
Anti-Inflammatory, Antioxidant, and Anti-Atherosclerotic Effects of Natural Supplements on Patients with FMF-Related AA Amyloidosis: A Non-Randomized 24-Week Open-Label Interventional Study

 ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
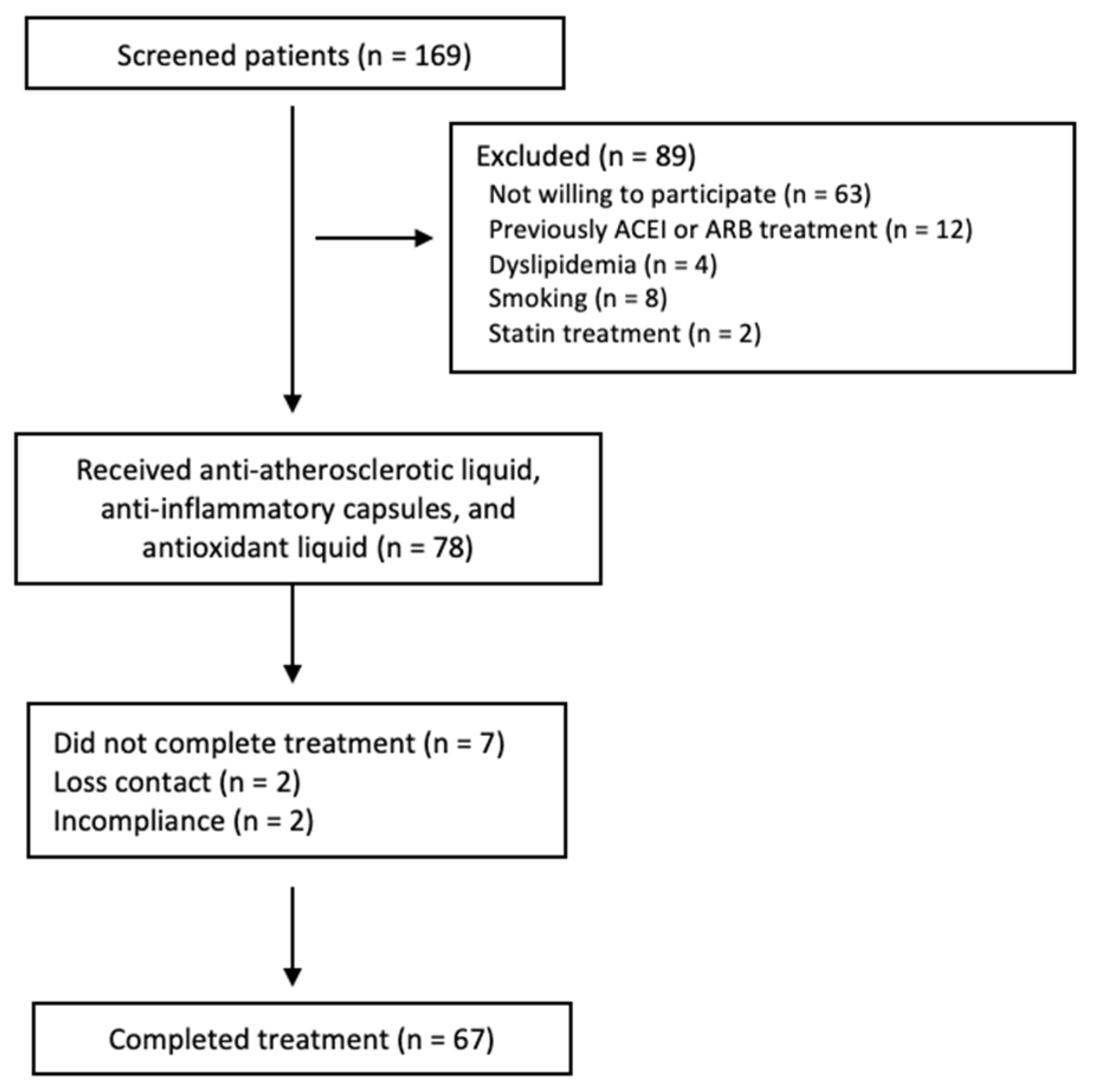
2.1. Patients
2.2. Intervention
2.3. Study Endpoints
2.4. Clinical and Cardiovascular Assessment
2.5. Assessment of Endothelial Dysfunction
2.6. Carotid-Intima-Media Thickness (CIMT)
2.7. Laboratory Measurements
2.8. Statistical Methods
3. Results
3.1. Baseline Characteristics
3.2. Effect of AAL, AIC, and AOL on FMD and Inflammation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bhat, A.; Naguwa, S.M.; Gershwin, M.E. Genetics and New Treatment Modalities for Familial Mediterranean Fever. Ann. N. Y. Acad. Sci. 2007, 1110, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Siligato, R.; Gembillo, G.; Calabrese, V.; Conti, G.; Santoro, D. Amyloidosis and Glomerular Diseases in Familial Mediterranean Fever. Medicina 2021, 57, 1049. [Google Scholar] [CrossRef] [PubMed]
- Ediz, L.; Ozkol, H.; Tekeoglu, I.; Tuluce, Y.; Gulcu, E.; Koyuncu, I. Increased oxidative stress in patients with familial Mediterranean fever during attack period. Afr. Health Sci. 2011, 11 (Suppl. S1), S6–S13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gurbuz, M.; Yamanel, L.; Bulucu, F.; Inal, V.; Aydin, A. Oxidative stress status in familial Mediterranean fever with or without proteinuria. Free Radic. Biol. Med. 2005, 38, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Guzel, S.; Andican, G.; Seven, A.; Aslan, M.; Bolayirli, M.; Guzel, E.C. Acute phase response and oxidative stress status in familial Mediterranean fever (FMF). Mod. Rheumatol. 2012, 22, 431–437. [Google Scholar] [CrossRef]
- Karaguezyan, K.G.; Haroutjunian, V.M.; Mamiconyan, R.S.; Hakobian, G.S.; Nazaretian, E.E.; Hovsepyan, L.M.; Hoveyan, G.A.; Gevorkian, E.M.; Hovakimyan, S.S.; Zakarian, A.E.; et al. Evidence of oxidative stress in erythrocyte phospholipid composition in the pathogenesis of familial Mediterranean fever (periodical disease). J. Clin. Pathol. 1996, 49, 453–455. [Google Scholar] [CrossRef] [Green Version]
- Kirkali, G.; Tunca, M.; Genc, S.; Jaruga, P.; Dizdaroglu, M. Oxidative DNA damage in polymorphonuclear leukocytes of patients with familial Mediterranean fever. Free Radic. Biol. Med. 2008, 44, 386–393. [Google Scholar] [CrossRef]
- Joffre, J.; Hellman, J. Oxidative Stress and Endothelial Dysfunction in Sepsis and Acute Inflammation. Antioxid. Redox Signal. 2021, 35, 1291–1307. [Google Scholar] [CrossRef]
