
Pictorial Essay on Ultrasound and Magnetic Resonance Imaging of Paraspinal Muscles for Myofascial Pain Syndrome

 , , ,
, , ,  , , and
, , and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Superficial Extrinsic Muscles
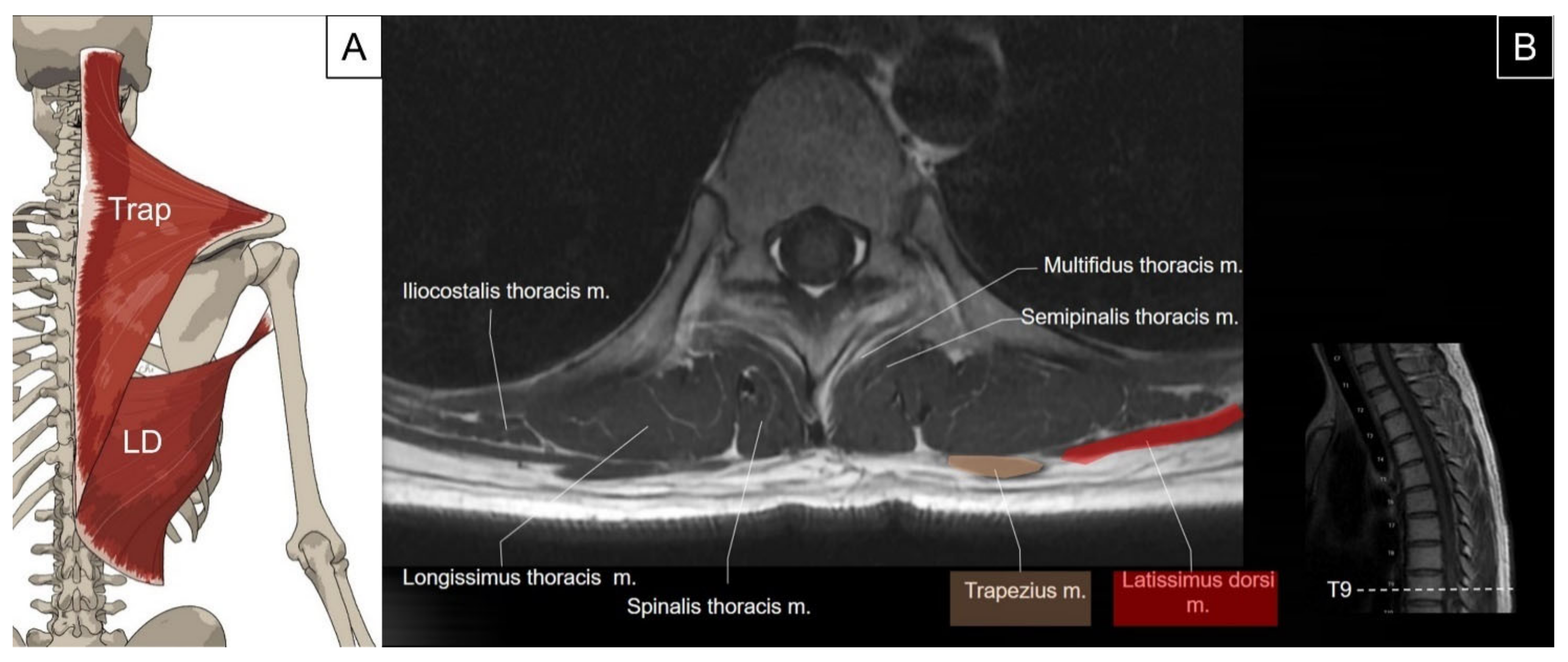
