

Adherence to CPAP Treatment: Can Mindfulness Play a Role?

 ,
,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Practical-Technical Issues Affecting CPAP Adherence
3. Other Variables Affecting CPAP Acceptance
4. Interventions to Improve Non-Adherence to CPAP Therapy
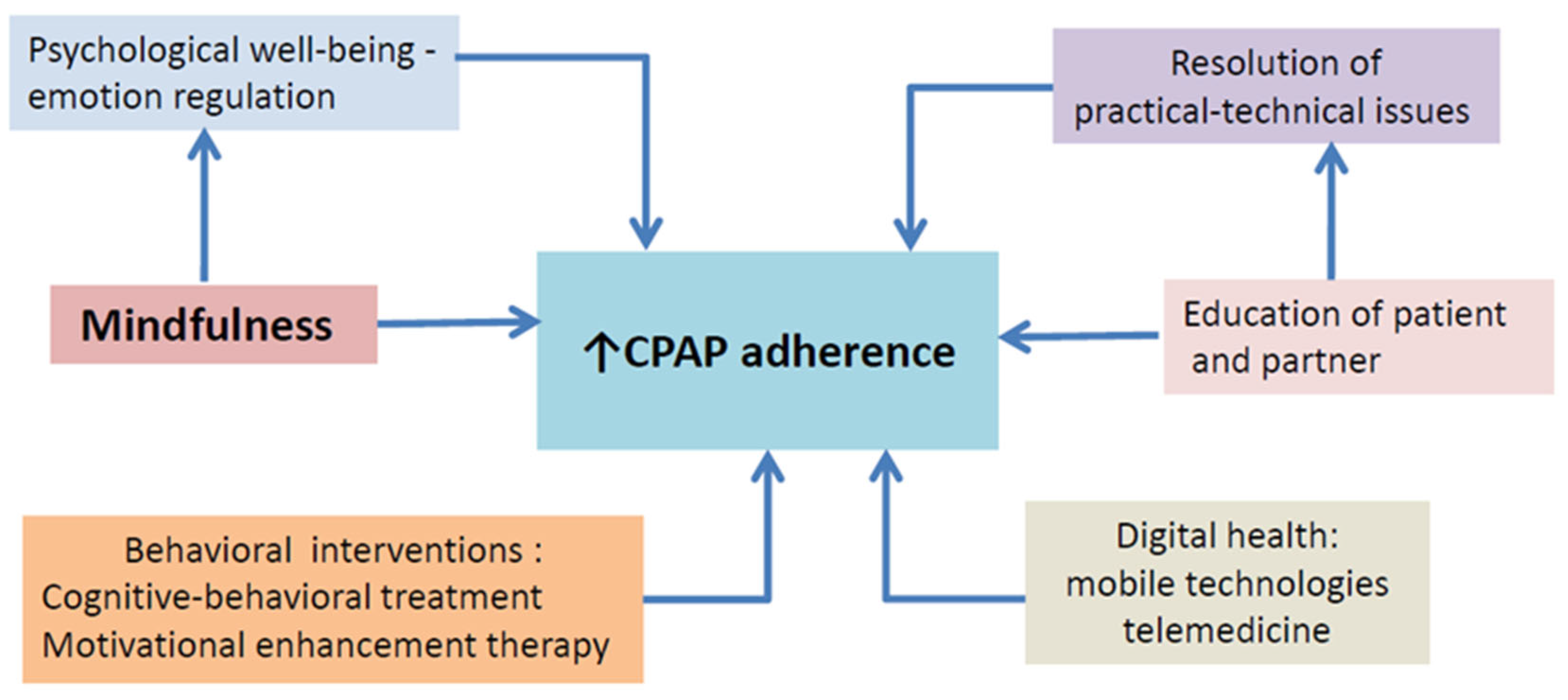
5. Mindfulness Interventions to Increase CPAP Adherence
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Matsumoto, T.; Murase, K.; Tabara, Y.; Gozal, D.; Smith, D.; Minami, T.; Chin, K. Impact of sleep characteristics and obesity on diabetes and hypertension across genders and menopausal status: The Nagahama Study. Sleep 2018, 41, zsy071. [Google Scholar] [CrossRef] [PubMed]
- Young, T.; Skatrud, J.; Peppard, P.E. Risk factors for obstructive sleep apnea in adult. JAMA 2004, 291, 2013–2016. [Google Scholar] [CrossRef] [PubMed]
- Pevernagie, D.; Bauters, F.A.; Hertegonne, K. The Role of Patient-Reported Outcomes in Sleep Measurements. Sleep Med. Clin. 2021, 16, 595–606. [Google Scholar] [CrossRef]
- Alomri, R.M.; Kennedy, G.A.; Wali, S.O.; Alhejaili, F.; Robinson, S.R. Association between nocturnal activity of the sympathetic nervous systemand cognitive dysfunction in obstructive sleep apnoea. Sci. Rep. 2021, 11, 11990. [Google Scholar] [CrossRef] [PubMed]
- Pépin, J.L.; Jullian-Desayes, I.; Sapène, M.; Treptow, E.; Joyeux-Faure, M.; Benmerad, M.; Bailly, S.; Grillet, Y.; Stach, B.; Richard, P.; et al. Multimodal remote monitoring of high cardiovascular risk patients with OSA initiating CPAP: A randomized trial. Chest 2019, 155, 730–739. [Google Scholar] [CrossRef]
- Jennum, P.; Castro, J.C.; Mettam, S.; Kharkevitch, T.; Cambron-Mellott, M.J. Socioeconomic and humanistic burden of illness of excessive daytime sleepiness severity associated with obstructive sleep apnoea in the European Union 5. Sleep Med. 2021, 84, 46–55. [Google Scholar] [CrossRef]
- Jordan, A.S.; McSharry, D.G.; Malhotra, A. Adult obstructive sleep apnoea. Lancet 2014, 383, 736–747. [Google Scholar] [CrossRef] [Green Version]
- Engleman, H.M.; Martin, S.E.; Deary, I.J.; Douglas, N.J. Effect of continuous positive airway pressure treatment on daytime function in sleep apnoea/hypopnoea syndrome. Lancet 1994, 343, 572–575. [Google Scholar] [CrossRef]
- Marin, J.M.; Carrizo, S.J.; Vicente, E.; Agusti, A.G.N. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: An observational study. Lancet 2005, 365, 1046–1053. [Google Scholar] [CrossRef]
- Dong, J.Y.; Zhang, Y.H.; Qin, L.Q. Obstructive sleep apnea and cardiovascular risk: Meta-analysis of prospective cohort studies. Atherosclerosis 2013, 229, 489–495. [Google Scholar] [CrossRef]
- Martínez-García, M.Á.; Soler-Cataluña, J.J.; Ejarque-Martínez, L.; Soriano, Y.; Román-Sánchez, P.; Illa, F.B.; Canal, J.M.; Duran-Cantolla, J. Continuous positive airway pressure treatment reduces mortality in patients with ischemic stroke and obstructive sleep apnea: A 5-year followup study. Am. J. Respir. Crit. Care Med. 2009, 180, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Gay, P.; Weaver, T.; Loube, D.; Iber, C. Evaluation of positive airway pressure treatment for sleep related breathing disorders in adults. Sleep 2006, 29, 381–401. [Google Scholar] [CrossRef] [PubMed]