- Dinç, G.; Fentoğlu, Ö.; Dogru, A.; Ilhan, I.; Kırzıoğlu, F.Y.; Orhan, H. The evaluation of salivary oxidative stress in patients with familial Mediterranean fever and chronic periodontitis. J. Periodontol. 2018, 89, 1112–1120. [Google Scholar] [CrossRef]
- Ugurlu, S.; Seyahi, E.; Cetinkaya, F.; Ozbakır, F.; Balci, H.; Ozdogan, H. Intima-media thickening in patients with familial Mediterranean fever. Rheumatology 2009, 48, 911–915. [Google Scholar] [CrossRef] [Green Version]
- Yilmaz, M.I.; Demirkaya, E.; Acikel, C.; Saldir, M.; Akar, S.; Cayci, T.; Saglam, M.; Unal, H.U.; Gok, M.; Polat, A.; et al. Endothelial function in patients with familial Mediterranean fever-related amyloidosis and association with cardiovascular events. Rheumatology 2014, 53, 2002–2008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozalper, V.; Kara, M.; Tanoglu, A.; Cetındaglı, I.; Ozturker, C.; Hancerlı, Y.; Hıra, S.; Kara, K.; Beyazıt, Y.; Yazgan, Y. Evaluation of endothelial dysfunction in patients with familial Mediterranean fever: The relationship between the levels of asymmetric dimethylarginine and endocan with carotid intima–media thickness and endothelium-dependent vasodilation. Clin. Rheumatol. 2017, 36, 2071–2077. [Google Scholar] [CrossRef] [PubMed]
- Bilginer, Y.; Ozaltin, F.; Basaran, C.; Duzova, A.; Besbas, N.; Topaloglu, R.; Ozen, S.; Bakkaloglu, A. Evaluation of intima media thickness of the common and internal carotid arteries with inflammatory markers in familial Mediterranean fever as possible predictors for atherosclerosis. Rheumatol. Int. 2008, 28, 1211–1216. [Google Scholar] [CrossRef]
- Dinarello, C.A. Interleukin-1 in the pathogenesis and treatment of inflammatory diseases. Blood 2011, 117, 3720–3732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ikonomidis, I.; Tzortzis, S.; Andreadou, I.; Paraskevaidis, I.; Katseli, C.; Katsimbri, P.; Pavlidis, G.; Parissis, J.; Kremastinos, D.; Anastasiou-Nana, M.; et al. Increased Benefit of Interleukin-1 Inhibition on Vascular Function, Myocardial Deformation, and Twisting in Patients With Coronary Artery Disease and Coexisting Rheumatoid Arthritis. Circ. Cardiovasc. Imaging 2014, 7, 619–628. [Google Scholar] [CrossRef] [Green Version]
- Pinney, J.H.; Hawkins, P.N. Amyloidosis. Ann. Clin. Biochem. 2012, 49, 229–241. [Google Scholar] [CrossRef] [Green Version]
- Twig, G.; Livneh, A.; Vivante, A.; Afek, A.; Shamiss, A.; Derazne, E.; Tzur, D.; Ben-Zvi, I.; Tirosh, A.; Barchana, M.; et al. Mortality risk factors associated with familial Mediterranean fever among a cohort of 1.25 million adolescents. Ann. Rheum. Dis. 2013, 73, 704–709. [Google Scholar] [CrossRef]
- Romano, M.; Piskin, D.; Berard, R.A.; Jackson, B.C.; Acikel, C.; Carrero, J.J.; Lachmann, H.J.; Yilmaz, M.I.; Demirkaya, E. Cardiovascular disease risk assessment in patients with familial Mediterranean fever related renal amyloidosis. Sci. Rep. 2020, 10, 18374. [Google Scholar] [CrossRef]
