

Effects of Neuromuscular Training on Physical Performance in Older People: A Systematic Review

 ,
,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Information and Database Search Process
2.4. Studies Selection and Data Collection Process
2.5. Methodological Quality Assessment and Risk of Bias
2.6. Data Synthesis
3. Results
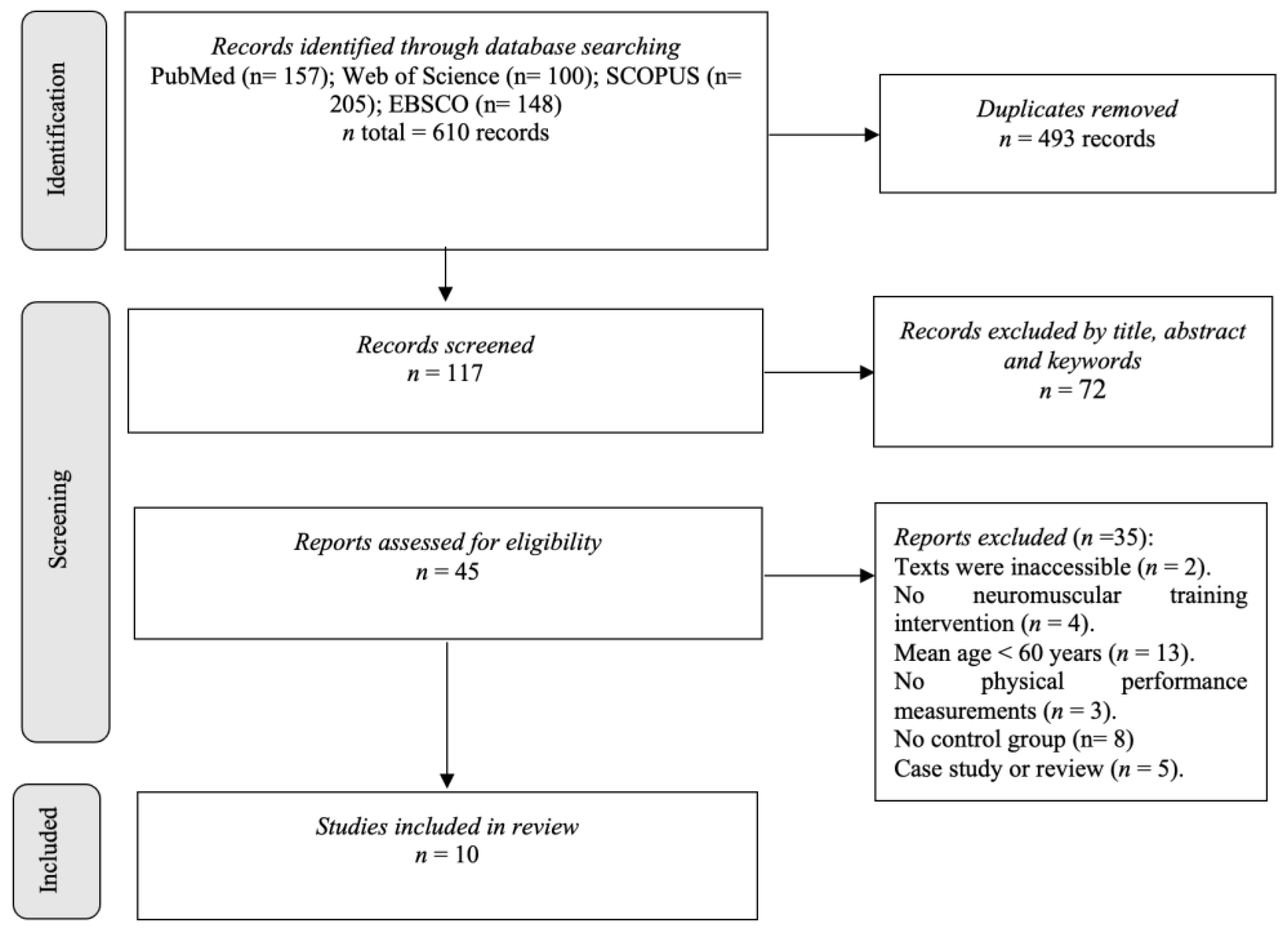
3.1. Studies Selection
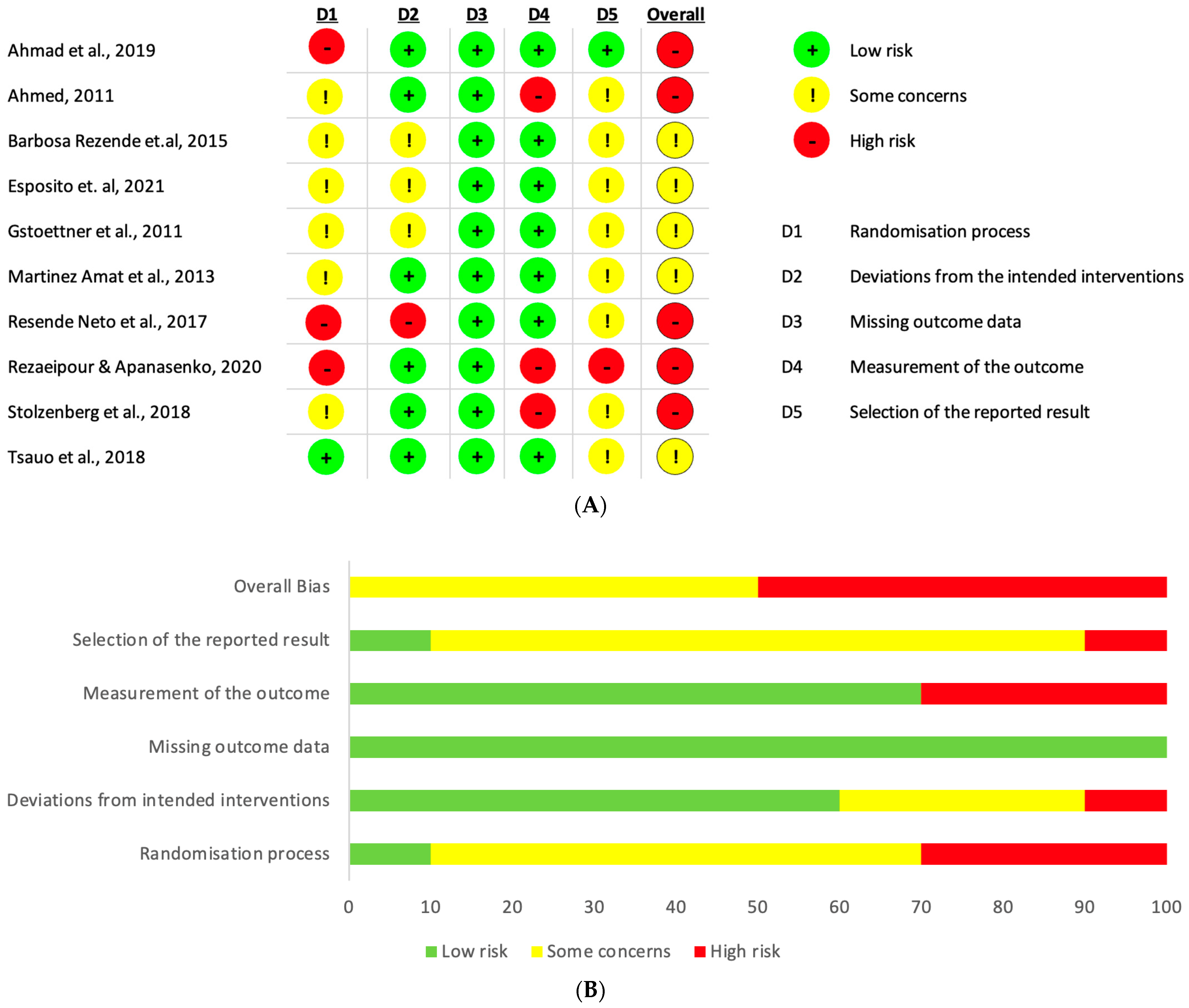
3.2. Risk of Bias
3.3. Studies Characteristics
3.4. Sample Characteristics
3.5. Physical Performance Outcomes and Collection Instruments
3.6. Interventions and Dosage
3.7. Main Outcomes
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Concha-Cisternas, Y.; Vargas-Vitoria, R.; Celis-Morales, C. Morphophysiological changes and fall risk in the older adult: A review of the literature. Rev. Salud Uninorte 2021, 36, 450–470. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 601. [Google Scholar] [CrossRef] [Green Version]
- Clark, B.C.; Manini, T.M. What is dynapenia? Nutrition 2012, 28, 495–503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anson, E.; Bigelow, R.T.; Swenor, B.; Deshpande, N.; Studenski, S.; Jeka, J.J.; Agrawal, Y. Loss of Peripheral Sensory Function Explains Much of the Increase in Postural Sway in Healthy Older Adults. Front. Aging Neurosci. 2017, 9, 202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le Mouel, C.; Tisserand, R.; Robert, T.; Brette, R. Postural adjustments in anticipation of predictable perturbations allow elderly fallers to achieve a balance recovery performance equivalent to elderly non-fallers. Gait Posture 2019, 71, 131–137. [Google Scholar] [CrossRef] [Green Version]
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical Activity, Exercise, and Physical Fitness: Definitions and Distinctions for Health-Related Research. Public Health Rep. 1985, 100, 126. [Google Scholar]
- Navarrete-Villanueva, D.; Gómez-Cabello, A.; Marín-Puyalto, J.; Moreno, L.A.; Vicente-Rodríguez, G.; Casajús, J.A. Frailty and Physical Fitness in Elderly People: A Systematic Review and Meta-analysis. Sport. Med. 2021, 51, 143–160. [Google Scholar] [CrossRef]
- Ortega, F.B.; Cadenas-Sanchez, C.; Lee, D.C.; Ruiz, J.R.; Blair, S.N.; Sui, X. Fitness and Fatness as Health Markers through the Lifespan: An Overview of Current Knowledge. Prog. Prev. Med. 2018, 3, e0013. [Google Scholar] [CrossRef]
- Milanović, Z.; Pantelić, S.; Trajković, N.; Sporiš, G.; Kostić, R.; James, N. Age-related decrease in physical activity and functional fitness among elderly men and women. Clin. Interv. Aging 2013, 8, 549–556, Corrigendum in Clin. Interv. Aging 2014, 9, 979–980. [Google Scholar] [CrossRef] [Green Version]
- Fragala, M.S.; Cadore, E.L.; Dorgo, S.; Izquierdo, M.; Kraemer, W.J.; Peterson, M.D.; Ryan, E.D. Resistance Training for Older Adults: Position Statement from the National Strength and Conditioning Association. J. Strength Cond. Res. 2019, 33, 2019–2052. [Google Scholar] [CrossRef]
