




Therapeutic Efficacy and Radiobiological Effects of Boric-Acid-Mediated BNCT in an Osteosarcoma-Bearing SD Rat Model

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation of Boric Acid (BA) Solution and Determination of Boron Concentration
2.2. UMR-106 Cell Culture
2.3. Animal Model
2.4. Pharmacokinetics and Biodistribution of BA in OS-Bearing SD Rats
2.4.1. Pharmacokinetic Analysis
2.4.2. Biodistribution Analysis
2.5. Neutron Irradiation In Vivo
2.6. Histological Analysis
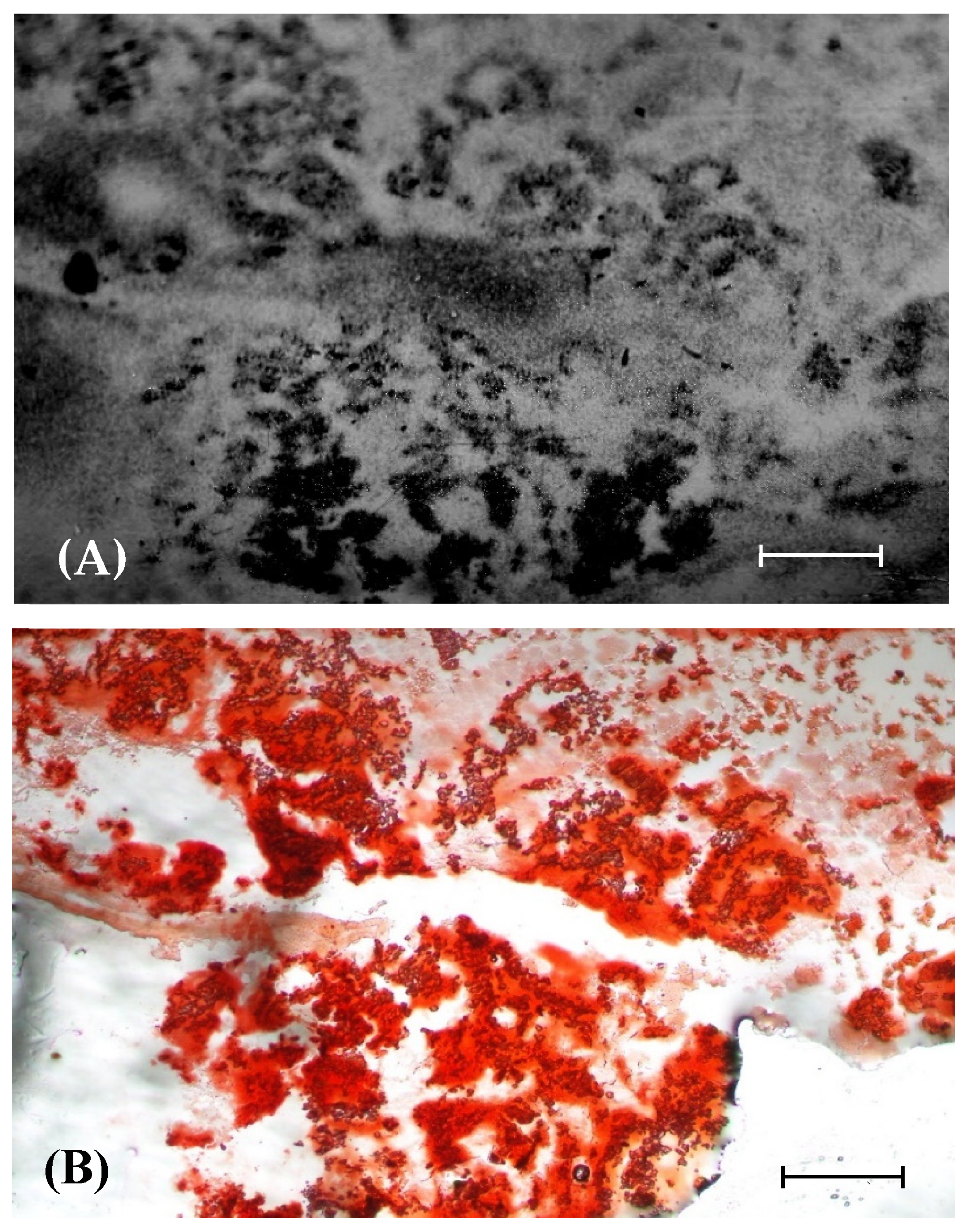
2.7. Autoradiography
2.8. Radiographic Examination
2.9. Statistical Analysis
3. Results
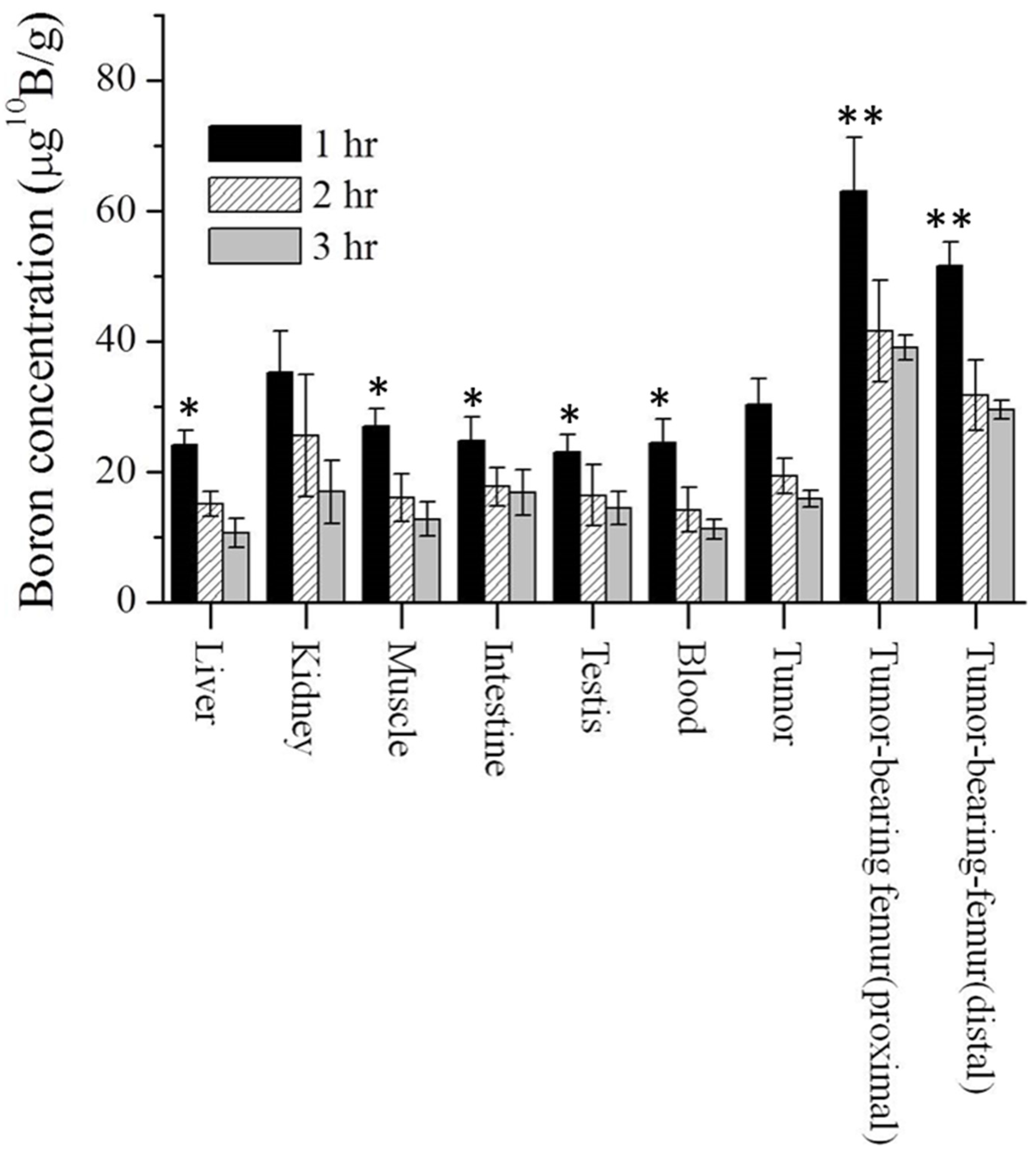
3.1. Biodistribution of Boron in Osteosarcoma-Bearing Rat
3.2. Physical Dose for BNCT
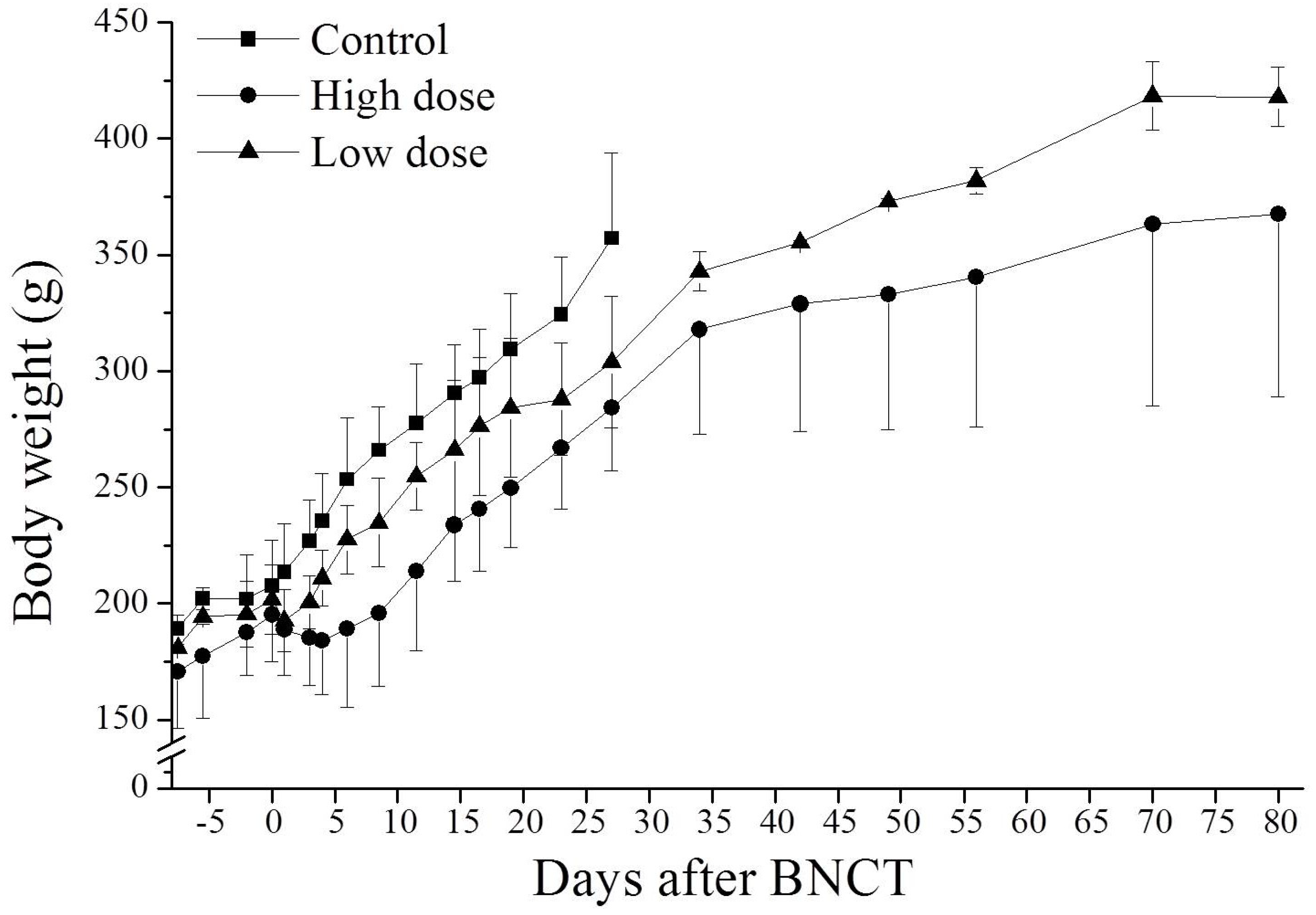
3.3. Effect of BNCT on Body Weight
3.4. Therapeutic Efficacy
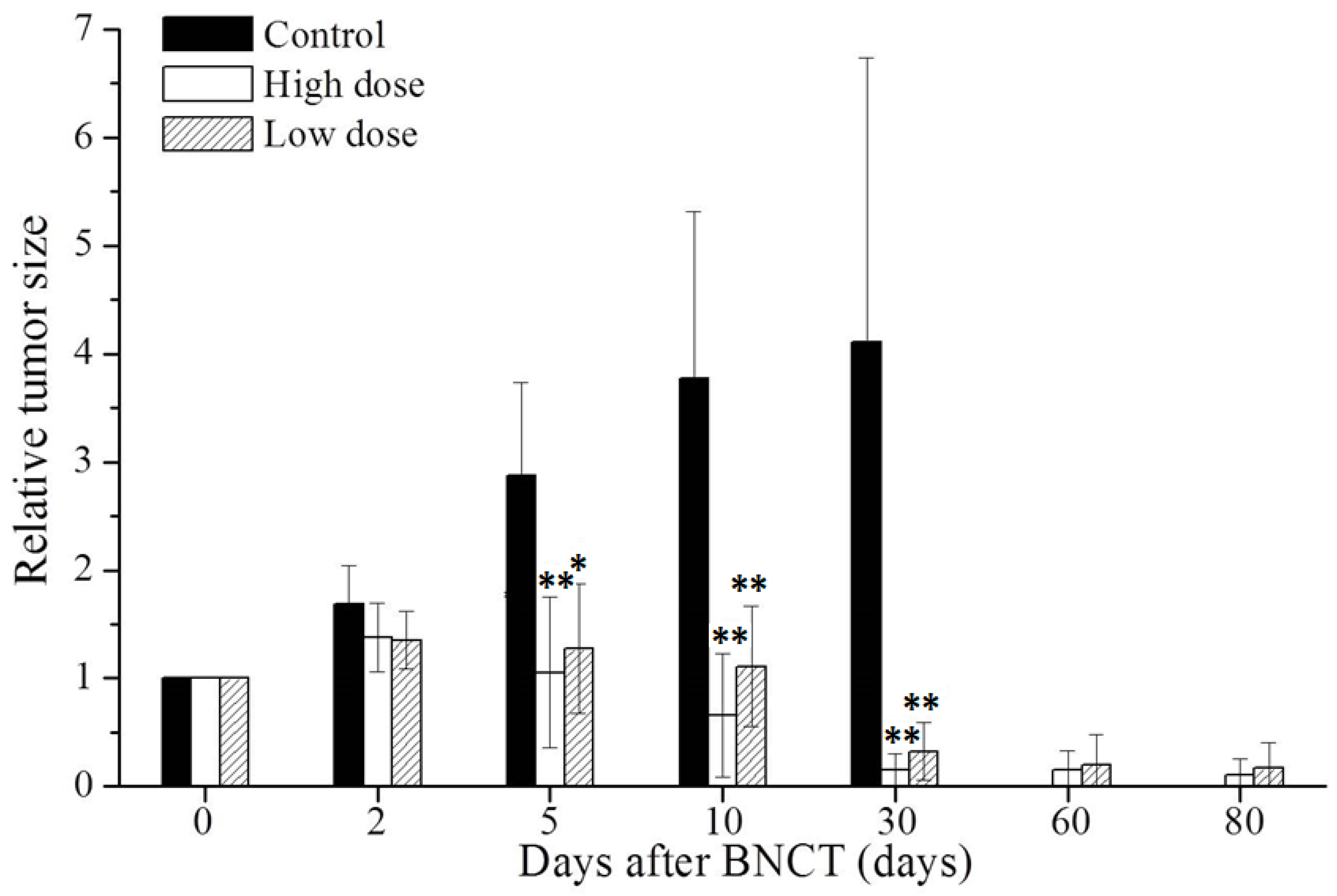
3.4.1. BNCT Reduces Size of Tumor
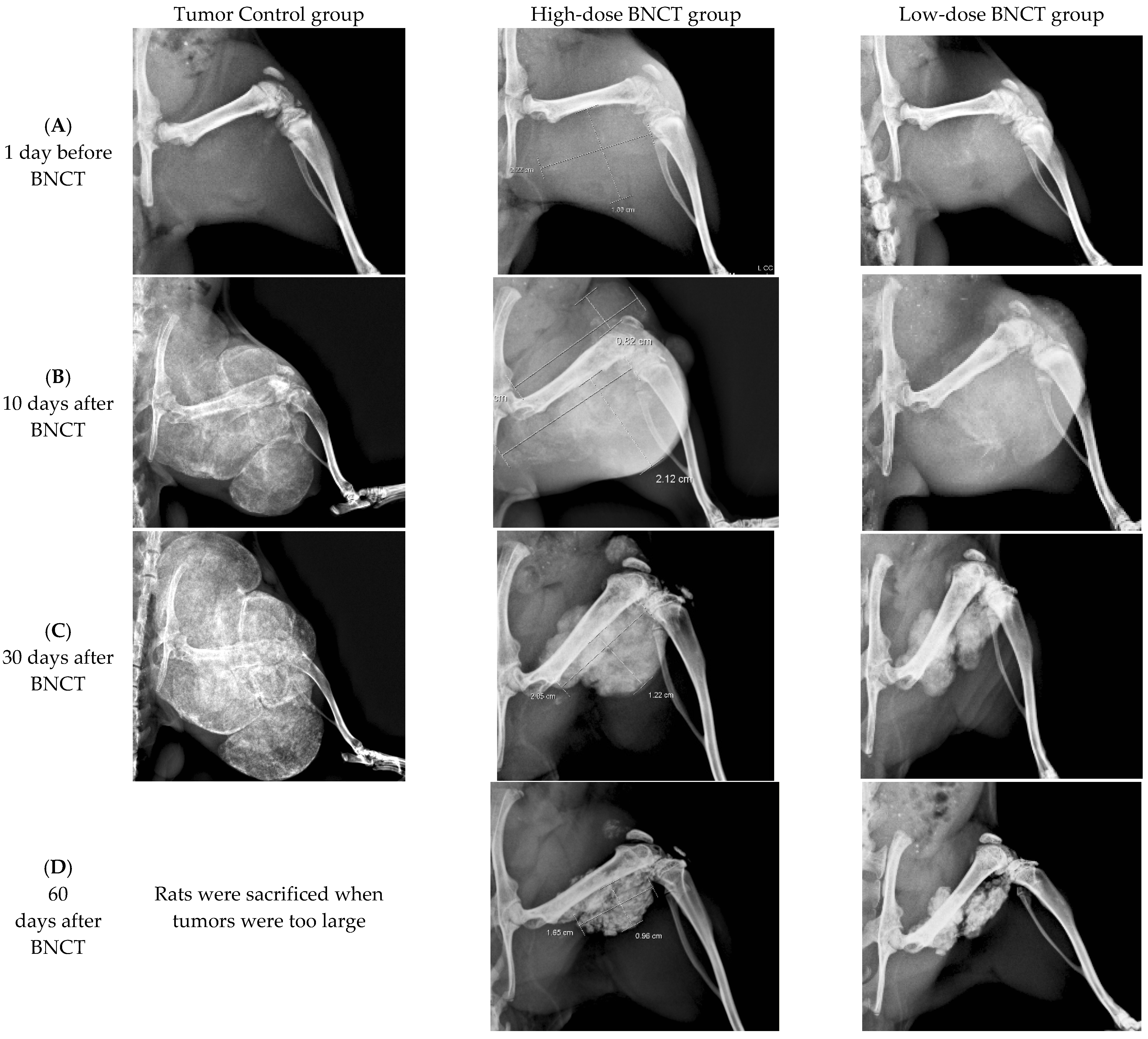
3.4.2. Radiographic Investigation
3.5. Relationship between BA Retention and Calcification in OS Tissue
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Klein, M.J.; Siegal, G.P. Osteosarcoma: Anatomic and histologic variants. Am. J. Clin. Pathol. 2006, 125, 481–555. [Google Scholar] [CrossRef] [PubMed]