- Giles, T.L.; Lasserson, T.J.; Smith, B.; White, J.; Wright, J.J.; Cates, C.J. Continuous positive airways pressure for obstructivesleep apnea in adults. Cochrane Database Syst. Rev 2006, 25, CD001106. [Google Scholar]
- Mashaqi, S.; Gozal, D. The impact of obstructive sleep apnea and PAP therapy on all-cause and cardiovascular mortality based on age and gender—A literature review. Respir. Investig. 2020, 58, 7–20. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, A.M.; Gooneratne, N.S.; Marcus, C.L.; Ofer, D.; Richards, K.C.; Weaver, T.E. A systematic review of CPAP adherence across age groups: Clinical and empiric insights for developing CPAP adherence interventions. Sleep Med. Rev. 2011, 15, 343–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zozula, R.; Rosen, R. Compliance with continuous positive airway pressure therapy: Assessing and improving treatment outcomes. Curr. Opin. Pulm. Med. 2001, 7, 391–398. [Google Scholar] [CrossRef]
- Weaver, T.; Grunstein, R. Adherence to continuous positive airway pressure therapy. Proc. Am. Thorac. Soc. 2008, 5, 173–178. [Google Scholar] [CrossRef] [Green Version]
- Rotenberg, B.W.; Murariu, D.; Pang, K.P. Trends in CPAP adherence over twenty years of data collection: A flattened curve. J. Otolaryngol. Head Neck Surg. 2016, 45, 43. [Google Scholar] [CrossRef] [Green Version]
- Contal, O.; Poncin, W.; Vaudan, S.; De Lys, A.; Takahashi, H.; Bochet, S.; Grandin, S.; Kehrer, P.; Charbonnier, F. One-year adherence to continuous positive airway pressure with telemonitoring in sleep apnea hypopnea syndrome: A randomized controlled trial. Front. Med. 2021, 8, 626361. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Full Catastrophe Living (Revised Version): Using the Wisdom of Your Body and Mind to Face Stress, Pain, and Illness; Bantam Books: New York, NY, USA, 2013. [Google Scholar]
- Kabat-Zinn, J.; Hanh, T.N. Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain, and Illness; Random House Publishing Group: New York, NY, USA, 2009. [Google Scholar]
- Rosa, D.; Amigoni, C.; Rimoldi, E.; Ripa, P.; Ligorio, A.; Fracchiolla, M.; Lombardi, C.; Parati, G.; Perger, E. Obstructive Sleep Apnea and Adherence to Continuous Positive Airway Pressure (CPAP) Treatment: Let’s Talk about Partners! Healthcare 2022, 10, 943. [Google Scholar] [CrossRef]
- Rash, J.A.; Kavanagh, V.A.J.; Garland, S.N. A Meta-Analysis of Mindfulness-Based Therapies for Insomnia and Sleep Disturbance: Moving Towards Processes of Change. Sleep Med. Clin. 2019, 14, 209–233. [Google Scholar] [CrossRef] [PubMed]
- Lewis, K.E.; Seale, L.; Bartle, I.E.; Watkins, A.J.; Ebden, P. Early predictors of CPAP use for the treatment of obstructive sleep apnea. Sleep 2004, 27, 134–138. [Google Scholar] [CrossRef] [PubMed]