- García-Hermoso, A.; Ramirez-Vélez, R.; Sáez de Asteasu, M.L.; Martínez-Velilla, N.; Zambom-Ferraresi, F.; Valenzuela, P.L.; Lucia, A.; Izquierdo, M. Safety and Effectiveness of Long-Term Exercise Interventions in Older Adults: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Sport. Med. 2020, 50, 1095–1106. [Google Scholar] [CrossRef]
- Lopez, P.; Pinto, R.S.; Radaelli, R.; Rech, A.; Grazioli, R.; Izquierdo, M.; Cadore, E.L. Benefits of resistance training in physically frail elderly: A systematic review. Aging Clin. Exp. Res. 2018, 30, 889–899. [Google Scholar] [CrossRef]
- Cadore, E.L.; Moneo, A.B.B.; Mensat, M.M.; Muñoz, A.R.; Casas-Herrero, A.; Rodriguez-Mañas, L.; Izquierdo, M. Positive effects of resistance training in frail elderly patients with dementia after long-term physical restraint. AGE 2014, 36, 801–811. [Google Scholar] [CrossRef]
- Concha-Cisternas, Y.F.; Guzman-Muñoz, E.E.; Marzuca-Nassr, G.N. Efectos de un programa de ejercicio físico combinado sobre la capacidad funcional de mujeres mayores sanas en Atención Primaria de Salud. Fisioterapia 2017, 39, 195–201. [Google Scholar] [CrossRef]
- Ribeiro, F.; Oliveira, J. Aging effects on joint proprioception: The role of physical activity in proprioception preservation. Eur. Rev. Aging Phys. Act. 2007, 4, 71–76. [Google Scholar] [CrossRef] [Green Version]
- Martins e Silva, D.C.; Bastos, V.H.; de Oliveira Sanchez, M.; Nunes, M.K.G.; Orsini, M.; Ribeiro, P.; Velasques, B.; Teixeira, S.S. Effects of vestibular rehabilitation in the elderly: A systematic review. Aging Clin. Exp. Res. 2016, 28, 599–606. [Google Scholar] [CrossRef]
- Silva-Moya, G.; Méndez-Rebolledo, G.; Valdes-Badilla, P.; Gómez-Álvarez, N.; Guzmán-Muñoz, E. Effects of neuromuscular training on psychomotor development and active joint position sense in school children. J. Mot. Behav. 2022, 54, 57–66. [Google Scholar] [CrossRef]
- 18. Espejo-Antúnez, L.; Pérez-Mármol, J.M.; Cardero-Durán, M.; de los, Á.; Toledo-Marhuenda, J.V.; Albornoz-Cabello, M. The Effect of Proprioceptive Exercises on Balance and Physical Function in Institutionalized Older Adults: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2020, 101, 1780–1788. [Google Scholar] [CrossRef]
- Risberg, M.A.; Mørk, M.; Jenssen, H.K.; Holm, I. Design and Implementation of a Neuromuscular Training Program Following Anterior Cruciate Ligament Reconstruction. J. Orthop. Sport. Phys. Ther. 2001, 31, 620–631. [Google Scholar] [CrossRef]
- Sazo-Rodríguez, S.; Méndez-Rebolledo, G.; Guzmán-Muñoz, E.; Rubio-Palma, P. The effects of progressive neuromuscular training on postural balance and functionality in elderly patients with knee osteoarthritis: A pilot study. J. Phys. Ther. Sci. 2017, 29, 1229–1235. [Google Scholar] [CrossRef] [Green Version]
- Knoop, J.; Steultjens, M.P.; van der Leeden, M.; van der Esch, M.; Thorstensson, C.A.; Roorda, L.D.; Lems, W.F.; Dekker, J. Proprioception in knee osteoarthritis: A narrative review. Osteoarthr. Cartil. 2011, 19, 381–388. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 88, n71. [Google Scholar] [CrossRef]