- Smeland, S.; Bielack, S.S.; Whelan, J.; Bernstein, M.; Hogendoorn, P.; Krailo, M.D.; Gorlick, R.; Janeway, K.A.; Ingleby, F.C.; Anninga, J.; et al. Survival and Prognosis with Osteosarcoma: Outcomes in More than 2000 Patients in the EURAMOS-1 (European and American Osteosarcoma Study) Cohort. Eur. J. Cancer 2019, 109, 36–50. [Google Scholar] [CrossRef] [PubMed]
- Nagarajan, R. Quality of life (QOL) in patients with osteosarcoma. In Treatment of Bone and Soft Tissue Sarcomas; Tunn, P.-U., Ed.; Recent Results in Cancer Research; Springer: Berlin/Heidelberg, Germany, 2009; Volume 179, pp. 339–344. ISBN 9783642096785. [Google Scholar]
- Picci, P. Osteosarcoma (osteogenic sarcoma). Orphanet J. Rare Dis. 2007, 2, 6. [Google Scholar] [CrossRef] [PubMed]
- Shimanovskaya, K.; Shiman, A.D. Radiation Injury of Bone: Bone Injuries Following Radiation Therapy of Tumors; Pergamon Press: New York, NY, USA, 1983. [Google Scholar]
- Heng, M.; Gupta, A.; Chung, P.W.; Healey, J.; Vaynrub, M.; Rose, P.S.; Houdek, M.T.; Lin, P.P.; Bishop, A.J.; Hornicek, F.J.; et al. The Role of Chemotherapy and Radiotherapy in Localized Extraskeletal Osteosarcoma. Eur. J. Cancer 2020, 125, 130–141. [Google Scholar] [CrossRef] [PubMed]
- Barth, R.F.; Coderre, J.A.; Vicente, M.G.H.; Blue, T.E. Boron neutron capture therapy of cancer: Current status and future prospects. Clin. Cancer Res. 2005, 11, 3987–4002. [Google Scholar] [CrossRef] [PubMed]