- Richard, W.; Venker, J.; den Herder, C.; Kox, D.; van den Berg, B.; Laman, M.; van Tinteren, H.; de Vries, N. Acceptance and long-term compliance of nCPAP in obstructive sleep apnea. Eur. Arch. Oto-Rhino-Laryngol. 2007, 264, 1081–1086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmerman, E.; Arnedt, J.T.; Stanchina, M.; Millman, R.P.; Aloia, M.S. Normalization of memory performance and positive airway pressure adherence in memory-impaired patients with obstructive sleep apnea. CHEST 2006, 130, 1772–1778. [Google Scholar] [CrossRef]
- Weaver, T.E.; Maislin, G.; Dinges, D.F.; Bloxham, T.; George, C.F.; Greenberg, H.; Kader, G.; Mahowald, M.; Younger, J.; Pack, A.I. Relationship between hours of CPAP use and achieving normal levels of sleepiness and daily functioning. Sleep 2007, 30, 711–719. [Google Scholar] [CrossRef] [Green Version]
- Mehrtash, M.; Bakker, J.P.; Ayas, N. Predictors of Continuous Positive Airway Pressure Adherence in Patients with Obstructive Sleep Apnea. Lung 2019, 197, 115–121. [Google Scholar] [CrossRef]
- Isetta, V.; Ruiz, M.; Farré, R.; Montserrat, J. Supporting patients receiving CPAP treatment: The role of training and telemedicine. ERS Monogr. 2015, 67, 280–292. [Google Scholar]
- Van Ryswyk, E.; Anderson, C.S.; Antic, N.A.; Barbe, F.; Bittencourt, L.; Freed, R.; Heeley, E.; Liu, Z.; Loffler, K.A.; Lorenzi-Filho, G.; et al. Predictors of long-term adherence to continuous positive airway pressure in patients with obstructive sleep apnea and cardiovascular disease. Sleep 2019, 42, zsz152. [Google Scholar] [CrossRef] [Green Version]
- Aloia, M.S.; Arnedt, J.T.; Riggs, R.L.; Hecht, J.; Borrelli, B. Clinical management of poor adherence to CPAP: Motivational enhancement. Behav. Sleep Med. 2004, 2, 205–222. [Google Scholar] [CrossRef]
- Popescu, G.; Latham, M.; Allgar, V.; Elliott, M.W. Continuous positive airway pressure for sleep apnoea/hypopnoea syndrome: Usefulness of a 2 week trial to identify factors associated with long term use. Thorax 2001, 56, 727–733. [Google Scholar] [CrossRef]
- Broström, A.; Strömberg, A.; Ulander, M.; Fridlund, B.; Mårtensson, J.; Svanborg, E. Perceived informational needs, side-effects and their consequences on adherence—A comparison between CPAP treated patients with OSAS and healthcare personnel. Patient Educ. Couns. 2009, 74, 228–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weaver, T.E. Novel Aspects of CPAP Treatment and Interventions to Improve CPAP Adherence. J. Clin. Med. 2019, 8, 2220. [Google Scholar] [CrossRef] [PubMed]
- Patil, S.; Ayappa, I.A.; Caples, S.M.; Kimoff, R.J.; Patel, S.R. Treatment of adult obstructive sleep apnea with positive airway pressure: An American Academy of Sleep Medicine clinical practice guideline. J. Clin. Sleep Med. 2019, 15, 335–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, S.; Lang, C.; Sullivan, K.; Warren, J. Two new tools for assessing patients’ knowledge and beliefs about obstructive sleep apnea and continuous positive airway pressure therapy. Sleep Med. 2004, 5, 359–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, M.; Kristensen, E.; Berg, S.; Midgren, B. Sexual function in male patients with obstructive sleep apnoea after 1 year of CPAP treatment. Clin. Respir. J. 2013, 7, 214–219. [Google Scholar] [CrossRef]