- Cardoso Ribeiro, C.; Gómez-Conesa, A.; Hidalgo Montesinos, M.D. Metodología para la adaptación de instrumentos de evaluación. Fisioterapia 2010, 32, 264–270. [Google Scholar] [CrossRef]
- Zhang, Y.; Zou, L.; Chen, S.-T.; Bae, J.H.; Kim, D.Y.; Liu, X.; Song, W. Effects and Moderators of Exercise on Sarcopenic Components in Sarcopenic Elderly: A Systematic Review and Meta-Analysis. Front. Med. 2021, 8, 649748. [Google Scholar] [CrossRef]
- Jørgensen, L.; Paludan-Müller, A.S.; Laursen, D.R.T.; Savović, J.; Boutron, I.; Sterne, J.A.C.; Higgins, J.P.T.; Hróbjartsson, A. Evaluation of the Cochrane tool for assessing risk of bias in randomized clinical trials: Overview of published comments and analysis of user practice in Cochrane and non-Cochrane reviews. Syst. Rev. 2016, 5, 80. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, I.; Noohu, M.M.; Verma, S.; Singla, D.; Hussain, M.E. Effect of sensorimotor training on balance measures and proprioception among middle and older age adults with diabetic peripheral neuropathy. Gait Posture 2019, 74, 114–120. [Google Scholar] [CrossRef]
- Ahmed, A.F. Effect of sensorimotor training on balance in elderly patients with knee osteoarthritis. J. Adv. Res. 2011, 2, 305–311. [Google Scholar] [CrossRef] [Green Version]
- Barbosa Rezende, A.A.; Fernandes de Miranda, E.; Souza Ramalho, H.; Borges Da Silva, J.D.; Silva Carlotto Herrera, S.D.; Rossone Reis, G.; Martin Dantas, E.H. Effects of sensory motor training of lower limb in sedentary elderly as part of functional autonomy. Rev. Andal. Med. Deporte 2015, 8, 61–66. [Google Scholar] [CrossRef] [Green Version]
- Esposito, G.; Altavilla, G.; Di Domenico, F.; Aliberti, S.; D’Isanto, T.; D’Elia, F. Proprioceptive Training to Improve Static and Dynamic Balance in Elderly. Int. J. Stat. Med. Res. 2021, 10, 194–199. [Google Scholar] [CrossRef]
- Gstoettner, M. Preoperative proprioceptive training in patients with total knee arthroplasty. Knee 2011, 18, 265–270. [Google Scholar] [CrossRef]
- Martinez-Amat, A.; Hita-Contreras, F.; Lomas-Vega, R.; Caballero, I.; Alvarez, P.J.; Pez, E.M.-L. Effects of 12-week proprioception training program on postural stability, gait, and balance in older adults: A controlled clinical trial. J. Strength Cond. Res. 2013, 27, 2180–2188. [Google Scholar] [CrossRef]
- Resende Neto, A.G.d.; Santos, M.S.; Silva, R.J.S.; Santana, J.M.d.; Silva-Grigoletto, M.E.D. Effects of different neuromuscular training protocols on the functional capacity of elderly women. Rev. Bras. Med. Esporte 2018, 24, 140–144. [Google Scholar] [CrossRef]
- Rezaeipour, M.; Apanasenko, G.L. Acute Improvement of Postural Steadiness through Neuromuscular and Proprioceptive Training in Sedentary Older Females. Middle East J. Rehabil. Health Stud. 2020, 7, e104894. [Google Scholar] [CrossRef]
- Stolzenberg, N.; Belavý, D.L.; Rawer, R.; Felsenberg, D. Whole-body vibration versus proprioceptive training on postural control in post-menopausal osteopenic women. Gait Posture 2013, 38, 416–420. [Google Scholar] [CrossRef]
