
A Critical Review of the Psychomotor Agitation Treatment in Youth


Abstract
:1. Introduction
1.1. Rationale
1.2. Objectives
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria/Information Source
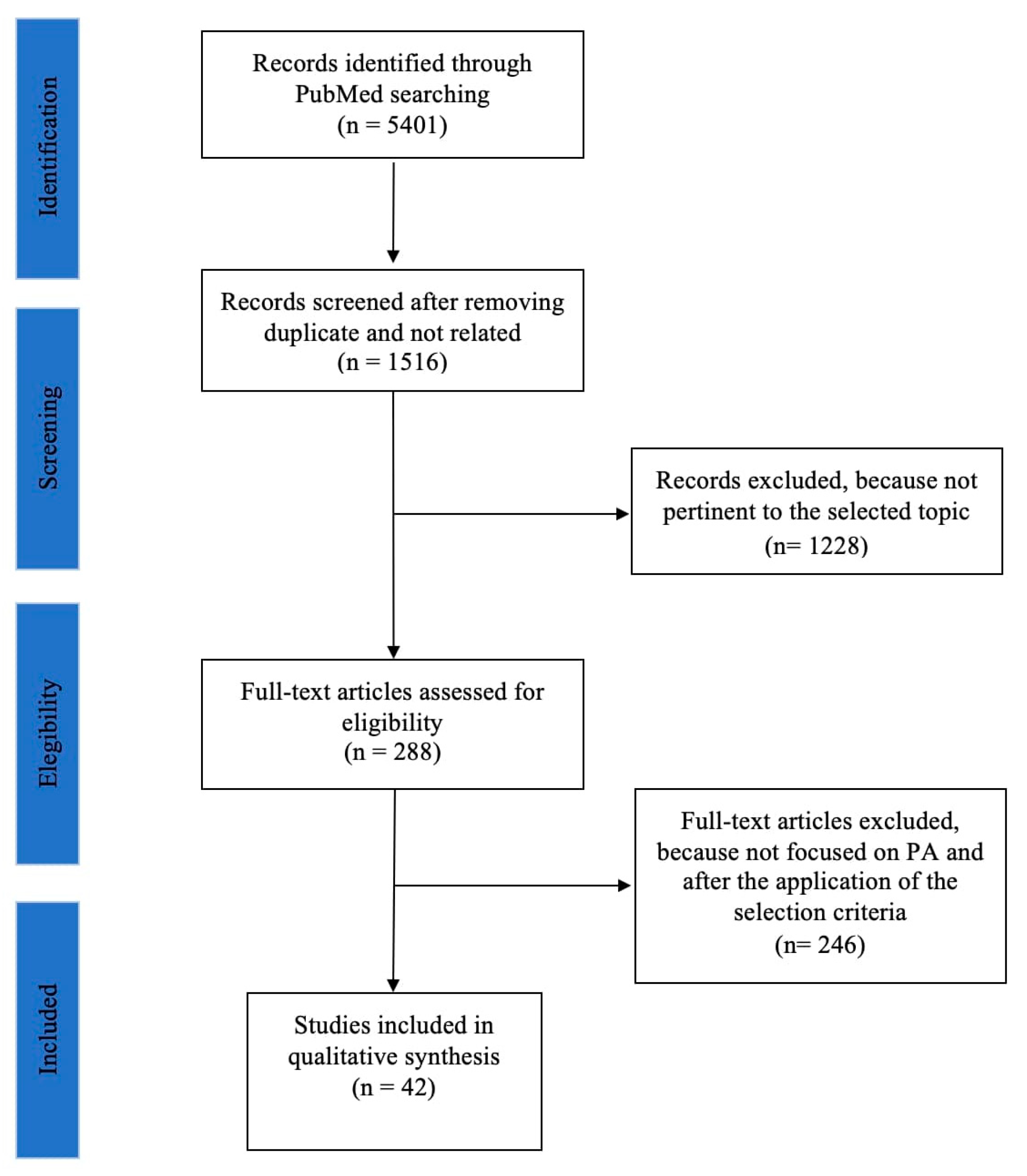
2.3. Search Strategy
2.4. Study Selection
2.5. Data Collection Process and Data Items
2.6. Data Synthesis
3. Results
3.1. Diagnostic Assessment
3.2. Pharmacological Treatment
3.2.1. Benzodiazepines
3.2.2. Valproic Acid
3.2.3. Risperidone
3.2.4. Olanzapine
3.2.5. Ziprasidone
3.2.6. Aripiprazole
3.2.7. Haloperidol
3.2.8. Other Pharmacological Treatments
4. Discussion
4.1. Summary of Evidence
4.2. Summary of Limitations
5. Conclusions and Areas for Future Research
Author Contributions
Funding
Conflicts of Interest
References
- Kunen, S.; Niederhauser, R.; Smith, P.O.; Morris, J.A.; Marx, B.D. Race disparities in psychiatric rates in emergency departments. J. Consult. Clin. Psychol. 2005, 73, 116–126. [Google Scholar] [CrossRef] [Green Version]
- Lindenmayer, J.P. The pathophysiology of agitation. J. Clin. Psychiatry 2000, 61 (Suppl. S14), 5–10. [Google Scholar] [PubMed]
- Baroni, A.; Lunsford, J.R.; Luckenbaugh, D.A.; Towbin, K.E.; Leibenluft, E. Practitioner review: The assessment of bipolar disorder in children and adolescents. J. Child Psychol. Psychiatry 2009, 50, 203–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreno, C.; Laje, G.; Blanco, C.; Jiang, H.; Schmidt, A.B.; Olfson, M. National trends in the outpatient diagnosis and treatment of bipolar disorder in youth. Arch. Gen. Psychiatry 2007, 64, 1032–1039. [Google Scholar] [CrossRef] [Green Version]
- Cummings, M.R.; Miller, B.D. Pharmacologic management of behavioral instability in medically ill pediatric patients. Curr. Opin. Pediatr. 2004, 16, 516–522. [Google Scholar] [CrossRef] [PubMed]
- Pappadopulos, E.; Jensen, P.S.; Schur, S.B.; MacIntyre, J.C., 2nd; Ketner, S.; Van Orden, K.; Sverd, J.; Sardana, S.; Woodlock, D.; Schweitzer, R.; et al. “Real world” atypical antipsychotic prescribing practices in public child and adolescent inpatient settings. Schizophr. Bull. 2002, 28, 111–121. [Google Scholar] [CrossRef] [Green Version]
- Pappadopulos, E.; Macintyre Ii, J.C.; Crismon, M.L.; Findling, R.L.; Malone, R.P.; Derivan, A.; Schooler, N.; Sikich, L.; Greenhill, L.; Schur, S.B.; et al. Treatment recommendations for the use of antipsychotics for aggressive youth (TRAAY). Part II. J. Am. Acad. Child Adolesc. Psychiatry 2003, 42, 145–161. [Google Scholar] [CrossRef]
- Schur, S.B.; Sikich, L.; Findling, R.L.; Malone, R.P.; Crismon, M.L.; Derivan, A.; Macintyre Ii, J.C.; Pappadopulos, E.; Greenhill, L.; Schooler, N.; et al. Treatment recommendations for the use of antipsychotics for aggressive youth (TRAAY). Part I: A review. J. Am. Acad. Child Adolesc. Psychiatry 2003, 42, 132–144. [Google Scholar] [CrossRef]
