

Effects of Motor Rehabilitation on Balance and Functional Activities in Elderly Patients with Peripheral Neuropathy and Recurrent Falls

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Assessments
2.3. Outcome Measures
2.4. Rehabilitation Program
2.5. Statistical Analysis
3. Results
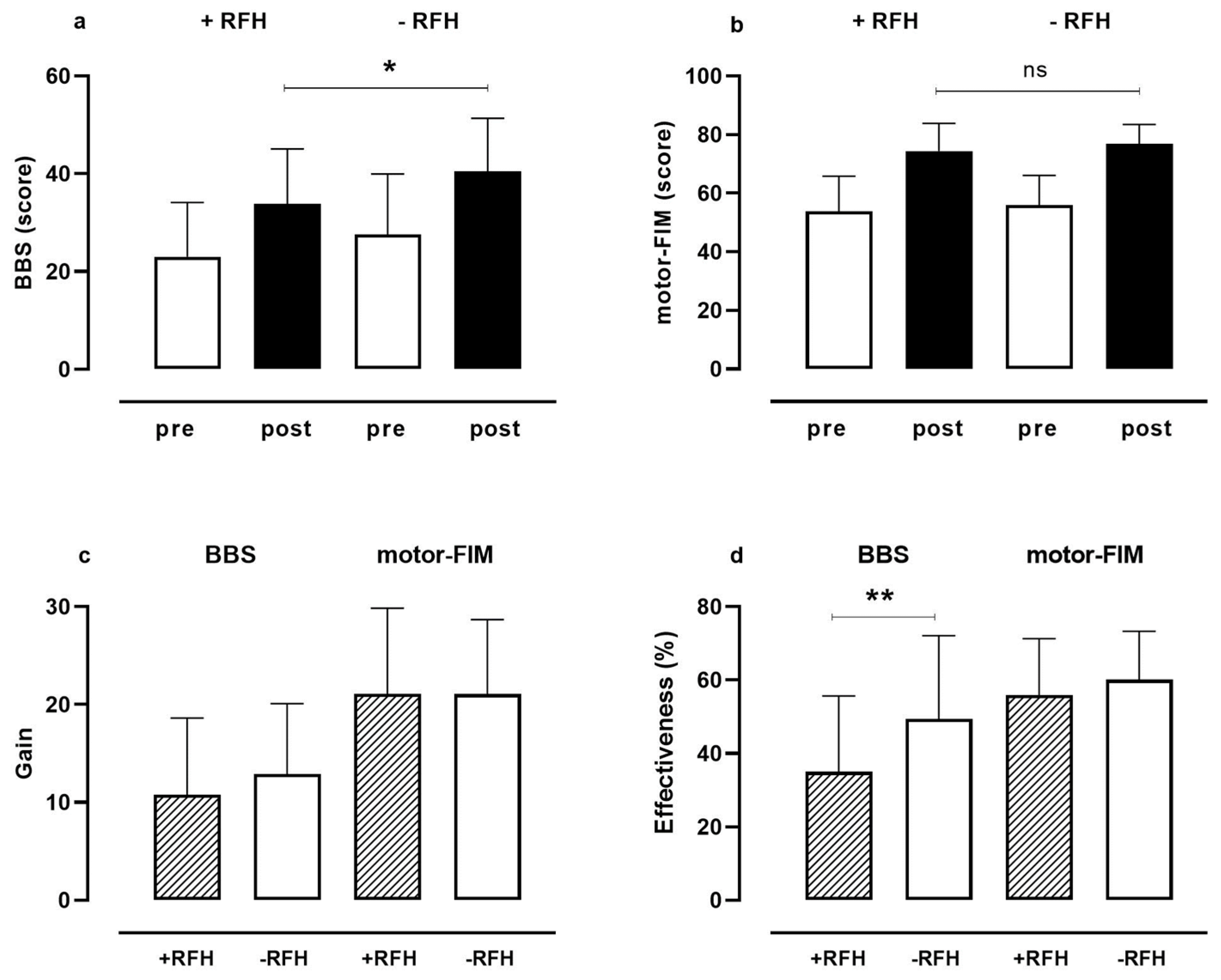
3.1. Total Berg Balance Scale and Motor FIM
3.2. Single Items of Berg Balance Scale
3.3. Single Items of Motor FIM
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- DeMott, T.K.; Richardson, J.K.; Thies, S.B.; Ashton-Miller, J.A. Falls and gait characteristics among older persons with peripheral neuropathy. Am. J. Phys. Med. Rehabil. 2007, 86, 125–132. [Google Scholar] [CrossRef]
- Hanewinckel, R.; Ikram, M.A.; Van Doorn, P.A. Peripheral neuropathies. In Handbook of Clinical Neurology; Aminoff, M.J., Boller, F., Swaab, D.F., Eds.; Elsevier: Amsterdam, The Netherlands, 2016; Volume 138, pp. 263–282. [Google Scholar]
- Singh, R.; Kishore, L.; Kaur, N. Diabetic peripheral neuropathy: Current perspective and future directions. Pharmacol. Res. 2014, 80, 21–35. [Google Scholar] [CrossRef] [PubMed]
- Watson, J.C.; Dyck, P.J. Peripheral Neuropathy: A Practical Approach to Diagnosis and Symptom Management. Mayo Clin. Proc. 2015, 90, 940–951. [Google Scholar] [CrossRef] [PubMed]
- Allet, L.; Armand, S.; de Bie, R.A.; Golay, A.; Monnin, D.; Aminian, K.; Staal, J.B.; de Bruin, E.D. The gait and balance of patients with diabetes can be improved: A randomised controlled trial. Diabetologia 2010, 53, 458–466. [Google Scholar] [CrossRef]
- Hanewinckel, R.; Drenthen, J.; Verlinden, V.J.A.; Darweesh, S.K.L.; van der Geest, J.N.; Hofman, A.; van Doorn, P.A.; Ikram, M.A. Polyneuropathy relates to impairment in daily activities, worse gait, and fall-related injuries. Neurology 2017, 89, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Xi Pan, X.; Bai, J. Balance training in the intervention of fall risk in elderly with diabetic peripheral neuropathy: A review. Int. J. Nurs. Sci. 2014, 1, 441–445. [Google Scholar]
- Chapman, A.; Meyer, C.; Renehan, E.; Hill, K.D.; Browning, C.J. Exercise interventions for the improvement of falls-related outcomes among older adults with diabetes mellitus: A systematic review and meta-analyses. J. Diabetes Complicat. 2017, 31, 631–645. [Google Scholar] [CrossRef] [PubMed]
- Riandini, T.; Khoo, E.Y.H.; Tai, B.C.; Tavintharan, S.; Phua, M.S.L.A.; Chandran, K.; Hwang, S.W.; Venkataraman, K. Fall Risk and Balance Confidence in Patients with Diabetic Peripheral Neuropathy: An Observational Study. Front. Endocrinol. 2020, 11, 573804. [Google Scholar] [CrossRef] [PubMed]