- Tsauo, J.-Y.; Cheng, P.-F.; Yang, R.-S. The effects of sensorimotor training on knee proprioception and function for patients with knee osteoarthritis: A preliminary report. Clin. Rehabil. 2008, 22, 448–457. [Google Scholar] [CrossRef]
- Silva, K.N.; Mizusaki Imoto, A.; Almeida, G.J.; Atallah, Á.N.; Peccin, M.S.; Fernandes Moça Trevisani, V. Balance training (proprioceptive training) for patients with rheumatoid arthritis. Cochrane Database Syst. Rev. 2010, 5, CD007648. [Google Scholar] [CrossRef]
- Vásquez-Orellana, K.; López-Vásquez, M.; Méndez-Rebolledo, G.; Guzman Muñoz, E. Efectos de un entrenamiento neuromuscular sobre el equilibrio postural dinámico y propiocepción en basquetbolistas juveniles con inestabilidad funcional de tobillo (Effects of neuromuscular training on dynamic postural balance and proprioception in youth. Retos 2022, 44, 1104–1112. [Google Scholar] [CrossRef]
- Guzmán-Muñoz, E.; Sazo-Rodriguez, S.; Concha-Cisternas, Y.; Valdés-Badilla, P.; Lira-Cea, C.; Silva-Moya, G.; Henríquez, R.; Farias, T.Y.; Cigarroa, I.; Castillo-Retamal, M.; et al. Four Weeks of Neuromuscular Training Improve Static and Dynamic Postural Control in Overweight and Obese Children: A Randomized Controlled Trial. J. Mot. Behav. 2020, 52, 761–769. [Google Scholar] [CrossRef]
- Kanekar, N.; Aruin, A.S. Improvement of anticipatory postural adjustments for balance control: Effect of a single training session. J. Electromyogr. Kinesiol. 2015, 25, 400–405. [Google Scholar] [CrossRef] [Green Version]
- Aruin, A.S.; Ota, T.; Latash, M.L. Anticipatory postural adjustments associated with lateral and rotational perturbations during standing. J. Electromyogr. Kinesiol. 2001, 11, 39–51. [Google Scholar] [CrossRef]
- Hung, Y. Neuromuscular control and rehabilitation of the unstable ankle. World J. Orthop. 2015, 6, 434. [Google Scholar] [CrossRef]
- Ageberg, E.; Nilsdotter, A.; Kosek, E.; Roos, E.M. Effects of neuromuscular training (NEMEX-TJR) on patient-reported outcomes and physical function in severe primary hip or knee osteoarthritis: A controlled before-and-after study. BMC Musculoskelet. Disord. 2013, 14, 232. [Google Scholar] [CrossRef] [Green Version]
- Ali Cader, S.; Dutra Pereira, F.; de Sousa, R.G.; Martin Dantas, E.H. Comparación de la fuerza de la musculatura inspiratoria entre mujeres mayores sedentarias y practicantes de hidrogimnasia. Rev. Esp. Geriatría Gerontol. 2007, 42, 271–275. [Google Scholar] [CrossRef]
- Barzegari, M.; Shojaedin, S.S.; Bayat Tork, M. The Effect of 8-Week Strength Training, Balance Training and Combined Training on the Dynamic and Static Balance of the Elderly Inactive Men. Phys. Treat. Specif. Phys. Ther. J. 2019, 9, 15–22. [Google Scholar] [CrossRef]
