
Detection of Lymphatic Vessels in the Superficial Fascia of the Abdomen

 , ,
, ,  ,
,  ,
,  and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Collection
2.2. Histological and Immunohistochemical Staining
2.3. Image Acquisition
2.4. Image Analysis of Lymphatic Vessels
2.5. Statistics
3. Results
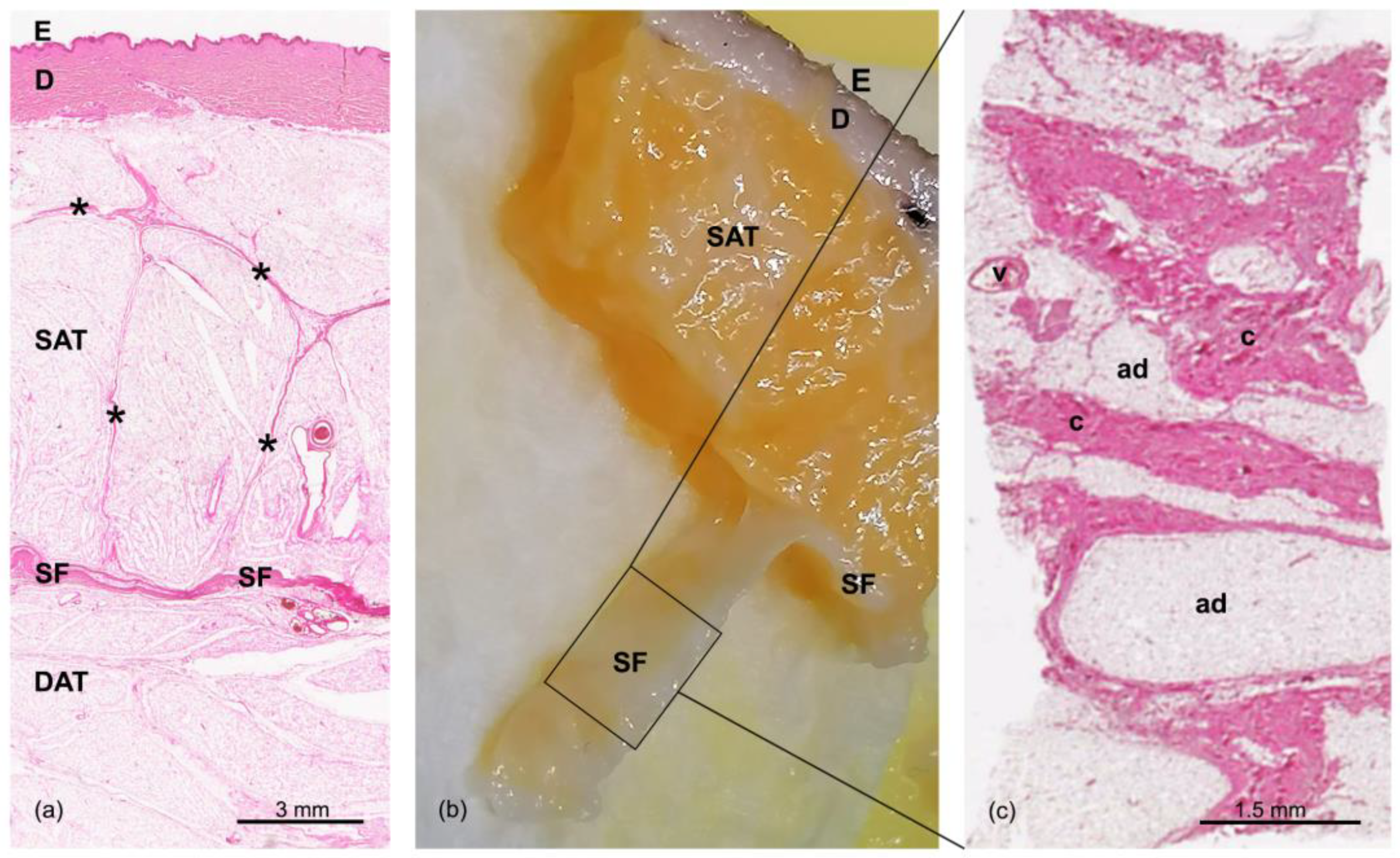
3.1. Morphological Structure of the Samples
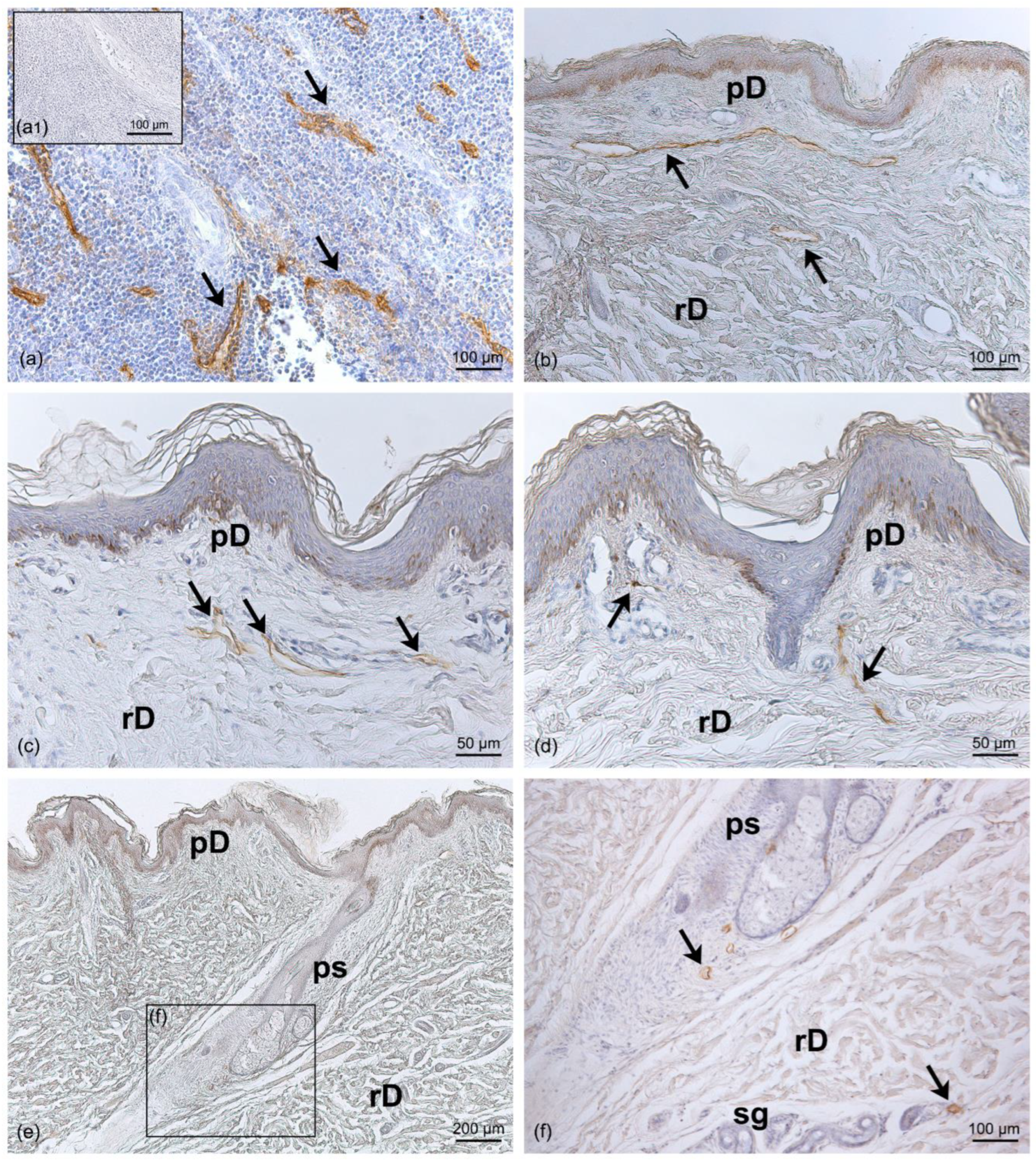
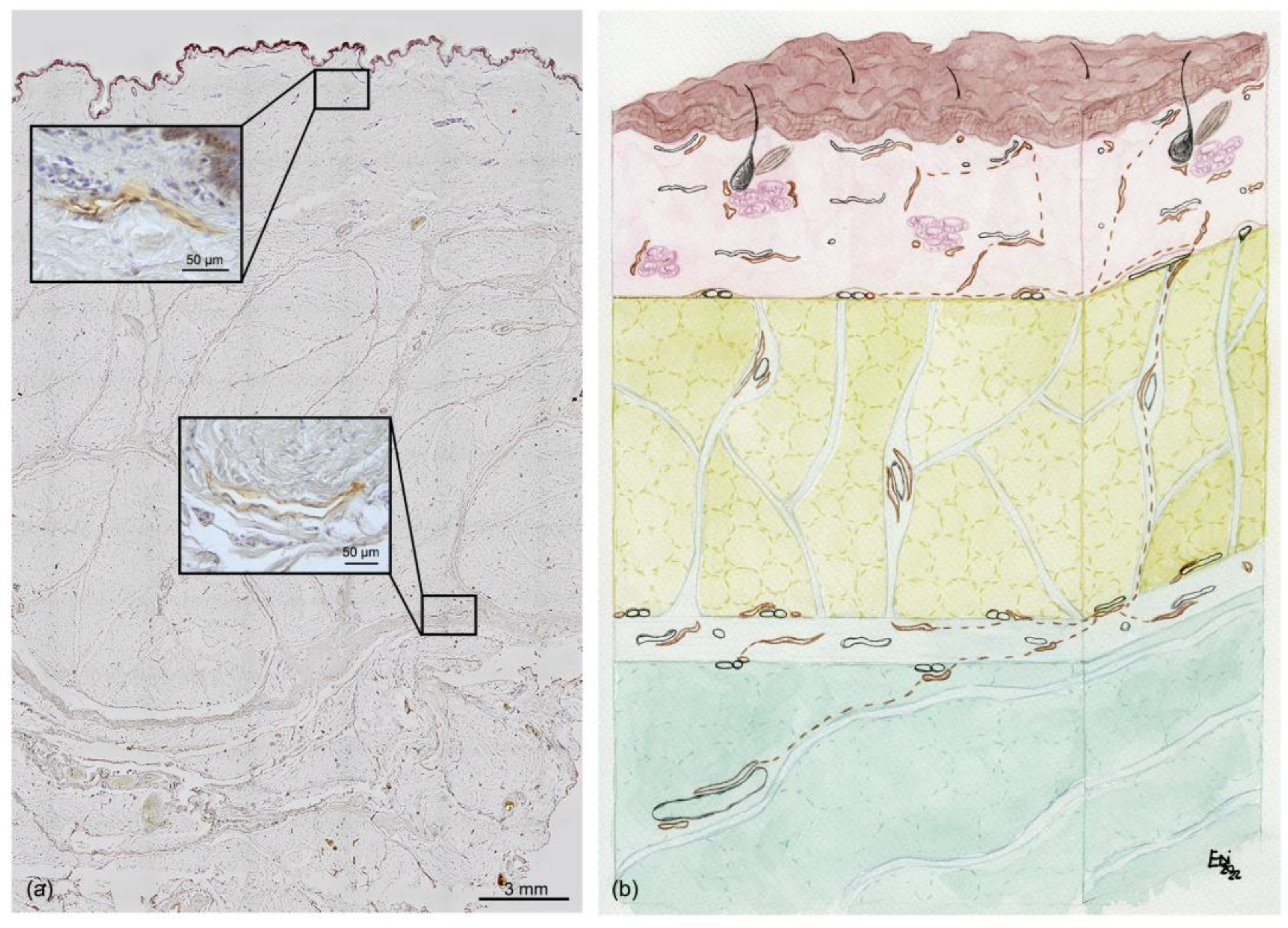
3.2. Distribution of Lymphatic Vessels
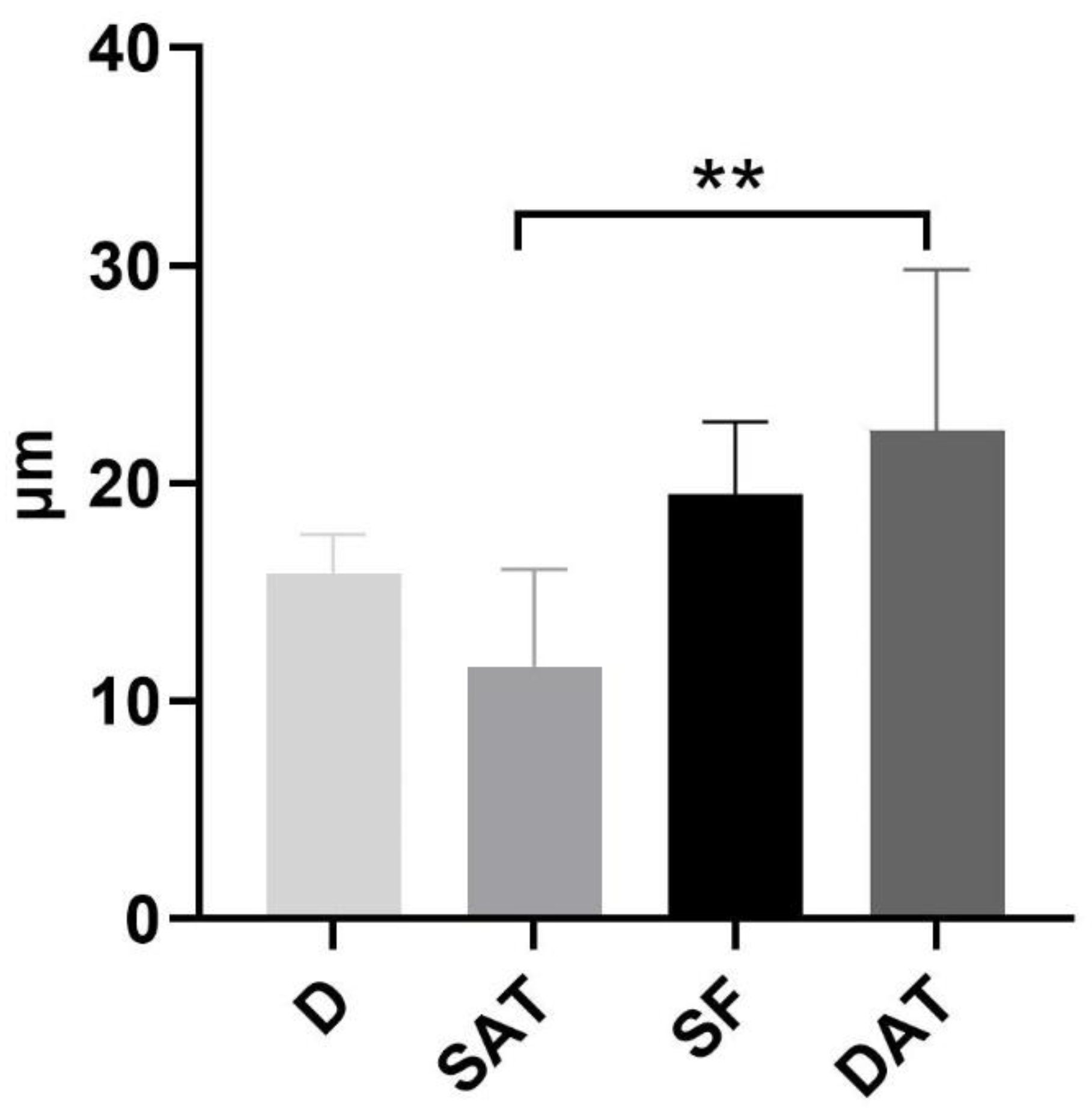
3.3. Density Analysis of Lymphatic Vessels
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Oliver, G.; Kipnis, J.; Randolph, G.J.; Harvey, N.L. The Lymphatic Vasculature in the 21st Century: Novel Functional Roles in Homeostasis and Disease. Cell 2020, 182, 270–296. [Google Scholar] [CrossRef]
- Weber, E.; Aglianò, M.; Bertelli, E.; Gabriele, G.; Gennaro, P.; Barone, V. Lymphatic Collecting Vessels in Health and Disease: A Review of Histopathological Modifications in Lymphedema. Lymphat. Res. Biol. 2022, 20, 468–477. [Google Scholar] [CrossRef]
- Mehrara, B.J.; Greene, A.K. Lymphedema and obesity: Is there a link? Plast. Reconstr. Surg. 2014, 134, 154e–160e. [Google Scholar] [CrossRef] [Green Version]
- Schaverien, M.V.; Coroneos, C.J. Surgical Treatment of Lymphedema. Plast. Reconstr. Surg. 2019, 144, 738–758. [Google Scholar] [CrossRef] [PubMed]
