
Clear Aligners and Smart Eye Tracking Technology as a New Communication Strategy between Ethical and Legal Issues



Abstract
:1. Introduction
2. Materials and Methods
3. Results
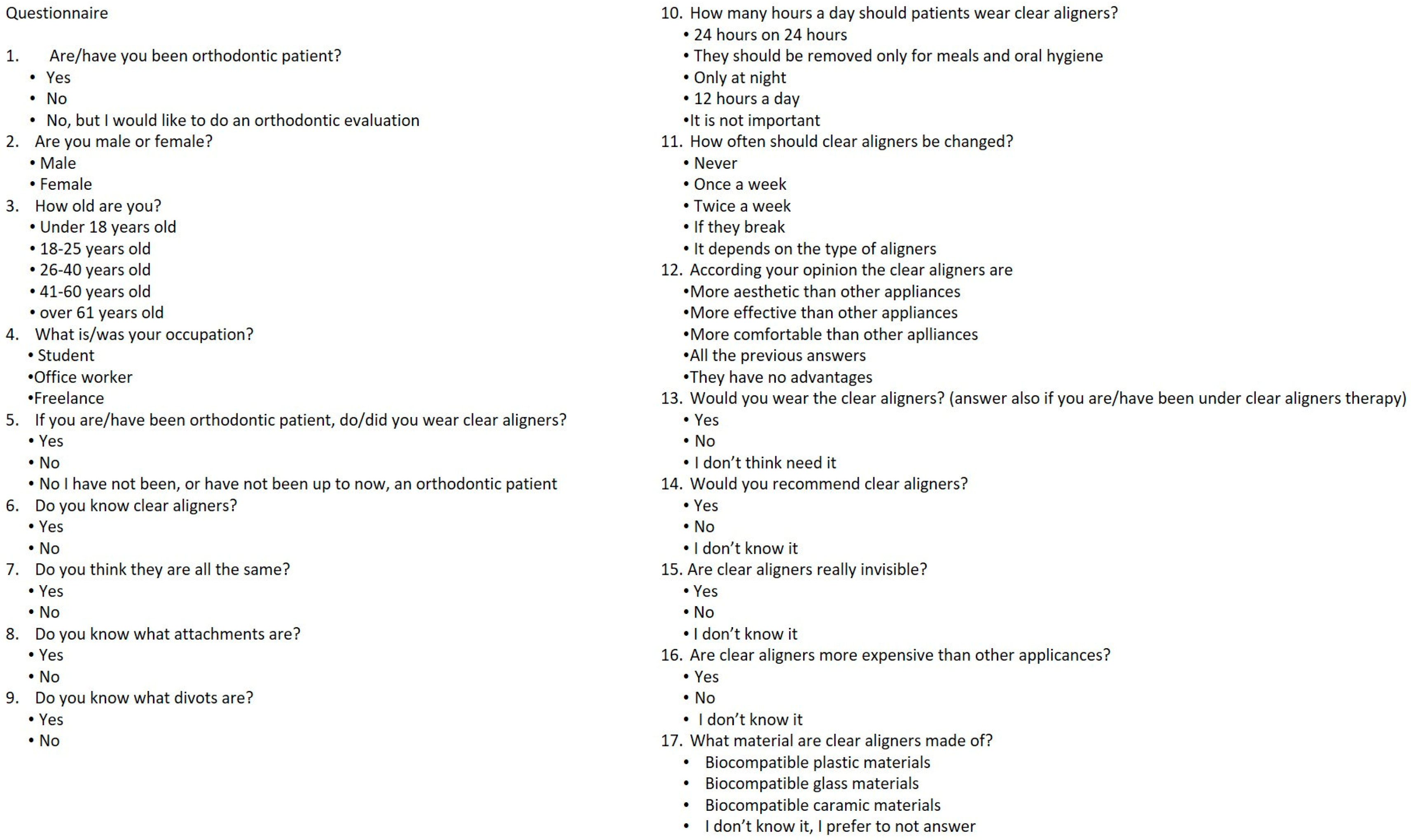
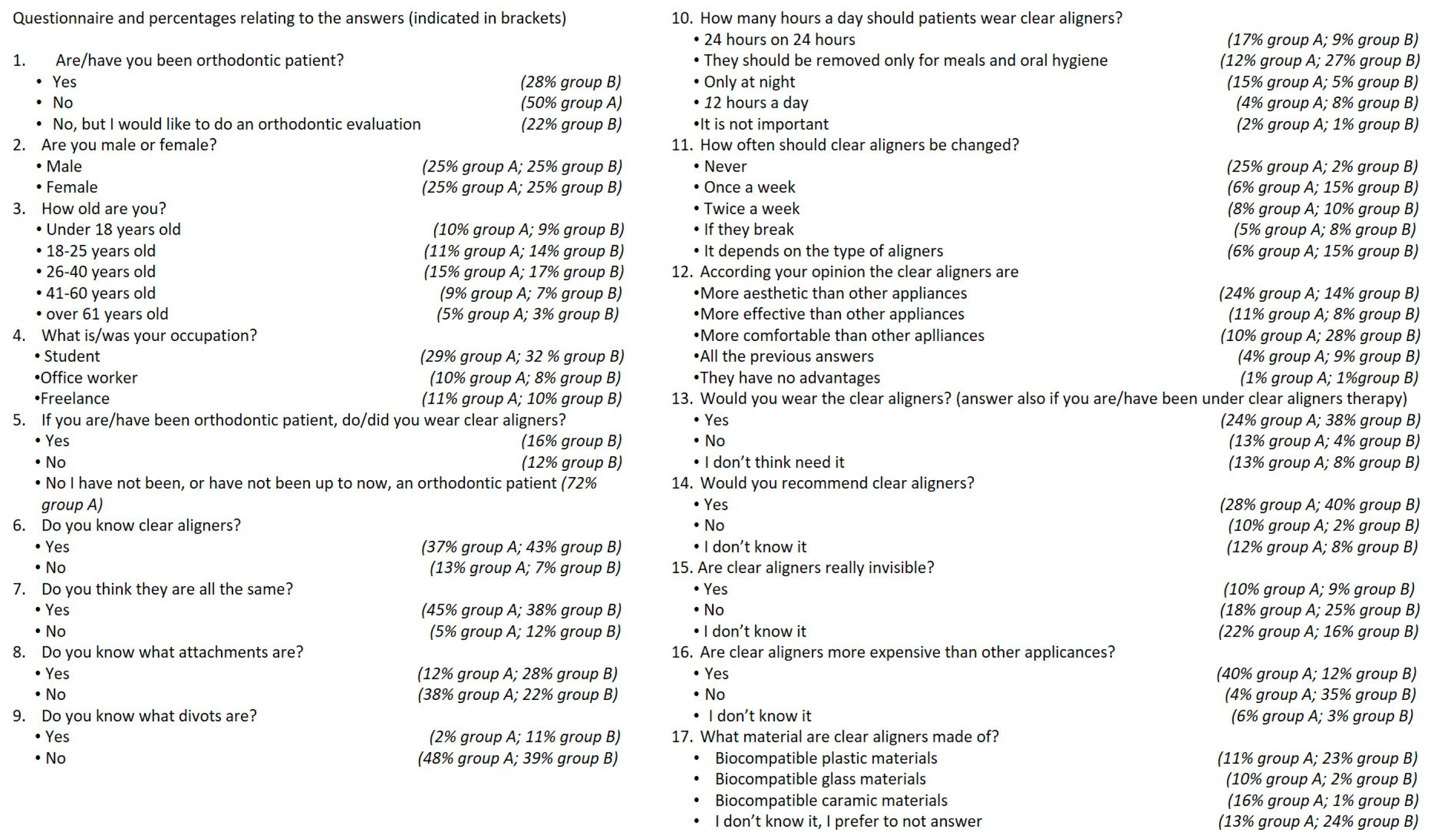
3.1. Answers to the Questionnaire
3.2. Statistical Analysis Applied to the Questionnaire Answers
3.3. Statistical Analysis Applied to First Point Gaze Time, Longest Fixation Time and Overall Gaze Time
3.4. Statistical Analysis Applied to Star Rating, First-Point Gaze Time, Longest Fixation Time, Overall Gaze Time
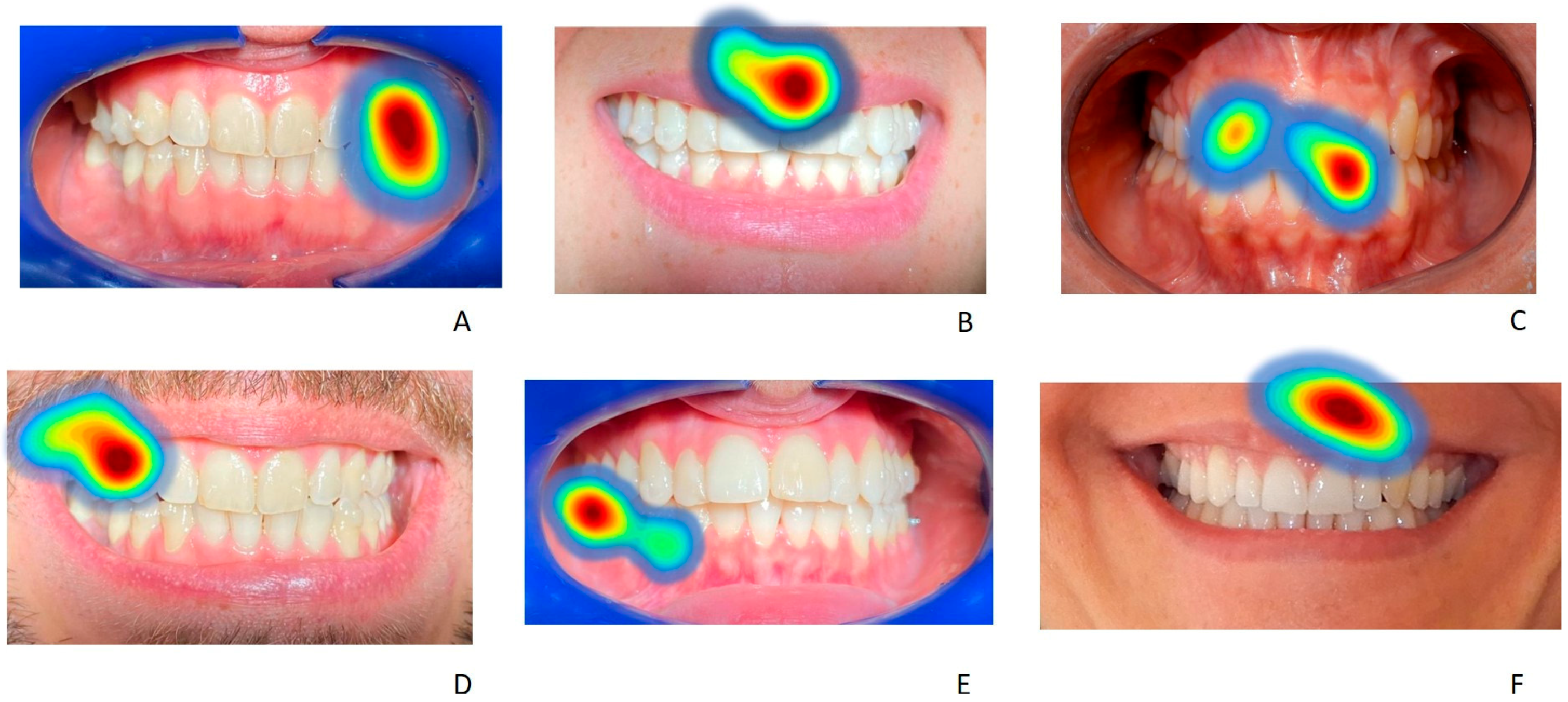
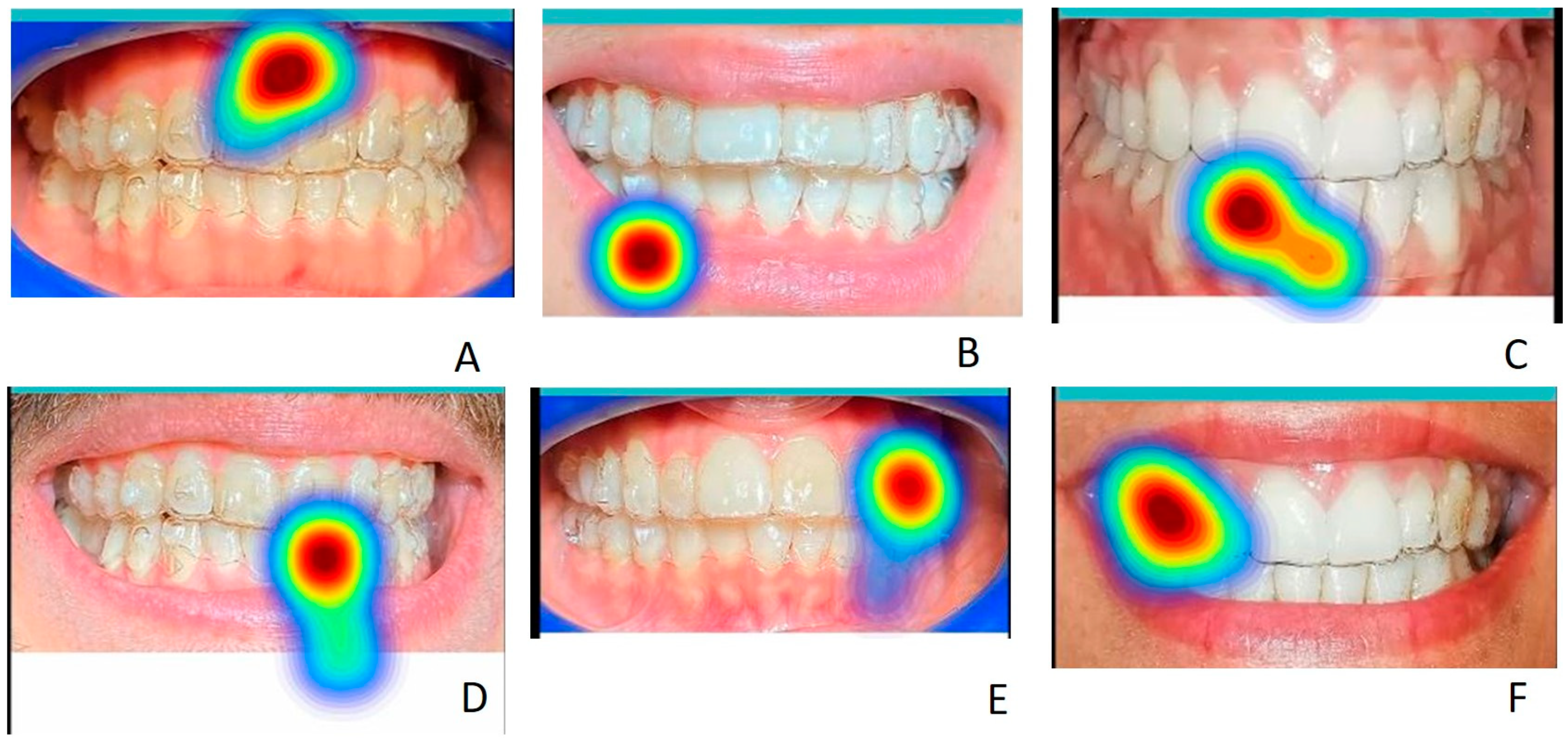
3.5. Statistical Analysis Applied to Initial Fixation Points and Longer Fixation Points in the Different Areas of Interest for Each Image
3.6. First Gaze Point and Areas of Interest: Comparisons Based on Groups and Images
3.7. Longest Gaze Point and Areas of Interest: Comparisons between Groups and Images
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Al Hamad, K.Q.; Almohammed, S.N.; Baba, N.Z. Analysis of the Effect Magnitude of Different Parameters on Smile Attractiveness. J. Esthet. Restor. Dent. 2022, 34, 888–896. [Google Scholar] [CrossRef] [PubMed]
- Horn, S.; Matuszewska, N.; Gkantidis, N.; Verna, C.; Kanavakis, G. Smile Dimensions Affect Self-Perceived Smile Attractiveness. Sci. Rep. 2021, 11, 2779. [Google Scholar] [CrossRef]
- Koidou, V.P.; Chatzopoulos, G.S.; Rosenstiel, S.F. Quantification of Facial and Smile Esthetics. J. Prosthet. Dent. 2018, 119, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Reis, G.M.; de Freitas, D.S.; Oliveira, R.C.; de Oliveira, R.C.G.; Pinzan-Vercelino, C.R.M.; Freitas, K.M.S.; Valarelli, F.P. Smile Attractiveness in Class III Patients after Orthodontic Camouflage or Orthognathic Surgery. Clin. Oral. Investig. 2021, 25, 6791–6797. [Google Scholar] [CrossRef] [PubMed]
- Soh, J.; Wang, Z.D.; Zhang, W.B.; Kau, C.H. Smile Attractiveness Evaluation of Patients Selected for a U.S.-Based Board Certification Examination. Eur. J. Dent. 2021, 15, 630–638. [Google Scholar] [CrossRef]
- Kumar, M.; Goyal, M.; Kaur, A.; Abrar, M. Smile Attractiveness after Orthodontic Treatment. Am. J. Orthod. Dentofac. Orthop. 2020, 158, 474–475. [Google Scholar] [CrossRef]
- Golshah, A.; Serenjianeh, A.M.; Imani, M.M. Smile Attractiveness of Persian Women after Orthodontic Treatment. Am. J. Orthod. Dentofac. Orthop. 2020, 158, 75–83. [Google Scholar] [CrossRef]
- Sriphadungporn, C.; Chamnannidiadha, N. Perception of Smile Esthetics by Laypeople of Different Ages. Prog. Orthod. 2017, 18, 8. [Google Scholar] [CrossRef] [Green Version]
- Almanea, R.; Modimigh, A.; Almogren, F.; Alhazzani, E. Perception of Smile Attractiveness among Orthodontists, Restorative Dentists, and Laypersons in Saudi Arabia. J. Conserv. Dent. 2019, 22, 69–75. [Google Scholar] [CrossRef]
- Silva, C.O.; Rezende, R.I.; Mazuquini, A.C.; Leal, V.C.; Amaral, G.S.A.; Guo, X.; Tatakis, D.N. Aesthetic Crown Lengthening and Lip Repositioning Surgery: Pre- and Post-Operative Assessment of Smile Attractiveness. J. Clin. Periodontol. 2021, 48, 826–833. [Google Scholar] [CrossRef]
- Mollabashi, V.; Abolvardi, M.; Akhlaghian, M.; Ghaffari, M.I. Smile Attractiveness Perception Regarding Buccal Corridor Size among Different Facial Types. Dent. Med. Probl. 2018, 55, 305–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mota Júnior, S.L.; Alvim, L.P.; Munck, I.S.; da Silva Campos, M.J.; Vitral, R.W.F. Evaluation of Smile Attractiveness with Mesiodistal Variations of the Upper Lateral Incisors. J. Clin. Orthod. 2021, 55, 750–756. [Google Scholar] [PubMed]