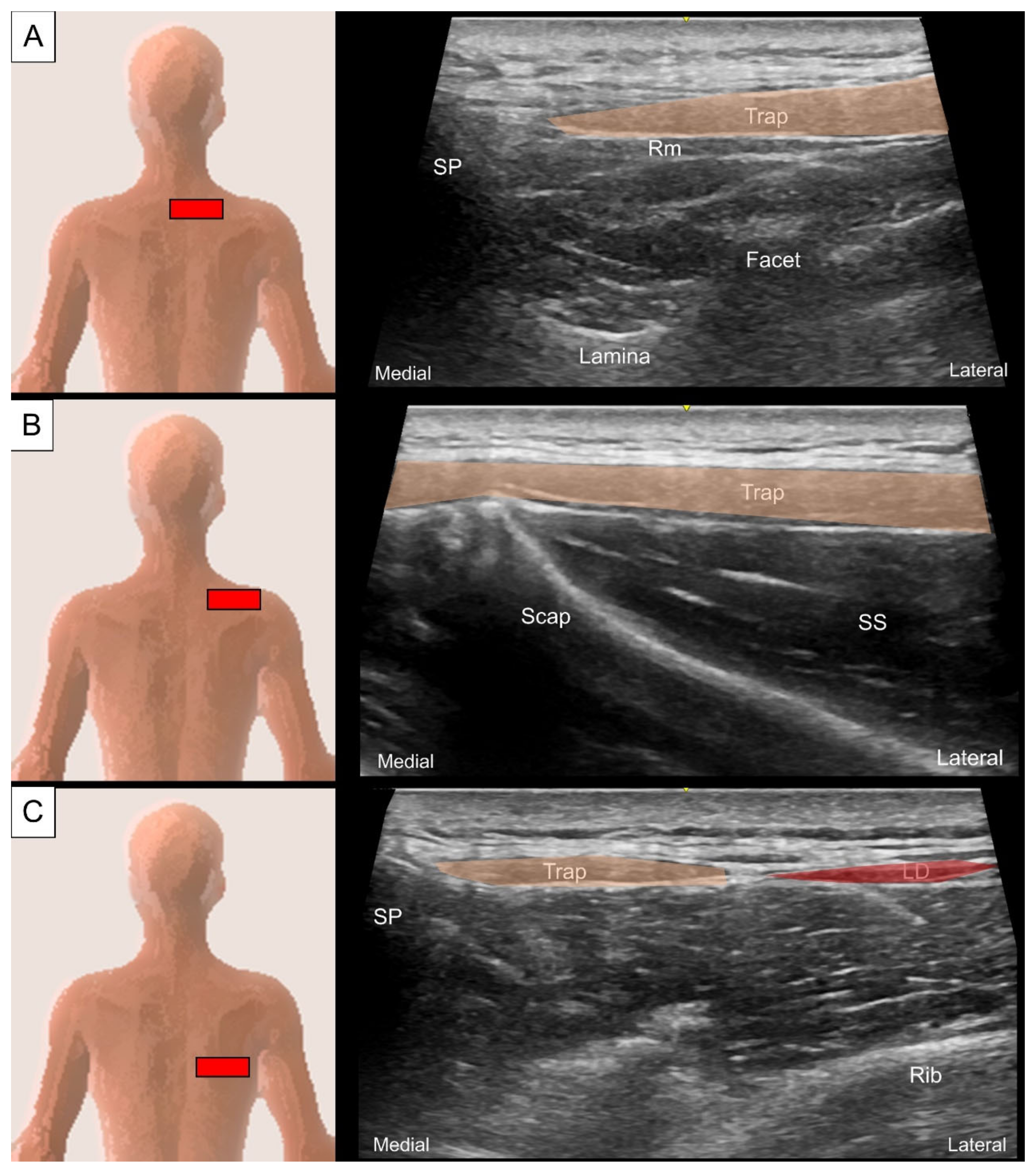
2.1. Trapezius and Latissimus dorsi
2.1.1. Anatomy
2.1.2. Sonographic Scanning
2.1.3. Clinical Relevance