- NCCMH. Violence and Aggression: Short-Term Management in Mental Health, Health and Community Settings: Updated Edition; NCCMH: London, UK, 2015. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [Green Version]
- Akhondzadeh, S.; Tajdar, H.; Mohammadi, M.R.; Mohammadi, M.; Nouroozinejad, G.H.; Shabstari, O.L.; Ghelichnia, H.A. A double-blind placebo controlled trial of piracetam added to risperidone in patients with autistic disorder. Child Psychiatry Hum. Dev. 2008, 39, 237–245. [Google Scholar] [CrossRef]
- Amery, B.; Minichiello, M.D.; Brown, G.L. Aggression in hyperactive boys: Response to d-amphetamine. J. Am. Acad. Child Psychiatry 1984, 23, 291–294. [Google Scholar] [CrossRef] [PubMed]
- Avari, J.M. Paradoxical Agitation in Adolescent Male on Valproate. J. Child Adolesc. Psychopharmacol. 2016, 26, 78–79. [Google Scholar] [CrossRef] [PubMed]
- Barzman, D.H.; DelBello, M.P.; Forrester, J.J.; Keck, P.E., Jr.; Strakowski, S.M. A retrospective chart review of intramuscular ziprasidone for agitation in children and adolescents on psychiatric units: Prospective studies are needed. J. Child Adolesc. Psychopharmacol. 2007, 17, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Battaglia, C.; Averna, R.; Labonia, M.; Riccioni, A.; Vicari, S. Intravenous Valproic Acid Add-On Therapy in Acute Agitation Adolescents With Suspected Substance Abuse: A Report of Six Cases. Clin. Neuropharmacol. 2018, 41, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Biederman, J.; Mick, E.; Faraone, S.V.; Wozniak, J.; Spencer, T.; Pandina, G. Risperidone for the treatment of affective symptoms in children with disruptive behavior disorder: A post hoc analysis of data from a 6-week, multicenter, randomized, double-blind, parallel-arm study. Clin. Ther. 2006, 28, 794–800. [Google Scholar] [CrossRef]
- Bregstein, J.S.; Wagh, A.M.; Tsze, D.S. Intranasal Lorazepam for Treatment of Severe Agitation in a Pediatric Behavioral Health Patient in the Emergency Department. Ann. Emerg. Med. 2020, 75, 86–89. [Google Scholar] [CrossRef] [Green Version]
- Cole, J.B.; Klein, L.R.; Strobel, A.M.; Blanchard, S.R.; Nahum, R.; Martel, M.L. The Use, Safety, and Efficacy of Olanzapine in a Level I Pediatric Trauma Center Emergency Department Over a 10-Year Period. Pediatr. Emerg. Care 2020, 36, 70–76. [Google Scholar] [CrossRef]
- Douglas, J.F.; Sanders, K.B.; Benneyworth, M.H.; Smith, J.L.; Dejean, V.M.; McGrew, S.G.; Veenstra-Vanderweele, J. Brief report: Retrospective case series of oxcarbazepine for irritability/agitation symptoms in autism spectrum disorder. J. Autism Dev. Disord. 2013, 43, 1243–1247. [Google Scholar] [CrossRef]
- Farnaghi, F.; Rahmani, R.; Hassanian-Moghaddam, H.; Zamani, N.; McDonald, R.; Gholami, N.; Gachkar, L. Oral clonazepam versus lorazepam in the treatment of methamphetamine-poisoned children: A pilot clinical trial. BMC Pediatr. 2020, 20, 543. [Google Scholar] [CrossRef]