- Chai-Coetzer, C.L.; Luo, Y.M.; Antic, N.A.; Zhang, X.L.; Chen, B.Y.; He, Q.Y.; Heeley, E.; Huang, S.G.; Anderson, C.; Zhong, N.S.; et al. Predictors of long-term adherence to continuous positive airway pressure therapy in patients with obstructive sleep apnea and cardiovascular disease in the SAVE study. Sleep 2013, 36, 1929–1937. [Google Scholar] [CrossRef] [Green Version]
- Pépin, J.L.; Krieger, J.; Rodenstein, D.; Cornette, A.; Sforza, E.; Delguste, P.; Deschaux, C.; Grillier, V.; Lévy, P. Effective compliance during the first 3 months of continuous positive airway pressure. A European prospective study of 121 patients. Am. J. Respir. Crit. Care Med. 1999, 160, 1124–1129. [Google Scholar] [CrossRef]
- Watach, A.J.; Hwang, D.; Sawyer, A.M. Personalized and Patient-Centered Strategies to Improve Positive Airway Pressure Adherence in Patients with Obstructive Sleep Apnea. Patient Prefer. Adherence 2021, 15, 1557–1570. [Google Scholar] [CrossRef]
- Scarpina, F.; Bastoni, I.; Cappelli, S.; Priano, L.; Giacomotti, E.; Castelnuovo, G.; Molinari, E.; Tovaglieri, I.M.A.; Cornacchia, M.; Fanari, P.; et al. Psychological Well-Being in Obstructive Sleep Apnea Syndrome Associated with Obesity: The Relationship with Personality, Cognitive Functioning, and Subjective and Objective Sleep Quality. Front. Psychol. 2021, 12, 588767. [Google Scholar] [CrossRef]
- Bodenhausen, G.V. Stereotypes as judgmental heuristics: Evidence of circadian variations in discrimination. Psychol. Sci. 1990, 1, 319–322. [Google Scholar] [CrossRef]
- Gordon, A.M.; Chen, S. The Role of Sleep in Interpersonal Conflict Do Sleepless Nights Mean Worse Fights? Soc. Psychol. Personal. Sci. 2014, 5, 168–175. [Google Scholar] [CrossRef]
- Maranges, H.M.; McNulty, J.K. The rested relationship: Sleep benefits marital evaluations. J. Fam. Psychol. 2017, 31, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Ye, L.; Malhotra, A.; Kayser, K.; Willis, D.G.; Horowitz, J.A.; Aloia, M.S.; Weaver, T.E. Spousal involvement and CPAP adherence: A dyadic perspective. Sleep Med. Rev. 2015, 19, 67–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luyster, F.S. Impact of obstructive sleep apnea and its treatments on partners: A literature review. J. Clin. Sleep Med. 2017, 13, 467. [Google Scholar] [CrossRef] [Green Version]
- Gentina, T.; Bailly, S.; Jounieaux, F.; Verkindre, C.; Broussier, P.M.; Guffroy, D.; Prigent, A.; Gres, J.J.; Kabbani, J.; Kedziora, L.; et al. Marital quality, partner’s engagement and continuous positive airway pressure adherence in obstructive sleep apnea. Sleep Med. 2019, 55, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Villa, G.; Mannarini, M.; Della Giovanna, G.; Marzo, E.; Manara, D.F.; Vellone, E. A literature review about self-care on ostomy patients and their caregivers. Int. J. Urol. Nurs. 2019, 13, 75–80. [Google Scholar] [CrossRef]