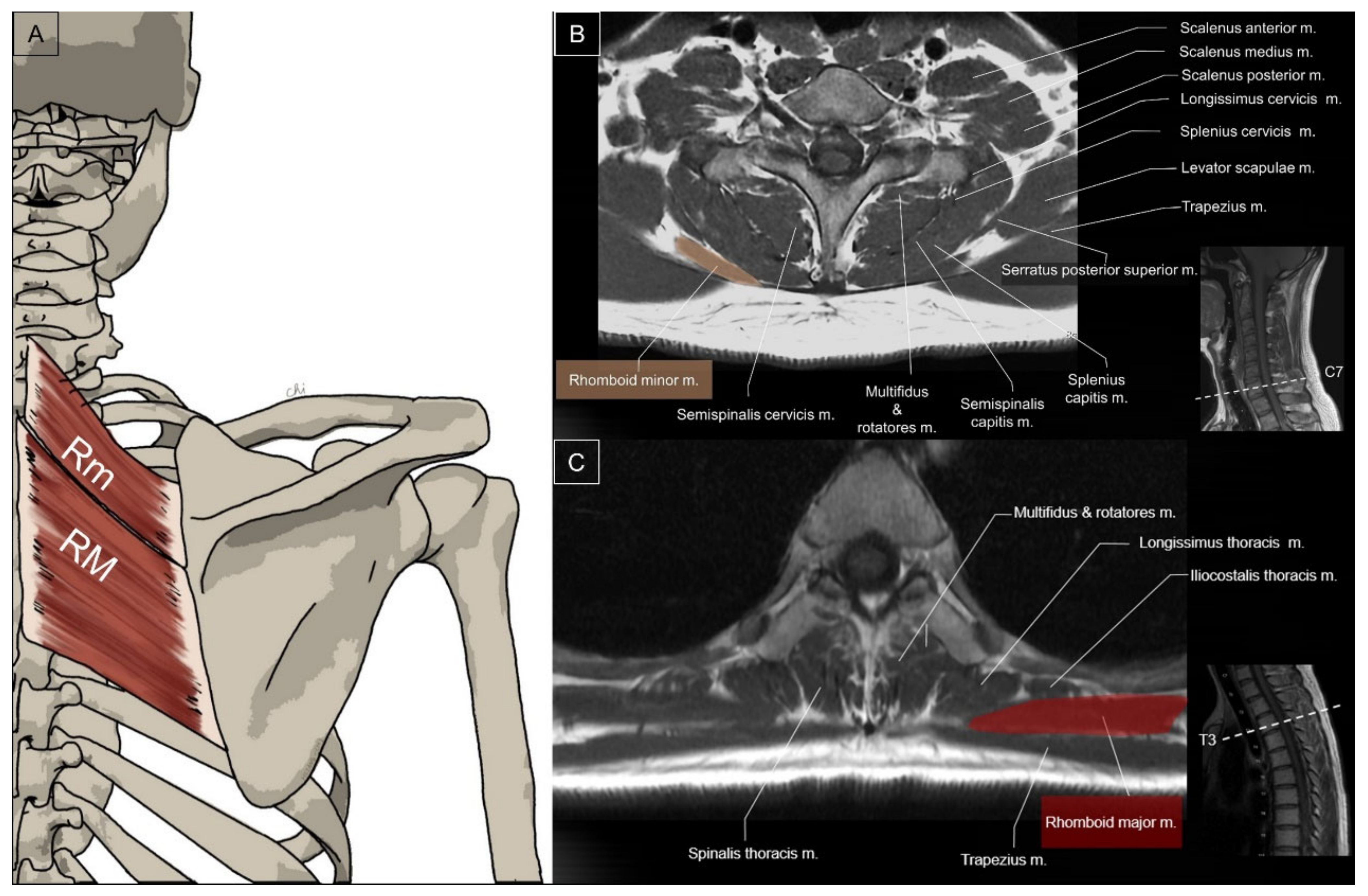
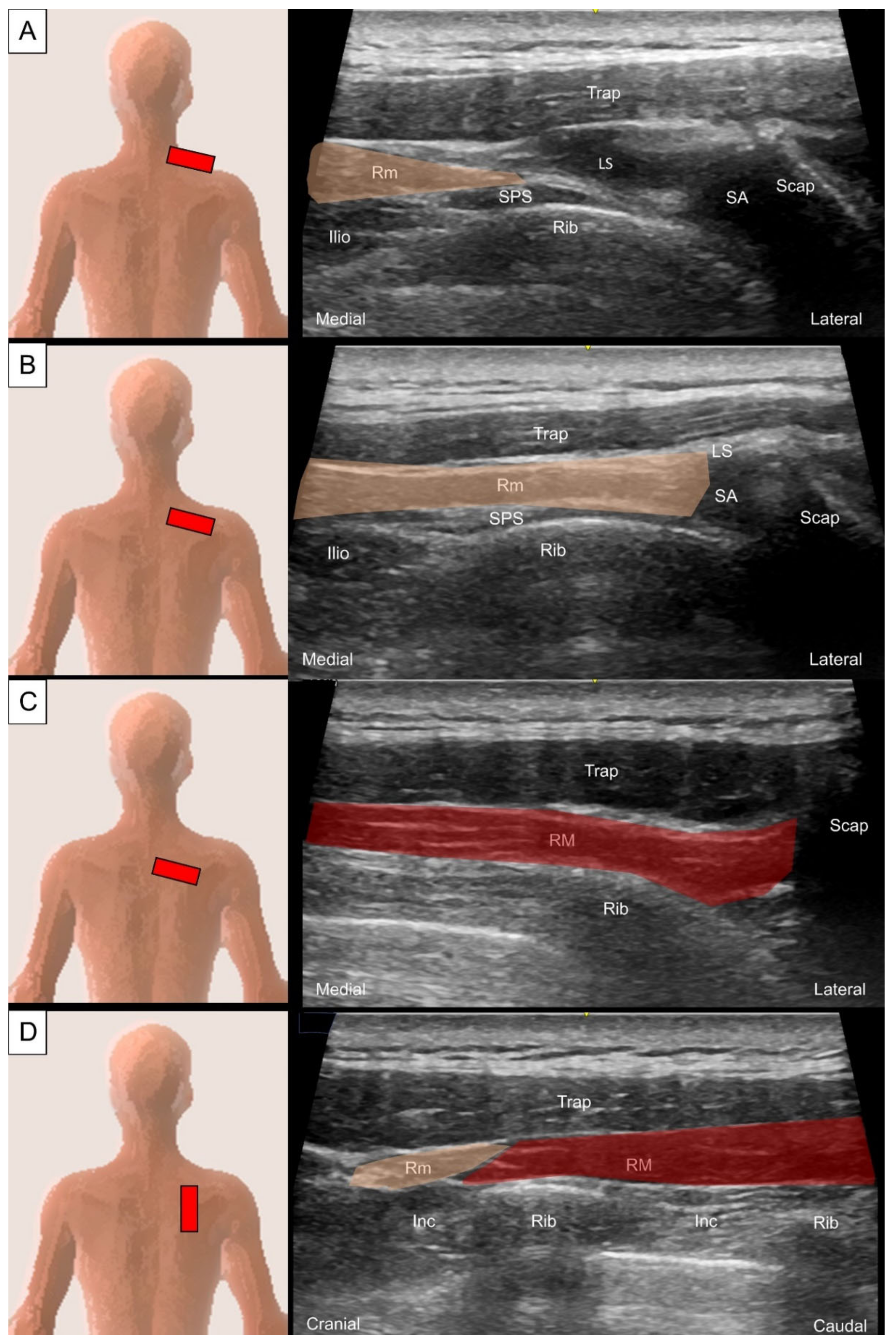
2.2. Rhomboids
2.2.1. Anatomy
2.2.2. Sonographic Scanning
2.2.3. Clinical Relevance
