

Evaluation of Rapid Multiplex Reverse Transcription-Quantitative Polymerase Chain Reaction Assays for SARS-CoV-2 Detection in Individual and Pooled Samples

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Specimen Collection and Preparation
2.2. Nucleic Acid Extraction
2.3. Selection of NPS Specimens Pooling and Generation of Pooled Samples
2.4. Multiplex RT-qPCR Assay
2.5. Interpretation of RT-qPCR Results
2.6. Analytical Performance and Limit of Detection
2.7. Statistical Analysis
3. Results
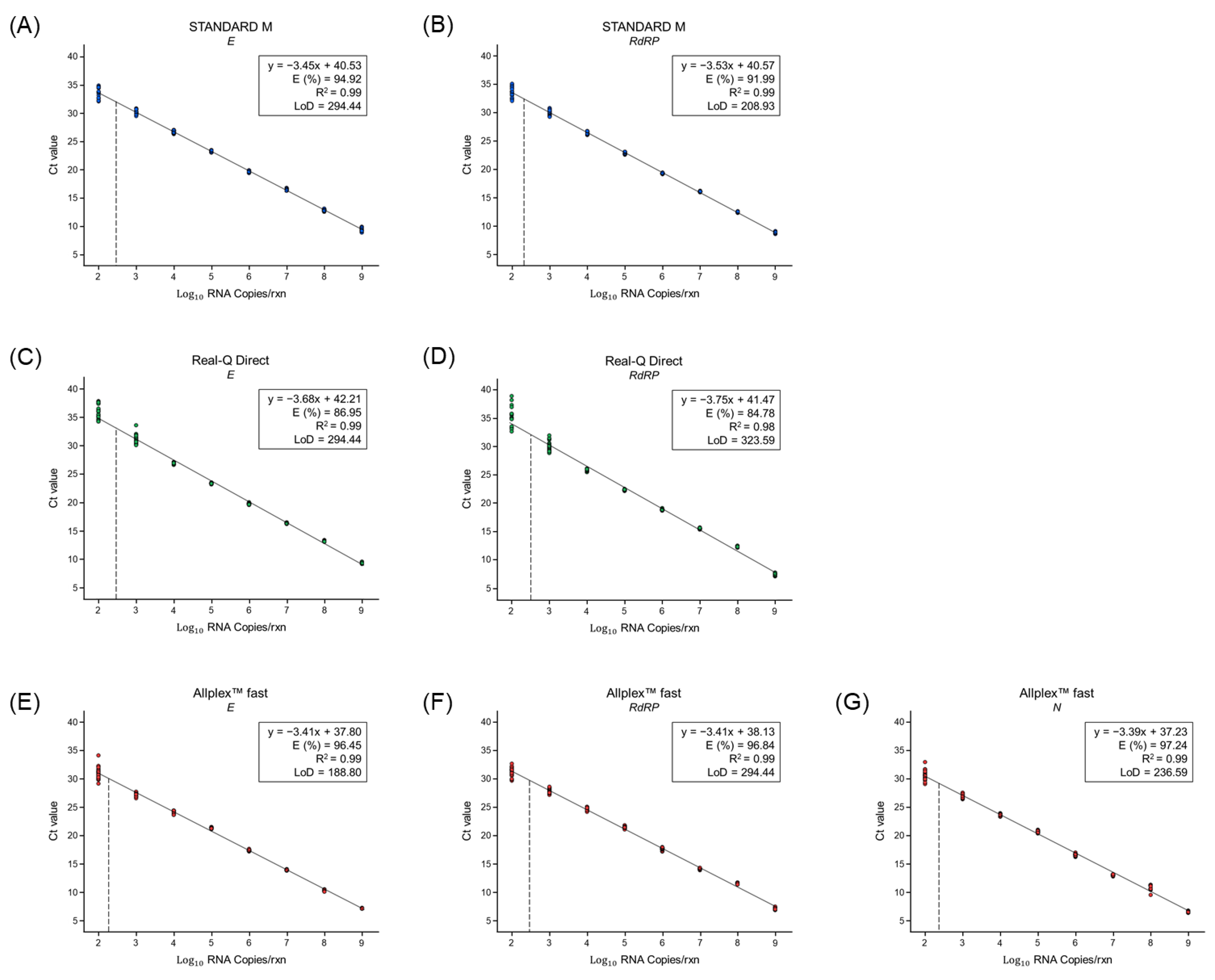
3.1. Evaluation of the Analytical Performance and LoD of the RT-qPCR Kits
3.2. Comparison of the Conventional and Rapid RT-qPCR Kits Using Individual Clinical Samples
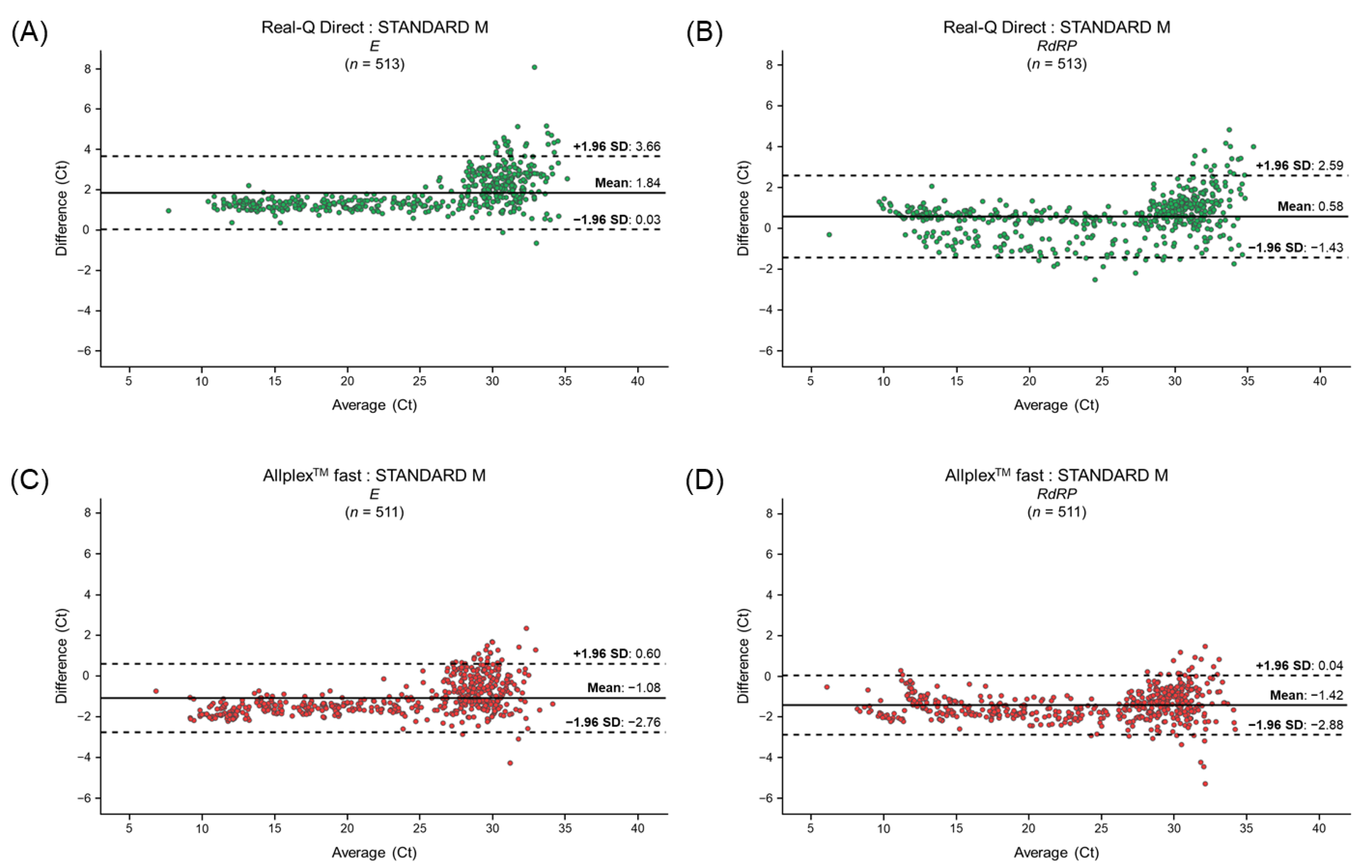
3.3. Differences in the Ct Values for Clinical Samples between the Conventional and Rapid RT-qPCR Kits
3.4. Comparative Evaluation of Pooled Samples Using the Two Rapid Assay Kits
3.5. Clinical Samples Showing Discordant Results for Pooled Samples
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Phelan, A.L.; Katz, R.; Gostin, L.O. The Novel Coronavirus Originating in Wuhan, China: Challenges for Global Health Governance. JAMA 2020, 