- Brown, A.C. Anticancer Activity of Morinda citrifolia (Noni) Fruit: A Review. Phytother. Res. 2012, 26, 1427–1440. [Google Scholar] [CrossRef]
- El-Abhar, H.S.; Schaalan, M.F. Phytotherapy in diabetes: Review on potential mechanistic perspectives. World J. Diabetes 2014, 5, 176–197. [Google Scholar] [CrossRef]
- Krupanidhi, S.; Sanjeevi, C.B. Omega-3 Fatty Acids for Nutrition and Medicine: Considering Microalgae Oil as a Vegetarian Source of EPA and DHA. Curr. Diabetes Rev. 2007, 3, 198–203. [Google Scholar] [CrossRef]
- Faria, A.; Oliveira, J.; Neves, P.; Gameiro, P.; Santos-Buelga, C.; de Freitas, V.; Mateus, N. Antioxidant Properties of Prepared Blueberry (Vaccinium myrtillus) Extracts. J. Agric. Food Chem. 2005, 53, 6896–6902. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Wang, T.T.Y.; Prior, R.L.; Pehrsson, P.R. Prevention of Atherosclerosis by Berries: The Case of Blueberries. J. Agric. Food Chem. 2018, 66, 9172–9188. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, M.I.; Romano, M.; Basarali, M.K.; Elzagallaai, A.; Karaman, M.; Demir, Z.; Demir, M.F.; Akcay, F.; Seyrek, M.; Haksever, N.; et al. The Effect of Corrected Inflammation, Oxidative Stress and Endothelial Dysfunction on Fmd Levels in Patients with Selected Chronic Diseases: A Quasi-Experimental Study. Sci. Rep. 2020, 10, 9018. [Google Scholar] [CrossRef]
- Arici, Z.; Romano, M.; Piskin, D.; Guzel, F.; Sahin, S.; Berard, R.; Yilmaz, M.; Demirkaya, E. Evaluation of E148Q and Concomitant AA Amyloidosis in Patients with Familial Mediterranean Fever. J. Clin. Med. 2021, 10, 3511. [Google Scholar] [CrossRef]
- Demirkaya, E.; Saglam, C.; Turker, T.; Koné-Paut, I.; Woo, P.; Doglio, M.; Amaryan, G.; Frenkel, J.; Uziel, Y.; Insalaco, A.; et al. Performance of Different Diagnostic Criteria for Familial Mediterranean Fever in Children with Periodic Fevers: Results from a Multicenter International Registry. J. Rheumatol. 2015, 43, 154–160. [Google Scholar] [CrossRef]
- Des Jarlais, D.C.; Lyles, C.; Crepaz, N.; the TREND Group. Improving the Reporting Quality of Nonrandomized Evaluations of Behavioral and Public Health Interventions: The TREND Statement. Am. J. Public Health 2004, 94, 361–366. [Google Scholar] [CrossRef]
- Bärnighausen, T.; Røttingen, J.-A.; Rockers, P.; Shemilt, I.; Tugwell, P. Quasi-experimental study designs series—paper 1: Introduction: Two historical lineages. J. Clin. Epidemiol. 2017, 89, 4–11. [Google Scholar] [CrossRef]