- Olsen, S.; Smith, S.; Oei, T.P. Adherence to continuous positive airway pressure therapy in obstructive sleep apnoea sufferers: Atheoretical approach to treatment adherence and intervention. Clin. Psychol. Rev. 2008, 28, 1355–1371. [Google Scholar] [CrossRef] [Green Version]
- Wild, M.R.; Engleman, H.M.; Douglas, N.J.; Espie, C.A. Can psychological factors help us to determine adherence to CPAP? A prospective study. Eur. Respir. J. 2004, 24, 461–465. [Google Scholar] [CrossRef]
- Maschauer, E.L.; Fairley, D.M.; Riha, R.L. Does personality play a role in continuous positive airway pressure compliance? Breathe 2017, 13, 32–43. [Google Scholar] [CrossRef]
- Edmonds, J.C.; Yang, H.; King, T.S.; Sawyer, D.A.; Rizzo, A.; Sawyer, A.M. Claustrophobic tendencies and continuous positive airway pressure therapy non-adherence in adults with obstructive sleep apnea. Heart Lung 2015, 44, 100–106. [Google Scholar] [CrossRef] [Green Version]
- Martin, L.R.; Williams, S.L.; Haskard, K.B.; DiMatteo, M.R. The challenge of patient adherence. Clin. Risk Manag. 2005, 1, 189–199. [Google Scholar]
- Rapelli, G.; Pietrabissa, G.; Manzoni, G.M.; Bastoni, I.; Scarpina, F.; Tovaglieri, I.; Perger, E.; Garbarino, S.; Fanari, P.; Lombardi, C.; et al. Improving CPAP Adherence in Adults with Obstructive Sleep Apnea Syndrome: A Scoping Review of Motivational Interventions. Front. Psychol. 2021, 12, 3266. [Google Scholar] [CrossRef] [PubMed]
- Weaver, T.E.; Sawyer, A.M. Adherence to continuous positive airway pressure treatment for obstructive sleep apnoea: Implications for future interventions. Indian J. Med. Res. 2010, 131, 245–248. [Google Scholar] [PubMed]
- Prasad, B.; Steffen, A.D.; Van Dongen, H.; Pack, F.M.; Strakovsky, I.; Staley, B.; Dinges, D.F.; Maislin, G.; Pack, A.I.; Weaver, T.E. Determinants of sleepiness in obstructive sleep apnea. Sleep 2018, 41, zsx199. [Google Scholar] [CrossRef] [Green Version]
- Sawyer, A.M.; Canamucio, A.; Moriarty, H.; Weaver, T.E.; Richards, K.C.; Kuna, S.T. Do cognitive perceptions influence CPAP use? Patient Educ. Couns. 2011, 85, 85–91. [Google Scholar] [CrossRef] [Green Version]
- Ceccarini, M.; Borrello, M.; Pietrabissa, G.; Manzoni, G.M.; Castelnuovo, G. Assessing motivation and readiness to change for weight management and control: An in-depth evaluation of three sets of instruments. Front. Psychol. 2015, 6, 511. [Google Scholar] [CrossRef] [Green Version]
- Shannon, R.; Donovan-Hall, M.; Bruton, A. Motivational interviewing in respiratory therapy:What do clinicians need to make it part of routine care? A qualitative study. PLoS ONE 2017, 12, e0187335. [Google Scholar] [CrossRef] [Green Version]
- Bakker, J.P.; Weaver, T.E.; Parthasarathy, S.; Aloia, M.S. Adherence to CPAP: What Should We Be Aiming For, and How Can We Get There? Chest 2019, 155, 1272–1287. [Google Scholar] [CrossRef]
