
The Role of Oxidative Stress in the Aging Eye


Abstract
:1. Introduction
2. External and Anterior Segment Changes
2.1. Eyelids and Lacrimal Glands
2.2. Sclera
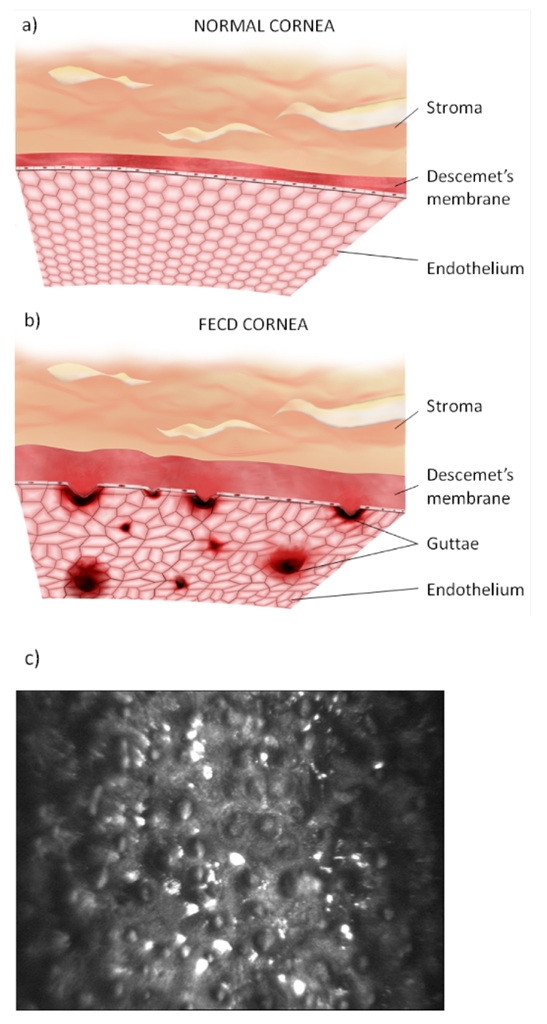
2.3. Cornea
2.4. Trabecular Meshwork
2.5. Ciliary Body
2.6. Crystalline Lens
3. Posterior Segment Aging Changes
3.1. Vitreous Humor
3.2. Retina and Retinal Pigment Epithelium
3.3. Choroid
3.4. Macula and Fovea
3.5. Optic Nerve
4. Age-Related Eye Disease and the Role of Oxidative Stress
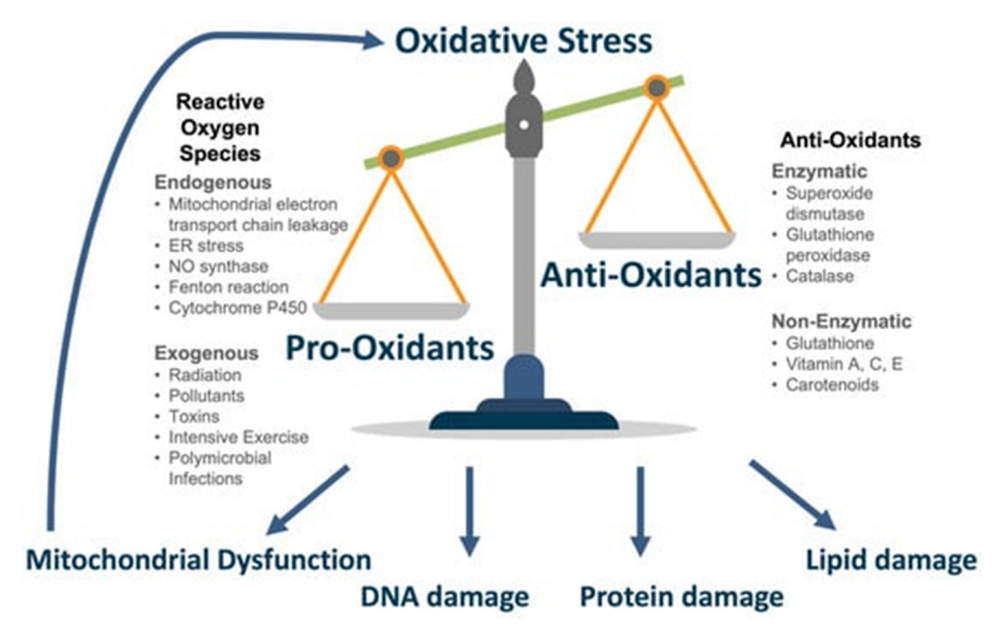
4.1. Role of Oxidative Stress in Aging
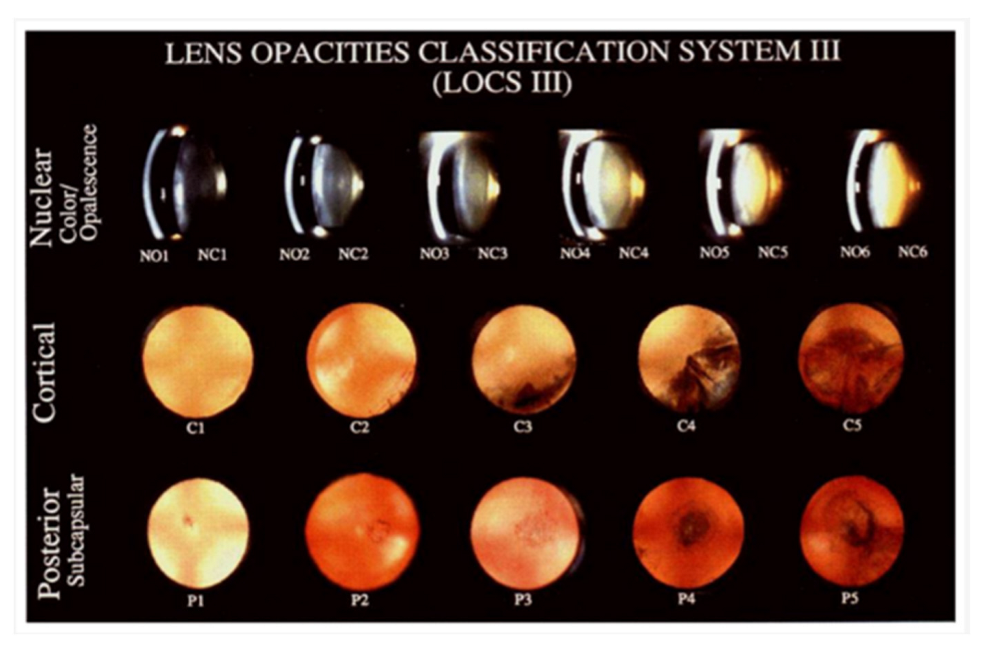
4.2. Cataracts
4.3. Glaucoma
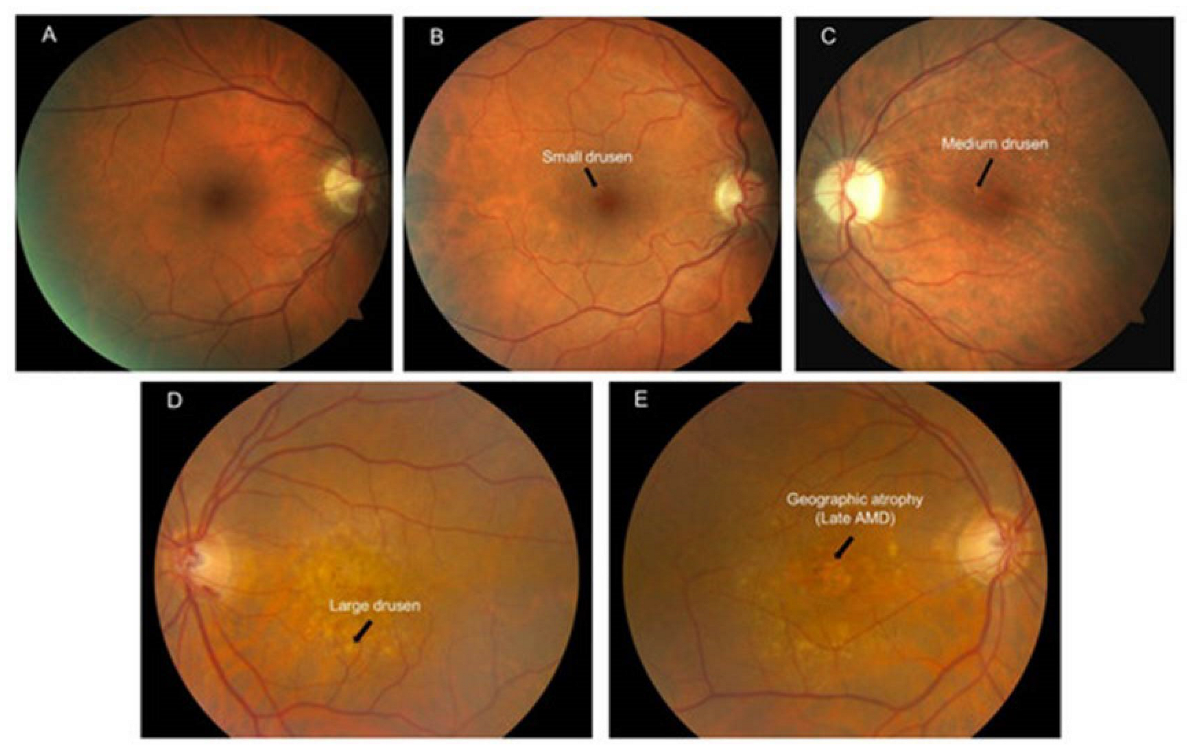
4.4. Age-Related Macular Degeneration
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Census Bureau. The U.S. Joins Other Countries with Large Aging Populations. Available online: https://www.census.gov/library/stories/2018/03/graying-america.html (accessed on 7 November 2022).
- Aging and Your Eyes|National Institute on Aging. Available online: https://www.nia.nih.gov/health/aging-and-your-eyes (accessed on 7 November 2022).
- Klein, R.; Klein, B.E.K. The Prevalence of Age-Related Eye Diseases and Visual Impairment in Aging: Current Estimates. Investig. Opthalmol. Vis. Sci. 2013, 54, ORSF5–ORSF13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salvi, S.M. Ageing changes in the eye. Postgrad. Med. J. 2006, 82, 581–587. [Google Scholar] [CrossRef]
- Eye Health Data and Statistics|National Eye Institute. Available online: https://www.nei.nih.gov/learn-about-eye-health/eye-health-data-and-statistics (accessed on 6 February 2023).
- Shmuely-Dulitzki, Y.; Rovner, B.W. Screening for Depression in Older Persons With Low Vision: Somatic Eye Symptoms and the Geriatric Depression Scale. Am. J. Geriatr. Psychiatry 1997, 5, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Quillen, D.A. Common Causes of Vision Loss in Elderly Patients. Am. Fam. Physician 1999, 60, 99–108. Available online: https://www.aafp.org/pubs/afp/issues/1999/0701/p99.html (accessed on 7 November 2022).
- Ko, A.C.; Korn, B.S.; Kikkawa, D.O. The aging face. Surv. Ophthalmol. 2016, 62, 190–202. [Google Scholar] [CrossRef]
- Naylor, E.C.; Watson, R.E.; Sherratt, M.J. Molecular aspects of skin ageing. Maturitas 2011, 69, 249–256. [Google Scholar] [CrossRef]
- Darcy, S.J.; Miller, T.A.; Goldberg, R.A.; Villablanca, J.P.; Demer, J.L.; Rudkin, G.H. Magnetic Resonance Imaging Characterization of Orbital Changes with Age and Associated Contributions to Lower Eyelid Prominence. Plast. Reconstr. Surg. 2008, 122, 921–929. [Google Scholar] [CrossRef]
- Wendell Damasceno, R.; Avgitidou, G.; Belfort R., R., Jr.; Correa Dantas, P.E.; M Holbach, L.; M Heindl, L. Eyelid aging: Pathophysiology and clinical management. Arq. Bras. Oftalmol. 2015, 78, 328–331. [Google Scholar] [CrossRef] [Green Version]
- Flament, F.; Francois, G.; Seyrek, I.; Saint-Leger, D. Age-related changes to characteristics of the human eyes in women from six different ethnicities. Ski. Res. Technol. 2020, 26, 520–528. [Google Scholar] [CrossRef]
- de Paiva, C.S. Effects of Aging in Dry Eye. Int. Ophthalmol. Clin. 2017, 57, 47–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bukhari, A.A.; Basheer, N.A.; Joharjy, H.I. Age, Gender, and Interracial Variability of Normal Lacrimal Gland Volume Using MRI. Ophthalmic Plast. Reconstr. Surg. 2014, 30, 388–391. [Google Scholar] [CrossRef]