- Macchi, V.; Tiengo, C.; Porzionato, A.; Stecco, C.; Galli, S.; Vigato, E.; Azzena, B.; Parenti, A.; De Caro, R. Anatomo-radiological study of the superficial musculo-aponeurotic system of the face. Ital. J. Anat. Embryol. 2007, 112, 247–253. [Google Scholar] [PubMed]
- Ingallina, F.; Frank, K.; Mardini, S.; Gavril, D.L.; Hernandez, C.A.; Benslimane, F.; Gotkin, R.H.; Davidovic, K.; Moellhoff, N.; Cotofana, S. Reevaluation of the Layered Anatomy of the Forehead: Introducing the Subfrontalis Fascia and the Retrofrontalis Fat Compartments. Plast. Reconstr. Surg. 2022, 149, 587–595. [Google Scholar] [CrossRef]
- Pirri, C.; Stecco, C.; Fede, C.; Macchi, V.; Özçakar, L. Ultrasound Imaging of the Fascial Layers: You See (Only) What You Know. J. Ultrasound Med. 2020, 39, 827–828. [Google Scholar] [CrossRef]
- Lancerotto, L.; Stecco, C.; Macchi, V.; Porzionato, A.; Stecco, A.; De Caro, R. Layers of the abdominal wall: Anatomical investigation of subcutaneous tissue and superficial fascia. Surg. Radiol. Anat. 2011, 33, 835–842. [Google Scholar] [CrossRef] [PubMed]
- Pirri, C.; Fede, C.; Petrelli, L.; Guidolin, D.; Fan, C.; De Caro, R.; Stecco, C. Elastic Fibres in the subcutaneous tissue: Is there a difference between superficial and muscular fascia? A cadaver study. Skin Res. Technol. 2022, 28, 21–27. [Google Scholar] [CrossRef]
- Monzon, J.R.; Basile, R.; Heneghan, S.; Udupi, V.; Green, A. Lipolysis in adipocytes isolated from deep and superficial subcutaneous adipose tissue. Obes. Res. 2002, 10, 266–269. [Google Scholar] [CrossRef] [PubMed]