- Graham, J.E.; Ostir, G.V.; Kuo, Y.-F.; Fisher, S.R.; Ottenbacher, K.J. Relationship between Test Methodology and Mean Velocity in Timed Walk Tests: A Review. Arch. Phys. Med. Rehabil. 2008, 89, 865–872. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.J.; Park, I.; joo Lee, H.; Lee, O. The reliability and validity of gait speed with different walking pace and distances against general health, physical function, and chronic disease in aged adults. J. Exerc. Nutr. Biochem. 2016, 20, 46–50. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study | Ahmad et al., 2019 [26] | Ahmed, 2011 [27] | Barbosa Rezende et al., 2015 [28] | Esposito et al., 2021 [29] | Gstoettner et al., 2011 [30] | Martinez-Amat et al., 2013 [31] | Resende Neto et al., 2017 [32] | Rezaeipour & Apanasenko, 2020 [33] | Stolzenberg et al., 2018 [34] | Tsauo et al., 2008 [35] |
|---|---|---|---|---|---|---|---|---|---|---|
| 1—Inclusion criteria * | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 2—Random allocation | Yes | No | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes |
| 3—Concealed allocation | No | No | No | No | Yes | No | No | No | No | No |
| 4—Group similarity at baseline | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 5—Blinding of participants | No | No | No | No | No | No | No | No | No | Yes |
| 6—Blinding of therapists | No | Yes | No | No | No | No | No | No | No | Yes |
| 7—Blinding of assessors | No | No | No | No | No | No | No | No | No | No |
| 8—Outcome measures in 85% of sample | Yes | Yes | No | No | Yes | Yes | Yes | Yes | No | Yes |
| 9—Intention-to-treat analysis | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 10—Comparison between groups | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 11—Measures of central tendency and dispersion | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Total score | 6/10 | 6/10 | 5/10 | 5/10 | 7/10 | 5/10 | 6/10 | 6/10 | 5/10 | 8/10 |
| Study | Country | Study Design | Sample’s Initial Health | Groups (n) and Sample Size Female (%) | Mean Age (Year) | Intervention (s) | Data Collection Instruments of Physical Performance | Main Outcomes | |
|---|---|---|---|---|---|---|---|---|---|
| Experiment Group (EG) | Control Group (CG) | ||||||||
| Ahmad et al., 2019 [26] | India | RCT | Diabetic peripheral neuropathy | 21 EG: 12 CG: 9 33.3% Female | 66.7 64.7 | Neuromuscular training and foot care. 3 × 80 min/week 8 weeks | Diabetes education and foot care. | FRT (cm) TUG (sec) OLS (sec) Balance in Force Platform (COP sway (open eyes) and COP sway (closed eyes)). | EG: ↑ FRT, ↑ OLS (closed eyes), ↓ TUG, ↓ COP sway AP (open eyes), ↓ COP sway AP *closed eyes), ↓ COP sway ML (closed eyes). EG vs. CG: significant differences in favor of EG. |
| Ahmed, 2011 [27] | Egypt | RCT | Knee OA | 40 EG: 20 CG: 20 100% Female | 60.0 62.0 | Traditional exercise program in addition to neuromuscular training 3 × 30 min/week 6 weeks | Traditional exercise program | Balance in Biodex Stability System (BBS) (overall stability index, AP stability index and ML stability index). | EG: ↓ overall stability index, ↓ ML stability index, ↓ AP stability index. EG vs. CG: significant differences in favor of EG. |