- Findling, R.L.; Robb, A.; McNamara, N.K.; Pavuluri, M.N.; Kafantaris, V.; Scheffer, R.; Frazier, J.A.; Rynn, M.; DelBello, M.; Kowatch, R.A.; et al. Lithium in the Acute Treatment of Bipolar I Disorder: A Double-Blind, Placebo-Controlled Study. Pediatrics 2015, 136, 885–894. [Google Scholar] [CrossRef]
- Frazier, J.A.; Biederman, J.; Tohen, M.; Feldman, P.D.; Jacobs, T.G.; Toma, V.; Rater, M.A.; Tarazi, R.A.; Kim, G.S.; Garfield, S.B.; et al. A prospective open-label treatment trial of olanzapine monotherapy in children and adolescents with bipolar disorder. J. Child Adolesc. Psychopharmacol. 2001, 11, 239–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hail, S.L.; Obafemi, A.; Kleinschmidt, K.C. Successful management of olanzapine-induced anticholinergic agitation and delirium with a continuous intravenous infusion of physostigmine in a pediatric patient. Clin. Toxicol. 2013, 51, 162–166. [Google Scholar] [CrossRef] [PubMed]
- Harrison, A.M.; Lugo, R.A.; Lee, W.E.; Appachi, E.; Bourdakos, D.; Davis, S.J.; McHugh, M.J.; Weise, K.L. The use of haloperidol in agitated critically ill children. Clin. Pediatr. 2002, 41, 51–54. [Google Scholar] [CrossRef] [PubMed]
- Hazaray, E.; Ehret, J.; Posey, D.J.; Petti, T.A.; McDougle, C.J. Intramuscular ziprasidone for acute agitation in adolescents. J. Child Adolesc. Psychopharmacol. 2004, 14, 464–470. [Google Scholar] [CrossRef]
- Hilty, D.M.; Rodriguez, G.D.; Hales, R.E. Intravenous valproate for rapid stabilization of agitation in neuropsychiatric disorders. J. Neuropsychiatry Clin. Neurosci. 1998, 10, 365–366. [Google Scholar] [CrossRef] [PubMed]
- Jackson, B.F.; Beck, L.A.; Losek, J.D. Successful flumazenil reversal of paradoxical reaction to midazolam in a child. J. Emerg. Med. 2015, 48, e67–e72. [Google Scholar] [CrossRef]
- Jangro, W.C.; Preval, H.; Southard, R.; Klotz, S.G.; Francis, A. Conventional intramuscular sedatives versus ziprasidone for severe agitation in adolescents: Case-control study. Child Adolesc. Psychiatry Ment. Health 2009, 3, 9. [Google Scholar] [CrossRef] [Green Version]
- Khan, S.S.; Mican, L.M. A naturalistic evaluation of intramuscular ziprasidone versus intramuscular olanzapine for the management of acute agitation and aggression in children and adolescents. J. Child Adolesc. Psychopharmacol. 2006, 16, 671–677. [Google Scholar] [CrossRef]
- Kim, K.M.; Lee, K.H.; Kim, Y.H.; Ko, M.J.; Jung, J.W.; Kang, E. Comparison of effects of intravenous midazolam and ketamine on emergence agitation in children: Randomized controlled trial. J. Int. Med. Res. 2016, 44, 258–266. [Google Scholar] [CrossRef]
- Koceroglu, I.; Devrim, S.; Bingol Tanriverdi, T.; Gura Celik, M. The effects of dexmedetomidine and tramadol on post-operative pain and agitation, and extubation quality in paediatric patients undergoing adenotonsillectomy surgery: A randomized trial. J. Clin. Pharm. Ther. 2020, 45, 340–346. [Google Scholar] [CrossRef]