323, 709–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.T.; Leung, K.; Leung, G.M. Nowcasting and forecasting the potential domestic and international spread of the 2019-nCoV outbreak originating in Wuhan, China: A modelling study. Lancet 2020, 395, 689–697. [Google Scholar] [CrossRef] [Green Version]
- Hui, D.S.; Azhar, E.I.; Madani, T.A.; Ntoumi, F.; Kock, R.; Dar, O.; Ippolito, G.; McHugh, T.D.; Memish, Z.A.; Drosten, C.; et al. The continuing 2019-nCoV epidemic threat of novel coronaviruses to global health—The latest 2019 novel coronavirus outbreak in Wuhan, China. Int. J. Infect. Dis. 2020, 91, 264–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 11 May 2023).
- Ding, K.; Jiang, W.; Xiong, C.; Lei, M. Turning point: A new global COVID-19 wave or a signal of the beginning of the end of the global COVID-19 pandemic? Immun. Inflamm. Dis. 2022, 10, e606. [Google Scholar] [CrossRef] [PubMed]
- Zarocostas, J. With the COVID-19 PHEIC over, what next? Lancet 2023, 401, 1642–1643. [Google Scholar] [CrossRef] [PubMed]
- Dhama, K.; Nainu, F.; Frediansyah, A.; Yatoo, M.I.; Mohapatra, R.K.; Chakraborty, S.; Zhou, H.; Islam, M.R.; Mamada, S.S.; Kusuma, H.I.; et al. Global emerging Omicron variant of SARS-CoV-2: Impacts, challenges and strategies. J. Infect. Public Health 2023, 16, 4–14. [Google Scholar] [CrossRef] [PubMed]