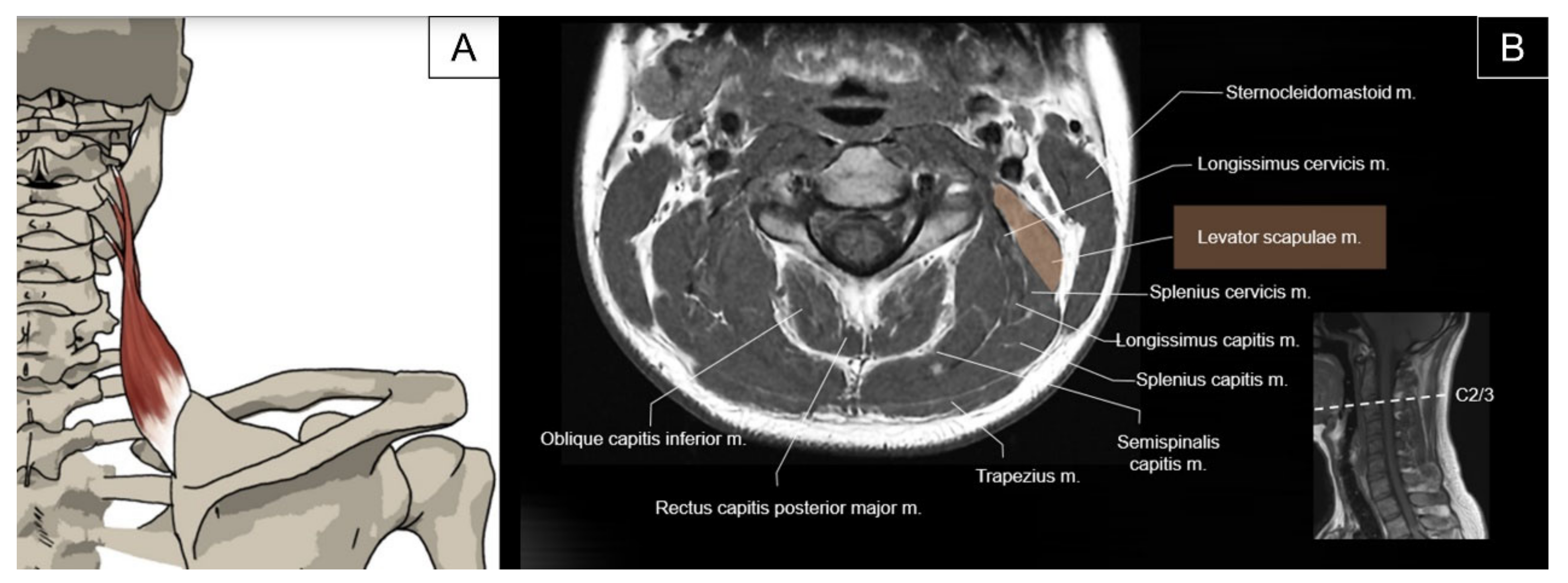
2.3. Levator Scapulae
2.3.1. Anatomy
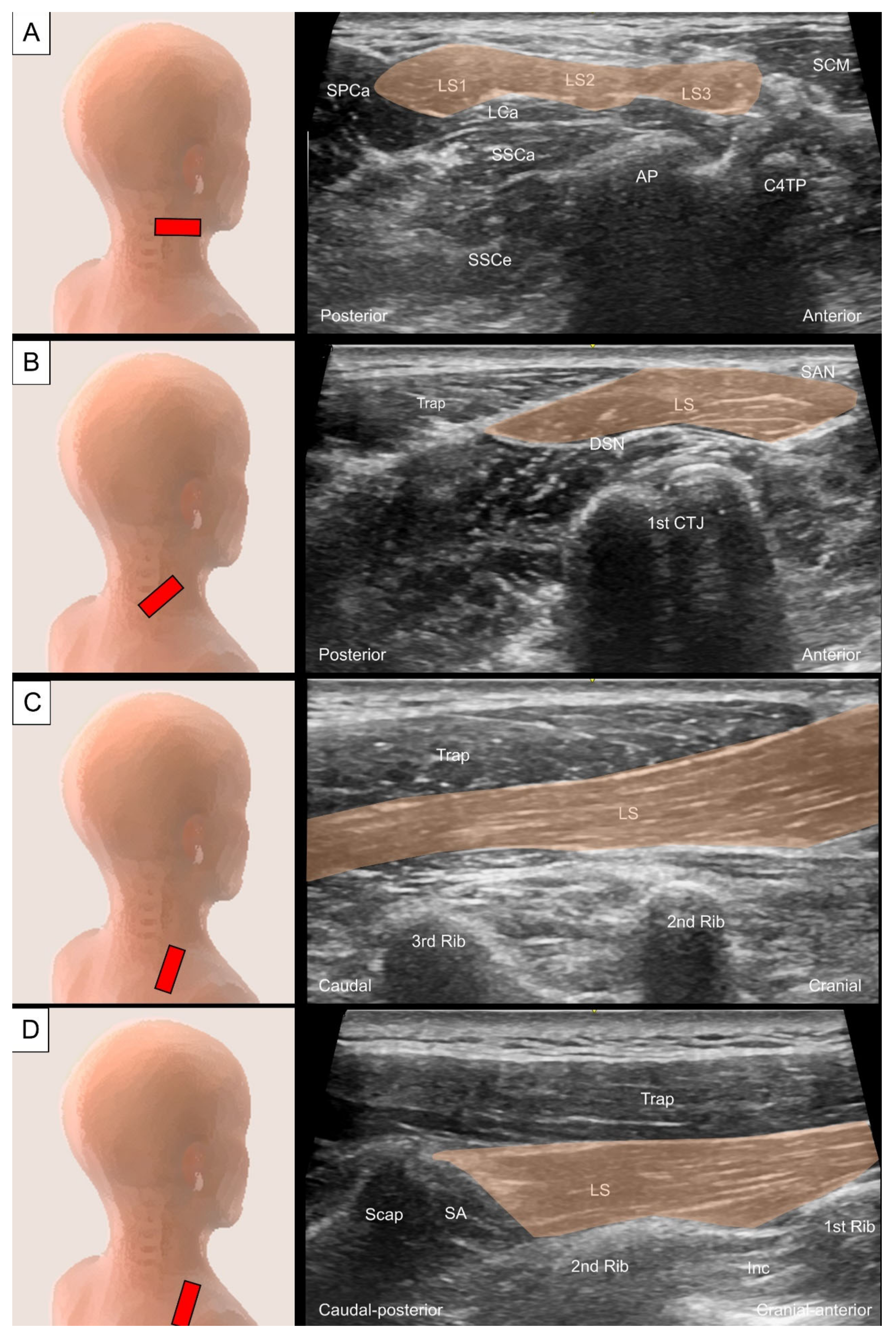
2.3.2. Sonographic Scanning