- Coderre, J.A.; Morris, G.M. The radiation biology of boron neutron capture therapy. Radiat. Res. 1999, 151, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Hall, E.J.; Giaccia, A.J. Radiobiology for the Radiologist, 7th ed.; Wolters Kluwer Health/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012. [Google Scholar]
- Nickoloff, J.A.; Sharma, N.; Taylor, L. Clustered DNA Double-Strand Breaks: Biological Effects and Relevance to Cancer Radiotherapy. Genes 2020, 11, 99. [Google Scholar] [CrossRef] [PubMed]
- Iliakis, G.; Mladenov, E.; Mladenova, V. Necessities in the Processing of DNA Double Strand Breaks and Their Effects on Genomic Instability and Cancer. Cancers 2019, 11, 1671. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.Y.; Lai, Z.Y.; Hsu, T.J. Boron Neutron Capture Therapy Eliminates Radioresistant Liver Cancer Cells by Targeting DNA Damage and Repair Responses. J. Hepatocell. Carcinoma 2022, 9, 1385–1401. [Google Scholar] [CrossRef]
- Coderre, J.A.; Makar, M.S.; Micca, P.L.; Nawrocky, M.M.; Liu, H.B.; Joel, D.D.; Slatkin, D.N.; Amols, H.I. Derivations of relative biological effectiveness for the high-let radiations produced during boron neutron capture irradiations of the 9L rat gliosarcoma in vitro and in vivo. Int. J. Radiat. Oncol. Biol. Phys. 1993, 27, 1121–1129. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.H.; Tsai, P.E.; Liu, H.M.; Jiang, S.-H. Characterization of a BNCT beam using neutron activation and indirect neutron radiography. Radiat. Meas. 2010, 45, 1167–1170. [Google Scholar]