- Khan, K.S.; Pop-Busui, R.; Devantier, L.; Kristensen, A.G.; Tankisi, H.; Dalgas, U.; Overgaard, K.; Andersen, H. Falls in individuals with type 2 diabetes; a cross-sectional study on the impact of motor dysfunction, postural instability and diabetic polyneuropathy. Diabet. Med. 2021, 38, e14470. [Google Scholar] [CrossRef]
- Grewal, G.S.; Sayeed, R.; Schwenk, M.; Bharara, M.; Menzies, R.; Talal, T.K.; Armstrong, D.G.; Najafi, B. Balance rehabilitation: Promoting the role of virtual reality in patients with diabetic peripheral neuropathy. J. Am. Podiatr. Med. Assoc. 2013, 103, 498–507. [Google Scholar] [CrossRef]
- Riva, N.; Faccendini, S.; Lopez, I.D.; Fratelli, A.; Velardo, D.; Quattrini, A.; Gatti, R.; Comi, G.; Comola, M.; Fazio, R. Balance exercise in patients with chronic sensory ataxic neuropathy: A pilot study. J. Peripher. Nerv. Syst. 2014, 19, 145–151. [Google Scholar] [CrossRef]
- Venkataraman, K.; Tai, B.C.; Khoo, E.Y.H.; Tavintharan, S.; Chandran, K.; Hwang, S.W.; Phua, M.S.L.A.; Wee, H.L.; Koh, G.C.H.; Tai, E.S. Short-term strength and balance training does not improve quality of life but improves functional status in individuals with diabetic peripheral neuropathy: A randomised controlled trial. Diabetologia 2019, 62, 2200–2210. [Google Scholar] [CrossRef]
- Chung, T.; Prasad, K.; Lloyd, T.E. Peripheral neuropathy: Clinical and electrophysiological considerations. Neuroimaging Clin. N. Am. 2014, 24, 49–65. [Google Scholar] [CrossRef]
- Arevalo-Rodriguez, I.; Smailagic, N.; Roqué-Figuls, M.; Ciapponi, A.; Sanchez-Perez, E.; Giannakou, A.; Pedraza, O.L.; Bonfill Cosp, X.; Cullum, S. Mini-Mental State Examination (MMSE) for the early detection of dementia in people with mild cognitive impairment (MCI). Cochrane Database Syst. Rev. 2021, 7, CD010783. [Google Scholar] [PubMed]
- Salvi, F.; Miller, M.D.; Grilli, A.; Giorgi, R.; Towers, A.L.; Morichi, V.; Spazzafumo, L.; Mancinelli, L.; Espinosa, E.; Rappelli, A.; et al. A manual of guidelines to score the modified cumulative illness rating scale and its validation in acute hospitalized elderly patients. J. Am. Geriatr. Soc. 2008, 56, 1926–1931. [Google Scholar] [CrossRef] [PubMed]
- Formiga, F.; Navarro, M.; Duaso, E.; Chivite, D.; Ruiz, D.; Perez-Castejon, J.M.; Lopez-Soto, A.; Pujol, R. Factors associated with hip fracture-related falls among patients with a history of recurrent falling. Bone 2008, 43, 941–944. [Google Scholar] [CrossRef]