2.3.3. Clinical Relevance
3. Intermediate Extrinsic Muscles
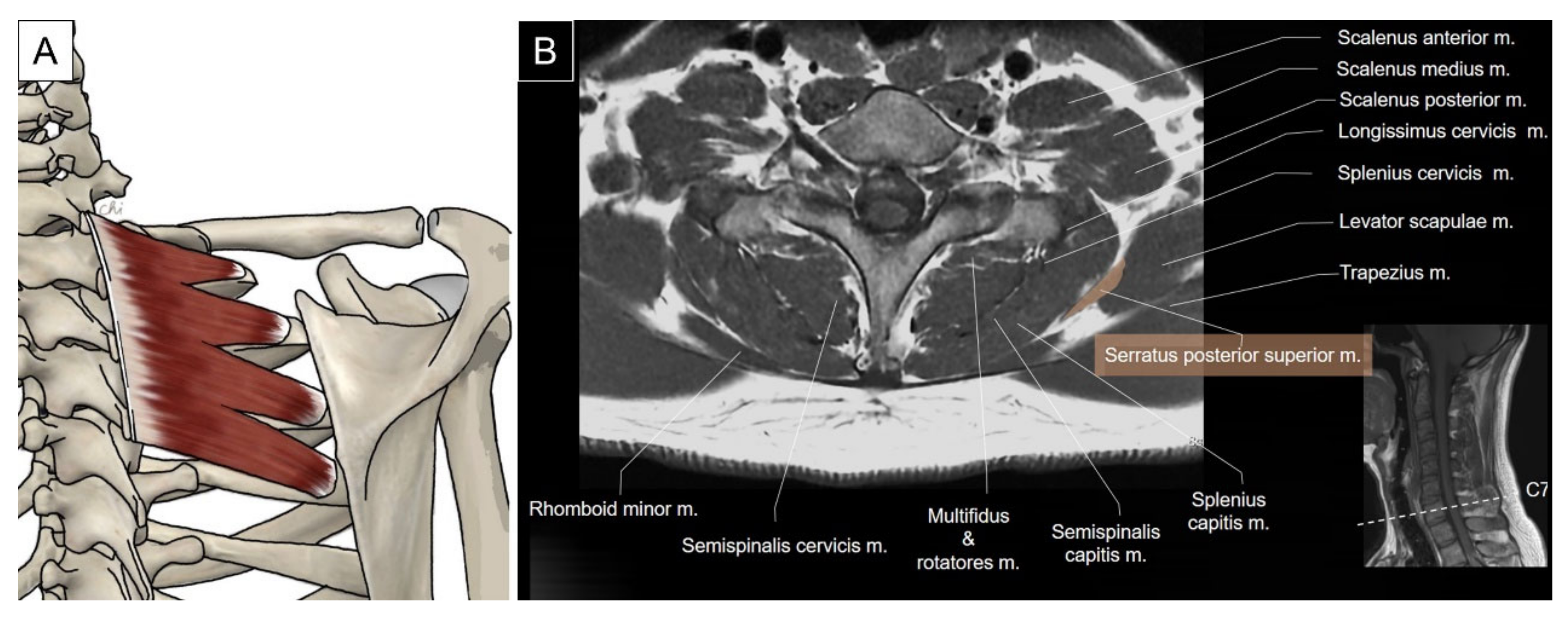
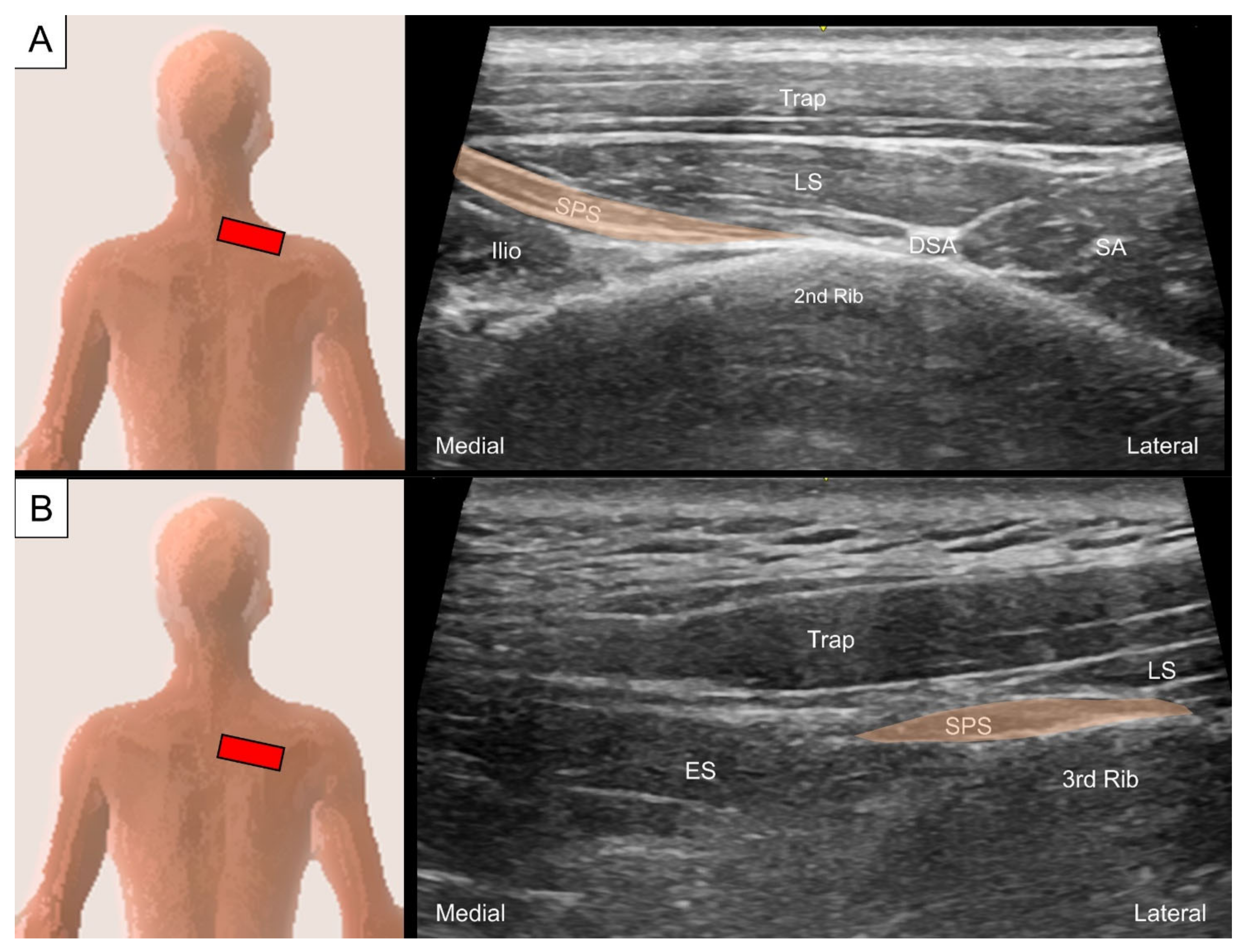