- Lundbom, J.; Hakkarainen, A.; Lundbom, N.; Taskinen, M.R. Deep subcutaneous adipose tissue is more saturated than superficial subcutaneous adipose tissue. Int. J. Obes. 2013, 37, 620–622. [Google Scholar] [CrossRef] [Green Version]
- Stecco, C. Functional Atlas of the Human Fascial System; Elsevier: London, UK, 2015. [Google Scholar]
- Cancello, R.; Zulian, A.; Gentilini, D.; Maestrini, S.; Della Barba, A.; Invitti, C.; Corà, D.; Caselle, M.; Liuzzi, A.; Di Blasio, A.M. Molecular and morphologic characterization of superficial- and deep-subcutaneous adipose tissue subdivisions in human obesity. Obesity 2013, 21, 2562–2570. [Google Scholar] [CrossRef] [PubMed]
- Kubik, S.; Manestar, M. Topographic relationship of the ventromedial lymphatic bundle and the superficial inguinal nodes to the subcutaneous veins. Clin. Anat. 1995, 8, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Tourani, S.S.; Taylor, G.I.; Ashton, M.W. Anatomy of the superficial lymphatics of the abdominal wall and the upper thigh and its implications in lymphatic microsurgery. J. Plast. Reconstr. Aesthet. Surg. 2013, 66, 1390–1395. [Google Scholar] [CrossRef]
- Culligan, K.; Sehgal, R.; Mulligan, D.; Dunne, C.; Walsh, S.; Quondamatteo, F.; Dockery, P.; Coffey, J.C. A detailed appraisal of mesocolic lymphangiology--an immunohistochemical and stereological analysis. J. Anat. 2014, 225, 463–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onder, L.; Mörbe, U.; Pikor, N.; Novkovic, M.; Cheng, H.W.; Hehlgans, T.; Pfeffer, K.; Becher, B.; Waisman, A.; Rülicke, T.; et al. Lymphatic Endothelial Cells Control Initiation of Lymph Node Organogenesis. Immunity 2017, 47, 80–92.e4. [Google Scholar] [CrossRef] [Green Version]