- Berardi, A.; Galeoto, G.; Valente, D.; Conte, A.; Fabbrini, G.; Tofani, M. Validity and reliability of the 12-item Berg Balance Scale in an Italian population with Parkinson’s disease: A cross sectional study. Arq. Neuropsiquiatr. 2020, 78, 419–423. [Google Scholar] [CrossRef] [PubMed]
- Blum, L.; Korner-Bitensky, N. Usefulness of the Berg Balance Scale in stroke rehabilitation: A systematic review. Phys. Ther. 2008, 88, 559–566. [Google Scholar] [CrossRef]
- Maritz, R.; Tennant, A.; Fellinghauer, C.; Stucki, G.; Prodinger, B. The Functional Independence Measure 18-item version can be reported as a unidimensional interval-scaled metric: Internal construct validity revisited. J. Rehabil. Med. 2019, 51, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Güner, A.; Altan, L.; Kasapoğlu Aksoy, M. The effectiveness of the low-power laser and kinesiotaping in the treatment of carpal tunnel syndrome, a pilot study. Rheumatol. Int. 2018, 38, 895–904. [Google Scholar] [CrossRef]
- Hosseini, Z.S.; Peyrovi, H.; Gohari, M. The Effect of Early Passive Range of Motion Exercise on Motor Function of People with Stroke: A Randomized Controlled Trial. J. Caring Sci. 2019, 8, 39–44. [Google Scholar] [CrossRef]
- Norkin, C.C.; White, D. (Eds.) Measurement of Joint Motion: A Guide to Goniometry, 5th ed.; McGraw Hill: New York, NY, USA, 2016. [Google Scholar]
- Tan, A.K.; Taiju, R.; Menon, E.B.; Koh, G.C. Postoperated hip fracture rehabilitation effectiveness and efficiency in a community hospital. Ann. Acad. Med. Singap. 2014, 43, 209–215. [Google Scholar] [CrossRef]
- Peat, J.; Barton, B.; Elliot, E. Statistics Workbook for Evidence-Based Health Care; John Wiley & Sons: Hoboken, NJ, USA, 2009. [Google Scholar]
- Bokan-Mirković, V.; Škarić-Karanikić, Ž.; Nejkov, S.; Vuković, M.; Ćirović, D. Diabetic Polyneuropathy and Risk of Falls: Fear of Falling and Other Factors. Acta Clin. Croat. 2017, 56, 721–727. [Google Scholar] [CrossRef] [PubMed]
- Reeves, N.D.; Orlando, G.; Brown, S.J. Sensory-Motor Mechanisms Increasing Falls Risk in Diabetic Peripheral Neuropathy. Medicina 2021, 57, 457. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, A.; Melzer, I. Balance perturbation system to improve balance compensatory responses during walking in old persons. J. Neuroeng. Rehabil. 2010, 7, 32. [Google Scholar] [CrossRef] [PubMed]
- Mansfield, A.; Peters, A.L.; Liu, B.A.; Maki, B.E. Effect of a perturbation-based balance training program on compensatory stepping and grasping reactions in older adults: A randomized controlled trial. Phys. Ther. 2010, 90, 476–491. [Google Scholar] [CrossRef] [PubMed]