- Obata, H.; Yamamoto, S.; Horiuchi, H.; Machinami, R. Histopathologic Study of Human Lacrimal Gland. Ophthalmology 1995, 102, 678–686. [Google Scholar] [CrossRef]
- Nasu, M.; Matsubara, O.; Yamamoto, H. Post-mortem prevalence of lymphocytic infiltration of the lacrymal gland: A comparative study in autoimmune and non-autoimmune diseases. J. Pathol. 1984, 143, 11–15. [Google Scholar] [CrossRef]
- El-Fadaly, A.B.; El-Shaarawy, E.A.; Rizk, A.A.; Nasralla, M.M.; Shuaib, D.M. Age-related alterations in the lacrimal gland of adult albino rat: A light and electron microscopic study. Ann. Anat.-Anat. Anz. 2014, 196, 336–351. [Google Scholar] [CrossRef]
- Kitazawa, K.; Inomata, T.; Shih, K.; Hughes, J.-W.B.; Bozza, N.; Tomioka, Y.; Numa, K.; Yokoi, N.; Campisi, J.; Dana, R.; et al. Impact of aging on the pathophysiology of dry eye disease: A systematic review and meta-analysis. Ocul. Surf. 2022, 25, 108–118. [Google Scholar] [CrossRef] [PubMed]
- Vurgese, S.; Panda-Jonas, S.; Jonas, J.B. Scleral Thickness in Human Eyes. PLoS ONE 2012, 7, e29692. [Google Scholar] [CrossRef]
- Coudrillier, B.; Tian, J.; Alexander, S.P.; Myers, K.; Quigley, H.A.; Nguyen, T.D. Biomechanics of the Human Posterior Sclera: Age- and Glaucoma-Related Changes Measured Using Inflation Testing. Investig. Opthalmol. Vis. Sci. 2012, 53, 1714–1728. [Google Scholar] [CrossRef]
- Ebneter, A.; Häner, N.U.; Zinkernagel, M.S. Metrics of the normal anterior sclera: Imaging with optical coherence tomography. Graefe’s Arch. Clin. Exp. Ophthalmol. 2015, 253, 1575–1580. [Google Scholar] [CrossRef] [Green Version]
- Read, S.A.; Alonso-Caneiro, D.; Vincent, S.J.; Bremner, A.; Fothergill, A.; Ismail, B.; McGraw, R.; Quirk, C.J.; Wrigley, E. Anterior eye tissue morphology: Scleral and conjunctival thickness in children and young adults. Sci. Rep. 2016, 6, 33796. [Google Scholar] [CrossRef] [Green Version]
- Boote, C.; Sigal, I.A.; Grytz, R.; Hua, Y.; Nguyen, T.D.; Girard, M.J. Scleral structure and biomechanics. Prog. Retin. Eye Res. 2019, 74, 100773. [Google Scholar] [CrossRef]
- A Rada, J.; Achen, V.R.; Penugonda, S.; Schmidt, R.W.; A Mount, B. Proteoglycan composition in the human sclera during growth and aging. Investig. Opthalmol. Vis. Sci. 2000, 41, 1639–1648. [Google Scholar]
- Cogan, D.G.; Kuwabara, T. Focal Senile Translucency of the Sclera. Arch. Ophthalmol. 1959, 62, 604–610. [Google Scholar] [CrossRef]
- Grossniklaus, H.E.; Nickerson, J.M.; Edelhauser, H.F.; Bergman, L.A.M.K.; Berglin, L. Anatomic Alterations in Aging and Age-Related Diseases of the Eye. Investig. Opthalmol. Vis. Sci. 2013, 54, ORSF23–ORSF27. [Google Scholar] [CrossRef]
- Fazio, M.A.; Grytz, R.; Morris, J.S.; Bruno, L.; Girkin, C.A.; Downs, J.C. Human Scleral Structural Stiffness Increases More Rapidly With Age in Donors of African Descent Compared to Donors of European Descent. Investig. Opthalmol. Vis. Sci. 2014, 55, 7189–7198. [Google Scholar] [CrossRef] [PubMed]
- Gipson, I.K. Age-Related Changes and Diseases of the Ocular Surface and Cornea. Investig. Opthalmol. Vis. Sci. 2013, 54, ORSF48–ORSF53. [Google Scholar] [CrossRef] [Green Version]