- Markov, P.V.; Ghafari, M.; Beer, M.; Lythgoe, K.; Simmonds, P.; Stilianakis, N.I.; Katzourakis, A. The evolution of SARS-CoV-2. Nat. Rev. Microbiol. 2023, 21, 361–379. [Google Scholar] [CrossRef] [PubMed]
- Yan, M.Z.; Yang, M.; Lai, C.L. Post-COVID-19 Syndrome Comprehensive Assessment: From Clinical Diagnosis to Imaging and Biochemical-Guided Diagnosis and Management. Viruses 2023, 15, 533. [Google Scholar] [CrossRef]
- Filchakova, O.; Dossym, D.; Ilyas, A.; Kuanysheva, T.; Abdizhamil, A.; Bukasov, R. Review of COVID-19 testing and diagnostic methods. Talanta 2022, 244, 123409. [Google Scholar] [CrossRef]
- Nanayakkara, L.; Pettigrew, T.R.; Overton, J.; Ryan, P.L.; Pawar, A.K.; Midson, H.M.; Coldwell, M.J.; Martin, J.E. Reduction in cycle time for a rapid polymerase chain reaction diagnostic test at the point of care. J. Infect. Prev. 2023, 24, 23–29. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. COVID-19 Testing. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/testing/index.html (accessed on 15 September 2021).