- Jáuregui-Renaud, K. Postural Balance and Peripheral Neuropathy. In Peripheral Neuropathy—A New Insight into the Mechanism, Evaluation and Management of a Complex Disorder; Souayah, N., Ed.; IntechOpen: London, UK, 2013. [Google Scholar]
- Allet, L.; Kim, H.; Ashton-Miller, J.; De Mott, T.; Richardson, J.K. Frontal plane hip and ankle sensorimotor function, not age, predicts unipedal stance time. Muscle Nerve 2012, 45, 578–585. [Google Scholar] [CrossRef]
- Ghanavati, T.; Shaterzadeh Yazdi, M.J.; Goharpey, S.; Arastoo, A.A. Functional balance in elderly with diabetic neuropathy. Diabetes Res. Clin. Pract. 2012, 96, 24–28. [Google Scholar] [CrossRef]
- Prata, M.G.; Scheicher, M.E. Correlation between balance and the level of functional independence among elderly people. Sao Paulo Med. J. 2012, 130, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Vincent-Onabajo, G.; Joseph, E.; Musa, H.Y. Impact of balance on functional independence after stroke: A cross-sectional study at rehabilitation settings in Nigeria. NeuroRehabilitation 2018, 42, 499–504. [Google Scholar] [CrossRef]
- Hewston, P.; Deshpande, N. Falls and Balance Impairments in Older Adults with Type 2 Diabetes: Thinking Beyond Diabetic Peripheral Neuropathy. Can. J. Diabetes 2016, 40, 6–9. [Google Scholar] [CrossRef] [PubMed]
- Ites, K.I.; Anderson, E.J.; Cahill, M.L.; Kearney, J.A.; Post, E.C.; Gilchrist, L.S. Balance interventions for diabetic peripheral neuropathy: A systematic review. J. Geriatr. Phys. Ther. 2011, 34, 109–116. [Google Scholar] [CrossRef]
- Khan, K.S.; Andersen, H. The Impact of Diabetic Neuropathy on Activities of Daily Living, Postural Balance and Risk of Falls—A Systematic Review. J. Diabetes Sci. Technol. 2022, 16, 289–294. [Google Scholar] [CrossRef]
- Gialanella, B.; Prometti, P.; Comini, L.; Monguzzi, V.; Santoro, R. Predictive factors of functional abilities in older patients with peripheral neuropathy. Aging Clin. Exp. Res. 2022, 34, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Zurales, K.; DeMott, T.K.; Kim, H.; Allet, L.; Ashton-Miller, J.A.; Richardson, J.K. Gait Efficiency on an Uneven Surface Is Associated with Falls and Injury in Older Subjects with a Spectrum of Lower Limb Neuromuscular Function: A Prospective Study. Am. J. Phys. Med. Rehabil. 2016, 95, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Macgilchrist, C.; Paul, L.; Ellis, B.M.; Howe, T.E.; Kennon, B.; Godwin, J. Lower-limb risk factors for falls in people with diabetes mellitus. Diabet. Med. 2010, 27, 162–168. [Google Scholar] [CrossRef]