- Wojcik, K.A.; Kaminska, A.; Blasiak, J.; Szaflik, J.; Szaflik, J.P. Oxidative Stress in the Pathogenesis of Keratoconus and Fuchs Endothelial Corneal Dystrophy. Int. J. Mol. Sci. 2013, 14, 19294–19308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Namba, H.; Sugano, A.; Murakami, T.; Utsunomiya, H.; Nishitsuka, K.; Ishizawa, K.; Kayama, T.; Yamashita, H. Age-Related Changes in Astigmatism and Potential Causes. Cornea 2020, 39, S34–S38. [Google Scholar] [CrossRef]
- Shao, X.; Zhou, K.-J.; Pan, A.-P.; Cheng, X.-Y.; Cai, H.-X.; Huang, J.; Yu, A.-Y. Age-Related Changes in Corneal Astigmatism. J. Refract. Surg. 2017, 33, 696–703. [Google Scholar] [CrossRef]
- Munjal, A.; Kaufman, E.J. “Arcus Senilis,” StatPearls. 2022. Available online: https://www-ncbi-nlm-nih-gov.ezproxy.bu.edu/books/NBK554370/ (accessed on 11 November 2022).
- Durand, L.; Bouvier, R.; Burillon, C.; Mutti, P. Cornea farinata. Report of a case: Clinical, histologic and ultrastructural study. J. Fr. Ophtalmol. 1990, 13, 449–455. [Google Scholar]
- Belliveau, M.J.; Brownstein, S.; Agapitos, P.; Font, R.L. Ultrastructural Features of Posterior Crocodile Shagreen of the Cornea. Surv. Ophthalmol. 2009, 54, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Hazlett, L.D.; Kreindler, F.B.; Berk, R.S.; Barrett, R. Aging alters the phagocytic capability of inflammatory cells induced into cornea. Curr. Eye Res. 1990, 9, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Hobden, J.A.; Masinick, S.A.; Barrett, R.P.; Hazlett, L.D. Aged mice fail to upregulate ICAM-1 after Pseudomonas aeruginosa corneal infection. Investig. Ophthalmol. Vis. Sci. 1995, 36, 1107–1114. [Google Scholar]
- van der Meulen, I.J.; van Rooij, J.; Nieuwendaal, C.P.; Van Cleijnenbreugel, H.; Geerards, A.J.; Remeijer, L. Age-related Risk Factors, Culture Outcomes, and Prognosis in Patients Admitted With Infectious Keratitis to Two Dutch Tertiary Referral Centers. Cornea 2008, 27, 539–544. [Google Scholar] [CrossRef]
- Constantinou, M.; Jhanji, V.; Tao, L.W.; Vajpayee, R.B. Clinical review of corneal ulcers resulting in evisceration and enucleation in elderly population. Graefe’s Arch. Clin. Exp. Ophthalmol. 2009, 247, 1389–1393. [Google Scholar] [CrossRef]
- McMenamin, P.; Lee, W.R.; Aitken, D.A. Age-related Changes in the Human Outflow Apparatus. Ophthalmology 1986, 93, 194–209. [Google Scholar] [CrossRef]
- Choi, W.; Bae, H.W.; Cho, H.; Kim, E.W.; Kim, C.Y.; Seong, G.J. Evaluation of the Relationship Between Age and Trabecular Meshwork Height to Predict the Risk of Glaucoma. Sci. Rep. 2020, 10, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Alvarado, J.; Murphy, C.; Polansky, J.; Juster, R. Age-related changes in trabecular meshwork cellularity. Investig. Opthalmol. Vis. Sci. 1981, 21, 714–727. Available online: https://pubmed-ncbi-nlm-nih-gov.ezproxy.bu.edu/7298275/ (accessed on 9 November 2022).
- Sundaresan, Y.; Veerappan, M.; Ramasamy, K.S.; Chidambaranathan, G.P. Identification, quantification and age-related changes of human trabecular meshwork stem cells. Eye Vis. 2019, 6, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Miyazaki, M.; Segawa, K.; Urakawa, Y. Age-related changes in the trabecular meshwork of the normal human eye. Jpn. J. Ophthalmol. 1987, 31, 558–569. Available online: https://pubmed-ncbi-nlm-nih-gov.ezproxy.bu.edu/3448324/ (accessed on 9 November 2022).