- Koner, O.; Ture, H.; Mercan, A.; Menda, F.; Sozubir, S. Effects of hydroxyzine-midazolam premedication on sevoflurane-induced paediatric emergence agitation: A prospective randomised clinical trial. Eur. J. Anaesthesiol. 2011, 28, 640–645. [Google Scholar] [CrossRef] [PubMed]
- Krishnamoorthy, J.; King, B.H. Open-label olanzapine treatment in five preadolescent children. J. Child Adolesc. Psychopharmacol. 1998, 8, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Marcus, R.N.; Owen, R.; Kamen, L.; Manos, G.; McQuade, R.D.; Carson, W.H.; Aman, M.G. A Placebo-Controlled, Fixed-Dose Study of Aripiprazole in Children and Adolescents with Irritability Associated with Autistic Disorder. J. Am. Acad. Child Adolesc. Psychiatry 2009, 48, 1110–1119. [Google Scholar] [CrossRef] [PubMed]
- McDougle, C.J.; Kem, D.L.; Posey, D.J. Case series: Use of ziprasidone for maladaptive symptoms in youths with autism. J. Am. Acad. Child Adolesc. Psychiatry 2002, 41, 921–927. [Google Scholar] [CrossRef]
- Nguyen, T.; Stanton, J.; Foster, R. Intramuscular Ziprasidone Dosing for Acute Agitation in the Pediatric Emergency Department: An Observational Study. J. Pharm. Pract. 2018, 31, 18–21. [Google Scholar] [CrossRef]
- Pavuluri, M.N.; Henry, D.B.; Carbray, J.A.; Naylor, M.W.; Janicak, P.G. Divalproex sodium for pediatric mixed mania: A 6-month prospective trial. Bipolar Disord. 2005, 7, 266–273. [Google Scholar] [CrossRef]
- Pleak, R.R.; Birmaher, B.; Gavrilescu, A.; Abichandani, C.; Williams, D.T. Mania and neuropsychiatric excitation following carbamazepine. J. Am. Acad. Child Adolesc. Psychiatry 1988, 27, 500–503. [Google Scholar] [CrossRef] [PubMed]
- Rapp, J.T.; Swanson, G.; Dornbusch, K. Temporary increases in problem behavior and sleep disruption following decreases in medication: A descriptive analysis of conditional rates. Behav. Modif. 2007, 31, 825–846. [Google Scholar] [CrossRef]
- Ratcliff, S.L.; Meyer, W.J., 3rd; Cuervo, L.J.; Villarreal, C.; Thomas, C.R.; Herndon, D.N. The use of haloperidol and associated complications in the agitated, acutely ill pediatric burn patient. J. Burn Care Rehabil. 2004, 25, 472–478. [Google Scholar] [CrossRef] [PubMed]
- Robb, A.S.; Carson, W.H.; Nyilas, M.; Ali, M.; Forbes, R.A.; Iwamoto, T.; Assunção-Talbott, S.; Whitehead, R.; Pikalov, A. Changes in Positive and Negative Syndrome Scale-Derived Hostility Factor in Adolescents with Schizophrenia Treated with Aripiprazole: Post Hoc Analysis of Randomized Clinical Trial Data. J. Child Adolesc. Psychopharmacol. 2010, 20, 33–38. [Google Scholar] [CrossRef]
- Roberts, C.; McEachern, M.; Mounsey, A. CSF studies which ultimately led to the possible diagnosis of anti-NMDAR encephalitis. BMJ Case Rep. 2020, 13, e233489. [Google Scholar] [CrossRef] [PubMed]