- Hayden, M.K.; Hanson, K.E.; Englund, J.A.; Lee, F.; Lee, M.J.; Loeb, M.; Morgan, D.J.; Patel, R.; El Alayli, A.; El Mikati, I.K.; et al. The Infectious Diseases Society of America Guidelines on the Diagnosis of COVID-19: Antigen Testing. Clin. Infect. Dis. 2023. [Google Scholar] [CrossRef]
- Widyasari, K.; Kim, S. Rapid Antigen Tests during the COVID-19 Era in Korea and Their Implementation as a Detection Tool for Other Infectious Diseases. Bioengineering 2023, 10, 322. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.; Calvez, R.; Atkins, M.; Fink, C.G. Comparing lateral flow testing with a rapid RT-PCR method for SARS-CoV-2 detection in the United Kingdom-A retrospective diagnostic accuracy study. Health Sci. Rep. 2022, 5, e811. [Google Scholar] [CrossRef] [PubMed]
- Kweon, O.J.; Kim, H.R.; Lee, M.K.; Lim, Y.K. Real-World Accuracy of a SARS-CoV-2 Rapid Diagnostic Tests in the Republic of Korea. J. Korean Med. Sci. 2022, 37, e310. [Google Scholar] [CrossRef]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.; Bleicker, T.; Brunink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Eurosurveillance 2020, 25, 2000045. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.R.; Kuo, C.Y.; Huang, H.Y.; Yu, I.L.; Hsieh, C.T.; Chen, B.S.; Liu, M.T. Evaluation of conventional and point-of-care real-time RT-PCR tests for the detection of SARS-CoV-2 through a pooled testing strategy. J. Clin. Lab. Anal. 2022, 36, e24491. [Google Scholar] [CrossRef]
- Alcoba-Florez, J.; Gonzalez-Montelongo, R.; Inigo-Campos, A.; de Artola, D.G.; Gil-Campesino, H.; The Microbiology Technical Support Team; Ciuffreda, L.; Valenzuela-Fernandez, A.; Flores, C. Fast SARS-CoV-2 detection by RT-qPCR in preheated nasopharyngeal swab samples. Int. J. Infect. Dis. 2020, 97, 66–68. [Google Scholar] [CrossRef] [PubMed]
- Hossain, M.W.; Hossain, M.; Arafath, K.; Ety, S.S.; Shetu, M.M.H.; Kabir, M.; Noor, F.A.; Mannoor, K. Real-Time fast PCR amplification using designated and conventional real time thermal cycler systems: COVID-19 perspective. PLoS ONE 2022, 17, e0276464. [Google Scholar] [CrossRef] [PubMed]
- Jayakody, H.; Rowland, D.; Pereira, C.; Blackwell, R.; Lasota, T.; Laverick, M.; Tisi, L.; Leese, H.S.; Walsham, A.D.S. Development of a high sensitivity RT-PCR assay for detection of SARS-CoV-2 in individual and pooled nasopharyngeal samples. Sci. Rep. 2022, 12, 5369. [Google Scholar] [CrossRef]
- Kim, S.Y.; Lee, J.; Sung, H.; Lee, H.; Han, M.G.; Yoo, C.K.; Lee, S.W.; Hong, K.H. Pooling Upper Respiratory Specimens for Rapid Mass Screening of COVID-19 by Real-Time RT-PCR. Emerg. Infect. Dis. 2020, 26, 2469–2472. [Google Scholar] [CrossRef]
- Ben-Ami, R.; Klochendler, A.; Seidel, M.; Sido, T.; Gurel-Gurevich, O.; Yassour, M.; Meshorer, E.; Benedek, G.; Fogel, I.; Oiknine-Djian, E.; et al. Large-scale implementation of pooled RNA extraction and RT-PCR for SARS-CoV-2 detection. Clin. Microbiol. Infect. 2020, 26, 1248–1253. [Google Scholar] [CrossRef] [PubMed]