- Engleman, H.M.; Wild, M.R. Improving CPAP use by patients with the sleep apnoea/hypopnoea syndrome (SAHS). Sleep Med. Rev. 2003, 7, 81–99. [Google Scholar] [CrossRef]
- Richards, D.; Bartlett, D.J.; Wong, K.; Malouff, J.; Grunstein, R.R. Increased adherence to CPAP with a group cognitive-behavioral treatment intervention: A randomized trial. Sleep 2007, 30, 635–640. [Google Scholar] [CrossRef] [Green Version]
- Donovan, L.M.; Boeder, S.; Malhotra, A.; Patel, S.R. New developments in the use of positive airway pressure for obstructive sleep apnea. J. Thorac. Dis. 2015, 7, 1323–1342. [Google Scholar]
- Chaiard, J.; Weaver, T.E. Update on Research and Practices in Major Sleep Disorders: Part I. Obstructive Sleep Apnea Syndrome. J. Nurs. Scholarsh. 2019, 51, 500–508. [Google Scholar] [CrossRef] [PubMed]
- Ragnoli, B.; Pochetti, P.; Raie, A.; Malerba, M. Comorbid Insomnia and Obstructive Sleep Apnea (COMISA): Current Concepts of Patient Management. Int. J. Environ. Res. Public Health 2021, 18, 9248. [Google Scholar] [CrossRef] [PubMed]
- Black, D.S.; O’Reilly, G.A.; Olmstead, R.; Breen, E.C.; Irwin, M.R. Mindfulness meditation and improvement in sleep quality and daytime impairment among older adults with sleep disturbances: A randomized clinical trial. JAMA Intern. Med. 2015, 175, 494–501. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Q.; Yue, C.; He, W.; Yu, J.-Y. The Mindful Self: A Mindfulness-Enlightened Self-view. Front. Psychol. 2017, 8, 1752. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.; Tang, R.; Braver, T.S. Investigating mindfulness influences on cognitive function: On the promise and potential of converging research strategies. Psychon. Bull. Rev. 2022, 29, 1198–1222. [Google Scholar] [CrossRef]
- Edinger, J.D.; Arnedt, J.T.; Bertisch, S.M.; Carney, C.E.; Harrington, J.J.; Lichstein, K.L.; Sateia, M.J.; Troxel, W.M.; Zhou, E.S.; Kazmi, U.; et al. Behavioral and psychological treatments for chronic insomnia disorder in adults: An American Academy of Sleep Medicine systematic review, meta-analysis, and GRADE assessment. J. Clin. Sleep Med. 2021, 17, 263–298. [Google Scholar] [CrossRef] [PubMed]
- Shonin, E.; Gordon, W.V.; Slade, K.; Griffiths, M.D. Mindfulness and other Buddhist-derived interventions in correctional settings: A systematic review. Aggress. Violent Behav. 2013, 18, 365–372. [Google Scholar] [CrossRef] [Green Version]
- Gawrysiak, M.J.; Baime, M.; King, T.S.; Watach, A.J.; McPhillips, M.V.; Kolanowski, A.; Schutte-Rodin, S.; Sawyer, A.M. Intervention Design and Trial Protocol: Mindfulness-based Exposure for PAP-associated Claustrophobia. West. J. Nurs. Res. 2021, 43, 261–272. [Google Scholar] [CrossRef]
- Jha, A.P.; Denkova, E.; Zanesco, A.P.; Witkin, J.E.; Rooks, J.; Rogers, S.L. Does mindfulness training help working memory ‘work’ better? Curr. Opin. Psychol. 2019, 28, 273–278. [Google Scholar] [CrossRef]