- Hayashida, K.; Yoshida, S.; Yoshimoto, H.; Fujioka, M.; Saijo, H.; Migita, K.; Kumaya, M.; Akita, S. Adipose-Derived Stem Cells and Vascularized Lymph Node Transfers Successfully Treat Mouse Hindlimb Secondary Lymphedema by Early Reconnection of the Lymphatic System and Lymphangiogenesis. Plast. Reconstr. Surg. 2017, 139, 639–651. [Google Scholar] [CrossRef]
- Saldanha, O.R.; Pinto, E.B.; Matos, W.N., Jr.; Lucon, R.L.; Magalhães, F.; Bello, E.M. Lipoabdominoplasty without undermining. Aesthet. Surg. J. 2001, 21, 518–526. [Google Scholar] [CrossRef]
- Saldanha, O.R.; Azevedo, S.F.; Delboni, P.S.; Saldanha Filho, O.R.; Saldanha, C.B.; Uribe, L.H. Lipoabdominoplasty: The Saldanha technique. Clin. Plast. Surg. 2010, 37, 469–481. [Google Scholar] [CrossRef]
- Costa-Ferreira, A.; Marco, R.; Vásconez, L.; Amarante, J. Abdominoplasty With Scarpa Fascia Preservation. Ann. Plast. Surg. 2016, 76 (Suppl. S4), S264–S274. [Google Scholar] [CrossRef]
- Macchi, V.; Porzionato, A.; Stecco, C.; Tiengo, C.; Parenti, A.; Cestrone, A.; De Caro, R. Body parts removed during surgery: A useful training source. Anat. Sci. Educ. 2011, 4, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Fede, C.; Petrelli, L.; Pirri, C.; Neuhuber, W.; Tiengo, C.; Biz, C.; De Caro, R.; Schleip, R.; Stecco, C. Innervation of human superficial fascia. Front. Neuroanat. 2022, 16, 981426. [Google Scholar] [CrossRef]