| Barbosa Rezende et al., 2015 [28] | Brazil | RCT | Sedentary lifestyle | 30 EG: 15 CG: 15 100% Female | NRS | Neuromuscular training 3 × 30 min/week 8 weeks | Usual activities | Functional autonomy (10 m walk, getting up from a sitting position, getting up from the prone position, getting up from a chair and moving around the house, GDLAM index). | EG: ↓10 m walk, ↓ getting up from a sitting position, ↓ getting up from the prone position, ↓ getting up from a chair and moving around the house, ↓ GDLAM index) in favor of EG. EG vs. CG: was not reported |
| Esposito et al., 2021 [29] | Italy | RCT | Apparently healthy | 30 EG: 15 CG: 15 60% Female | NRS | Neuromuscular training 2 × 60 min/week 12 weeks | Not reported | Balance: Berg balance scale (score) Four Square Step Test (sec). | EG: ↑ Berg balance scale and ↓ Four Square Step Test. EG vs. CG: significant differences in favor of EG. |
| Gstoettner et al., 2011 [30] | Austria | RCT | Knee OA | 38 EG: 18 CG: 20 79% Female | 72.8 66.9 | Neuromuscular training 3 × 30 min/week 6 weeks | Usual activities | Balance in BBS (overall stability index, AP stability index and ML stability index). Gait speed (60 m walk test). | EG: ↓ overall stability index. EG vs. CG: significant differences in favor of EG in AP stability index |
| Martinez-Amat et al., 2013 [31] | Spain | Quasi-experimental | Apparently healthy | 44 EG: 20 CG: 24 43% Female | 79.3 77.0 | Neuromuscular training 2 × 50 min/week 12 weeks | Usual activities | Balance in Force Platform (AP displacement and ML displacement (open eyes and closed eyes), COP speed and Romberg quotient (open eyes and closed eyes). Berg balance scale (score) Tinetti scale (score). | EG: ↓ Romberg speed, ↑ Tinetti scale and ↑ balance Berg scale. EG vs. CG: significant differences in favor of EG in ML displacement (open eyes), AP displacement (open eyes), AP displacement (closed eyes), Romberg speed, Tinetti and Berg balance scale. |
| Resende Neto et al., 2017 [32] | Brazil | RCT | Sedentary lifestyle | 32 EG: 16 CG: 16 100% Female | 64.6 66.6 | Neuromuscular training 3 × 60 min/week 8 weeks | Traditional training | Physical performance (sit and reach, back scratch, TUG, sit to stand, elbow flexion, six-minute walk). Dynamic strength (supine, rowing and squatting) Muscle power (supine, rowing and squatting). | EG: ↓ sit and reach, ↓ back scratch, ↓ TUG, ↑ sit to stand, ↑ elbow flexion, ↑six-minute walk. ↑ Dynamic strength (supine, rowing and squatting) ↑ Muscle power (supine, rowing and squatting). EG vs. CG: TUG, sit to stand, elbow flexion and six-minute walk in favor of EG. |
| Rezaeipour & Apanasenko, 2020 [33] | Ukraine | Quasi-experimental | Sedentary lifestyle | 48 EG: 24 CG: 24 100% Female | 70.1 69.3 | Neuromuscular and proprioceptive training 3 × 60 min/week 6 weeks | Seated Rest | Balance in Force Platform (COP total mean velocity, COP velocity AP and COP velocity ML (open eyes and closed eyes)). | EG: ↓ COP velocity ML (closed eyes), ↓ COP total mean velocity. EG vs. CG: significant differences in favor of EG. |
| Stolzenberg et al., 2013 [34] | Germany | RCT | Post-menopausal women | 68 EG: 31 CG: 26 100% Female | 67.3 65.9 | Neuromuscular training 2 × 15 min/week 36 weeks | Whole-body vibration | Balance in Force Platform (COP velocity and COP area). Balance on unstable surface (velocity of movement mm/s). | EG: ↓ velocity of movement and ↑ COP velocity semi-tandem (closed eyes). EG vs. CG: No differences. |