- Celermajer, D.; Sorensen, K.; Gooch, V.; Spiegelhalter, D.; Miller, O.; Sullivan, I.; Lloyd, J.; Deanfield, J. Non-invasive detection of endothelial dysfunction in children and adults at risk of atherosclerosis. Lancet 1992, 340, 1111–1115. [Google Scholar] [CrossRef]
- Chen, B.M.; Xia, L.W.; Zhao, R.Q. Determination of N(G),N(G)-dimethylarginine in human plasma by high-performance liquid chromatography. J. Chromatogr. B Biomed. Sci. Appl. 1997, 692, 467–471. [Google Scholar] [CrossRef]
- Aydın, A.; Orhan, H.; Sayal, A.; Özata, M.; Şahin, G.; Işımer, A. Oxidative stress and nitric oxide related parameters in type II diabetes mellitus: Effects of glycemic control. Clin. Biochem. 2001, 34, 65–70. [Google Scholar] [CrossRef]
- Jain, S.K. Hyperglycemia can cause membrane lipid peroxidation and osmotic fragility in human red blood cells. J. Biol. Chem. 1989, 264, 21340–21345. [Google Scholar] [CrossRef]
- Hull, K.M.; Kastner, D.L.; Balow, J.E. Hereditary periodic fever. N. Engl. J. Med. 2002, 346, 1415–1416. [Google Scholar] [PubMed]
- Mafra, D.; Borges, N.A.; Lindholm, B.; Shiels, P.G.; Evenepoel, P.; Stenvinkel, P. Food as medicine: Targeting the uraemic phenotype in chronic kidney disease. Nat. Rev. Nephrol. 2020, 17, 153–171. [Google Scholar] [CrossRef] [PubMed]
- Ozen, S.; Demirkaya, E.; Amaryan, G.; Koné-Paut, I.; Polat, A.; Woo, P.; Uziel, Y.; Modesto, C.; Finetti, M.; Quartier, P.; et al. Results from a multicentre international registry of familial Mediterranean fever: Impact of environment on the expression of a monogenic disease in children. Ann. Rheum. Dis. 2013, 73, 662–667. [Google Scholar] [CrossRef] [PubMed]
- Caliskan, M.; Gullu, H.; Yilmaz, S.; Erdogan, D.; Unler, G.K.; Ciftci, O.; Topcu, S.; Kayhan, Z.; Yucel, E.; Muderrisoglu, H. Impaired coronary microvascular function in familial Mediterranean fever. Atherosclerosis 2007, 195, e161–e167. [Google Scholar] [CrossRef]
- Terekeci, H.M.; Oktenli, C.; Ozgurtas, T.; Nalbant, S.; Top, C.; Celik, S.; Tapan, S.; Kucukardali, Y.; Sanisoglu, Y.S.; Solmazgul, E.; et al. Increased asymmetric dimethylarginine levels in young men with familial Mediterranean fever (FMF): Is it early evidence of interaction between inflammation and endothelial dysfunction in FMF? J. Rheumatol. 2008, 35, 2024–2029. [Google Scholar]
- Peru, H.; Altun, B.; Doğan, M.; Kara, F.; Elmaci, A.M.; Oran, B. The evaluation of carotid intima-media thickness in children with familial Mediterranean fever. Clin. Rheumatol. 2007, 27, 689–694. [Google Scholar] [CrossRef]
- Procopio, V.; Manti, S.; Bianco, G.; Conti, G.; Romeo, A.; Maimone, F.; Arrigo, T.; Cutrupi, M.C.; Salpietro, C.; Cuppari, C. Genotype-phenotype correlation in FMF patients: A “non classic” recessive autosomal or “atypical” dominant autosomal inheritance? Gene 2018, 641, 279–286. [Google Scholar] [CrossRef]