- Florez-Vargas, A.; Vargas, S.O.; Debelenko, L.V.; Perez-Atayde, A.R.; Archibald, T.; Kozakewich, H.P.; Zurakowski, D. Comparative analysis of D2-40 and LYVE-1 immunostaining in lymphatic malformations. Lymphology 2008, 41, 103–110. [Google Scholar]
- Fukunaga, M. Expression of D2-40 in lymphatic endothelium of normal tissues and in vascular tumours. Histopathology 2005, 46, 396–402. [Google Scholar] [CrossRef]
- Heinzelbecker, J.; Kempf, K.M.; Kurz, K.; Steidler, A.; Weiss, C.; Jackson, D.G.; Bolenz, C.; Haecker, A.; Trojan, L. Lymph vessel density in seminomatous testicular cancer assessed with the specific lymphatic endothelium cell markers D2-40 and LYVE-1: Correlation with pathologic parameters and clinical outcome. Urol. Oncol. 2013, 31, 1386–1394. [Google Scholar] [CrossRef]
- Schneider, C.A.; Rasband, W.S.; Eliceiri, K.W. NIH image to imageJ: 25 years of image analysis. Nat. Methods 2012, 9, 671–675. [Google Scholar] [CrossRef] [PubMed]
- Pirri, C.; Petrelli, L.; Fede, C.; Guidolin, D.; Tiengo, C.; De Caro, R.; Stecco, C. Blood supply to the superficial fascia of the abdomen: An anatomical study. Clin. Anat. 2022. [Google Scholar] [CrossRef]
- Ryan, T.J.; De Berker, D. The interstitium, the connective tissue environment of the lymphatic, and angiogenesis in human skin. Clin. Dermatol. 1995, 13, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Solari, E.; Marcozzi, C.; Negrini, E.; Moriondo, A. Lymphatic Vessels and Their Surroundings: How Local Physical Factors Affect Lymph Flow. Biology 2020, 9, 463. [Google Scholar] [CrossRef] [PubMed]