- Lim, K.L.; Johari, N.A.; Wong, S.T.; Khaw, L.T.; Tan, B.K.; Chan, K.K.; Wong, S.F.; Chan, W.L.E.; Ramzi, N.H.; Lim, P.K.C.; et al. A novel strategy for community screening of SARS-CoV-2 (COVID-19): Sample pooling method. PLoS ONE 2020, 15, e0238417. [Google Scholar] [CrossRef] [PubMed]
- Ambrosi, C.; Prezioso, C.; Checconi, P.; Scribano, D.; Sarshar, M.; Capannari, M.; Tomino, C.; Fini, M.; Garaci, E.; Palamara, A.T.; et al. SARS-CoV-2: Comparative analysis of different RNA extraction methods. J. Virol. Methods 2021, 287, 114008. [Google Scholar] [CrossRef] [PubMed]
- Campos, K.R.; Sacchi, C.T.; Goncalves, C.R.; Pagnoca, E.; Dias, A.D.S.; Fukasawa, L.O.; Caterino-de-Araujo, A. COVID-19 laboratory diagnosis: Comparative analysis of different RNA extraction methods for SARS-CoV-2 detection by two amplification protocols. Rev. Inst. Med. Trop. São Paulo 2021, 63, e52. [Google Scholar] [CrossRef]
- Lim, H.J.; Jung, H.S.; Park, M.Y.; Baek, Y.H.; Kannappan, B.; Park, J.Y.; Yang, J.H.; Seol, J.H.; Lee, M.W.; Jung, S.K.; et al. Evaluation of Three Automated Extraction Systems for the Detection of SARS-CoV-2 from Clinical Respiratory Specimens. Life 2022, 12, 68. [Google Scholar] [CrossRef]
- Kim, H.N.; Yoon, S.Y.; Lim, C.S.; Yoon, J. Comparison of three molecular diagnostic assays for SARS-CoV-2 detection: Evaluation of analytical sensitivity and clinical performance. J. Clin. Lab. Anal. 2022, 36, e24242. [Google Scholar] [CrossRef]
- Jeong, S.; Lee, N.; Lee, S.K.; Cho, E.J.; Hyun, J.; Park, M.J.; Song, W.; Kim, H.S. STANDARD M10 SARS-CoV-2 Assay for Rapid Detection of SARS-CoV-2: Comparison of Four Real-Time PCR Assays. Diagnostics 2022, 12, 1998. [Google Scholar] [CrossRef]
- Pawar, S.D.; Khare, A.B.; Keng, S.S.; Kode, S.S.; Tare, D.S.; Singh, D.K.; More, R.L.; Mullick, J. Selection and application of biological safety cabinets in diagnostic and research laboratories with special emphasis on COVID-19. Rev. Sci. Instrum. 2021, 92, 081401. [Google Scholar] [CrossRef]
- Yang, S.; Stanzione, N.; Uslan, D.Z.; Garner, O.B.; de St Maurice, A. Clinical and Epidemiologic Evaluation of Inconclusive COVID-19 PCR Results Using a Quantitative Algorithm. Am. J. Clin. Pathol. 2021, 155, 376–380. [Google Scholar] [CrossRef]
- Hong, K.H.; Kim, G.J.; Roh, K.H.; Sung, H.; Lee, J.; Kim, S.Y.; Kim, T.S.; Park, J.S.; Huh, H.J.; Park, Y.; et al. Update of Guidelines for Laboratory Diagnosis of COVID-19 in Korea. Ann. Lab. Med. 2022, 42, 391–397. [Google Scholar] [CrossRef]