- Sari, I.; Karaoglu, O.; Can, G.; Akar, S.; Gulcu, A.; Birlik, M.; Akkoc, N.; Tunca, M.; Goktay, Y.; Onen, F. Early ultrasonographic markers of atherosclerosis in patients with familial Mediterranean fever. Clin. Rheumatol. 2007, 26, 1467–1473. [Google Scholar] [CrossRef]
- Böger, R.H.; Schwedhelm, E.; Maas, R.; Quispe-Bravo, S.; Skamira, C. ADMA and oxidative stress may relate to the progression of renal disease: Rationale and design of the VIVALDI study. Vasc. Med. 2005, 10 (Suppl. S1), S97–S102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Triches, C.B.; Quinto, M.; Mayer, S.; Batista, M.; Zanella, M.T. Relation of asymmetrical dimethylarginine levels with renal outcomes in hypertensive patients with and without type 2 diabetes mellitus. J. Diabetes Its Complicat. 2017, 32, 316–320. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Mehrotra, P.; Basile, D.; Ullah, M.; Singh, A.; Skill, N.; Younes, S.T.; Sasser, J.; Shekhar, A.; Singh, J. Specific Lowering of Asymmetric Dimethylarginine by Pharmacological Dimethylarginine Dimethylaminohydrolase Improves Endothelial Function, Reduces Blood Pressure and Ischemia-Reperfusion Injury. J. Pharmacol. Exp. Ther. 2020, 376, 181–189. [Google Scholar] [CrossRef]
- Stenvinkel, P.; Chertow, G.M.; Devarajan, P.; Levin, A.; Andreoli, S.P.; Bangalore, S.; Warady, B.A. Chronic Inflammation in Chronic Kidney Disease Progression: Role of Nrf2. Kidney Int. Rep. 2021, 6, 1775–1787. [Google Scholar] [CrossRef] [PubMed]
- Barton, P.; Andronis, L.; Briggs, A.; McPherson, K.; Capewell, S. Effectiveness and cost effectiveness of cardiovascular disease prevention in whole populations: Modelling study. BMJ 2011, 343, d4044. [Google Scholar] [CrossRef] [Green Version]
- Ben-Chetrit, E.; Touitou, I. Familial Mediterranean Fever in the World. Arthritis Care Res. 2009, 61, 1447–1453. [Google Scholar] [CrossRef]
- Yilmaz, M.I.; Sonmez, A.; Saglam, M.; Qureshi, A.R.; Carrero, J.J.; Caglar, K.; Eyileten, T.; Cakir, E.; Oguz, Y.; Vural, A.; et al. ADMA Levels Correlate with Proteinuria, Secondary Amyloidosis, and Endothelial Dysfunction. J. Am. Soc. Nephrol. 2008, 19, 388–395. [Google Scholar] [CrossRef] [Green Version]
- Güçlü, A.; Yilmaz, M.I.; Tokmak, T.T.; Unal, H.U.; Karaman, M.; Gezer, M.; Taş, A.; Aydin, I.; Akçılar, R.; Dursun, Y. Chitotriosidase as a novel biomarker of early atherosclerosis in hemodialysis patients. Hemodial. Int. 2016, 21, 41–46. [Google Scholar] [CrossRef]
- Kocyigit, I.; Yilmaz, M.I.; Gungor, O.; Eroglu, E.; Unal, A.; Orscelik, O.; Tokgoz, B.; Sipahioglu, M.; Sen, A.; Carrero, J.J.; et al. Vasopressin-related copeptin is a novel predictor of early endothelial dysfunction in patients with adult polycystic kidney disease. BMC Nephrol. 2016, 17, 196. [Google Scholar] [CrossRef] [Green Version]