- Cracknell, K.P.; Grierson, I.; Hogg, P.; Majekodunmi, A.A.; Watson, P.; Marmion, V. Melanin in the trabecular meshwork is associated with age, POAG but not Latanoprost treatment. A masked morphometric study. Exp. Eye Res. 2006, 82, 986–993. [Google Scholar] [CrossRef]
- Pardue, M.T.; Sivak, J.G. Age-Related Changes in Human Ciliary Muscle. Optom. Vis. Sci. 2000, 77, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Xie, X.; Corradetti, G.; Song, A.; Pardeshi, A.; Sultan, W.; Lee, J.Y.; Yu, F.; Zhang, L.; Chen, S.; Chopra, V.; et al. Age- and refraction-related changes in anterior segment anatomical structures measured by swept-source anterior segment OCT. PLoS ONE 2020, 15, e0240110. [Google Scholar] [CrossRef]
- A Strenk, S.; Semmlow, J.L.; Strenk, L.M.; Munoz, P.; Gronlund-Jacob, J.; Demarco, J.K. Age-related changes in human ciliary muscle and lens: A magnetic resonance imaging study. Investig. Opthalmol. Vis. Sci. 1999, 40, 1162–1169. [Google Scholar]
- Martinez-Enriquez, E.; de Castro, A.; Mohamed, A.; Sravani, N.G.; Ruggeri, M.; Manns, F.; Marcos, S. Age-Related Changes to the Three-Dimensional Full Shape of the Isolated Human Crystalline Lens. Investig. Opthalmol. Vis. Sci. 2020, 61, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, K.H.; Gibson, G.A. Intraocular lens short wavelength light filtering. Clin. Exp. Optom. 2010, 93, 390–399. [Google Scholar] [CrossRef] [PubMed]
- Turner, P.L.; Mainster, M.A. Circadian photoreception: Ageing and the eye’s important role in systemic health. Br. J. Ophthalmol. 2008, 92, 1439–1444. [Google Scholar] [CrossRef] [Green Version]
- Zaki, W.M.D.W.; Mutalib, H.A.; Ramlan, L.A.; Hussain, A.; Mustapha, A. Towards a Connected Mobile Cataract Screening System: A Future Approach. J. Imaging 2022, 8, 41. [Google Scholar] [CrossRef]
- Wishart, T.F.; Flokis, M.; Shu, D.Y.; Das, S.J.; Lovicu, F.J. Hallmarks of lens aging and cataractogenesis. Exp. Eye Res. 2021, 210, 108709. [Google Scholar] [CrossRef] [PubMed]
- Richdale, K.; Sinnott, L.T.; Bullimore, M.A.; Wassenaar, P.A.; Schmalbrock, P.; Kao, C.-Y.; Patz, S.; Mutti, N.O.; Glasser, A.; Zadnik, K. Quantification of Age-Related and per Diopter Accommodative Changes of the Lens and Ciliary Muscle in the Emmetropic Human Eye. Investig. Opthalmol. Vis. Sci. 2013, 54, 1095–1105. [Google Scholar] [CrossRef] [Green Version]
- Croft, M.A.; Glasser, A.; Heatley, G.; McDonald, J.; Ebbert, T.; Dahl, D.B.; Nadkarni, N.V.; Kaufman, P.L. Accommodative Ciliary Body and Lens Function in Rhesus Monkeys, I: Normal Lens, Zonule and Ciliary Process Configuration in the Iridectomized Eye. Investig. Opthalmol. Vis. Sci. 2006, 47, 1076–1086. [Google Scholar] [CrossRef] [PubMed]
- Tamm, E.; Croft, M.A.; Jungkunz, W.; Lütjen-Drecoll, E.; Kaufman, P.L. Age-Related Loss of Ciliary Muscle Mobility in the Rhesus Monkey. Arch. Ophthalmol. 1992, 110, 871–876. [Google Scholar] [CrossRef] [PubMed]
- Heys, K.R.; Cram, S.L.; Truscott, R.J.W. Massive increase in the stiffness of the human lens nucleus with age: The basis for presbyopia? Mol. Vis. 2004, 10, 956–963. [Google Scholar]
- Heys, K.R.; Friedrich, M.G.; Truscott, R.J.W. Presbyopia and heat: Changes associated with aging of the human lens suggest a functional role for the small heat shock protein, α-crystallin, in maintaining lens flexibility. Aging Cell 2007, 6, 807–815. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Grami, V.; Marrero, Y.; Tang, D.; Yappert, M.C.; Rasi, V.; Borchman, D. Human Lens Phospholipid Changes with Age and Cataract. Investig. Opthalmol. Vis. Sci. 2005, 46, 1682–1689. [Google Scholar] [CrossRef] [PubMed]
- Lumi, X.; Hawlina, M.; Glavač, D.; Facskó, A.; Moe, M.C.; Kaarniranta, K.; Petrovski, G. Ageing of the vitreous: From acute onset floaters and flashes to retinal detachment. Ageing Res. Rev. 2015, 21, 71–77. [Google Scholar] [CrossRef]
- Bishop, P.N.; Holmes, D.F.; Kadler, K.E.; McLeod, D.; Bos, K.J. Age-related changes on the surface of vitreous collagen fibrils. Investig. Opthalmol. Vis. Sci. 2004, 45, 1041–1046. [Google Scholar] [CrossRef] [Green Version]
- Sebag, J. Ageing of the vitreous. Eye 1987, 1, 254–262. [Google Scholar] [CrossRef]
- Gastaud, P.; Paoli, V.; Freton, A. Le vieillissement du vitré. J. Fr. D’ophtalmologie 2012, 35, 371–377. [Google Scholar] [CrossRef]
- Walton, K.A.; Meyer, C.H.; Harkrider, C.J.; Cox, T.A.; Toth, C.A. Age-Related Changes in Vitreous Mobility as Measured by Video B Scan Ultrasound. Exp. Eye Res. 2002, 74, 173–180. [Google Scholar] [CrossRef]
- Teng, C.; Chi, H. Vitreous Changes and the Mechanism of Retinal Detachment. Am. J. Ophthalmol. 1957, 44, 335–356. [Google Scholar] [CrossRef]
- Levin, M.; Cohen, N. The effects of aging on the mechanical properties of the vitreous. J. Biomech. 2021, 119, 110310. [Google Scholar] [CrossRef]
- Schulz, A.; Wahl, S.; Rickmann, A.; Ludwig, J.; Stanzel, B.V.; von Briesen, H.; Szurman, P. Age-Related Loss of Human Vitreal Viscoelasticity. Transl. Vis. Sci. Technol. 2019, 8, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonnel, S.; Mohand-Said, S.; Sahel, J.-A. The aging of the retina. Exp. Gerontol. 2003, 38, 825–831. [Google Scholar] [CrossRef]
- Gao, H.; Hollyfield, J.G. Aging of the human retina. Differential loss of neurons and retinal pigment epithelial cells. Investig. Opthalmol. Vis. Sci. 1992, 33, 1–17. [Google Scholar]
- A Curcio, C.; Millican, C.L.; A Allen, K.; E Kalina, R. Aging of the human photoreceptor mosaic: Evidence for selective vulnerability of rods in central retina. Investig. Opthalmol. Vis. Sci. 1993, 34, 3278–3296. [Google Scholar]
- Cunea, A.; Jeffery, G. The ageing photoreceptor. Vis. Neurosci. 2007, 24, 151–155. [Google Scholar] [CrossRef] [Green Version]
- Aggarwal, P.; Nag, T.C.; Wadhwa, S. Age-related decrease in rod bipolar cell density of the human retina: An immunohistochemical study. J. Biosci. 2007, 32, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, Y.; Yamamoto, Y.; Marugame, A.; Ogura, M.; Saito, A.; Ohta, K.; Fukumoto, M.; Murata, T. Age-Related Decrease of the Retinal Vasculature Area Identified with a Novel Computer-Aided Analysis System. Tohoku J. Exp. Med. 2012, 228, 229–237. [Google Scholar] [CrossRef] [Green Version]