- Dobreva, D.; Gkantidis, N.; Halazonetis, D.; Verna, C.; Kanavakis, G. Smile Reproducibility and Its Relationship to Self-Perceived Smile Attractiveness. Biology 2022, 11, 719. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.A.; Fields, H.W.; Beck, F.M.; Springer, N.C.; Firestone, A.R.; Rosenstiel, S.; Christensen, J.C. Smile Esthetics from Patients’ Perspectives for Faces of Varying Attractiveness. Am. J. Orthod. Dentofac. Orthop. 2011, 140, e171–e180. [Google Scholar] [CrossRef] [PubMed]
- Masch, L.; Gassner, A.; Rosar, U. Can a Beautiful Smile Win the Vote? The Role of Candidates’ Physical Attractiveness and Facial Expressions in Elections. Politics Life Sci. 2021, 40, 213–223. [Google Scholar] [CrossRef]
- Shan, B.; Werger, M.; Huang, W.; Giddon, D.B. Quantitating the Art and Science of Esthetic Clinical Success. J. World Fed. Orthod. 2021, 10, 49–58. [Google Scholar] [CrossRef]
- Kalsi, H.; Khan, A.; Bomfim, D.; Tsakos, G.; McDonald, A.V.; Rodriguez, J.M. Quality of Life and Other Psychological Factors in Patients with Tooth Wear. Br. Dent. J. 2021. [Google Scholar] [CrossRef]
- Richard, A.; Harbeck, N.; Wuerstlein, R.; Wilhelm, F.H. Recover Your Smile: Effects of a Beauty Care Intervention on Depressive Symptoms, Quality of Life, and Self-Esteem in Patients with Early Breast Cancer. Psychooncology 2019, 28, 401–407. [Google Scholar] [CrossRef]
- Mathur, V.P.; Dhillon, J.K. Dental Caries: A Disease Which Needs Attention. Indian J. Pediatr. 2018, 85, 202–206. [Google Scholar] [CrossRef]
- Baiju, R.M.; Peter, E.; Varghese, N.O.; Sivaram, R. Oral Health and Quality of Life: Current Concepts. J. Clin. Diagn. Res. 2017, 11, ZE21–ZE26. [Google Scholar] [CrossRef]
- Putrino, A.; Abed, M.R.; Barbato, E.; Galluccio, G. A Current Tool in Facial Aesthetics Perception of Orthodontic Patient: The Digital Warping. Dent. Cadmos 2021, 89, 46. [Google Scholar] [CrossRef]
- Alansari, R.A. Youth Perception of Different Orthodontic Appliances. Patient Prefer Adherence 2020, 14, 1011–1019. [Google Scholar] [CrossRef] [PubMed]
- Alansari, R.A.; Faydhi, D.A.; Ashour, B.S.; Alsaggaf, D.H.; Shuman, M.T.; Ghoneim, S.H.; Linjawi, A.I.; Marghalani, H.Y.; Dause, R.R. Adult Perceptions of Different Orthodontic Appliances. Patient Prefer Adherence 2019, 13, 2119–2128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolas-Colvee, B.; Tarazona, B.; Paredes-Gallardo, V.; Arias-De Luxan, S. Relationship between Perception of Smile Esthetics and Orthodontic Treatment in Spanish Patients. PLoS ONE 2018, 13, e0201102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iared, W.; Koga da Silva, E.M.; Iared, W.; Rufino Macedo, C. Esthetic Perception of Changes in Facial Profile Resulting from Orthodontic Treatment with Extraction of Premolars: A Systematic Review. J. Am. Dent. Assoc. 2017, 148, 9–16. [Google Scholar] [CrossRef]
- Kuhlman, D.C.; de Lima, T.A.; Duplat, C.B.; Capelli, J. Esthetic Perception of Orthodontic Appliances by Brazilian Children and Adolescents. Dent. Press J. Orthod. 2016, 21, 58–66. [Google Scholar] [CrossRef] [Green Version]
- Meade, M.J.; Weir, T. A Survey of Orthodontic Clear Aligner Practices among Orthodontists. Am. J. Orthod. Dentofac. Orthop. 2022, 162, e302–e311. [Google Scholar] [CrossRef]
- Cardoso, P.C.; Espinosa, D.G.; Mecenas, P.; Flores-Mir, C.; Normando, D. Pain Level between Clear Aligners and Fixed Appliances: A Systematic Review. Prog. Orthod. 2020, 21, 3. [Google Scholar] [CrossRef] [Green Version]