- Yilmaz, M.I.; Siriopol, D.; Saglam, M.; Ünal, H.U.; Karaman, M.; Gezer, M.; Kilinc, A.; Eyileten, T.; Guler, A.K.; Aydin, I.; et al. Osteoprotegerin in Chronic Kidney Disease: Associations with Vascular Damage and Cardiovascular Events. Calcif. Tissue Res. 2016, 99, 121–130. [Google Scholar] [CrossRef]
- Nowak, J.; Nilsson, T.; Sylvén, C.; Jogestrand, T. Potential of carotid ultrasonography in the diagnosis of coronary artery disease: A comparison with exercise test and variance ECG. Stroke 1998, 29, 439–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stenvinkel, P.; Heimbürger, O.; Paultre, F.; Diczfalusy, U.; Wang, T.; Berglund, L.; Jogestrand, T. Strong association between malnutrition, inflammation, and atherosclerosis in chronic renal failure. Kidney Int. 1999, 55, 1899–1911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, M.D.; Dizdaroglu, M.; Cooke, M.S. Oxidative DNA damage and disease: Induction, repair and significance. Mutat. Res. Mutat. Res. 2004, 567, 1–61. [Google Scholar] [CrossRef] [PubMed]
- Ando, Y.; Nyhlinb, N.; Suhrb, O.; Holmgren, G.; Uchidad, K.; El Sahly, M.; Yamashitaa, T.; Terasakia, H.; Nakamuraa, M.; Uchinoe, M.; et al. Oxidative Stress Is Found in Amyloid Deposits in Systemic Amyloidosis. Biochem. Biophys. Res. Commun. 1997, 232, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Sarkisian, T.; Emerit, I.; Arutyunyan, R.; Levy, A.; Cernjavski, L.; Filipe, P. Familial Mediterranean fever: Clastogenic plasma factors correlated with increased O2(-)—Production by neu-trophils. Hum. Genet. 1997, 101, 238–242. [Google Scholar] [CrossRef]
- Ichikawa, I.; Kiyama, S.; Yoshioka, T. Renal antioxidant enzymes: Their regulation and function. Kidney Int. 1994, 45, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Langevitz, P.; Livneh, A.; Neumann, L.; Buskila, D.; Shemer, J.; Amolsky, D.; Pras, M. Prevalence of ischemic heart disease in patients with familial Mediterranean fever. Isr. Med Assoc. J. IMAJ 2001, 3, 9–12. [Google Scholar]
- Pantaler, E.; Lückhoff, A. Inhibitors of TRP channels reveal stimulus-dependent differential activation of Ca2+ influx pathways in human neutrophil granulocytes. Naunyn-Schmiedebergs Arch. Exp. Pathol. Pharmakol. 2009, 380, 497–507. [Google Scholar] [CrossRef]
- Şahin, M.; Uğuz, A.C.; Demirkan, H.; Nazıroğlu, M. Colchicine Modulates Oxidative Stress in Serum and Leucocytes from Remission Patients with Family Mediterranean Fever Through Regulation of Ca2+ Release and the Antioxidant System. J. Membr. Biol. 2011, 240, 55–62. [Google Scholar] [CrossRef]