| Tsauo et al., 2008 [35] | Taiwan | RCT | Knee OA | 29 EG: 15 CG: 14 100% Female | 61.7 60.1 | Physical therapy program in addition to neuromuscular training 3 × 30 min/week 8 weeks | Physical therapy program and instructions for exercise at home | Physical performance (60 m walk test, Figure-of-8 walk test, climbing up and down stairs) | EG: no changes significant. EG vs. CG: No differences. |
| Neuromuscular Training | |
|---|---|
| Ahmad et al., 2019 [26] | Warm-up: used cycle ergometer or treadmill at the intensity of 50% to 60% HRmax (10 min). Developing: wall slides, core exercises, balance exercises on an unstable surface, and gait training (different patterns of walking) (50 to 60 min). Cool-down: included deep breathing, abdominal breathing and mild stretching (10 min). |
| Ahmed, 2011 [27] | Consisted of three stages: static, dynamic and functional (30 min). First phase (static): Standing upright position on a firm surface, then on a soft surface; Single Leg Stance with closed eyes (first the affected limb, then the non-affected limb) on a firm surface, then on a soft surface, half-step position, one-leg balance. Second phase (dynamic) in addition: Forward-stepping lunge and T-band kick exercises. Third phase (functional) in addition: Walking exercise on a firm surface, then on a foam surface, squatting exercise, balance exercise on a wobble board. Warm-up and cool-down were not reported. |
| Barbosa Rezende et al., 2015 [28] | Developing: Consisted of eight stages, which included activities such as: walking over 35 cm wide cylindrical blocks, stepping over five 0.75 cm high signal cones, walking in a straight line over 3 m of mats placed end-to-end on the floor, moving forwards and sideways to negotiate obstacles, among others (30 min). Warm-up and cool-down were not reported. |
| Esposito et al., 2021 [29] | Warm-up: joint mobilization (6 min). Developing: circuit with five exercises: balance on one leg, getting up from a 60 cm high chair, walking on a proprioceptive pad, walking in a straight line of 10 ms and throwing softballs toward a wall. Cool-down: walking, stretching and mobilization (50 to 60 min). |
| Gstoettner et al., 2011 [30] | Warm-up: walking on heels and toes and brisk walking (5 to 10 min). Developing: Proprioception and balance training were carried out barefoot on different mats and included exercises with eyes open and repeated with eyes closed. The program included four exercises: slide/step forward/backward, step forward/backward, Single Leg Stance and squats. (30 min). Cool-down was not reported. |
| Martinez-Amat et al., 2013 [31] | No warming-up exercises were performed. Developing: Consisted of three stages (initial, intermediate and advanced) progressing to static and dynamic exercises. Six exercises of hip and knee on a firm surface, then on a soft surface (BOSU ball), were included (30 min). Cool-down: 10 min with slow walk, mobility and stretching exercises. |