- Orlov, N.V.; Coletta, C.; Van Asten, F.; Qian, Y.; Ding, J.; AlGhatrif, M.; Lakatta, E.; Chew, E.; Wong, W.; Swaroop, A.; et al. Age-related changes of the retinal microvasculature. PLoS ONE 2019, 14, e0215916. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, E.; Ripandelli, G.; Taurone, S.; Feher, J.; Plateroti, R.; Kovacs, I.; Magliulo, G.; Orlando, M.P.; Micera, A.; Battaglione, E.; et al. Age and diabetes related changes of the retinal capillaries: An ultrastructural and immunohistochemical study. Int. J. Immunopathol. Pharmacol. 2015, 29, 40–53. [Google Scholar] [CrossRef] [Green Version]
- Friedman, E. The Retinal Pigment Epithelium. Arch. Ophthalmol. 1968, 79, 315–320. [Google Scholar] [CrossRef]
- Bonilha, V.L. Age and disease-related structural changes in the retinal pigment epithelium. Clin. Ophthalmol. 2008, 2, 413–424. [Google Scholar] [CrossRef] [Green Version]
- Schütt, F.; Davies, S.; Kopitz, J.; Holz, F.G.; Boulton, M.E. Photodamage to human RPE cells by A2-E, a retinoid component of lipofuscin. Investig. Ophthalmol. Vis. Sci. 2000, 41, 2303–2308. [Google Scholar]
- Boulton, M.; Dontsov, A.; Jarvis-Evans, J.; Ostrovsky, M.; Svistunenko, D. Lipofuscin is a photoinducible free radical generator. J. Photochem. Photobiol. B Biol. 1993, 19, 201–204. [Google Scholar] [CrossRef]
- Boulton, M.; Docchio, F.; Dayhaw-Barker, P.; Ramponi, R.; Cubeddu, R. Age-related changes in the morphology, absorption and fluorescence of melanosomes and lipofuscin granules of the retinal pigment epithelium. Vis. Res. 1990, 30, 1291–1303. [Google Scholar] [CrossRef]
- Sarna, T.; Burke, J.M.; Korytowski, W.; Różanowska, M.; Skumatz, C.M.; Zaręba, A.; Zaręba, M. Loss of melanin from human RPE with aging: Possible role of melanin photooxidation. Exp. Eye Res. 2002, 76, 89–98. [Google Scholar] [CrossRef]
- Spaide, R.F. Age-Related Choroidal Atrophy. Am. J. Ophthalmol. 2009, 147, 801–810. [Google Scholar] [CrossRef]
- Zhou, H.; Dai, Y.; Shi, Y.; Russell, J.F.; Lyu, C.; Noorikolouri, J.; Feuer, W.J.; Chu, Z.; Zhang, Q.; de Sisternes, L.; et al. Age-Related Changes in Choroidal Thickness and the Volume of Vessels and Stroma Using Swept-Source OCT and Fully Automated Algorithms. Ophthalmol. Retin. 2019, 4, 204–215. [Google Scholar] [CrossRef]
- Ramrattan, R.S.; van der Schaft, T.L.; Mooy, C.M.; de Bruijn, W.C.; Mulder, P.G.; de Jong, P.T. Morphometric analysis of Bruch’s membrane, the choriocapillaris, and the choroid in aging. Investig. Ophthalmol. Vis. Sci. 1994, 35, 2857–2864. [Google Scholar]
- Nag, T.C. Ultrastructural changes in the melanocytes of aging human choroid. Micron 2015, 79, 16–23. [Google Scholar] [CrossRef]
- Ardeljan, D.; Chan, C.-C. Aging is not a disease: Distinguishing age-related macular degeneration from aging. Prog. Retin. Eye Res. 2013, 37, 68–89. [Google Scholar] [CrossRef] [Green Version]
- Hussain, A.; Starita, C.; Hodgetts, A.; Marshall, J. Macromolecular diffusion characteristics of ageing human Bruch’s membrane: Implications for age-related macular degeneration (AMD). Exp. Eye Res. 2010, 90, 703–710. [Google Scholar] [CrossRef]
- Hussain, A.A.; Rowe, L.; Marshall, J. Age-related alterations in the diffusional transport of amino acids across the human Bruch’s-choroid complex. J. Opt. Soc. Am. A 2002, 19, 166–172. [Google Scholar] [CrossRef]
- Harris, A.; Wirostko, B. Age-related macular degeneration and the aging eye. Clin. Interv. Aging 2008, ume 3, 473–482. [Google Scholar] [CrossRef] [Green Version]
- Nittala, M.G.; Corvi, F.; Maram, J.; Velaga, S.B.; Haines, J.; Pericak-Vance, M.A.; Stambolian, D.; Sadda, S.R. Risk Factors for Progression of Age-Related Macular Degeneration: Population-Based Amish Eye Study. J. Clin. Med. 2022, 11, 5110. [Google Scholar] [CrossRef]
- Kadhim, Z.G.; Mohammad, N.K. Effect of aging and lifestyle on healthy macular photoreceptors and retinal pigment epithelium-Bruch membrane complex thickness. Eur. J. Ophthalmol. 2022, 33, 441–447. [Google Scholar] [CrossRef]
- Ito, Y.N.; Mori, K.; Young-Duvall, J.; Yoneya, S. Aging changes of the choroidal dye filling pattern in indocyanine green angiography of normal subjects. Retina 2001, 21, 237–242. [Google Scholar] [CrossRef]
- Grunwald, J.E.; Hariprasad, S.M.; Dupont, J. Effect of aging on foveolar choroidal circulation. Arch. Ophthalmol. 1998, 116, 150–154. [Google Scholar] [CrossRef] [Green Version]
- Balazsi, A.; Rootman, J.; Drance, S.; Schulzer, M.; Douglas, G. The Effect of Age on the Nerve Fiber Population of the Human Optic Nerve. Am. J. Ophthalmol. 1984, 97, 760–766. [Google Scholar] [CrossRef]
- Moya, F.J.; Brigatti, L.; Caprioli, J. Effect of aging on optic nerve appearance: A longitudinal study. Br. J. Ophthalmol. 1999, 83, 567–572. [Google Scholar] [CrossRef] [Green Version]
- Johnson, B.M.; Miao, M.; Sadun, A.A. Age-related decline of human optic nerve axon populations. Age 1987, 10, 5–9. [Google Scholar] [CrossRef]
- Coleman-Belin, J.; Harris, A.; Chen, B.; Zhou, J.; Ciulla, T.; Verticchio, A.; Antman, G.; Chang, M.; Siesky, B. Aging Effects on Optic Nerve Neurodegeneration. Int. J. Mol. Sci. 2023, 24, 2573. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.B.; Lim, M.; Gajjar, A.; Evans, K.B.; Harwerth, R.S. Age-Associated Changes in the Retinal Nerve Fiber Layer and Optic Nerve Head. Investig. Opthalmol. Vis. Sci. 2014, 55, 5134–5143. [Google Scholar] [CrossRef]
- Boehm, A.G.; Koeller, A.U.; Pillunat, L.E. The Effect of Age on Optic Nerve Head Blood Flow. Investig. Opthalmol. Vis. Sci. 2005, 46, 1291–1295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wickens, A.P. Ageing and the free radical theory. Respir. Physiol. 2001, 128, 379–391. [Google Scholar] [CrossRef] [PubMed]
- Hurley, D.J.; Normile, C.; Irnaten, M.; O’Brien, C. The Intertwined Roles of Oxidative Stress and Endoplasmic Reticulum Stress in Glaucoma. Antioxidants 2022, 11, 886. [Google Scholar] [CrossRef]
- Cataract Tables|National Eye Institute. Available online: https://www.nei.nih.gov/learn-about-eye-health/eye-health-data-and-statistics/cataract-data-and-statistics/cataract-tables (accessed on 18 November 2022).