- Gasparello, G.G.; Júnior, S.L.M.; Hartmann, G.C.; Meira, T.M.; Camargo, E.S.; Pithon, M.M.; Tanaka, O. The Influence of Malocclusion on Social Aspects in Adults: Study via Eye Tracking Technology and Questionnaire. Prog. Orthod. 2022, 23, 4. [Google Scholar] [CrossRef]
- Försch, M.; Krull, L.; Hechtner, M.; Rahimi, R.; Wriedt, S.; Wehrbein, H.; Jacobs, C.; Jacobs, C. Perception of Esthetic Orthodontic Appliances: An Eye Tracking and Cross-Sectional Study. Angle Orthod. 2020, 90, 109–117. [Google Scholar] [CrossRef]
- Thai, J.K.; Araujo, E.; McCray, J.; Schneider, P.P.; Kim, K.B. Esthetic Perception of Clear Aligner Therapy Attachments Using Eye-Tracking Technology. Am. J. Orthod. Dentofac. Orthop. 2020, 158, 400–409. [Google Scholar] [CrossRef]
- Holmqvist, K.; Örbom, S.L.; Hooge, I.T.C.; Niehorster, D.C.; Alexander, R.G.; Andersson, R.; Benjamins, J.S.; Blignaut, P.; Brouwer, A.-M.; Chuang, L.L.; et al. Eye Tracking: Empirical Foundations for a Minimal Reporting Guideline. Behav. Res. Methods 2022. [Google Scholar] [CrossRef]
- Fuentes, S.; Gonzalez Viejo, C.; Torrico, D.D.; Dunshea, F.R. Digital Integration and Automated Assessment of Eye-Tracking and Emotional Response Data Using the BioSensory App to Maximize Packaging Label Analysis. Sensors 2021, 21, 7641. [Google Scholar] [CrossRef]
- Bissoli, A.; Lavino-Junior, D.; Sime, M.; Encarnação, L.; Bastos-Filho, T. A Human−Machine Interface Based on Eye Tracking for Controlling and Monitoring a Smart Home Using the Internet of Things. Sensors 2019, 19, 859. [Google Scholar] [CrossRef] [Green Version]
- Golparvar, A.J.; Yapici, M.K. Toward Graphene Textiles in Wearable Eye Tracking Systems for Human-Machine Interaction. Beilstein J. Nanotechnol. 2021, 12, 180–189. [Google Scholar] [CrossRef]
- Vodrahalli, K.; Filipkowski, M.; Chen, T.; Zou, J.; Liao, Y.J. Predicting Visuo-Motor Diseases from Eye Tracking Data. Pac. Symp. Biocomput. 2022, 27, 242–253. [Google Scholar]
- de Bougrenet de la Tocnaye, J.-L.; Nourrit, V.; Lahuec, C. Design of a Multimodal Oculometric Sensor Contact Lens. Sensors 2022, 22, 6731. [Google Scholar] [CrossRef]
- Wästlund, E.; Sponseller, K.; Pettersson, O.; Bared, A. Evaluating Gaze-Driven Power Wheelchair with Navigation Support for Persons with Disabilities. J. Rehabil Res. Dev. 2015, 52, 815–826. [Google Scholar] [CrossRef]
- Kankam, H.K.N.; Gupta, H.; Sawh-Martinez, R.; Steinbacher, D.M. Segmental Multiple-Jaw Surgery without Orthodontia: Clear Aligners Alone. Plast Reconstr. Surg. 2018, 142, 181–184. [Google Scholar] [CrossRef]
- Zhang, W.; Liu, H. Toward a Reliable Collection of Eye-Tracking Data for Image Quality Research: Challenges, Solutions, and Applications. IEEE Trans. Image Process 2017, 26, 2424–2437. [Google Scholar] [CrossRef] [Green Version]
- Vozzi, A.; Ronca, V.; Aricò, P.; Borghini, G.; Sciaraffa, N.; Cherubino, P.; Trettel, A.; Babiloni, F.; Di Flumeri, G. The Sample Size Matters: To What Extent the Participant Reduction Affects the Outcomes of a Neuroscientific Research. A Case-Study in Neuromarketing Field. Sensors 2021, 21, 6088. [Google Scholar] [CrossRef] [PubMed]
- Law Decree n. 211 Enacted on 24 June 2003. Attuazione Della Direttiva 2001/20/CE Relativa All’applicazione Della Buona Pratica Clinica Nell’esecuzione Delle Sperimentazioni Cliniche di Medicinali per uso Clinico. (GU Serie Generale n.184 del 09-08-2003—Suppl. Ordinario n. 130), Came into Force 1st January 2004. Available online: https://www.gazzettaufficiale.it/eli/id/2003/08/09/003G0229/sg (accessed on 22 November 2022).