- Gueulette, J.; Liu, H.M.; Jiang, S.H.; Liu, H.Y.W.; De Coster, B.M.; Liu, Y.H.; Tsai, W.C.; Wambersie, A.; Chen, A.Y. Radiobiological Characterization of the Epithermal Neutron Beam Produced at the Tsing Hua Open-Pool Reactor (THOR) for BNCT: Comparison with Other BNCT Facilities. Ther. Radiol. Oncol. 2006, 13, 135–146. [Google Scholar]
- Chen, Y.W.; Lee, Y.Y.; Lin, C.F.; Pan, P.-S.; Chen, J.-K.; Wang, C.-W.; Hsu, S.-M.; Kuo, Y.-C.; Lan, T.-L.; Hsu, S.; et al. Salvage Boron Neutron Capture Therapy for Malignant Brain Tumor Patients in Compliance with Emergency and Compassionate Use: Evaluation of 34 Cases in Taiwan. Biology 2021, 10, 334. [Google Scholar] [CrossRef] [PubMed]
- Ternane, R.; Cohen-Adad, M.T.; Panczer, G.; Goutaudier, C.; Kbir-Ariguib, N.; Trabelsi-Ayedi, M.; Florian, P.; Massiot, D. Introduction of boron in hydroxyapatite: Synthesis and structural characterization. J. Alloy Compd. 2002, 333, 62–71. [Google Scholar] [CrossRef]
- Jodati, H.; Tezcaner, A.; Alshemary, A.Z.; Şahin, V.; Evis, Z. Effects of the doping concentration of boron on physicochemical, mechanical, and biological properties of hydroxyapatite. Ceram. Int. 2022, 48, 22743–22758. [Google Scholar] [CrossRef]
- Kim, D.H.; Faull, K.F.; Norris, A.J.; Eckhert, C.D. Borate-nucleotide complex formation depends on charge and phosphorylation state. J. Mass Spectrom. 2004, 39, 743–751. [Google Scholar] [CrossRef] [PubMed]