- Avraham, T.; Clavin, N.W.; Daluvoy, S.V.; Fernandez, J.; Soares, M.A.; Cordeiro, A.P.; Mehrara, B.J. Fibrosis is a key inhibitor of lymphatic regeneration. Plast. Reconstr. Surg. 2009, 124, 438–450. [Google Scholar] [CrossRef] [Green Version]
- O’Kelly, N.; Nguyen, K.; Gibstein, A.; Bradley, J.P.; Tanna, N.; Matarasso, A. Standards and Trends in Lipoabdominoplasty. Plast. Reconstr. Surg. Glob. Open 2020, 8, e3144. [Google Scholar] [CrossRef] [PubMed]
- Bassalobre, M.; Liebano, R.E.; da Silva, M.P.; Castiglioni, M.L.V.; Sadala, A.Y.; Ferreira, L.M.; Nahas, F.X. Changes in the Pattern of Superficial Lymphatic Drainage of the Abdomen after Abdominoplasty. Plast. Reconstr. Surg. 2022, 149, 1106e–1113e. [Google Scholar] [CrossRef] [PubMed]
- Tourani, S.S.; Taylor, G.I.; Ashton, M.W. Scarpa Fascia Preservation in Abdominoplasty: Does It Preserve the Lymphatics? Plast. Reconstr. Surg. 2015, 136, 258–262. [Google Scholar] [CrossRef]
- Lee, D.G.; Lee, S.; Kim, K.T. Computed Tomography-Based Quantitative Analysis of Fibrotic Changes in Skin and Subcutaneous Tissue in Lower Extremity Lymphedema Following Gynecologic Cancer Surgery. Lymphat. Res. Biol. 2022, 20, 488–495. [Google Scholar] [CrossRef]
- Viviano, S.L.; Neligan, P.C. Updates on Excisional Procedures for Lymphedema. Adv. Wound Care 2022, 11, 419–427. [Google Scholar] [CrossRef]