- Ministry of Health Decree 13A03474. Criteri per la Composizione e il Funzionamento dei Comitati Etici. Issued on 8 February 2013. Available online: https://www.gazzettaufficiale.it/eli/id/2013/04/24/13A03474/sg (accessed on 26 November 2022).
- Law Decree n. 139 Enacted on 8 October 2021. Disposizioni Urgenti per L’accesso Alle Attivita’ Culturali, Sportive e Ricreative, Nonche’ per L’organizzazione di Pubbliche Amministrazioni e in Materia di Protezione dei Dati Personali. Came into Force 9 October 2021. Available online: http://documenti.camera.it/leg18/dossier/pdf/D21139b.pdf?_1674054553792 (accessed on 26 November 2022).
- Regulation (EU) 2016/679 of the European Parliament and of the Council, passed on 27th April 2016, on the Protection of Natural Persons with Regard to the Processing of Personal Data and on the Free Movement of Such Data, and Repealing Directive 95/46/EC (General Data Protection Regulation). Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32016R0679&from=IT (accessed on 22 November 2022).
- Jaber, S.T.; Hajeer, M.Y.; Burhan, A.S. The Effectiveness of In-House Clear Aligners and Traditional Fixed Appliances in Achieving Good Occlusion in Complex Orthodontic Cases: A Randomized Control Clinical Trial. Cureus 2022, 14, e30147. [Google Scholar] [CrossRef] [PubMed]
- Mampieri, G.; Condò, R.; Di Caccamo, G.; Pirelli, P.; Giancotti, A. Clear Aligner Treatments in Orthoperio Patients. Case Rep. Dent. 2022, 2022, 8932770. [Google Scholar] [CrossRef] [PubMed]
- Long, H.; Wu, Z.; Yan, X.; Wang, Q.; Liu, L.; Wang, Y.; Jian, F.; Liao, L.; Li, X.; Lai, W. An Objective System for Appraising Clear Aligner Treatment Difficulty: Clear Aligner Treatment Complexity Assessment Tool (CAT-CAT). BMC Oral. Health 2020, 20, 312. [Google Scholar] [CrossRef] [PubMed]
- Putrino, A.; Barbato, E.; Galluccio, G. Clear Aligners: Between Evolution and Efficiency-A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 2870. [Google Scholar] [CrossRef]
- Nucera, R.; Dolci, C.; Bellocchio, A.M.; Costa, S.; Barbera, S.; Rustico, L.; Farronato, M.; Militi, A.; Portelli, M. Effects of Composite Attachments on Orthodontic Clear Aligners Therapy: A Systematic Review. Materials 2022, 15, 533. [Google Scholar] [CrossRef]
- Mencattelli, M.; Donati, E.; Cultrone, M.; Stefanini, C. Novel Universal System for 3-Dimensional Orthodontic Force-Moment Measurements and Its Clinical Use. Am. J. Orthod. Dentofac. Orthop. 2015, 148, 174–183. [Google Scholar] [CrossRef]
- D’Alessandro, A.C.; D’Antò, V.; Razionale, A.V.; Allesandri-Bonetti, G. Integrating CBCT and Virtual Models for Root Movement with Clear Aligners. J. Clin. Orthod. 2020, 54, 159–166. [Google Scholar]
- Putrino, A.; Abed, M.R.; Lilli, C. Clear Aligners with Differentiated Thickness and without Attachments—A Case Report. J. Clin. Exp. Dent. 2022, 14, e514–e519. [Google Scholar] [CrossRef]
- Weckmann, J.; Scharf, S.; Graf, I.; Schwarze, J.; Keilig, L.; Bourauel, C.; Braumann, B. Influence of Attachment Bonding Protocol on Precision of the Attachment in Aligner Treatments. J. Orofac. Orthop. 2020, 81, 30–40. [Google Scholar] [CrossRef]
- Cowley, D.P.; Mah, J.; O’Toole, B. The Effect of Gingival-Margin Design on the Retention of Thermoformed Aligners. J. Clin. Orthod. 2012, 46, 697–702; quiz 705. [Google Scholar]
- Bucci, R.; Rongo, R.; Levatè, C.; Michelotti, A.; Barone, S.; Razionale, A.V.; D’Antò, V. Thickness of Orthodontic Clear Aligners after Thermoforming and after 10 Days of Intraoral Exposure: A Prospective Clinical Study. Prog. Orthod. 2019, 20, 36. [Google Scholar] [CrossRef] [Green Version]
- Nowak, C.-M.; Othman, A.; Ströbele, D.-A.; von See, C. Comparative Mechanical Testing for Different Orthodontic Aligner Materials over Time—In Vitro Study. J. Clin. Exp. Dent. 2022, 14, e457–e463. [Google Scholar] [CrossRef]
- Panova, T.; Carbonell, X. Is Smartphone Addiction Really an Addiction? J. Behav. Addict. 2018, 7, 252–259. [Google Scholar] [CrossRef]
- Thomas, M.; Sindwani, G.; Suri, A. Smartphone Smart Apps—Breaking the Communication Barriers. Ann. Card. Anaesth. 2020, 23, 379–380. [Google Scholar] [CrossRef]
- Abi-Jaoude, E.; Naylor, K.T.; Pignatiello, A. Smartphones, Social Media Use and Youth Mental Health. CMAJ 2020, 192, E136–E141. [Google Scholar] [CrossRef] [Green Version]
- Marañón-Vásquez, G.A.; da Costa Barreto, L.S.; Pithon, M.M.; Nojima, L.I.; Nojima, M.D.; de Souza Araújo, M.T.; de Souza, M.M. Reasons Influencing the Preferences of Prospective Patients and Orthodontists for Different Orthodontic Appliances. Korean J. Orthod. 2021, 51, 115–125. [Google Scholar] [CrossRef]
- d’Apuzzo, F.; Perillo, L.; Carrico, C.K.; Castroflorio, T.; Grassia, V.; Lindauer, S.J.; Shroff, B. Clear Aligner Treatment: Different Perspectives between Orthodontists and General Dentists. Prog. Orthod. 2019, 20, 10. [Google Scholar] [CrossRef] [Green Version]
- Linjawi, A.I.; Alsadat, M.A.; Othman, M.A.; Fakhry, L.M.; Basalaim, A.S.; Alansari, R.A.; Abushal, A.M.; Baeshen, H.A. Awareness, Perception and Readiness Regarding Clear Aligner Therapy among Orthodontists and Other Dental Specialists. J. Biol. Regul. Homeost. Agents 2020, 34, 1061–1066. [Google Scholar] [CrossRef]
- Heath, E.M.; English, J.D.; Johnson, C.D.; Swearingen, E.B.; Akyalcin, S. Perceptions of Orthodontic Case Complexity among Orthodontists, General Practitioners, Orthodontic Residents, and Dental Students. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 335–341. [Google Scholar] [CrossRef]
- Ben Gassem, A.A. Does Clear Aligner Treatment Result in Different Patient Perceptions of Treatment Process and Outcomes Compared to Conventional/Traditional Fixed Appliance Treatment: A Literature Review. Eur. J. Dent. 2022, 16, 274–285. [Google Scholar] [CrossRef] [PubMed]
- Celine, G.R.; Cho, V.V.Y.; Kogan, A.; Anthonappa, R.P.; King, N.M. Eye-Tracking in Dentistry: What Do Children Notice in the Dental Operatory? Clin. Oral. Investig. 2021, 25, 3663–3668. [Google Scholar] [CrossRef] [PubMed]
- Kröger, J.L.; Lutz, O.H.-M.; Müller, F. What Does Your Gaze Reveal About You? On the Privacy Implications of Eye Tracking. In Privacy and Identity Management. Data for Better Living: AI and Privacy; Friedewald, M., Önen, M., Lievens, E., Krenn, S., Fricker, S., Eds.; Springer International Publishing: Cham, Switzerland, 2020; Volume 576, pp. 226–241. ISBN 9783030425036. [Google Scholar]
- Wang, C.-Y.; Tsai, M.-J.; Tsai, C.-C. Multimedia Recipe Reading: Predicting Learning Outcomes and Diagnosing Cooking Interest Using Eye-Tracking Measures. Comput. Hum. Behav. 2016, 62, 9–18. [Google Scholar] [CrossRef]