| Resende Neto et al., 2017 [32] | Warm-up: joint mobility. Developing: intermittent activities organized in a circuit that required agility, coordination, velocity and muscle power of a set of complex motor systems. In addition, they included multi-articular exercises for lower and upper limbs with intense activation of stabilizing muscles of the spine, organized in a circuit and intermittent high-intensity activities (60 min). Cool-down was not reported. |
| Rezaeipour & Apanasenko, 2020 [33] | Warm-up: shuttle run, backward running, five stretching techniques for the trunk and lower extremities, two strengthening exercises, two impact-training techniques, such as box jumps, as well as doing two-leg versus one-leg jumping exercises. Agility: walk and run in different directions. (20 min). Developing: weight training, based on the recommendations of the American Heart Association and the American College of Sports Medicine (45 to min). Cool-down: activities not reported (10 min). |
| Stolzenberg et al., 2013 [34] | Warm-up: cycle ergometry (15 min). Developing: one set of training using standard gym equipment. Finally, neuromuscular training including Romberg, Tandem and Single Leg Stance were performed on surfaces of varying degrees of instability and with varying degrees of difficulty: firm mat, soft mat, wobble board, air-pillows, with and without shoes, with eyes open or with eyes closed. Softballs, tennis balls, staves and elastic bands were used for coordination training. Warm-up and cool-down were not reported. |
| Tsauo et al., 2008. [35] | Developing: sling suspension systems (TerapiMaster, Nordisk Terapi AS, Norway), where exercises in the supine, sitting and standing positions were performed sequentially. Warm-up and cool-down were not reported. * Time was not reported. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Concha-Cisternas, Y.; Castro-Piñero, J.; Leiva-Ordóñez, A.M.; Valdés-Badilla, P.; Celis-Morales, C.; Guzmán-Muñoz, E. Effects of Neuromuscular Training on Physical Performance in Older People: A Systematic Review. Life 2023, 13, 869. https://doi.org/10.3390/life13040869
Concha-Cisternas Y, Castro-Piñero J, Leiva-Ordóñez AM, Valdés-Badilla P, Celis-Morales C, Guzmán-Muñoz E. Effects of Neuromuscular Training on Physical Performance in Older People: A Systematic Review. Life. 2023; 13(4):869. https://doi.org/10.3390/life13040869
Chicago/Turabian StyleConcha-Cisternas, Yeny, José Castro-Piñero, Ana María Leiva-Ordóñez, Pablo Valdés-Badilla, Carlos Celis-Morales, and Eduardo Guzmán-Muñoz. 2023. "Effects of Neuromuscular Training on Physical Performance in Older People: A Systematic Review" Life 13, no. 4: 869. https://doi.org/10.3390/life13040869
APA StyleConcha-Cisternas, Y., Castro-Piñero, J., Leiva-Ordóñez, A. M., Valdés-Badilla, P., Celis-Morales, C., & Guzmán-Muñoz, E. (2023). Effects of Neuromuscular Training on Physical Performance in Older People: A Systematic Review. Life, 13(4), 869. https://doi.org/10.3390/life13040869