- Asbell, P.A.; Dualan, I.; Mindel, J.; Brocks, D.; Ahmad, M.; Epstein, S. Age-related cataract. Lancet 2005, 365, 599–609. [Google Scholar] [CrossRef]
- Su, S.-P.; McArthur, J.D.; Truscott, R.J.; Aquilina, J.A. Truncation, cross-linking and interaction of crystallins and intermediate filament proteins in the aging human lens. Biochim. Biophys. Acta 2011, 1814, 647–656. [Google Scholar] [CrossRef]
- Truscott, R.J.; Mizdrak, J.; Friedrich, M.G.; Hooi, M.Y.; Lyons, B.; Jamie, J.; Davies, M.; Wilmarth, P.A.; David, L.L. Is protein methylation in the human lens a result of non-enzymatic methylation by S-adenosylmethionine? Exp. Eye Res. 2012, 99, 48–54. [Google Scholar] [CrossRef] [Green Version]
- Franke, S.; Dawczynski, J.; Strobel, J.; Niwa, T.; Stahl, P.; Stein, G. Increased levels of advanced glycation end products in human cataractous lenses. J. Cataract. Refract. Surg. 2003, 29, 998–1004. [Google Scholar] [CrossRef]
- Tweeddale, H.J.; Hawkins, C.L.; Janmie, J.F.; Truscott, R.J.W.; Davies, M.J. Cross-linking of lens crystallin proteins induced by tryptophan metabolites and metal ions: Implications for cataract development. Free. Radic. Res. 2016, 50, 1116–1130. [Google Scholar] [CrossRef] [PubMed]
- Hooi, M.Y.S.; Truscott, R.J.W. Racemisation and human cataract. d-Ser, d-Asp/Asn and d-Thr are higher in the lifelong proteins of cataract lenses than in age-matched normal lenses. Age 2010, 33, 131–141. [Google Scholar] [CrossRef] [Green Version]
- Hains, P.G.; Truscott, R.J.W. Age-Dependent Deamidation of Lifelong Proteins in the Human Lens. Investig. Opthalmol. Vis. Sci. 2010, 51, 3107–3114. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Estrada, R.; Yappert, M.C.; Borchman, D. Oxidation-induced changes in human lens epithelial cells. Free. Radic. Biol. Med. 2006, 41, 1425–1432. [Google Scholar] [CrossRef]
- Tinaztepe, E.; Ay, M.; Eser, E. Nuclear and Mitochondrial DNA of Age-Related Cataract Patients Are Susceptible to Oxidative Damage. Curr. Eye Res. 2016, 42, 583–588. [Google Scholar] [CrossRef] [PubMed]
- Richardson, R.B.; Ainsbury, E.A.; Prescott, C.R.; Lovicu, F.J. Etiology of posterior subcapsular cataracts based on a review of risk factors including aging, diabetes, and ionizing radiation. Int. J. Radiat. Biol. 2020, 96, 1339–1361. [Google Scholar] [CrossRef]
- Srinivasan, M.; Ravindran, R.D.; O’Brien, K.S.; Kim, U.R.; Wilkins, J.H.; Whitcher, J.P.; Lietman, T.M.; Gritz, D.C.; Keenan, J.D. Antioxidant Vitamins for Cataracts: 15-Year Follow-up of a Randomized Trial. Ophthalmology 2020, 127, 986–987. [Google Scholar] [CrossRef]
- Delamere, N.A.; Tamiya, S. Lens ion transport: From basic concepts to regulation of Na,K-ATPase activity. Exp. Eye Res. 2009, 88, 140–143. [Google Scholar] [CrossRef] [Green Version]
- Tanwar, J.; Singh, J.B.; Motiani, R.K. Molecular machinery regulating mitochondrial calcium levels: The nuts and bolts of mitochondrial calcium dynamics. Mitochondrion 2021, 57, 9–22. [Google Scholar] [CrossRef] [PubMed]
- Brookes, P.; Yoon, Y.; Robotham, J.L.; Anders, M.W.; Sheu, S.-S. Calcium, ATP, and ROS: A mitochondrial love-hate triangle. Am. J. Physiol. Physiol. 2004, 287, C817–C833. [Google Scholar] [CrossRef]
- Tham, Y.-C.; Li, X.; Wong, T.Y.; Quigley, H.A.; Aung, T.; Cheng, C.-Y. Global Prevalence of Glaucoma and Projections of Glaucoma Burden through 2040. Ophthalmology 2014, 121, 2081–2090. [Google Scholar] [CrossRef]
- Allison, K.; Patel, D.G.; Greene, L. Racial and Ethnic Disparities in Primary Open-Angle Glaucoma Clinical Trials. JAMA Netw. Open 2021, 4, e218348. [Google Scholar] [CrossRef]
- Vajaranant, T.S.; Wu, S.; Torres, M.; Varma, R. The Changing Face of Primary Open-Angle Glaucoma in the United States: Demographic and Geographic Changes from 2011 to 2050. Am. J. Ophthalmol. 2012, 154, 303–314.e3. [Google Scholar] [CrossRef] [Green Version]
- Saccà, S.C.; Gandolfi, S.; Bagnis, A.; Manni, G.; Damonte, G.; Traverso, C.E.; Izzotti, A. From DNA damage to functional changes of the trabecular meshwork in aging and glaucoma. Ageing Res. Rev. 2016, 29, 26–41. [Google Scholar] [CrossRef] [PubMed]
- Recommendation: Primary Open-Angle Glaucoma: Screening|United States Preventive Services Taskforce. Available online: https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/primary-open-angle-glaucoma-screening (accessed on 18 November 2022).