- Pechtel, P.; Pizzagalli, D.A. Effects of Early Life Stress on Cognitive and Affective Function: An Integrated Review of Human Literature. Psychopharmacology 2011, 214, 55–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, A.; Xia, L.; Duchowski, A.; Bailey, R.; Holmqvist, K.; Jain, E. Differential privacy for eye-tracking data. In Proceedings of the 11th ACM Symposium on Eye Tracking Research & Applications (ETRA ‘19), Denver, CO, USA, 25–28 June 2019; Association for Computing Machinery: New York, NY, USA, 2019; p. 28. [Google Scholar] [CrossRef]
- Swann, L.; Popovic, V.; Blackler, A.; Thompson, H. Airport Security Screener Problem-Solving Knowledge and Implications. Hum. Factors 2020, 62, 1265–1285. [Google Scholar] [CrossRef] [PubMed]
- Bafna, T.; Hansen, J.P. Mental Fatigue Measurement Using Eye Metrics: A Systematic Literature Review. Psychophysiology 2021, 58, e13828. [Google Scholar] [CrossRef]
- Heuer, S.; Pinke, M.L. Development of an Eye-Tracking Method to Assess Mental Set Switching in People with Aphasia. Brain Inj. 2017, 31, 686–696. [Google Scholar] [CrossRef]
- Wolf, A.; Ueda, K. Contribution of Eye-Tracking to Study Cognitive Impairments Among Clinical Populations. Front. Psychol. 2021, 12, 590986. [Google Scholar] [CrossRef]
- Ceh, S.M.; Annerer-Walcher, S.; Koschutnig, K.; Körner, C.; Fink, A.; Benedek, M. Neurophysiological Indicators of Internal Attention: An FMRI-Eye-Tracking Coregistration Study. Cortex 2021, 143, 29–46. [Google Scholar] [CrossRef]
- García-Baos, A.; D’Amelio, T.; Oliveira, I.; Collins, P.; Echevarria, C.; Zapata, L.P.; Liddle, E.; Supèr, H. Novel Interactive Eye-Tracking Game for Training Attention in Children with Attention-Deficit/Hyperactivity Disorder. Prim. Care Companion CNS Disord. 2019, 21, 19m02428. [Google Scholar] [CrossRef]
- Mesmoudi, S.; Hommet, S.; Peschanski, D. Eye-Tracking and Learning Experience: Gaze Trajectories to Better Understand the Behavior of Memorial Visitors. J. Eye Mov. Res. 2020, 13. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.S.; Lee, T.-L.; Sze, S.L.; Yang, N.S.; Han, Y.M.Y. Eye-Tracking Training Improves the Learning and Memory of Children with Learning Difficulty. Sci. Rep. 2022, 12, 13974. [Google Scholar] [CrossRef] [PubMed]
- Ashraf, H.; Sodergren, M.H.; Merali, N.; Mylonas, G.; Singh, H.; Darzi, A. Eye-Tracking Technology in Medical Education: A Systematic Review. Med. Teachnol. 2018, 40, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Scharinger, C.; Schüler, A.; Gerjets, P. Using Eye-Tracking and EEG to Study the Mental Processing Demands during Learning of Text-Picture Combinations. Int. J. Psychophysiol. 2020, 158, 201–214. [Google Scholar] [CrossRef] [PubMed]
- Howell, D.R.; Brilliant, A.N.; Master, C.L.; Meehan, W.P. Reliability of Objective Eye-Tracking Measures Among Healthy Adolescent Athletes. Clin. J. Sport Med. 2020, 30, 444–450. [Google Scholar] [CrossRef]
- Toole, A.J.; Fogt, N. Review: Head and Eye Movements and Gaze Tracking in Baseball Batting. Optom. Vis. Sci. 2021, 98, 750–758. [Google Scholar] [CrossRef]
- Rassweiler, J.J.; Autorino, R.; Klein, J.; Mottrie, A.; Goezen, A.S.; Stolzenburg, J.-U.; Rha, K.H.; Schurr, M.; Kaouk, J.; Patel, V.; et al. Future of Robotic Surgery in Urology. BJU Int. 2017, 120, 822–841. [Google Scholar] [CrossRef] [Green Version]
- Gremsl, A.; Schwab, D.; Höfler, C.; Schienle, A. Placebo Effects in Spider Phobia: An Eye-Tracking Experiment. Cogn. Emot. 2018, 32, 1571–1577. [Google Scholar] [CrossRef] [Green Version]
- Günther, V.; Kropidlowski, A.; Schmidt, F.M.; Koelkebeck, K.; Kersting, A.; Suslow, T. Attentional Processes during Emotional Face Perception in Social Anxiety Disorder: A Systematic Review and Meta-Analysis of Eye-Tracking Findings. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 111, 110353. [Google Scholar] [CrossRef]
- Konovalova, I.; Antolin, J.V.; Bolderston, H.; Gregory, N.J. Adults with Higher Social Anxiety Show Avoidant Gaze Behaviour in a Real-World Social Setting: A Mobile Eye Tracking Study. PLoS ONE 2021, 16, e0259007. [Google Scholar] [CrossRef]
- Bek, J.; Poliakoff, E.; Lander, K. Measuring Emotion Recognition by People with Parkinson’s Disease Using Eye-Tracking with Dynamic Facial Expressions. J. Neurosci. Methods 2020, 331, 108524. [Google Scholar] [CrossRef]
- Davis, R. The Feasibility of Using Virtual Reality and Eye Tracking in Research with Older Adults with and without Alzheimer’s Disease. Front. Aging Neurosci. 2021, 13, 607219. [Google Scholar] [CrossRef]
- Lotze, A.; Love, K.; Velisar, A.; Shanidze, N.M. A Low-Cost Robotic Oculomotor Simulator for Assessing Eye Tracking Accuracy in Health and Disease. Behav. Res. Methods 2022. [Google Scholar] [CrossRef]
- Cognolato, M.; Atzori, M.; Müller, H. Head-Mounted Eye Gaze Tracking Devices: An Overview of Modern Devices and Recent Advances. J. Rehabil. Assist Technol. Eng. 2018, 5, 2055668318773991. [Google Scholar] [CrossRef]
- Bozkir, E.; Günlü, O.; Fuhl, W.; Schaefer, R.F.; Kasneci, E. Differential Privacy for Eye Tracking with Temporal Correlations. PLoS ONE 2021, 16, e0255979. [Google Scholar] [CrossRef]
- David-John, B.; Hosfelt, D.; Butler, K.; Jain, E. A Privacy-Preserving Approach to Streaming Eye-Tracking Data. IEEE Trans. Vis. Comput. Graph. 2021, 27, 2555–2565. [Google Scholar] [CrossRef]

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Questions | Chi Square Test | p-Value | Meaning | Chi-Square Test with Yates Correction | p-Value | Meaning |
|---|---|---|---|---|---|---|
| Do you know about clear aligners? | 2.25 | 0.133614 | Not significant | 1.5625 | 0.2113 | Not significant |
| Do you think they are all the same? | 3.4727 | 0.062389 | Not significant | 2.5514 | 0.110198 | Not significant |
| Do you know about attachments? | 10.6667 | 0.001091 | Significant | 9.375 | 0.0022 | Significant |
| Do you know about divots? | 7.1618 | 0.007447 | Significant | 5.6587 | 0.017369 | Significant |
| How many hours a day should patients wear aligners? | 14.8974 | 0.004919 | Significant | Not Applicable | 0 | 0 |
| How often should aligners be changed? | 28.2214 | 0.000011 | Significant | Not Applicable | 0 | 0 |
| How would you define clear aligners? | 7.3141 | 0.120194 | Not significant | Not Applicable | 0 | 0 |
| Would you wear clear aligners? (answer also if you are under clear aligner therapy) | 9.1165 | 0.010481 | Significant | Not Applicable | 0 | 0 |
| Would you recommend clear aligners? | 8.251 | 0.016156 | Significant | Not Applicable | 0 | 0 |
| Are clear aligners really invisible? | 2.1395 | 0.343088 | Not significant | Not Applicable | 0 | 0 |
| Are clear aligners more expensive than other appliances? | 40.7179 | <0.00001 | Significant | Not Applicable | 0 | 0 |
| What material are clear aligners made of? | 26.0742 | <0.00001 | Significant | Not Applicable | 0 | 0 |
| First-Point Gaze | Longest Gaze during the Test | Overall Observation Time | ||||
|---|---|---|---|---|---|---|