- Veltri, A.; Scarpellini, P.; Piccinni, A.; Conversano, C.; Giacomelli, C.; Bombardieri, S.; Bazzichi, L.; Dell’Osso, L. Methodological approach to depressive symptoms in fibromyalgia patients. Clin. Exp. Rheumatol 2012, 30, S136–S142. [Google Scholar]
- Bilyukov, R.G.; Nikolov, M.S.; Pencheva, V.P.; Petrova, D.S.; Georgiev, O.B.; Mondeshki, T.L.; Milanova, V.K. Cognitive Impairment and Affective Disorders in Patients with Obstructive Sleep Apnea Syndrome. Front. Psychiatry 2018, 9, 357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haddock, N.; Wells, M.E. The association between treated and untreated obstructive sleep apnea and depression. NeurodiagnJ 2018, 58, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Labarca, G.; Saavedra, D.; Dreyse, J.; Jorquera, J.; Barbe, F. Efficacy of CPAP for improvements in sleepiness, cognition, mood, and quality of life in elderly patients with OSA: Systematic review and meta-analysis of randomized controlled trials. Chest 2020, 158, 751–764. [Google Scholar] [CrossRef] [PubMed]
- Carneiro-Barrera, A.; Amaro-Gahete, F.J.; Sáez-Roca, G.; Martín-Carrasco, C.; Ruiz, J.R.; Buela-Casal, G. Anxiety and Depression in Patients with Obstructive Sleep Apnoea before and after Continuous Positive Airway Pressure: The ADIPOSA Study. J. Clin. Med. 2019, 8, 2099. [Google Scholar] [CrossRef]
- Chiesa, A.; Serretti, A.; Jakobsen, J.C. Mindfulness: Top-down or bottom-up emotion regulation strategy? Clin. Psychol. Rev. 2013, 33, 82–96. [Google Scholar] [CrossRef]
- Goyal, M.; Singh, S.; Sibinga, E.M.; Gould, N.F.; Rowland-Seymour, A.; Sharma, R.; Berger, Z.; Sleicher, D.; Maron, D.D.; Shihab, H.M.; et al. Meditation programs for psychological stress and well-being: A systematic review and meta-analysis. JAMA Intern. Med. 2014, 174, 357–368. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Huang, X.; Su, J.; Wang, Y. Mindfulness may be a novel factor associated with CPAP adherence in OSAHS patients. Sleep Breath. 2020, 24, 183–190. [Google Scholar] [CrossRef]
- Gross, J.J. The Emerging Field of Emotion Regulation: An Integrative Review. Rev. Gen. Psychol. 1998, 2, 271–299. [Google Scholar] [CrossRef]
- Cunningham, T.J.; Kishore, D.; Guo, M.; Igue, M.; Malhotra, A.; Stickgold, R.; Djonlagic, I. The Effect of Obstructive Sleep Apnea on Sleep-Dependent Emotional Memory Consolidation. Ann. Am. Thorac. Soc. 2022, 10, 1513. [Google Scholar] [CrossRef]
- Huberty, J.L.; Green, J.; Puzia, M.E.; Larkey, L.; Laird, B.; Vranceanu, A.M.; Vlisides-Henry, R.; Irwin, M.R. Testing a mindfulness meditation mobile app for the treatment of sleep-related symptoms in adults with sleep disturbance: A randomized controlled trial. PLoS ONE 2021, 16, e0244717. [Google Scholar] [CrossRef] [PubMed]
- Gao, M.; Roy, A.; Deluty, A.; Sharkey, K.M.; Hoge, E.A.; Liu, T.; Brewer, J.A. Targeting Anxiety to Improve Sleep Disturbance: A Randomized Clinical Trial of App-Based Mindfulness Training. Psychosom. Med. 2022, 84, 632–642. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Problem | Solution |