- Van Kasteren, P.B.; van der Veer, B.; van den Brink, S.; Wijsman, L.; de Jonge, J.; van den Brandt, A.; Molenkamp, R.; Reusken, C.; Meijer, A. Comparison of seven commercial RT-PCR diagnostic kits for COVID-19. J. Clin. Virol. 2020, 128, 104412. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.J.; Kang, E.R.; Park, M.Y.; Kim, B.K.; Kim, M.J.; Jung, S.; Roh, K.H.; Sung, N.; Yang, J.H.; Lee, M.W.; et al. Development of a multiplex real-time PCR assay for the simultaneous detection of four bacterial pathogens causing pneumonia. PLoS ONE 2021, 16, e0253402. [Google Scholar] [CrossRef] [PubMed]
- Myles, P.S.; Cui, J. Using the Bland-Altman method to measure agreement with repeated measures. Br. J. Anaesth. 2007, 99, 309–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massetti, G.M.; Jackson, B.R.; Brooks, J.T.; Perrine, C.G.; Reott, E.; Hall, A.J.; Lubar, D.; Williams, I.T.; Ritchey, M.D.; Patel, P.; et al. Summary of Guidance for Minimizing the Impact of COVID-19 on Individual Persons, Communities, and Health Care Systems—United States, August 2022. Morb. Mortal. Wkly. Rep. 2022, 71, 1057–1064. [Google Scholar] [CrossRef] [PubMed]
- Qasem, A.; Shaw, A.M.; Elkamel, E.; Naser, S.A. Coronavirus Disease 2019 (COVID-19) Diagnostic Tools: A Focus on Detection Technologies and Limitations. Curr. Issues Mol. Biol. 2021, 43, 728–748. [Google Scholar] [CrossRef] [PubMed]
- Pu, R.; Liu, S.; Ren, X.; Shi, D.; Ba, Y.; Huo, Y.; Zhang, W.; Ma, L.; Liu, Y.; Yang, Y.; et al. The screening value of RT-LAMP and RT-PCR in the diagnosis of COVID-19: Systematic review and meta-analysis. J. Virol. Methods 2022, 300, 114392. [Google Scholar] [CrossRef]
- Mak, G.C.; Cheng, P.K.; Lau, S.S.; Wong, K.K.; Lau, C.S.; Lam, E.T.; Chan, R.C.; Tsang, D.N. Evaluation of rapid antigen test for detection of SARS-CoV-2 virus. J. Clin. Virol. 2020, 129, 104500. [Google Scholar] [CrossRef] [PubMed]
- Nagura-Ikeda, M.; Imai, K.; Tabata, S.; Miyoshi, K.; Murahara, N.; Mizuno, T.; Horiuchi, M.; Kato, K.; Imoto, Y.; Iwata, M.; et al. Clinical Evaluation of Self-Collected Saliva by Quantitative Reverse Transcription-PCR (RT-qPCR), Direct RT-qPCR, Reverse Transcription-Loop-Mediated Isothermal Amplification, and a Rapid Antigen Test to Diagnose COVID-19. J. Clin. Microbiol. 2020, 58. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Kit | STANDARD M nCoV Real-Time Detection Kit | Real-Q Direct SARS-CoV-2 Detection Kit | Allplex™ SARS-CoV-2 Fast PCR Assay |
|---|---|---|---|
| Target genes | E, RdRP | E, RdRP | E, RdRP, N |
| Template volume | 10 μL | 5 μL | 5 μL |
| PCR running time (individual) | 1 h 26 min | 49 min | 53 min |
| PCR running time (pooled) | 1 h 26 min | 1 h 12 min | 53 min |
| SARS-CoV-2 Variants (lineage) | 16 strains | N/A | 20 strains |
| Interpretation (individual) | Positive—All target genes detected Negative—Even if one target gene is not detected | ||
| Interpretation (pooled) | Positive—Even if one target gene is detected Negative—No target genes detected | ||
| Target | Assay | AUC | 95% CI | p-Value | Cut-Off |
|---|---|---|---|---|---|