| Smile | Group A | Group B | Group A | Group B | Group A | Group B |
| 1 | 0.16 | 0.28 | 1.30 | 1.35 | 24 | 22.7 |
| 2 | 0.17 | 0.12 | 1.87 | 1.71 | 19 | 21 |
| 3 | 0.13 | 0.19 | 2 | 1.50 | 21 | 16 |
| 4 | 0.18 | 0.13 | 1.23 | 1.25 | 17.9 | 16 |
| 5 | 0.12 | 0.10 | 1.67 | 1.44 | 21.3 | 22.6 |
| 6 | 0.10 | 0.11 | 1.86 | 1.56 | 19 | 23.1 |
| First-Point Gaze | Longest Gaze during the Test | Overall Observation Time | ||||
|---|---|---|---|---|---|---|
| Smile | Group A | Group B | Group A | Group B | Group A | Group B |
| 1 | 0.26 | 0.39 | 1.43 | 1.36 | 33 | 27.2 |
| 2 | 0.23 | 0.22 | 2.1 | 1.82 | 25 | 23 |
| 3 | 0.19 | 0.25 | 2.13 | 1.91 | 20 | 19.6 |
| 4 | 0.24 | 0.26 | 1.96 | 1.72 | 27 | 25.5 |
| 5 | 0.14 | 0.17 | 1.51 | 1.83 | 26.3 | 26 |
| 6 | 0.18 | 0.16 | 1.77 | 1.52 | 18.6 | 20 |
| t-Test | p | Meaning | |
|---|---|---|---|
| First-point gaze (comparison between groups) | −0.37731 | 0.356915 | Not significant |
| Longest gaze (comparison between groups) | 1.27362 | 0.115803 | Not significant |
| Overall observation time (comparison between groups) | 0.08133 | 0.468391 | Not significant |
| First-point gaze–Longest gaze comparison in A group | −11.54622 | <0.00001 | Significant |
| First-point gaze–Longest gaze comparison in B group | −18.32856 | <0.00001 | Significant |
| First-point gaze–overall observation time in A group | −22.47117 | <0.00001 | Significant |
| First-point gaze–overall observation time in B group | −14.6492 | <0.00001 | Significant |
| Longest gaze–overall observation time comparison in A group | −20.57699 | <0.00001 | Significant |
| Longest gaze–overall observation time comparison in B group | −13.67807 | <0.00001 | Significant |
| t-Test | p | Meaning | |
|---|---|---|---|
| First-point gaze (comparison between groups) | 1.567863 | 0.1777 | Not significant |
| Longest gaze (comparison between groups) | −1.317402 | 0.24484 | Not significant |
| Overall observation time (comparison between groups) | −1.438779 | 0.20974 | Not significant |
| First-point gaze–Longest gaze comparison in A group | 13.291117 | 0.00004 | Significant |
| First-point gaze–Longest gaze comparison in B group | 13.453603 | 0.00004 | Significant |
| First-point gaze–overall observation time in A group | 11.708622 | 0.00008 | Significant |
| First-point gaze–overall observation time in B group | 17.995506 | <0.00001 | Significant |
| Longest gaze–overall observation time comparison in A group | 10.536119 | 0.00013 | Significant |
| Longest gaze–overall observation time comparison in B group | 16.270141 | 0.00002 | Significant |
| t-Test | p | Meaning | |
|---|---|---|---|
| First-point gaze in A group (comparison between images) | −2.84503 | 0.008699 | Significant |
| First-point gaze in B group (comparison between images) | −1.96373 | 0.038976 | Significant |
| Longest gaze in A group (comparison between images) | −0.90427 | 0.193559 | Not significant |
| Longest gaze in B group (comparison between images) | −2.07183 | 0.032542 | Significant |
| Overall observation time in A group (comparison between images) | −1.99944 | 0.036728 | Significant |
| Overall observation time in B group (comparison between images) | −1.74829 | 0.055493 | Not significant |
| Rating in Stars | Group A | Group B |
|---|---|---|
| Smile 1 | 3 | 2 |
| Smile 2 | 2.5 | 2.5 |
| Smile 3 | 3.5 | 4 |
| Smile 4 | 3.5 | 3.5 |
| Smile 5 | 3 | 3 |
| Smile 6 | 4 | 4.5 |
| Rating in Stars | Group A | Group B |
|---|---|---|
| Smile 1 | 2 | 1.5 |
| Smile 2 | 3 | 2.5 |
| Smile 3 | 4.5 | 4.5 |
| Smile 4 | 3 | 3 |
| Smile 5 | 3 | 2 |
| Smile 6 | 5 | 5 |
| Mann–Whitney U Test | p | Meaning | |
|---|---|---|---|
| Rating in stars comparison between groups for images without clear aligners worn | U = 18 | 5 | Not significant |
| Rating in stars comparison between groups for images with clear aligners worn | U = 14 | 5 | Not significant |
| Rating in stars comparison between images with and without clear aligners worn in group A | U = 18 | 5 | Not significant |
| Rating in stars comparison between images with and without clear aligners worn in group B | U = 16 | 5 | Not significant |
| Spearman’s rho test (rs) | |||
| Rating in stars comparison with first-point gaze in group A for images without clear aligners worn | −0.2354 | 0.65343 | Not significant |
| Rating in stars comparison with first-point gaze in group A for images with clear aligners worn | −0.63754 | 0.17326 | Not sig-nificant |
| Rating in stars comparison with first-point gaze in group B for images without clear aligners worn | −0.54286 | 0.2657 | Not significant |
| Rating in stars comparison with first-point gaze in group B for images with clear aligners worn | −0.48571 | 0.32872 | Not significant |
| Rating in stars comparison with longest gaze in group A for images without clear aligners worn | −0.02942 | 0.95588 | Not significant |
| Rating in stars comparison with longest gaze in group A for images with clear aligners worn | 0.5161 | 0.29458 | Not significant |
| Rating in stars comparison with longest gaze in group B for images without clear aligners worn | 0.25714 | 0.62279 | Not significant |
| Rating in stars comparison with longest gaze in group B for images with clear aligners worn | 0.2 | 0.704 | Not significant |
| Rating in stars comparison with overall observation time in group A for images without clear aligners worn | −0.47079 | 0.34599 | Not significant |
| Rating in stars comparison with overall observation time in group A for images with clear aligners worn | −0.94112 | 0.0051 | Significant |
| Rating in stars comparison with overall observation time in group B for images without clear aligners worn | −0.77143 | 0.0724 | Not sig-nificant |
| Rating in stars comparison with overall observation time in group B for images with clear aligners worn | −0.88571 | 0.01885 | Significant |
| W Walue | Mean Difference | z Value | Sample Size N | Meaning | |
|---|---|---|---|---|---|
| Overall observation time related to presence of lips/cheek retractors in both groups for images without clear aligners worn | 10 | 4.62 | −0.1048 | 5 | Not significant |
| Overall observation time related to presence of lips/cheek retractors in both groups for images with clear aligners worn | 1 | −0.15 | −1.299917 | 6 | Significant |
| Rating in stars related to the presence of lips/cheek retractors in both groups for images without clear aligners worn | 6 | −0.42 | 0.9435 | 6 | Not significant |
| Rating in stars related to the presence of lips/cheek retractors in both groups for images with clear aligners worn | 0 | −0.1 | −2.0226 | 5 | Significant |
| Overall observation time related to presence/absence of clear aligners in both groups | 7 | −4.7 | −2.5103 | 12 | Significant |
| Overall observation time related to presence/absence of clear aligners and cheek retractors in both groups | 1 | −5.93 | −1.9917 | 6 | Significant |