- Baptista, L.S.; Côrtes, I.; Montenegro, B.; Claudio-da-Silva, C.; Bouschbacher, M.; Jobeili, L.; Auxenfans, C.; Sigaudo-Roussel, D. A novel conjunctive microenvironment derived from human subcutaneous adipose tissue contributes to physiology of its superficial layer. Stem Cell Res. Ther. 2021, 12, 480. [Google Scholar] [CrossRef]
- Hsu, J.F.; Yu, R.P.; Stanton, E.W.; Wang, J.; Wong, A.K. Current Advancements in Animal Models of Postsurgical Lymphedema: A Systematic Review. Adv. Wound Care 2022, 11, 399–418. [Google Scholar] [CrossRef]
- Savetsky, I.L.; Torrisi, J.S.; Cuzzone, D.A.; Ghanta, S.; Albano, N.J.; Gardenier, J.C.; Joseph, W.J.; Mehrara, B.J. Obesity increases inflammation and impairs lymphatic function in a mouse model of lymphedema. Am. J. Physiol. Heart Circ. Physiol. 2014, 307, H165–H172. [Google Scholar] [CrossRef] [Green Version]
- Scallan, J.P.; Zawieja, S.D.; Castorena-Gonzalez, J.A.; Davis, M.J. Lymphatic pumping: Mechanics, mechanisms and malfunction. J. Physiol. 2016, 594, 5749–5768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiig, H.; Schröder, A.; Neuhofer, W.; Jantsch, J.; Kopp, C.; Karlsen, T.V.; Boschmann, M.; Goss, J.; Bry, M.; Rakova, N.; et al. Immune cells control skin lymphatic electrolyte homeostasis and blood pressure. J. Clin. Investig. 2013, 123, 2803–2815. [Google Scholar] [CrossRef]
- Fede, C.; Pirri, C.; Fan, C.; Albertin, G.; Porzionato, A.; Macchi, V.; De Caro, R.; Stecco, C. Sensitivity of the fasciae to sex hormone levels: Modulation of collagen-I, collagen-III and fibrillin production. PLoS ONE 2019, 14, e0223195. [Google Scholar] [CrossRef] [PubMed]