- Modriansky, M.; Tyurina, Y.Y.; Tyurin, V.A.; TatsuyaMatsura; Shvedova, A.A.; Yalowich, J.C.; Kagan, V.E. Anti-/pro-oxidant effects of phenolic compounds in cells: Are colchicine metabolites chain-breaking antioxi-dants? Toxicology 2002, 177, 105–117. [Google Scholar] [CrossRef]


{kind=link}
| Demographic and Clinical Features | |
|---|---|
| Gender (male, n, %) | 52 (77.6%) |
| Current age, year (median, range) | 36 (21–66) |
| Age at FMF diagnosis, year (median, range) | 16 (6–26) |
| Age at Amyloidosis diagnosis, year (median, range) | 24 (17–48) |
| BMI (kg/m2) (mean, SD) | 25.3 ± 2.4 |
| Systolic blood pressure (SBP) (mmHg) (mean, SD) | 139 ± 15 |
| Diastolic blood pressure (DBP) (mmHg) (mean, SD) | 86 ± 9 |
| Colchicine usage (n, %) | 56 (83.6%) |
| MEFV Alleles frequency (n, %) | |
| M694V | 97 (74%) |
| M680I | 13 (9.9%) |
| E148Q | 11 (8.4%) |
| V726A | 5 (3.8%) |
| M694I | 4 (3.1%) |
| L695A | 1 (0.8%) |
| Total | 131 (100%) |
| Clinical Feature (n = 67) | n (%) |
|---|---|
| Fever | 59 (88.1) |
| Abdominal pain | 46 (68.7) |
| Arthritis | 45 (67.2) |
| Chest pain | 33 (50.3) |
| Arthralgia | 26 (38.8) |
| Myalgia | 17 (25.3) |
| Erysipelas like erythema | 16 (23.9) |
| Diarrhea | 11 (16.4) |
| Vomiting | 8 (11.9) |
| Protracted febrile myalgia | 5 (7.5) |
| Pericarditis | 3 (4.5) |
| Complications (n = 67) | |
| Appendectomy | 29 (43.3) |
| Splenomegaly | 16 (23.9) |
| Peritoneal adhesion | 5 (7.5) |
| Intestinal occlusion | 5 (7.5) |
| Thrombosis | 3 (4.5) |
| Acute orchitis | 3 (4.5) |
| AAL, AIC and AOL Therapies (n = 67) | ||||
|---|---|---|---|---|
| Baseline | 24th Week | ∆ | p | |
| FMD (%) | 5.0 ± 0.7 | 6.4 ± 0.8 ** | 1.3 ± 0.9 | <0.001 |
| CIMT (mm) | 0.9 ± 0.2 | 0.7 ± 0.1 | −0.2 ± 0.2 | <0.001 |
| hs-CRP (mg/L) | 25.5 (4.4–48.0) | 3.0 (1.0–9.1) * | −21.6 (−11.4–0.4) | <0.001 |
| PTX3 (ng/mL) | 13.4 (2.3–67.0) | 2.3 (0.4–14.5) * | −10.4 (−66.2–3.14) | <0.001 |
| Serum Amyloid A (mg/dL) | 6.6 ± 2.2 | 2.7 ± 1.7 | −3.8 ± 2.6 | <0.001 |
| Total Cholesterol (mg/dL) | 221.2 ± 60.3 | 155.8 ± 35.4 ** | −65.3 ± 55.5 | <0.001 |
| Triglycerides (mg/dL) | 145.7 ± 36.7 | 139.7 ± 20.3 ** | −6.1 ± 34.5 | 0.15 |
| LDL-cholesterol (mg/dL) | 131.7 ± 26.4 | 119.7 ± 17.8 ** | −12.1 ± 23.5 | <0.001 |
| HDL-cholesterol (mg/dL) | 38.8 ± 6.2 | 45.4 ± 4.6 ** | 6.6 ± 7.6 | <0.001 |
| eGFR (mL/min/1.73 m2) | 110.2 ± 12.8 | 104.1 ± 11.2 ** | −6.1 ± 11.9 | <0.001 |
| HOMA-IR | 1.6 ± 0.8 | 1.2 ± 0.4 ** | −0.44 ± 0.87 | <0.001 |
| Serum albumin (g/dL) | 3.6 ± 0.2 | 4.0 ± 0.4 ** | 0.4 ± 0.5 | <0.001 |
| MDA (nmol/mL) | 4.2 ± 1.8 | 1.8 ± 0.5 ** | −2.2 ± 1.8 | <0.001 |
| CuZn-SOD (U/mL) | 431.5 ± 154.7 | 538.1 ± 146.4 ** | 159.7 ± 211.8 | <0.001 |
| GSH-Px (U/mL) | 47.8 ± 13.2 | 74.1 ± 20.3 ** | 26.3 ± 21.1 | <0.001 |