- Richardson, J.K. Factors associated with falls in older patients with diffuse polyneuropathy. J. Am. Geriatr. Soc. 2002, 50, 1767–1773. [Google Scholar] [CrossRef]
- Muir, S.W.; Berg, K.; Chesworth, B.; Speechley, M. Use of the Berg Balance Scale for predicting multiple falls in community-dwelling elderly people: A prospective study. Phys. Ther. 2008, 88, 449–459. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| PN with Recurrent Falls (n = 35) | PN without Recurrent Falls (n = 29) | p-Value | |
|---|---|---|---|
| Age, years | 83.22 ± 4.29 | 81.06 ± 5.63 | 0.072 |
| Male/Female, n | 11/24 | 13/16 | 0.485 |
| Diabetes mellitus: Yes/No | 14/21 | 15/14 | 0.540 |
| CIRS severity score | 2.56 ± 0.32 | 3.05 ± 3.57 | 0.419 |
| Body Mass Index, Kg/m2 | 28.61 ± 6.70 | 27.52 ± 6.21 | 0.504 |
| EMG: demyelinating neuropathy, axonal neuropathies (sensitive and motor ones), axonal demyelinating neuropathy | 4/20/11 | 2/20/7 | 0.730 |
| MMSE * | 21.70 ± 4.81 | 22.17 ± 5.44 | 0.772 |
| PN with Recurrent Falls (n = 35) | PN without Recurrent Falls (n = 29) | p-Value | |
|---|---|---|---|
| At admission | |||
| VNS pain, score | 6.42 ± 1.83 | 6.41 ± 2.48 | 0.978 |
| ROM, ° | 455.00 ± 46.57 | 456.51 ± 51.15 | 0.901 |
| Muscle strength, score | 12.77 ± 1.84 | 13.15 ± 1.49 | 0.371 |
| Cognitive-FIM, score | 26.31 ± 3.67 | 27.37 ± 3.44 | 0.239 |
| At discharge | |||
| VNS pain, score | 3.71 ± 1.60 | 3.31 ± 1.77 | 0.342 |
| ROM, ° | 455.71 ± 77.45 | 477.58 ± 29.29 | 0.155 |
| Muscle strength, score | 14.71 ± 1.63 | 14.86 ± 1.15 | 0.684 |
| Cognitive-FIM, score | 26.77 ± 3.87 | 28.10 ± 3.72 | 0.168 |
| Length of hospital stay, days | 35.37 ± 12.64 | 34.96 ± 9.79 | 0.888 |
| Diabetes and Falls (n = 14) | No Diabetes and No Falls (n = 14) | p-Value | |
|---|---|---|---|
| At admission | |||
| Age, years | 81.57 ± 5.10 | 80.28 ± 5.29 | 0.519 |
| Male/Female, n | 8/6 | 6/8 | 0.449 |
| Body Mass Index, Kg/m2 | 29.74 ± 8.58 | 25.66 ± 5.01 | 0.136 |
| CIRS, score | 2.59 ± 0.28 | 3.66 ± 5.14 | 0.444 |
| MMSE *, score | 20.17 ± 4.69 | 20.71 ± 6.13 | 0.826 |
| VNS pain, score | 6.00 ± 2.11 | 6.78 ± 2.39 | 0.365 |
| ROM, ° | 455.71 ± 39.46 | 448.50 ± 65.17 | 0.725 |
| Muscle strength, score | 12.28 ± 1.54 | 13.32 ± 1.74 | 0.108 |
| Cognitive-FIM, score | 25.21 ± 3.26 | 28.42 ± 2.82 | 0.009 |
| Berg Balance Scale, score | 19.71 ± 11.03 | 29.64 ± 12.04 | 0.031 |
| Motor-FIM, score | 49.21 ± 13.82 | 56.85 ± 10.53 | 0.111 |