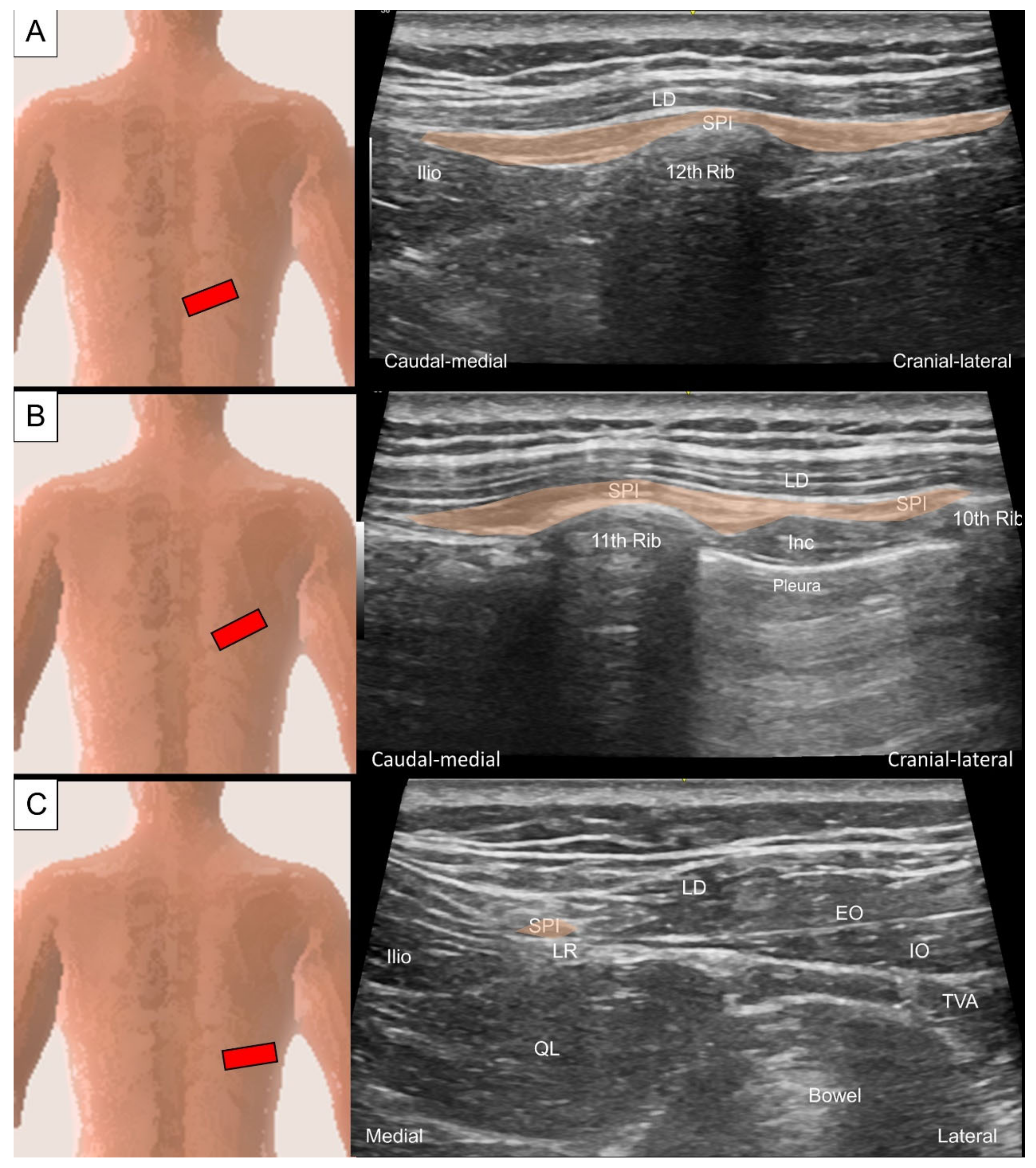
3.1. Serratus Posterior Superior/Inferior
3.1.1. Anatomy
3.1.2. Sonographic Scanning