| ADMA (µmol/L) | 4.5 ± 2.6 | 1.3 ± 0.6 ** | −3.2 ± 2.5 | <0.001 |
| Proteinuria (mg/24 h) | 6856 ± 3117 | 4090 ± 2360 | −2776 ± 2875 | <0.001 |
| Pearson Correlation | ∆FMD | ∆Proteinuria | ∆CIMT | ∆Cholesterol | ∆MDA | ∆hsCRP | ∆ptx3 | |
|---|---|---|---|---|---|---|---|---|
| ∆proteinuria | r | −0.533 | 1 | |||||
| p | <0.001 | |||||||
| ∆CIMT | r | −0.373 | 0.320 | 1 | ||||
| p | 0.002 | 0.008 | ||||||
| ∆Cholesterol | r | −0.263 | 0.479 | 0.389 | 1 | |||
| p | 0.031 | <0.001 | 0.001 | |||||
| ∆MDA | r | −0.384 | 0.409 | 0.485 | 0.407 | 1 | ||
| p | 0.001 | 0.001 | <0.001 | 0.001 | ||||
| ∆hsCRP | r | −0.476 | 0.414 | 0.460 | 0.554 | 0.648 | 1 | |
| p | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | |||
| ∆PTX3 | r | −0.497 | 0.363 | 0.477 | 0.563 | 0.682 | 0.652 | 1 |
| p | <0.001 | 0.003 | <0.001 | <0.001 | <0.001 | <0.001 | ||
| ∆ADMA | r | −0.485 | 0.406 | 0.440 | 0.577 | 0.693 | 0.562 | 0.717 |
| p | <0.001 | 0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romano, M.; Garcia-Bournissen, F.; Piskin, D.; Rodoplu, U.; Piskin, L.; Elzagallaai, A.A.; Tuncer, T.; Sezer, S.; Ucuncuoglu, D.; Honca, T.; et al. Anti-Inflammatory, Antioxidant, and Anti-Atherosclerotic Effects of Natural Supplements on Patients with FMF-Related AA Amyloidosis: A Non-Randomized 24-Week Open-Label Interventional Study. Life 2022, 12, 896. https://doi.org/10.3390/life12060896
Romano M, Garcia-Bournissen F, Piskin D, Rodoplu U, Piskin L, Elzagallaai AA, Tuncer T, Sezer S, Ucuncuoglu D, Honca T, et al. Anti-Inflammatory, Antioxidant, and Anti-Atherosclerotic Effects of Natural Supplements on Patients with FMF-Related AA Amyloidosis: A Non-Randomized 24-Week Open-Label Interventional Study. Life. 2022; 12(6):896. https://doi.org/10.3390/life12060896
Chicago/Turabian StyleRomano, Micol, Facundo Garcia-Bournissen, David Piskin, Ulkumen Rodoplu, Lizzy Piskin, Abdelbaset A. Elzagallaai, Tunc Tuncer, Siren Sezer, Didar Ucuncuoglu, Tevfik Honca, and et al. 2022. "Anti-Inflammatory, Antioxidant, and Anti-Atherosclerotic Effects of Natural Supplements on Patients with FMF-Related AA Amyloidosis: A Non-Randomized 24-Week Open-Label Interventional Study" Life 12, no. 6: 896. https://doi.org/10.3390/life12060896
APA StyleRomano, M., Garcia-Bournissen, F., Piskin, D., Rodoplu, U., Piskin, L., Elzagallaai, A. A., Tuncer, T., Sezer, S., Ucuncuoglu, D., Honca, T., Poddighe, D., Yavuz, I., Stenvinkel, P., Yilmaz, M. I., & Demirkaya, E. (2022). Anti-Inflammatory, Antioxidant, and Anti-Atherosclerotic Effects of Natural Supplements on Patients with FMF-Related AA Amyloidosis: A Non-Randomized 24-Week Open-Label Interventional Study. Life, 12(6), 896. https://doi.org/10.3390/life12060896