| E | Real-Q Direct | 0.96 | 0.91–1 | <0.001 | 30.27 |
| Allplex™ fast | 0.97 | 0.94–0.99 | <0.001 | 30.81 | |
| RdRP | Real-Q Direct | 0.97 | 0.93–1 | <0.001 | 32.71 |
| Allplex™ fast | 0.97 | 0.95–0.98 | <0.001 | 32.44 |
| Assay | STANDARD M | Sensitivity % (95% CI) | Specificity % (95% CI) | PPV % (95% CI) | NPV % (95% CI) | κ Value | |||
|---|---|---|---|---|---|---|---|---|---|
| TP | FP | FN | TN | ||||||
| Real-Q Direct | 513 | 3 | 9 | 608 | 98.28 (96.75–99.21) | 99.51 (98.57–99.90) | 99.42 (98.31–99.88) | 98.54 (97.25–99.33) | 0.98 |
| Allplex™ fast | 511 | 1 | 11 | 610 | 97.89 (96.26–98.94) | 99.84 (99.09–100) | 99.80 (98.92–100) | 98.23 (96.85–99.11) | 0.98 |
| Sample | STANDARD M | Real-Q Direct | Allplex™ Fast | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| E | RdRP | Result | E | RdRP | Result | E | RdRP | N | Result | |
| A | 34.36 | 33.35 | Detected | - | - | Not detected | 33.60 | - | 32.32 | Detected |
| B | 34.00 | 35.01 | Detected | - | - | Not detected | 34.16 | 31.76 | - | Detected |
| C | 34.55 | 34.38 | Detected | - | - | Not detected | 33.51 | 32.62 | - | Detected |
| D | 34.62 | 34.53 | Detected | - | - | Not detected | - | - | 32.21 | Detected |
| E | 34.02 | 34.2 | Detected | - | - | Not detected | - | - | 33.17 | Detected |
| F | - | 34.64 | Detected | - | - | Not detected | - | - | - | Not detected |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baek, Y.-H.; Park, M.-Y.; Lim, H.-J.; Youm, D.-J.; You, Y.; Ahn, S.; Park, J.-E.; Kim, M.-J.; Lee, S.-H.; Sohn, Y.-H.; et al. Evaluation of Rapid Multiplex Reverse Transcription-Quantitative Polymerase Chain Reaction Assays for SARS-CoV-2 Detection in Individual and Pooled Samples. Life 2023, 13, 1717. https://doi.org/10.3390/life13081717
Baek Y-H, Park M-Y, Lim H-J, Youm D-J, You Y, Ahn S, Park J-E, Kim M-J, Lee S-H, Sohn Y-H, et al. Evaluation of Rapid Multiplex Reverse Transcription-Quantitative Polymerase Chain Reaction Assays for SARS-CoV-2 Detection in Individual and Pooled Samples. Life. 2023; 13(8):1717. https://doi.org/10.3390/life13081717
Chicago/Turabian StyleBaek, Young-Hyun, Min-Young Park, Ho-Jae Lim, Dong-Jae Youm, Youngshin You, Seojin Ahn, Jung-Eun Park, Min-Jin Kim, Sun-Hwa Lee, Yong-Hak Sohn, and et al. 2023. "Evaluation of Rapid Multiplex Reverse Transcription-Quantitative Polymerase Chain Reaction Assays for SARS-CoV-2 Detection in Individual and Pooled Samples" Life 13, no. 8: 1717. https://doi.org/10.3390/life13081717
APA StyleBaek, Y. -H., Park, M. -Y., Lim, H. -J., Youm, D. -J., You, Y., Ahn, S., Park, J. -E., Kim, M. -J., Lee, S. -H., Sohn, Y. -H., & Yang, Y. -J. (2023). Evaluation of Rapid Multiplex Reverse Transcription-Quantitative Polymerase Chain Reaction Assays for SARS-CoV-2 Detection in Individual and Pooled Samples. Life, 13(8), 1717. https://doi.org/10.3390/life13081717