- Sabuncuoglu, O. Risperidone-to-methylphenidate switch reaction in children: Three cases. J. Psychopharmacol. 2007, 21, 216–219. [Google Scholar] [CrossRef] [PubMed]
- Salpekar, J.A.; Conry, J.A.; Doss, W.; Cushner-Weinstein, S.; Pearl, P.L.; Weinstein, S.L.; Gaillard, W.D. Clinical experience with anticonvulsant medication in pediatric epilepsy and comorbid bipolar spectrum disorder. Epilepsy Behav. 2006, 9, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Scott, L.K.; Green, R.; McCarthy, P.J.; Conrad, S.A. Agitation and/or aggression after traumatic brain injury in the pediatric population treated with ziprasidone. Clinical article. J. Neurosurg. Pediatr. 2009, 3, 484–487. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, R.M.; Ahmed, K. The efficacy of olanzapine, as needed, to treat acute agitation in juveniles. J. Child Adolesc. Psychopharmacol. 2002, 12, 71–73. [Google Scholar] [CrossRef]
- Staller, J.A. Intramuscular ziprasidone in youth: A retrospective chart review. J. Child Adolesc. Psychopharmacol. 2004, 14, 590–592. [Google Scholar] [CrossRef]
- Steingard, R.J.; Zimnitzky, B.; DeMaso, D.R.; Bauman, M.L.; Bucci, J.P. Sertraline treatment of transition-associated anxiety and agitation in children with autistic disorder. J. Child Adolesc. Psychopharmacol. 1997, 7, 9–15. [Google Scholar] [CrossRef]
- van der Zwaan, S.; Blankespoor, R.J.; Wolters, A.M.; Creten, C.; Leroy, P.L.; Schieveld, J.N. Additional use of methotrimeprazine for treating refractory agitation in pediatric patients. Intensive Care Med. 2012, 38, 175–176. [Google Scholar] [CrossRef] [Green Version]
- Wakai, S.; Yoto, Y.; Higashidate, Y.; Tachi, N.; Chiba, S. Benign partial epilepsy with affective symptoms: Hyperkinetic behavior during interictal periods. Epilepsia 1994, 35, 810–812. [Google Scholar] [CrossRef]
- Wang, G.S.; Baker, K.; Ng, P.; Janis, G.C.; Leonard, J.; Mistry, R.D.; Heard, K. A randomized trial comparing physostigmine vs. lorazepam for treatment of antimuscarinic (anticholinergic) toxidrome. Clin. Toxicol. 2021, 59, 698–704. [Google Scholar] [CrossRef]
- Yip, L.; Aeng, E.; Elbe, D. Management of Acute Agitation and Aggression in Children and Adolescents with Pro Re Nata Oral Immediate Release Antipsychotics in the Pediatric Emergency Department. J. Child Adolesc. Psychopharmacol. 2020, 30, 534–541. [Google Scholar] [CrossRef]
- Aman, M.G.; Singh, N.N.; Stewart, A.W.; Field, C.J. The aberrant behavior checklist: A behavior rating scale for the assessment of treatment effects. Am. J. Ment. Defic. 1985, 89, 485–491. [Google Scholar] [PubMed]
- Young, R.C.; Biggs, J.T.; Ziegler, V.E.; Meyer, D.A. A rating scale for mania: Reliability, validity and sensitivity. Br. J. Psychiatry 1978, 133, 429–435. [Google Scholar] [CrossRef]
- Guy, W. ECDEU Assessment Manual for Psychopharmacology; US Department of Health, Education, and Welfare, Public Health Service: Boston, MA, USA, 1976.