- Murray, F.J. A comparative review of the pharmacoketics of boric acid in rodents and humans. Biol. Trace Elem. Res. 1998, 66, 331–341. [Google Scholar] [CrossRef]
- Devirian, T.A.; Volpe, S.L. The physiological effects of dietary boron. Crit. Rev. Food Sci. Nutr. 2003, 43, 219–231. [Google Scholar] [CrossRef] [PubMed]
- Hunt, C.D. Regulation of enzymatic activity one possible role of dietary boron in higher animals and humans. Biol. Trace Elem. Res. 1998, 66, 205–225. [Google Scholar] [CrossRef]
- Hsu, C.F.; Lin, S.Y.; Peir, J.J.; Liao, J.; Lin, Y.; Chou, F. Potential of using boric acid as a boron drug for boron neutron capture therapy for osteosarcoma. Appl. Radiat. Isot. 2011, 69, 1782–1785. [Google Scholar] [CrossRef]
- Hung, Y.S.; Lin, Y.C.; Lin, Y.T.; Shih, G.-W.; Liao, J.-W.; Chen, K.-S.; Liu, H.-M.; Chen, Y.-W.; Chuang, Y.-J.; Yang, C.-M.; et al. Therapeutic Efficacy and Radiobiological Effects of Boric Acid-mediated BNCT in a VX2 Multifocal Liver Tumor-bearing Rabbit Model. Anticancer Res. 2019, 39, 5495–5504. [Google Scholar] [CrossRef] [PubMed]
- Chou, F.I.; Lui, W.Y.; Wei, Y.Y.; Chung, R.J.; Kai, J.-J.; Chi, C.W. Preparation and in vitro evaluation of B-lipiodol as a boron delivery agent for neutron capture therapy of hepatoma. Anticancer Res. 1999, 19, 1759–1764. [Google Scholar] [PubMed]