|---|---|
| Leaks | Better fitting of the mask For the nose mask, use a chinstrap for mouth leaks Try different mask |
| Skin lesions | Better fitting of the mask Try different mask Topical application of products for skin issues |
| Rhinitis | If existed previously:
|
| Conjunctivitis | Better fitting of the mask Try different mask |
| Dry mouth | Better fitting of the mask For nose mask, use a chinstrap for mouth leaks Try oronasal mask Humidification |
| Noise | Better fitting of the mask |
| Aerophagia | Better fitting of the mask A transient problem usually |
| Removal during the night involuntary | Better fitting of the mask to avoid leaks Try different mask Explain that nothing will happen Set an alarm clock in order to put on the mask |
| Cold air | Humidification |
| Claustrophobia | Select smaller interfaces such as a nasal pillows or nasal masks Wear CPAP while awake and practice breathing through the mask during the day while reading a book, watching TV Gradually increasing the time of use Select Ramp facility and Expiratory Pressure Relief |
| Anxiety, phobia, negative social aspects | Psychotherapy Enhance self-efficacy |
| Education | Educational material (leaflets, videos) by one-on-one clinic visits, group meetings, telephone calls, telemedicine interactions, official internet sites |
| Behavioral Interventions | Cognitive behavioral therapy (CBT) Motivational enhancement therapy (MET), |
| Telemonitoring | Data on treatment effectiveness and level of adherence. Possible mask leaks, residual respiratory events, CPAP use duration |
| Explain about OSA and its impact on patients’ health if left untreated |
| Suggest lifestyle changes such as weight loss, sleep hygiene |
| Explaining the importance of treatment with CPAP |
| CPAP device demonstration: different types of masks, humidifier, ramp |
| Discuss a follow-up plan (short-term and long-term: face-to-face, telephone, telemedicine) |
| Solve practical issues with CPAP (see Table 1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pataka, A.; Kotoulas, S.C.; Gavrilis, P.R.; Karkala, A.; Tzinas, A.; Stefanidou, A. Adherence to CPAP Treatment: Can Mindfulness Play a Role? Life 2023, 13, 296. https://doi.org/10.3390/life13020296
Pataka A, Kotoulas SC, Gavrilis PR, Karkala A, Tzinas A, Stefanidou A. Adherence to CPAP Treatment: Can Mindfulness Play a Role? Life. 2023; 13(2):296. https://doi.org/10.3390/life13020296
Chicago/Turabian StylePataka, Athanasia, Seraphim Chrysovalantis Kotoulas, Panagiotis Raphael Gavrilis, Alice Karkala, Asterios Tzinas, and Aimiliza Stefanidou. 2023. "Adherence to CPAP Treatment: Can Mindfulness Play a Role?" Life 13, no. 2: 296. https://doi.org/10.3390/life13020296
APA StylePataka, A., Kotoulas, S. C., Gavrilis, P. R., Karkala, A., Tzinas, A., & Stefanidou, A. (2023). Adherence to CPAP Treatment: Can Mindfulness Play a Role? Life, 13(2), 296. https://doi.org/10.3390/life13020296