- Riker, R.R.; Picard, J.T.; Fraser, G.L. Prospective evaluation of the Sedation-Agitation Scale for adult critically ill patients. Crit. Care Med. 1999, 27, 1325–1329. [Google Scholar] [CrossRef] [PubMed]
- Kay, S.R.; Fiszbein, A.; Opler, L.A. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. 1987, 13, 261–276. [Google Scholar] [CrossRef]
- King, B.H.; Hollander, E.; Sikich, L.; McCracken, J.T.; Scahill, L.; Bregman, J.D.; Donnelly, C.L.; Anagnostou, E.; Dukes, K.; Sullivan, L.; et al. Lack of efficacy of citalopram in children with autism spectrum disorders and high levels of repetitive behavior: Citalopram ineffective in children with autism. Arch. Gen. Psychiatry 2009, 66, 583–590. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Delgar, B.; Morer, A.; Varela, E.; Romero, S.; Garcia, M.; Coffey, B.J.; Lazaro, L. Activation in Children and Adolescents Treated With Selective Serotonin Reuptake Inhibitors: A Weighty Reason? J. Clin. Psychopharmacol. 2018, 38, 475–480. [Google Scholar] [CrossRef]
- Connor, D.F.; Glatt, S.J.; Lopez, I.D.; Jackson, D.; Melloni, R.H., Jr. Psychopharmacology and aggression. I: A meta-analysis of stimulant effects on overt/covert aggression-related behaviors in ADHD. J. Am. Acad. Child Adolesc. Psychiatry 2002, 41, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Currier, G.W.; Medori, R. Orally versus intramuscularly administered antipsychotic drugs in psychiatric emergencies. J. Psychiatr. Pract. 2006, 12, 30–40. [Google Scholar] [CrossRef]
- Sonnier, L.; Barzman, D. Pharmacologic management of acutely agitated pediatric patients. Paediatr. Drugs 2011, 13, 1–10. [Google Scholar] [CrossRef]


{kind=link}
| Author/Publication Year | Study Design | Sample Characteristics | Diagnosis | Treatment | Outcomes |
|---|---|---|---|---|---|
| Akhondzadeh et al., 2008 [11] | Double-blind, randomized, placebo-controlled trial | 40 pts (10 females) Age range: 3–11 Mean age/SD: 6.83 ± 1.81 | ASD | Risperidone vs. Risperidone + Piracetam | The ABC-C Rating Scale scores improved |
| Amery et al., 1984 [12] | Double-blind, randomized, placebo-controlled trial | 10 male pts Age range: 8–11 years Mean age/SD: 9.6 ± 1.6 | ADHD | d-Amphetamine | ↓ PA |
| Avari et al., 2016 [13] | Case report | 1 male pt (17 years old) | Mood Disorder | Quetiapine administration after valproate suspension | Quetiapine improved disorganized thought and paranoia |
| Barzman et al., 2007 [14] | Chart review | 59 pts (20 females) Age range: 5–19 years Mean age: 13.5 years | Any mental illness | Ziprasidone | ↓ PA Side effects reported |
| Battaglia et al., 2018 [15] | Case series | 6 pts (1 female) Age range: 16–17 years Mean age/SD: 16.6 ± 0.4 | Mood Disorders Conduct Disorder Substance Abuse | VPA in add-on to SGAs or BDZs | ↓ PA Side effects reported |
| Biederman et al., 2006 [16] | Double-blind, randomized, placebo-controlled trial | 110 pts (21 females) Mean age/SD: 8.32 ± 2.3 | DBD | Risperidone | Effective in treating the factors of explosive irritability and the management of agitation |
| Bregstein et al., 2019 [17] | Case report | 1 male pt (7 years old) | Oppositional Disorder and Anxiety Disorders | Lorazepam | Transiently effective in treating severe agitation (~90 min) |
| Cole et al., 2020 [18] | Chart review | 285 pts (20 females) Age range: 9–18 years Mean age: 16.4 years | Subjects accessed in the emergency pediatric level I trauma center | Olanzapine | Effective for acute agitation No patient died or had dysrhythmia; one patient experienced dystonia |
| Douglas et al., 2013 [19] | Case series | 30 pts (4 females) Age range: 5–21 Mean age/SD: 12.00 ± 3.6 | ASD | Oxcarbazepine | 14 significantly reduced the CGI score, 10 reduced the CGI score, 7 discontinued for AE |
| Farnaghi et al., 2020 [20] | Single-center clinical trial | 30 pts (11 females) Age range: 6 months–12 years Mean age: 16 months | Methamphetamine-poisoned children | Clonazepam vs. lorazepam | Clonazepam and lorazepam treatments were equally effective at similar doses. However, considering the higher potency of clonazepam, it seems that lorazepam is the safer treatment. |