| Overall observation time related to presence/absence of clear aligners and lips in both groups | 4 | −3.67 | −1.3628 | 6 | Not significant |
| Rating in stars related to the presence/absence of clear aligners in both groups | 27.5 | 0.3 | 0 | 10 | Not significant |
| Rating in stars related to the presence/absence of clear aligners and cheek retractors in both groups | 5.5 | 1.9 | −0.5394 | 5 | Not significant |
| Rating in stars related to the presence/absence of clear aligners and lips in both groups | 5 | 1.1 | −0.6742 | 5 | Not significant |
| First-Point Gaze (Area of Interest) | |||||||
|---|---|---|---|---|---|---|---|
| GROUP A | Anterior Attachments | Posterior Attachments | Gingival Margin | Upper Lip | Lower Lip | Anterior Teeth | Posterior Teeth |
| Smile 1—no clear aligners | 51% | 30% | 14% | NV | NV | 5% | NV |
| Smile 1—with clear aligners | 63% | 33% | 2% | NV | NV | 2% | NV |
| Smile 2—no clear aligners | NV | 16% | 3% | 30% | 41% | 10% | NV |
| Smile 2—with clear aligners | NV | 19% | 1% | 26% | 52% | 3% | NV |
| Smile 3—no clear aligners | NV | NV | 37% | NV | NV | 45% | 18% |
| Smile 3—with clear aligners | NV | NV | 34% | NV | NV | 37% | 29% |
| Smile 4—no clear aligners | 37% | 14% | 5% | 16% | 20% | 8% | NV |
| Smile 4—with clear aligners | 31% | 22% | 2% | 22% | 18% | 5% | NV |
| Smile 5—no clear aligners | NV | 50% | 11% | NV | NV | 39% | NV |
| Smile 5—with clear aligners | NV | 46% | 13% | NV | NV | 41% | NV |
| Smile 6—no clear aligners | NV | NV | 18% | 30% | 28% | 18% | 8% |
| Smile 6—with clear aligners | NV | NV | 11% | 32% | 24% | 20% | 13% |
| GROUP B | Anterior attachments | Posterior attachments | Gingival margin | Upper Lip | Lower Lip | Anterior teeth | Posterior teeth |
| Smile 1—no clear aligners | 57% | 30% | 8% | NV | NV | 5% | NV |
| Smile 1—with clear aligners | 55% | 39% | 4% | NV | NV | 2% | NV |
| Smile 2—no clear aligners | NV | 23% | 3% | 28% | 30% | 16% | NV |
| Smile 2—with clear aligners | NV | 27% | 3% | 29% | 23% | 12% | NV |
| Smile 3—no clear aligners | NV | NV | 48% | NV | NV | 42% | 10% |
| Smile 3—with clear aligners | NV | NV | 41% | NV | NV | 38% | 21% |
| Smile 4—no clear aligners | 29% | 28% | 5% | 23% | 11% | 4% | NV |
| Smile 4—with clear aligners | 33% | 26% | 3% | 23% | 9% | 6% | NV |
| Smile 5—no clear aligners | NV | 35% | 24% | NV | NV | 41% | NV |
| Smile 5—with clear aligners | NV | 39% | 21% | NV | NV | 40% | NV |
| Smile 6—no clear aligners | NV | NV | 11% | 26% | 31% | 24% | 8% |
| Smile 6—with clear aligners | NV | NV | 9% | 27% | 29% | 27% | 8% |
| Longest gaze (area of interest) | |||||||
| GROUP A | Anterior attachments | Posterior attachments | Gingival margin | Upper Lip | Lower Lip | Anterior teeth | Posterior teeth |
| Smile 1—no clear aligners | 56% | 40% | 2% | NV | NV | 2% | NV |
| Smile 1—with clear aligners | 52% | 41% | 3% | NV | NV | 4% | NV |
| Smile 2—no clear aligners | NV | 31% | 5% | 30% | 24% | 10% | NV |
| Smile 2—with clear aligners | NV | 26% | 8% | 36% | 22% | 8% | NV |
| Smile 3—no clear aligners | NV | NV | 28% | NV | NV | 40% | 32% |
| Smile 3—with clear aligners | NV | NV | 21% | NV | NV | 33% | 46% |
| Smile 4—no clear aligners | 30% | 28% | 5% | 18% | 11% | 8% | NV |
| Smile 4—with clear aligners | 26% | 24% | 1% | 20% | 22% | 7% | NV |
| Smile 5—no clear aligners | NV | 60% | 27% | NV | NV | 13% | NV |
| Smile 5—with clear aligners | NV | 64% | 24% | NV | NV | 12% | NV |
| Smile 6—no clear aligners | NV | NV | 20% | 42% | 28% | 7 | 3% |
| Smile 6—with clear aligners | NV | NV | 26% | 38% | 26% | 9% | 1% |
| GROUP B | Anterior attachments | Posterior attachments | Gingival margin | Upper Lip | Lower Lip | Anterior teeth | Posterior teeth |
| Smile 1—no clear aligners | 54% | 38% | 5% | NV | NV | 3% | NV |
| Smile 1—with clear aligners | 58% | 37% | 3% | NV | NV | 2% | NV |
| Smile 2—no clear aligners | NV | 32% | 4% | 36% | 18% | 10% | NV |
| Smile 2—with clear aligners | NV | 29% | 6% | 33% | 19% | 13% | NV |
| Smile 3—no clear aligners | NV | NV | 42% | NV | NV | 38% | 20% |
| Smile 3—with clear aligners | NV | NV | 40% | NV | NV | 34% | 26% |
| Smile 4—no clear aligners | 31% | 35% | 4% | 12% | 8% | 10% | NV |
| Smile 4—with clear aligners | 34% | 37% | 1% | 15% | 7% | 6% | NV |
| Smile 5—no clear aligners | NV | 41% | 14% | NV | NV | 45% | NV |
| Smile 5—with clear aligners | NV | 42% | 18% | NV | NV | 40% | NV |
| Smile 6—no clear aligners | NV | NV | 13% | 29% | 22% | 29% | 7% |
| Smile 6—with clear aligners | NV | NV | 12% | 27% | 20% | 31% | 10% |
| Chi-Square Test | p-Value | |
|---|---|---|
| Smile 1 first-point gaze (area of interest)—comparison between A and B groups | 1.9697 | 0.57872 |
| Smile 2 first-point gaze (area of interest)—comparison between A and B groups | 4.4142 | 0.352841 |
| Smile 3 first-point gaze (area of interest)—comparison between A and B groups | 3.8127 | 0.148622 |
| Smile 4 first-point gaze (area of interest)—comparison between A and B groups | 10.839 | 0.05466725 |
| Smile 5 first-point gaze (area of interest)—comparison between A and B groups | 7.5256 | 0.023218 |
| Smile 6 first-point gaze (area of interest)—comparison between A and B groups | 3.7279 | 0.444079 |
| Smile 1 longest gaze (area of interest)—comparison between A and B groups | 1.5734 | 0.665445 |
| Smile 2 longest gaze (area of interest)—comparison between A and B groups | 1.5296 | 0.821389 |
| Smile 3 longest gaze (area of interest)—comparison between A and B groups | 5.6205 | 0.06019 |
| Smile 4 longest gaze (area of interest)—comparison between A and B groups | 2.801 | 0.73063284 |
| Smile 5 longest gaze (area of interest)—comparison between A and B groups | 25.3514 | <0.00001 |
| Smile 6 longest gaze (area of interest)—comparison between A and B groups | 19.6296 | 0.000591 |
| Chi-Square Test | p-Value | |
|---|---|---|
| Smile 1 first-point gaze (area of interest)—comparison between A and B groups | 2.0374 | 0.564681 |
| Smile 2 first-point gaze (area of interest)—comparison between A and B groups | 19.8667 | 0.000531 |
| Smile 3 first-point gaze (area of interest)—comparison between A and B groups | 1.9474 | 0.37768 |
| Smile 4 first-point gaze (area of interest)—comparison between A and B groups | 4.085 | 0.53724414 |
| Smile 5 first-point gaze (area of interest)—comparison between A and B groups | 9.7966 | 0.007459 |
| Smile 6 first-point gaze (area of interest)—comparison between A and B groups | 2.6045 | 0.626034 |
| Smile 1 longest gaze (area of interest)—comparison between A and B groups | 1.0921 | 0.778988 |
| Smile 2 longest gaze (area of interest)—comparison between A and B groups | 1.9898 | 0.73764 |
| Smile 3 longest gaze (area of interest)—comparison between A and B groups | 11.4885 | 0.003201 |
