± 3 | ns |
| Hypertension (%) | 9 (43) | 11 (52) | 9 (45) | ns |
| Smoking (%) | (25) | (35) | (35) | ns |
| Hyperlipidemia (%) | (40) | (45) | (50) | ns |
| NIHSS score | - | 15 ± 1.4 | 16 ± 1.6 | ns * |
| Modified Rankin scale | - | 3.7 ± 0.4 | 3.5 ± 0.3 | ns * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giordano, M.; Trotta, M.C.; Ciarambino, T.; D’Amico, M.; Schettini, F.; Sisto, A.D.; D’Auria, V.; Voza, A.; Malatino, L.S.; Biolo, G.; et al. Circulating miRNA-195-5p and -451a in Patients with Acute Hemorrhagic Stroke in Emergency Department. Life 2022, 12, 763. https://doi.org/10.3390/life12050763
Giordano M, Trotta MC, Ciarambino T, D’Amico M, Schettini F, Sisto AD, D’Auria V, Voza A, Malatino LS, Biolo G, et al. Circulating miRNA-195-5p and -451a in Patients with Acute Hemorrhagic Stroke in Emergency Department. Life. 2022; 12(5):763. https://doi.org/10.3390/life12050763
Chicago/Turabian StyleGiordano, Mauro, Maria Consiglia Trotta, Tiziana Ciarambino, Michele D’Amico, Federico Schettini, Angela Di Sisto, Valentina D’Auria, Antonio Voza, Lorenzo Salvatore Malatino, Gianni Biolo, and et al. 2022. "Circulating miRNA-195-5p and -451a in Patients with Acute Hemorrhagic Stroke in Emergency Department" Life 12, no. 5: 763. https://doi.org/10.3390/life12050763
APA StyleGiordano, M., Trotta, M. C., Ciarambino, T., D’Amico, M., Schettini, F., Sisto, A. D., D’Auria, V., Voza, A., Malatino, L. S., Biolo, G., Mearelli, F., Franceschi, F., Paolisso, G., & Adinolfi, L. E. (2022). Circulating miRNA-195-5p and -451a in Patients with Acute Hemorrhagic Stroke in Emergency Department. Life, 12(5), 763. https://doi.org/10.3390/life12050763