| Findling et al., 2015 [21] | Double-blind, randomized, placebo-controlled trial | 81 pts (44 females) Age range: 7–17 Mean age/SD: 11.4 ± 2.9 | Bipolar I Disorder | Lithium | ↓ in YMRS score and ↓ in CGI score. Lithium was superior to placebo in reducing manic symptoms and the frequency of psychomotor agitation episodes |
| Frazier et al., 2001 [22] | Open-label trial | 23 pts (10 females) Age range: 5–14 years Mean age/SD: 10.3 ± 6.2 | Bipolar I-II Disorders | Olanzapine | ↓ YMRS aggression subscale scores Side effects reported |
| Hail et al., 2013 [23] | Case report | 1 male pt (6 years old) | ADHD | Physostigmine | ↓ agitation and delirium |
| Harrison et al., 2002 [24] | Case series | 5 pts (1 females) Age range: 9 m–16 y Mean age/SD: 8.83 ± 7.35 | Critical ill patients (ARDS, peritonitis, graft vs. host, intussusception) | Haloperidol | Reduction in agitation and improvement in ventilator weaning. One patient had a dystonic reaction |
| Hazaray et al., 2004 [25] | Case series | 3 male pts Age range: 12–13 years Mean age/SD: 12.3 ± 0.47 | Conduct Disorder; ADHD; Oppositional Disorder; Bipolar I Disorder | Ziprasidone | ↓ aggression; syncope reported |
| Hilty et al., 1998 [26] | Case report | 1 male pt (8 years old) | ASD | Valproate | ↓ PA |
| Jackson et al., 2015 [27] | Case report | 1 female pt (4 years old) | Laceration in upper lip | Flumazenil to reverse the midazolam paradoxical effect | Paradoxical reaction with psychomotor agitation successfully treated with flumazenil |
| Jangro et al., 2009 [28] | Case control | 52 pts (25 females) Age range: 12–17 years Mean age/SD: 15.7 ± 1.35 | Psychotic Disorders; SUD; Adjustement Disorder; Impulse-control Disoder | Ziprasidone, haloperidol, BDZs | ↓ PA |
| Khan and Mican, 2006 [29] | Chart review | 100 pts (50 females) Age range: 12–17 years Mean age/SD: 14.5 ± 2.25 | Any mental illness | Ziprasidone vs. Olanzapine | ↓ PA |
| Kim et al., 2016 [30] | Double-blind, randomized trial | 67 pts (36 females) Age range: 2–6 Mean age/SD: 4.18 ± 1.33 | Pediatric patients undergoing ophthalmic surgery | Midazolam and Ketamine following sevoflurane anesthesia | Ketamine was more efficient in ↓ the incidence of emergence agitation at 10 and 20 min after the transfer to the post-anesthetic care unit than midazolam |
| Koceroglu et al., 2020 [31] | Randomized trial | 60 pts (32 females) Age range: 2–9 Mean age: 5.8 | Pediatric patients undergoing an adenotonsillectomy using sevoflurane | Dexmedetomidine vs. tramadol | Dexmedetomidine was more effective than tramadol for mitigating post-operative agitation |
| Koner et al., 2011 [32] | Double-blind, randomized trial | 84 pts (12 females) Age range: 1–7 Mean age: 2.4 | Pediatric patients undergoing infraumbilical surgery with a caudal block | Midazolam and hydroxyzine | The incidence of sevoflurane-induced emergence agitation was significantly lower in children premedicated with a midazolam and hydroxyzine combination compared to those premedicated with midazolam only |
| Krishnamoorthy and King, 1998 [33] | Case series | 5 pts (3 females) Age range: 6–11 Mean age/SD: 9.2 ± 2.0 | Bipolar disorder, ADHD, Impulse Disorder Psychotic Disorder NOS | Olanzapine | ↓ aggressive behavior in 3 pts |
| Marcus et al., 2009 [34] | Double-blind, randomized, placebo-controlled trial | 218 pts (23 females) Age range: 6–17 Mean age: 9.7 | ASD | Aripiprazole | Improvement in mean Aberrant Behavior Checklist Irritability subscale scores and CGI score |
| McDougle et al., 2002 [35] | Open-label trial | 12 pts (2 females) Age Range: 8–20 Mean age/SD: 11.62 ± 4.38 | ASD | Ziprasidone | ↓ agitation, irritability and aggressiveness (CGI score) |
| Nguyen et al., 2018 [36] | Chart review | 40 pts (8 females) Age range: 5–18 years Mean age: 11.8 | ADHD, ASD, Bipolar I Disorder, PTSD | Ziprasidone | ↓ PA 13 non-responders (32%) |
| Pavuluri et al., 2005 [37] | Open-label trial | 34 pts (13 females) Mean age/SD/12: 12.3 ± 3.7 | Mixed Episode (Bipolar I Disorder) | Valproate | ↓ CGI-BP aggression subscale scores |