- Fede, C.; Pirri, C.; Fan, C.; Petrelli, L.; Guidolin, D.; De Caro, R.; Stecco, C. A Closer Look at the Cellular and Molecular Components of the Deep/Muscular Fasciae. Int. J. Mol. Sci. 2021, 22, 1411. [Google Scholar] [CrossRef] [PubMed]








Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albertin, G.; Astolfi, L.; Fede, C.; Simoni, E.; Contran, M.; Petrelli, L.; Tiengo, C.; Guidolin, D.; De Caro, R.; Stecco, C. Detection of Lymphatic Vessels in the Superficial Fascia of the Abdomen. Life 2023, 13, 836. https://doi.org/10.3390/life13030836
Albertin G, Astolfi L, Fede C, Simoni E, Contran M, Petrelli L, Tiengo C, Guidolin D, De Caro R, Stecco C. Detection of Lymphatic Vessels in the Superficial Fascia of the Abdomen. Life. 2023; 13(3):836. https://doi.org/10.3390/life13030836
Chicago/Turabian StyleAlbertin, Giovanna, Laura Astolfi, Caterina Fede, Edi Simoni, Martina Contran, Lucia Petrelli, Cesare Tiengo, Diego Guidolin, Raffaele De Caro, and Carla Stecco. 2023. "Detection of Lymphatic Vessels in the Superficial Fascia of the Abdomen" Life 13, no. 3: 836. https://doi.org/10.3390/life13030836
APA StyleAlbertin, G., Astolfi, L., Fede, C., Simoni, E., Contran, M., Petrelli, L., Tiengo, C., Guidolin, D., De Caro, R., & Stecco, C. (2023). Detection of Lymphatic Vessels in the Superficial Fascia of the Abdomen. Life, 13(3), 836. https://doi.org/10.3390/life13030836