- Cherrier, B.; Gouin, F.; Heymann, M.F.; Thiéry, J.; Rédini, F.; Heymann, D.; Duteille, F. A new experimental rat model of osteosarcoma established by intrafemoral tumor cell inoculation, useful for biology and therapy investigations. Tumour Biol. 2005, 26, 121–130. [Google Scholar] [CrossRef]
- Berlin, O.; Samid, D.; Donthineni-Rao, R.; Akeson, W.; Amiel, D.; Woods, V.L. Development of a novel spontaneous metastasis model of human osteosarcoma transplanted orthotopically into bone of athymic mice. Cancer Res. 1993, 53, 4890–4895. [Google Scholar]
- Yu, Z.; Sun, H.; Fan, Q.; Long, H.; Yang, T.; Ma, B. Establishment of reproducible osteosarcoma rat model using orthotopic implantation technique. Oncol. Rep. 2009, 21, 1175–1180. [Google Scholar]
- Farese, J.P.; Coomer, A.R.; Milner, R.; Taylor, D.; Salute, M.E.; Rajon, D.A.; Bova, F.J.; Siemann, D.W. Development of an intramuscular xenograft model of canine osteosarcoma in mice for evaluation of the effects of radiation therapy. Am. J. Vet. Res. 2009, 70, 127–133. [Google Scholar]
- Mori, F.; Tanji, K.; Wakabayashi, K. Widespread calcium deposits, as detected using the alizarin red S technique, in the nervous system of rats treated with dimethyl mercury. Neuropathology 2000, 20, 210–215. [Google Scholar] [CrossRef]