- Lawler, T.; Liu, Y.; Christensen, K.; Vajaranant, T.S.; Mares, J. Dietary Antioxidants, Macular Pigment, and Glaucomatous Neurodegeneration: A Review of the Evidence. Nutrients 2019, 11, 1002. [Google Scholar] [CrossRef] [Green Version]
- Bourdel-Marchasson, I.; Delmas-Beauvieux, M.; Peuchant, E.; Richard-Harston, S.; Decamps, A.; Reignier, B.; Emeriau, J.; Rainfray, M. Antioxidant defences and oxidative stress markers in erythrocytes and plasma from normally nourished elderly Alzheimer patients. Age Ageing 2001, 30, 235–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goyal, A.; Srivastava, A.; Sihota, R.; Kaur, J. Evaluation of Oxidative Stress Markers in Aqueous Humor of Primary Open Angle Glaucoma and Primary Angle Closure Glaucoma Patients. Curr. Eye Res. 2014, 39, 823–829. [Google Scholar] [CrossRef]
- Ghanem, A.A.; Arafa, L.F.; El-Baz, A. Oxidative Stress Markers in Patients with Primary Open-Angle Glaucoma. Curr. Eye Res. 2010, 35, 295–301. [Google Scholar] [CrossRef]
- Cáceres-Vélez, P.R.; Hui, F.; Hercus, J.; Bui, B.; Jusuf, P.R. Restoring the oxidative balance in age-related diseases—An approach in glaucoma. Ageing Res. Rev. 2022, 75, 101572. [Google Scholar] [CrossRef]
- Sorkhabi, R.; Ghorbanihaghjo, A.; Javadzadeh, A.; Rashtchizadeh, N.; Moharrery, M. Oxidative DNA damage and total antioxidant status in glaucoma patients. Mol. Vis. 2011, 17, 41–46. [Google Scholar] [PubMed]
- Nucci, C.; Di Pierro, D.; Varesi, C.; Ciuffoletti, E.; Russo, R.; Gentile, R.; Cedrone, C.; Duran, M.D.P.; Coletta, M.; Mancino, R. Increased malondialdehyde concentration and reduced total antioxidant capacity in aqueous humor and blood samples from patients with glaucoma. Mol. Vis. 2013, 19, 1841–1846. [Google Scholar] [PubMed]
- Pinazo-Durán, M.D.; Zanón-Moreno, V.; Gallego-Pinazo, R.; García-Medina, J.J. Oxidative stress and mitochondrial failure in the pathogenesis of glaucoma neurodegeneration. Prog. Brain Res. 2015, 220, 127–153. [Google Scholar] [CrossRef] [PubMed]
- Bailey, J.N.C.; Loomis, S.J.; Kang, J.H.; Allingham, R.R.; Gharahkhani, P.; Khor, C.C.; Burdon, K.P.; Aschard, H.; Chasman, D.I.; et al.; ANZRAG Consortium Genome-wide association analysis identifies TXNRD2, ATXN2 and FOXC1 as susceptibility loci for primary open-angle glaucoma. Nat. Genet. 2016, 48, 189–194. [Google Scholar] [CrossRef] [Green Version]
- Luo, J.; Mills, K.; le Cessie, S.; Noordam, R.; van Heemst, D. Ageing, age-related diseases and oxidative stress: What to do next? Ageing Res. Rev. 2019, 57, 100982. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Pan, X.; Zhao, X.; Luo, J.; Xu, M.; Bai, D.; Hu, Y.; Liu, X.; Yu, Q.; Gao, D. Autophagy and Age-Related Eye Diseases. BioMed Res. Int. 2019, 2019, 5763658. [Google Scholar] [CrossRef]
- Chaudhry, S.; Dunn, H.; Carnt, N.; White, A. Nutritional supplementation in the prevention and treatment of glaucoma. Surv. Ophthalmol. 2021, 67, 1081–1098. [Google Scholar] [CrossRef]
- Klein, R.; Chou, C.-F.; Klein, B.E.K.; Zhang, X.; Meuer, S.M.; Saaddine, J.B. Prevalence of Age-Related Macular Degeneration in the US Population. Arch. Ophthalmol. 2011, 129, 75–80. [Google Scholar] [CrossRef] [Green Version]
- Wong, W.L.; Su, X.; Li, X.; Cheung, C.M.G.; Klein, R.; Cheng, C.Y.; Wong, T.Y. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: A systematic review and meta-analysis. Lancet Glob. Health 2014, 2, e106–e116. [Google Scholar] [CrossRef] [Green Version]
- Stahl, A. The Diagnosis and Treatment of Age-Related Macular Degeneration. Dtsch. Ärzteblatt Int. 2020, 117, 513–520. [Google Scholar] [CrossRef]
- Armento, A.; Ueffing, M.; Clark, S.J. The complement system in age-related macular degeneration. Cell. Mol. Life Sci. 2021, 78, 4487–4505. [Google Scholar] [CrossRef]
- van Lookeren Campagne, M.; LeCouter, J.; Yaspan, B.L.; Ye, W. Mechanisms of age-related macular degeneration and therapeutic opportunities. J. Pathol. 2014, 232, 151–164. [Google Scholar] [CrossRef]
- Mitchell, P.; Liew, G.; Gopinath, B.; Wong, T.Y. Age-related macular degeneration. Lancet 2018, 392, 1147–1159. [Google Scholar] [CrossRef] [PubMed]
- Karunadharma, P.P.; Kapphahn, R.J.; Stahl, M.R.; Olsen, T.W.; Ferrington, D.A. Dissecting Regulators of Aging and Age-Related Macular Degeneration in the Retinal Pigment Epithelium. Oxidative Med. Cell. Longev. 2022, 2022, 609787. [Google Scholar] [CrossRef] [PubMed]
- Beatty, S.; Koh, H.-H.; Phil, M.; Henson, D.; Boulton, M. The Role of Oxidative Stress in the Pathogenesis of Age-Related Macular Degeneration. Surv. Ophthalmol. 2000, 45, 115–134. [Google Scholar] [CrossRef] [Green Version]
- Tate, D.J.; Miceli, M.V.; A Newsome, D. Phagocytosis and H2O2 induce catalase and metallothionein gene expression in human retinal pigment epithelial cells. Investig. Opthalmol. Vis. Sci. 1995, 36, 1271–1279. [Google Scholar]
- Delmelle, M. Retinal sensitized photodynamic damage to liposomes. Photochem. Photobiol. 1978, 28, 357–360. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Aal, E.-S.M.; Akhtar, H.; Zaheer, K.; Ali, R. Dietary Sources of Lutein and Zeaxanthin Carotenoids and Their Role in Eye Health. Nutrients 2013, 5, 1169–1185. [Google Scholar] [CrossRef] [Green Version]
- Chew, E.Y.; Clemons, T.E.; Agrón, E.; Domalpally, A.; Keenan, T.D.L.; Vitale, S.; Weber, C.; Smith, D.C.; Christen, W.; et al.; AREDS2 Research Group Long-term Outcomes of Adding Lutein/Zeaxanthin and ω-3 Fatty Acids to the AREDS Supplements on Age-Related Macular Degeneration Progression: AREDS2 Report 28. JAMA Ophthalmol 2022, 140, 692. [Google Scholar] [CrossRef]
- Feng, L.; Nie, K.; Jiang, H.; Fan, W. Effects of lutein supplementation in age-related macular degeneration. PLoS ONE 2019, 14, e0227048. [Google Scholar] [CrossRef] [Green Version]
- García-Layana, A.; Recalde, S.; Hernandez, M.; Abraldes, M.; Nascimento, J.; Hernández-Galilea, E.; Olmedilla-Alonso, B.; Escobar-Barranco, J.; Zapata, M.; Silva, R.; et al. A Randomized Study of Nutritional Supplementation in Patients with Unilateral Wet Age-Related Macular Degeneration. Nutrients 2021, 13, 1253. [Google Scholar] [CrossRef]