| Pleak et al., 1988 [38] | Case series | 6 male pts Age range: 6–10 Mean age/SD: 12.83 ± 2.48 | ADHD, Conduct Disorder, Intermittent Explosive Disorder | Carbamazepine | ↑ irritability, aggressiveness, impulsivity, manic and hypomanic symptoms, risk seizures |
| Rapp et al., 2007 [39] | Case series | 17 pts (7 females), Age range: 9–17 Mean age/SD: 12.7 ± 2.7 | Neurodevelopmental Disorders | Antipsychotics, Antihistaminics, Mood stabilizers | A reduction in the doses of the medications increased aggression, agitation, self-injuries, anger, etc. |
| Ratcliff et al., 2004 [40] | Chart review | 26 pts (7 females) Mean age/SD: 11.7 ± 3.9 | Agitated, Acutely Ill Pediatric Burn Patient | Haloperidol | ↓ agitation, but 23% had AE (hyperpyrexia or dystonic reaction) |
| Robb et al., 2010 [41] | Double-blind, randomized, placebo-controlled trial | 302 pts (131 females) Age range: 13–17 Mean age: 15.5 | Schizophrenia | Aripiprazole | ↓ PANSS Hostility, Uncooperativeness and Poor Impulse Control items |
| Roberts et al., 2020 [42] | Case report | 1 male pt (17 years old) | Anti-NMDAR encephalitis | Olanzapine | ↓ agitation and irritability and ↑ cooperativity |
| Sabuncuoglu, 2008 [43] | Case series | 3 pts (2 females) Age range: 6–15 Mean age/SD: 9 ± 5.2 | ADHD | Switch from Risperidone to Metylphenidate | Increase in PA and aggressive behavior |
| Salpekar et al., 2006 [44] | Chart review | 38 pts (17 females) Age range: 6–17 Mean age: 10.4 | Complex partial seizure, primary generalized seizure disorder, Bipolar Disorder | Anticonvulsivants | ↑ CGI ratings |
| Scott et al., 2009 [45] | Case series | 20 pts (8 females) Age range: 9 months–17 years Mean age: 7.19 | Traumatic brain injury | Ziprasidone | ↓ PA |
| Sheikh and Ahmed., 2002 [46] | Case report | 1 female pt (10 years old) | ADHD and ODD | Olanzapine | ↓ agitation, irritability and aggressiveness |
| Staller et al., 2004 [47] | Chart review | 49 pts (32 females) Mean age: 17.49 | Psychomotor agitation, Agitation/anxiety/threat, Psychotic Disorder NOS | Ziprasidone | ↓ agitation and aggressiveness |
| Steingart et al., 1997 [48] | Case series | 9 male pts Age range: 6–12 years Mean age: 8.56 | ASD | Sertraline as add-on to haloperidol | 8 patients reported ↓ PA; 1 drop-out (stomachache) |
| van der Zwaan et al., 2012 [49] | Case series | 4 pts (1 female) Age range: 7 months–15 years Mean age/SD: 8.4 ± 5.8 | Any mental illness | Methotrimeprazine | ↓ PA |
| Wakai et al., 1994 [50] | Case report | 1 male pt (4 years old) | Benign partial epilepsy | Carbamazepine | ↓ frequency of the attacks and the hyperkinetic behavior |
| Wang et al., 2021 [51] | Blinded, randomized clinical trial | 19 pts (12 females) Age range: 10–18 Mean age: 13.9 | Antimuscarinic toxidrome | Physostigmine vs. lorazepam | Physostigmine was superior to lorazepam in controlling antimuscarinic delirium and agitation after bolus dosing |
| Yip et al., 2020 [52] | Chart review | 69 pts (39 females) Age range: 5–16 | Agitated or aggressive patients arrived at the emergency department | Quetiapine, haloperidol, loxapine, chlorpromazine | Drugs have comparable efficacy in managing agitation, but quetiapine has a lower risk of inducing EPS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tripodi, B.; Matarese, I.; Carbone, M.G. A Critical Review of the Psychomotor Agitation Treatment in Youth. Life 2023, 13, 293. https://doi.org/10.3390/life13020293
Tripodi B, Matarese I, Carbone MG. A Critical Review of the Psychomotor Agitation Treatment in Youth. Life. 2023; 13(2):293. https://doi.org/10.3390/life13020293
Chicago/Turabian StyleTripodi, Beniamino, Irene Matarese, and Manuel Glauco Carbone. 2023. "A Critical Review of the Psychomotor Agitation Treatment in Youth" Life 13, no. 2: 293. https://doi.org/10.3390/life13020293
APA StyleTripodi, B., Matarese, I., & Carbone, M. G. (2023). A Critical Review of the Psychomotor Agitation Treatment in Youth. Life, 13(2), 293. https://doi.org/10.3390/life13020293