- Yang, C.H.; Lin, Y.T.; Hung, Y.H. Autoradiographic and histopathological studies of boric acid-mediated BNCT in hepatic VX2 tumor-bearing rabbits: Specific boron retention and damage in tumor and tumor vessels. Appl. Radiat. Isot. 2015, 106, 178–180. [Google Scholar] [CrossRef]
- Zonta, A.; Prati, U.; Roveda, L. Clinical lessons from the first applications of BNCT on unresectable liver metastases. J. Phys. Conf. Ser. 2006, 41, 484–495. [Google Scholar] [CrossRef]
- Sefa Gök, M.D.; Fırat Ozan, M.D.; Ebru Akay, M.D.; Yamak, K.; Kayalı, C.; Altay, T. Effect of boric acid on cartilage formation of osteochondral defects in rabbit knee: An experimental study. Ulus. Travma Ve Acil Cerrahi Derg. 2021, 27, 504–509. [Google Scholar]
- Carmeliet, P.; Jain, R.K. Angiogenesis in cancer and other diseases. Nature 2000, 407, 249–257. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Organ | Low-Dose BNCT Group (Gy) (% of Total Dose) | High-Dose BNCT Group (Gy) (% of Total Dose) | ||||||
|---|---|---|---|---|---|---|---|---|
| Total Dose | Neutron Dose | Gamma Dose | Boron Dose | Total Dose | Neutron Dose | Gamma Dose | Boron Dose | |
| Rat body | 1.27 | 0.14 (11%) | 0.37 (29 %) | 0.76 (60 %) | 2.43 | 0.26 (11%) | 0.71 (29 %) | 1.46 (60%) |
| Tumor-bearing femur | 7.90 | 0.58 (7%) | 1.02 (13%) | 6.30 (80%) | 15.09 | 1.11 (7%) | 1.95 (13%) | 12.03 (80%) |
| Extraskeletal Tumor | 5.77 | 0.82 (14%) | 1.20 (21%) | 3.76 (65%) | 11.03 | 1.56 (14%) | 2.30 (21%) | 7.18 (65 %) |