- Parravano, M.; Tedeschi, M.; Manca, D.; Costanzo, E.; Di Renzo, A.; Giorno, P.; Barbano, L.; Ziccardi, L.; Varano, M.; Parisi, V. Effects of Macuprev® Supplementation in Age-Related Macular Degeneration: A Double-Blind Randomized Morpho-Functional Study Along 6 Months of Follow-Up. Adv. Ther. 2019, 36, 2493–2505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGwin, G.; Kar, D.; Berlin, A.; Clark, M.E.; Swain, T.A.; Crosson, J.N.; Sloan, K.R.; Owsley, C.; Curcio, C.A. Macular and Plasma Xanthophylls Are Higher in Age-related Macular Degeneration than in Normal Aging: Alabama Study on Early Age-related Macular Degeneration 2 Baseline. Ophthalmol. Sci. 2022, 3, 100263. [Google Scholar] [CrossRef] [PubMed]
- Jarrett, S.G.; Boulton, M.E. Consequences of oxidative stress in age-related macular degeneration. Mol. Asp. Med. 2012, 33, 399–417. [Google Scholar] [CrossRef] [Green Version]
- Wang, A.L.; Lukas, T.J.; Yuan, M.; Neufeld, A.H. Increased mitochondrial DNA damage and down-regulation of DNA repair enzymes in aged rodent retinal pigment epithelium and choroid. Mol. Vis. 2008, 14, 644–651. [Google Scholar] [PubMed]
- Gu, X.; Meer, S.G.; Miyagi, M.; Rayborn, M.E.; Hollyfield, J.G.; Crabb, J.W.; Salomon, R. Carboxyethylpyrrole Protein Adducts and Autoantibodies, Biomarkers for Age-related Macular Degeneration. J. Biol. Chem. 2003, 278, 42027–42035. [Google Scholar] [CrossRef] [Green Version]
- Justilien, V.; Pang, J.-J.; Renganathan, K.; Zhan, X.; Crabb, J.W.; Kim, S.R.; Sparrow, J.R.; Hauswirth, W.W.; Lewin, A.S. SOD2 Knockdown Mouse Model of Early AMD. Investig. Opthalmol. Vis. Sci. 2007, 48, 4407–4420. [Google Scholar] [CrossRef] [Green Version]
- Imamura, Y.; Noda, S.; Hashizume, K.; Shinoda, K.; Yamaguchi, M.; Uchiyama, S.; Shimizu, T.; Mizushima, Y.; Shirasawa, T.; Tsubota, K. Drusen, choroidal neovascularization, and retinal pigment epithelium dysfunction in SOD1-deficient mice: A model of age-related macular degeneration. Proc. Natl. Acad. Sci. USA 2006, 103, 11282–11287. [Google Scholar] [CrossRef] [Green Version]
- Tisi, A.; Feligioni, M.; Passacantando, M.; Ciancaglini, M.; Maccarone, R. The Impact of Oxidative Stress on Blood-Retinal Barrier Physiology in Age-Related Macular Degeneration. Cells 2021, 10, 64. [Google Scholar] [CrossRef]
- Wang, H.; Han, X.; Wittchen, E.S.; Hartnett, M.E. TNF-α mediates choroidal neovascularization by upregulating VEGF expression in RPE through ROS-dependent β-catenin activation. Mol. Vis. 2016, 22, 116–128. Available online: https://pmc/articles/PMC4736754/ (accessed on 11 February 2023).
- Heesterbeek, T.J.; Lechanteur, Y.T.E.; Lorés-Motta, L.; Schick, T.; Daha, M.R.; Altay, L.; Liakopoulos, S.; Smailhodzic, D.; Hollander, A.I.D.; Hoyng, C.B.; et al. Complement Activation Levels Are Related to Disease Stage in AMD. Investig. Opthalmol. Vis. Sci. 2020, 61, 18. [Google Scholar] [CrossRef] [Green Version]
- McLeod, D.S.; Bhutto, I.; Edwards, M.M.; Gedam, M.; Baldeosingh, R.; Lutty, G.A. Mast Cell-Derived Tryptase in Geographic Atrophy. Investig. Opthalmol. Vis. Sci. 2017, 58, 5887–5896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- A Bhutto, I.; McLeod, D.S.; Jing, T.; Sunness, J.S.; Seddon, J.M.; A Lutty, G. Increased choroidal mast cells and their degranulation in age-related macular degeneration. Br. J. Ophthalmol. 2016, 100, 720–726. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease | 2010 | 2030 | 2050 |
|---|---|---|---|
| Cataracts | 24,409,978 | 38,737,561 | 50,231,932 |
| Glaucoma | 2,719,379 | 4,284,823 | 6,290,760 |
| Age-Related Macular Degeneration | 2,069,403 | 3,664,044 | 5,442,265 |
| Anatomical Feature | Age-Related Changes |
|---|---|
| Eyelids and Lacrimal Glands | Horizontal lid laxity |
| Ectropion | |
| Entropion | |
| Dermatochalasis | |
| Blepharoptosis | |
| Gland atrophy and fibrosis | |
| Sclera | Increase in stiffness and rigidity |
| Senile scleral plaques | |
| Cornea | Thickening of the Descemet’s and epithelial basement membranes |
| Decrease in corneal stromal density | |
| Decrease in corneal endothelial cell (Fuchs’ dystrophy) and conjunctival keratocyte numbers | |
| Shift from with-the-rule astigmatism to against-the-rule astigmatism | |
| Arcus senilis | |
| Cornea farinata | |
| Crocodile shagreen | |
| Phagocytic dysfunction and loss of phagocytically active cells | |
| Trabecular Meshwork | Reduction in height |
| Decrease in cellularity | |
| Increase in extracellular components | |
| Hyperpigmentation | |
| Ciliary Body | Shortening and widening of the muscle |
| Decrease in diameter | |
| Loss of vascularization and cellularity | |
| Crystalline Lens | Increase in radii of curvature, lens volume, surface area, cross-sectional area, diameter, lens thickness, and weight |
| Blue blindness | |
| Cataract formation | |
| Presbyopia secondary to increased stiffness |
| Anatomical Feature | Age-Related Changes |
|---|---|
| Vitreous Humor | Aggregation of collagenous fibrils |
| Thickening of the vitreous base | |
| Increased stiffness, dehydration, and mobility | |
| Retina and Retinal Pigment Epithelium | Neuronal cell loss |
| Diminished total retinal blood vessel area | |
| Decrease in the number of pericytes and endothelial cells | |
| Retinal pigment epithelium cell vacuolization and loss of cytoplasm | |
| Accumulation of lipofuscin | |
| Impaired melanin antioxidant properties | |
| Choroid | Lower mean thickness, vessel volume, and stroma volume |
| Diminished choriocapillaris density and diameter | |
| Loss of melanosomes within choroidal melanocytes | |
| Macula and Fovea | Increase in macular retinal pigment epithelium cell height |
| Thickening and calcification of Bruch’s membrane | |
| Drusen deposition | |
| Decline in macular vascular flow | |
| Optic Nerve | Reduction in nerve fiber density |
| Lower neural rim volume and minimum rim width | |
| Decreased perfusion of optic nerve head |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goodman, D.; Ness, S. The Role of Oxidative Stress in the Aging Eye. Life 2023, 13, 837. https://doi.org/10.3390/life13030837
Goodman D, Ness S. The Role of Oxidative Stress in the Aging Eye. Life. 2023; 13(3):837. https://doi.org/10.3390/life13030837
Chicago/Turabian StyleGoodman, Deniz, and Steven Ness. 2023. "The Role of Oxidative Stress in the Aging Eye" Life 13, no. 3: 837. https://doi.org/10.3390/life13030837
APA StyleGoodman, D., & Ness, S. (2023). The Role of Oxidative Stress in the Aging Eye. Life, 13(3), 837. https://doi.org/10.3390/life13030837