| Smile 4 longest gaze (area of interest)—comparison between A and B groups | 13.093 | 0.02252267 |
| Smile 5 longest gaze (area of interest)—comparison between A and B groups | 20.5001 | 0.000035 |
| Smile 6 longest gaze (area of interest)—comparison between A and B groups | 27.2657 | 0.000018 |
| Chi-Square Test | p-Value | |
|---|---|---|
| Smile 1 first-point gaze (area of interest)—comparison between image without and with clear aligners | 17.5352 | 0.040965 |
| Smile 2 first-point gaze (area of interest)—comparison between image without and with clear aligners | 26.348 | 0.00958 |
| Smile 3 first-point gaze (area of interest)—comparison between image without and with clear aligners | 13.2495 | 0.03924 |
| Smile 4 first-point gaze (area of interest)—comparison between image without and with clear aligners | 16.991 | 0.31940271 |
| Smile 5 first-point gaze (area of interest)—comparison between image without and with clear aligners | 10.06 | 0.122149 |
| Smile 6 first-point gaze (area of interest)—comparison between image without and with clear aligners | 10.7241 | 0.552695 |
| Smile 1 longest gaze (area of interest)—comparison between image without and with clear aligners | 3.0816 | 0.960972 |
| Smile 2 longest gaze (area of interest)—comparison between image without and with clear aligners | 5.3072 | 0.946922 |
| Smile 3 longest gaze (area of interest)—comparison between image without and with clear aligners | 22.0256 | 0.001198 |
| Smile 4 longest gaze (area of interest)—comparison between image without and with clear aligners | 26.08 | 0.03719016 |
| Smile 5 longest gaze (area of interest)—comparison between image without and with clear aligners | 46.4368 | <0.00001 |
| Smile 6 longest gaze (area of interest)—comparison between image without and with clear aligners | 48.4195 | <0.00001 |
| Source | Sum of Squares SS | Degrees of Freedom νν | Mean Square MS | F-Statistic | p-Value |
|---|---|---|---|---|---|
| Between | 3968.5429 | 5 | 793.7086 | 4.1751 | 0.0018 |
| Within | 18,630.2167 | 98 | 190.1043 | ||
| Total | 22,598.7596 | 103 |
| Source | Sum of Squares SS | Degrees of Freedom νν | Mean Square MS | F-Statistic | p-Value |
|---|---|---|---|---|---|
| Between | 3948.7179 | 5 | 789.7436 | 3.7366 | 0.0039 |
| Within | 20,712.667 | 98 | 211.3537 | ||
| Total | 24,661.3846 | 103 |
| Comparison Pair | Tukey HSD Q Statistic | Tukey HSD p-Value | Scheffè T-Statistic | Scheffè p-Value | Bonferroni and Holm T-Statistic | Bonferroni p-Value | Holm p-Value |
|---|---|---|---|---|---|---|---|
| Smile 1 vs. Smile 2 | 1.6055 | 0.8517601 | 1.1352 | 0.9349495 | 1.1352 | 3.8856641 | 1.5542657 |
| Smile 1 vs. Smile 3 | 2.2383 | 0.5970256 | 1.5827 | 0.7748420 | 1.5827 | 1.7507304 | 0.9337229 |
| Smile 1 vs. Smile 4 | 2.6483 | 0.4269844 | 1.8727 | 0.6237152 | 1.8727 | 0.9614499 | 0.5768699 |
| Smile 1 vs. Smile 5 | 2.2383 | 0.5970256 | 1.5827 | 0.7748420 | 1.5827 | 1.7507304 | 0.8170075 |
| Smile 1 vs. Smile 6 | 1.4984 | 0.8948455 | 1.0596 | 0.9511189 | 1.0596 | 4.3792674 | 1.4597558 |
| Smile 2 vs. Smile 3 | 3.8155 | 0.0850264 | 2.6980 | 0.2113136 | 2.6980 | 0.1232246 | 0.1067946 |
| Smile 2 vs. Smile 4 | 1.0446 | 0.8999947 | 0.7386 | 0.9900823 | 0.7386 | 6.9285801 | 1.3857160 |
| Smile 2 vs. Smile 5 | 3.8155 | 0.0850264 | 2.6980 | 0.2113136 | 2.6980 | 0.1232246 | 0.0985797 |
| Smile 2 vs. Smile 6 | 0.1135 | 0.8999947 | 0.0803 | 0.9999998 | 0.0803 | 14.0427517 | 1.8723669 |
| Smile 3 vs. Smile 4 | 4.8352 | 0.0114955 * | 3.4190 | 0.0473774 * | 3.4190 | 0.0137588 * | 0.0137588 * |
| Smile 3 vs. Smile 5 | 0.0000 | 0.8999947 | 0.0000 | 1.0000000 | 0.0000 | 15.0000000 | 1.0000000 |
| Smile 3 vs. Smile 6 | 3.7172 | 0.1000928 | 2.6285 | 0.2377420 | 2.6285 | 0.1493660 | 0.1095351 |
| Smile 4 vs. Smile 5 | 4.8352 | 0.0114955 * | 3.4190 | 0.0473774 * | 3.4190 | 0.0137588 * | 0.0128415 * |
| Smile 4 vs. Smile 6 | 1.1631 | 0.8999947 | 0.8225 | 0.9838156 | 0.8225 | 6.1921848 | 1.6512493 |
| Smile 5 vs. Smile 6 | 3.7172 | 0.1000928 | 2.6285 | 0.2377420 | 2.6285 | 0.1493660 | 0.0995774 |
| Comparison Pair | Tukey HSD Q Statistic | Tukey HSD p-Value | Scheffè T-Statistic | Scheffè p-Value | Bonferroni and Holm T-Statistic | Bonferroni p-Value | Holm p-Value |
|---|---|---|---|---|---|---|---|
| Smile 1 vs. Smile 2 | 1.4501 | 0.8999947 | 1.0254 | 0.9574354 | 1.0254 | 4.6155589 | 1.8462236 |
| Smile 1 vs. Smile 3 | 2.1228 | 0.6435194 | 1.5010 | 0.8119233 | 1.5010 | 2.0484975 | 1.0925320 |
| Smile 1 vs. Smile 4 | 2.5117 | 0.4862373 | 1.7760 | 0.6766135 | 1.7760 | 1.1824840 | 0.7094904 |
| Smile 1 vs. Smile 5 | 2.1228 | 0.6435194 | 1.5010 | 0.8119233 | 1.5010 | 2.0484975 | 0.9559655 |
| Smile 1 vs. Smile 6 | 1.4501 | 0.8999947 | 1.0254 | 0.9574354 | 1.0254 | 4.6155589 | 1.5385196 |
| Smile 2 vs. Smile 3 | 3.5521 | 0.1304538 | 2.5117 | 0.2866552 | 2.5117 | 0.2047503 | 0.1774502 |
| Smile 2 vs. Smile 4 | 1.0710 | 0.8999947 | 0.7573 | 0.9888774 | 0.7573 | 6.7603059 | 1.8027482 |
| Smile 2 vs. Smile 5 | 3.5521 | 0.1304538 | 2.5117 | 0.2866552 | 2.5117 | 0.2047503 | 0.1638002 |
| Smile 2 vs. Smile 6 | 0.0000 | 0.8999947 | 0.0000 | 1.0000000 | 0.0000 | 15.0000000 | 2.0000000 |
| Smile 3 vs. Smile 4 | 4.5857 | 0.0195893 * | 3.2426 | 0.0714119 | 3.2426 | 0.0242962 * | 0.0242962 * |
| Smile 3 vs. Smile 5 | 0.0000 | 0.8999947 | 0.0000 | 1.0000000 | 0.0000 | 15.0000000 | 1.0000000 |
| Smile 3 vs. Smile 6 | 3.5521 | 0.1304538 | 2.5117 | 0.2866552 | 2.5117 | 0.2047503 | 0.1501502 |
| Smile 4 vs. Smile 5 | 4.5857 | 0.0195893 * | 3.2426 | 0.0714119 | 3.2426 | 0.0242962 * | 0.0226765 * |
| Smile 4 vs. Smile 6 | 1.0710 | 0.8999947 | 0.7573 | 0.9888774 | 0.7573 | 6.7603059 | 1.3520612 |
| Smile 5 vs. Smile 6 | 3.5521 | 0.1304538 | 2.5117 | 0.2866552 | 2.5117 | 0.2047503 | 0.1365002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Putrino, A.; Marinelli, E.; Raso, M.; Calace, V.; Zaami, S. Clear Aligners and Smart Eye Tracking Technology as a New Communication Strategy between Ethical and Legal Issues. Life 2023, 13, 297. https://doi.org/10.3390/life13020297
Putrino A, Marinelli E, Raso M, Calace V, Zaami S. Clear Aligners and Smart Eye Tracking Technology as a New Communication Strategy between Ethical and Legal Issues. Life. 2023; 13(2):297. https://doi.org/10.3390/life13020297
Chicago/Turabian StylePutrino, Alessandra, Enrico Marinelli, Mario Raso, Valeria Calace, and Simona Zaami. 2023. "Clear Aligners and Smart Eye Tracking Technology as a New Communication Strategy between Ethical and Legal Issues" Life 13, no. 2: 297. https://doi.org/10.3390/life13020297
APA StylePutrino, A., Marinelli, E., Raso, M., Calace, V., & Zaami, S. (2023). Clear Aligners and Smart Eye Tracking Technology as a New Communication Strategy between Ethical and Legal Issues. Life, 13(2), 297. https://doi.org/10.3390/life13020297