| Testes | 3.30 | 0.44 (13%) | 0.89 (27%) | 1.97 (60%) | 6.30 | 0.85 (13%) | 1.70 (27%) | 3.76 (60%) |
| Intestine | 3.01 | 0.24 (8%) | 0.84 (28%) | 1.93 (64%) | 5.99 | 0.49 (8%) | 1.67 (28%) | 3.83 (64%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, C.-F.; Liu, H.-M.; Peir, J.-J.; Liao, J.-W.; Chen, K.-S.; Chen, Y.-W.; Chuang, Y.-J.; Chou, F.-I. Therapeutic Efficacy and Radiobiological Effects of Boric-Acid-Mediated BNCT in an Osteosarcoma-Bearing SD Rat Model. Life 2023, 13, 514. https://doi.org/10.3390/life13020514
Hsu C-F, Liu H-M, Peir J-J, Liao J-W, Chen K-S, Chen Y-W, Chuang Y-J, Chou F-I. Therapeutic Efficacy and Radiobiological Effects of Boric-Acid-Mediated BNCT in an Osteosarcoma-Bearing SD Rat Model. Life. 2023; 13(2):514. https://doi.org/10.3390/life13020514
Chicago/Turabian StyleHsu, Chen-Fang, Hong-Ming Liu, Jinn-Jer Peir, Jiunn-Wang Liao, Kuan-Sheng Chen, Yi-Wei Chen, Yung-Jen Chuang, and Fong-In Chou. 2023. "Therapeutic Efficacy and Radiobiological Effects of Boric-Acid-Mediated BNCT in an Osteosarcoma-Bearing SD Rat Model" Life 13, no. 2: 514. https://doi.org/10.3390/life13020514
APA StyleHsu, C. -F., Liu, H. -M., Peir, J. -J., Liao, J. -W., Chen, K. -S., Chen, Y. -W., Chuang, Y. -J., & Chou, F. -I. (2023). Therapeutic Efficacy and Radiobiological Effects of Boric-Acid-Mediated BNCT in an Osteosarcoma-Bearing SD Rat Model. Life, 13(2), 514. https://doi.org/10.3390/life13020514