| At discharge | |||
| VNS pain, score | 3.78 ± 1.96 | 3.50 ± 1.78 | 0.690 |
| ROM, ° | 470.71 ± 24.09 | 483.57 ± 25.82 | 0.162 |
| Muscle strength, score | 14.14 ± 1.87 | 15.07 ± 1.26 | 0.136 |
| Cognitive-FIM, score | 25.07 ± 3.17 | 29.21 ± 2.75 | 0.001 |
| Berg Balance Scale, score | 31.00 ± 12.47 | 42.57 ± 9.97 | 0.011 |
| Effectiveness in Berg Balance Scale, % | 32.70 ± 22.80 | 52.89 ± 21.80 | 0.024 |
| Gain in Berg Balance Scale, score | 11.28 ± 9.10 | 12.92 ± 7.62 | 0.608 |
| Motor-FIM, score | 69.78 ± 12.96 | 78.14 ± 4.52 | 0.031 |
| Effectiveness in motor-FIM, % | 50.12 ± 21.27 | 60.78 ± 11.71 | 0.112 |
| Gain in motor-FIM, score | 20.42 ± 10.74 | 22.07 ± 9.19 | 0.667 |
| BBS | |||
|---|---|---|---|
| Score at Admission | Score at Discharge | Effectiveness | |
| Age, years | −0.23 | −0.28 * | −0.33 ** |
| Cognitive-FIM score at admission | 0.25 * | 0.31 * | 0.32 * |
| Cognitive-FIM score at discharge | 0.24 | 0.35 ** | 0.36 ** |
| Motor FIM | |||
|---|---|---|---|
| Score at Admission | Score at Discharge | Effectiveness | |
| Age, years | −0.13 | −0.29 * | −0.36 ** |
| Muscle strength, score at admission | 0.46 ** | 0.23 | −0.08 |
| Muscle strength, score at discharge | 0.32 * | 0.23 | 0.04 |
| Cognitive-FIM score at admission | 0.06 | 0.30 * | 0.35 ** |
| Cognitive-FIM score at discharge | 0.09 | 0.35 ** | 0.41 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gialanella, B.; Comini, L.; Prometti, P.; Vanoglio, F.; Santoro, R. Effects of Motor Rehabilitation on Balance and Functional Activities in Elderly Patients with Peripheral Neuropathy and Recurrent Falls. Life 2023, 13, 1059. https://doi.org/10.3390/life13041059
Gialanella B, Comini L, Prometti P, Vanoglio F, Santoro R. Effects of Motor Rehabilitation on Balance and Functional Activities in Elderly Patients with Peripheral Neuropathy and Recurrent Falls. Life. 2023; 13(4):1059. https://doi.org/10.3390/life13041059
Chicago/Turabian StyleGialanella, Bernardo, Laura Comini, Paola Prometti, Fabio Vanoglio, and Raffaele Santoro. 2023. "Effects of Motor Rehabilitation on Balance and Functional Activities in Elderly Patients with Peripheral Neuropathy and Recurrent Falls" Life 13, no. 4: 1059. https://doi.org/10.3390/life13041059
APA StyleGialanella, B., Comini, L., Prometti, P., Vanoglio, F., & Santoro, R. (2023). Effects of Motor Rehabilitation on Balance and Functional Activities in Elderly Patients with Peripheral Neuropathy and Recurrent Falls. Life, 13(4), 1059. https://doi.org/10.3390/life13041059