3.1.3. Clinical Relevance
4. Intrinsic Muscles of the Cervical Region
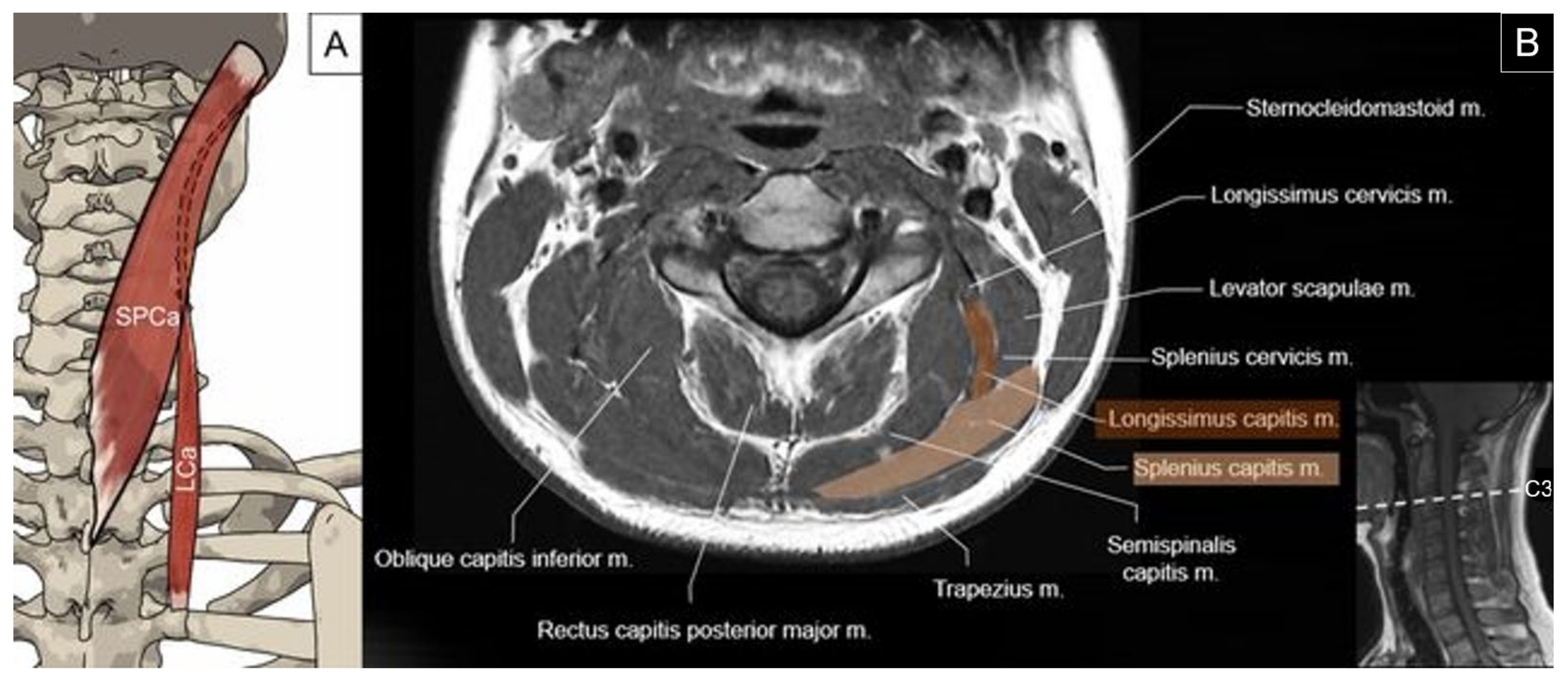
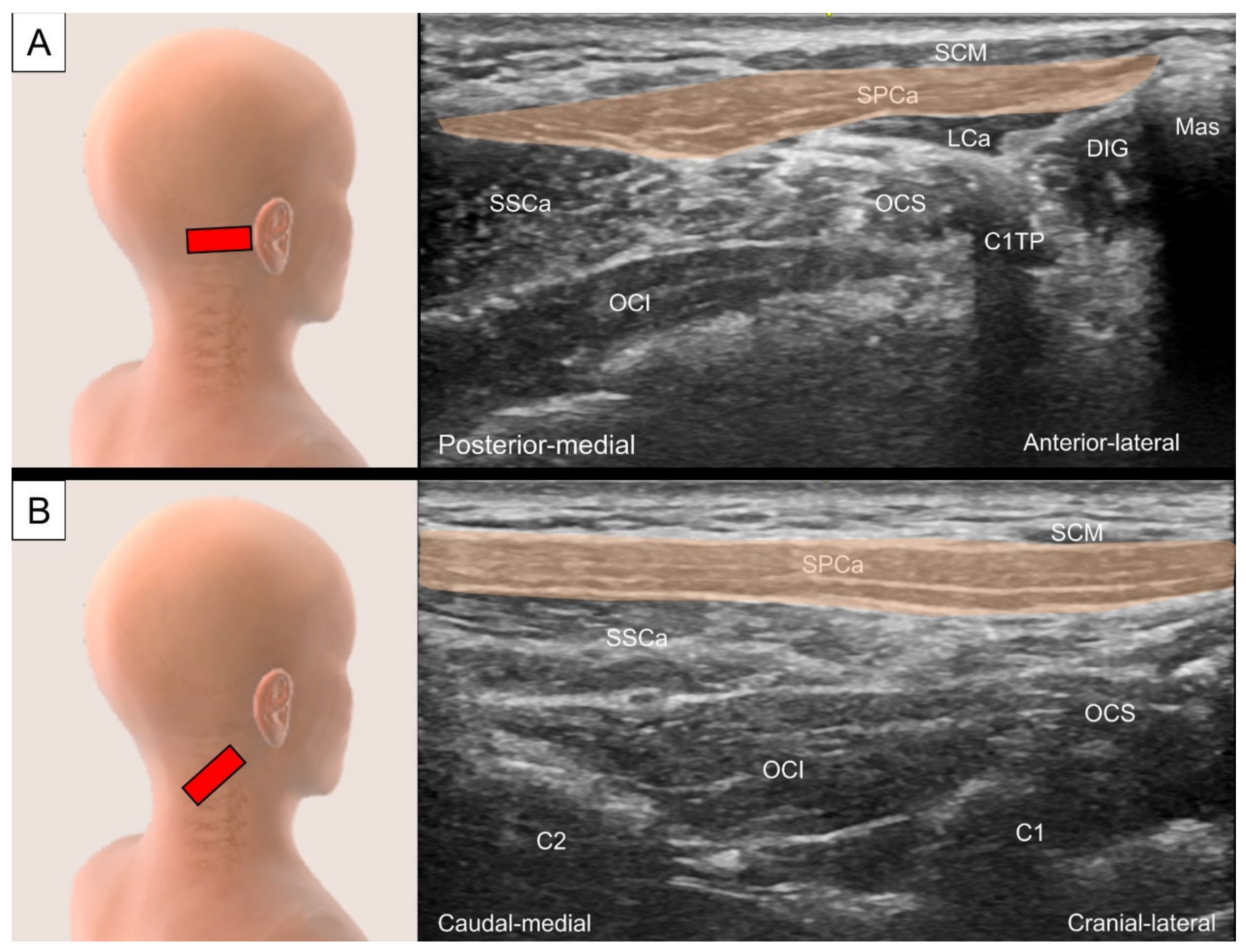
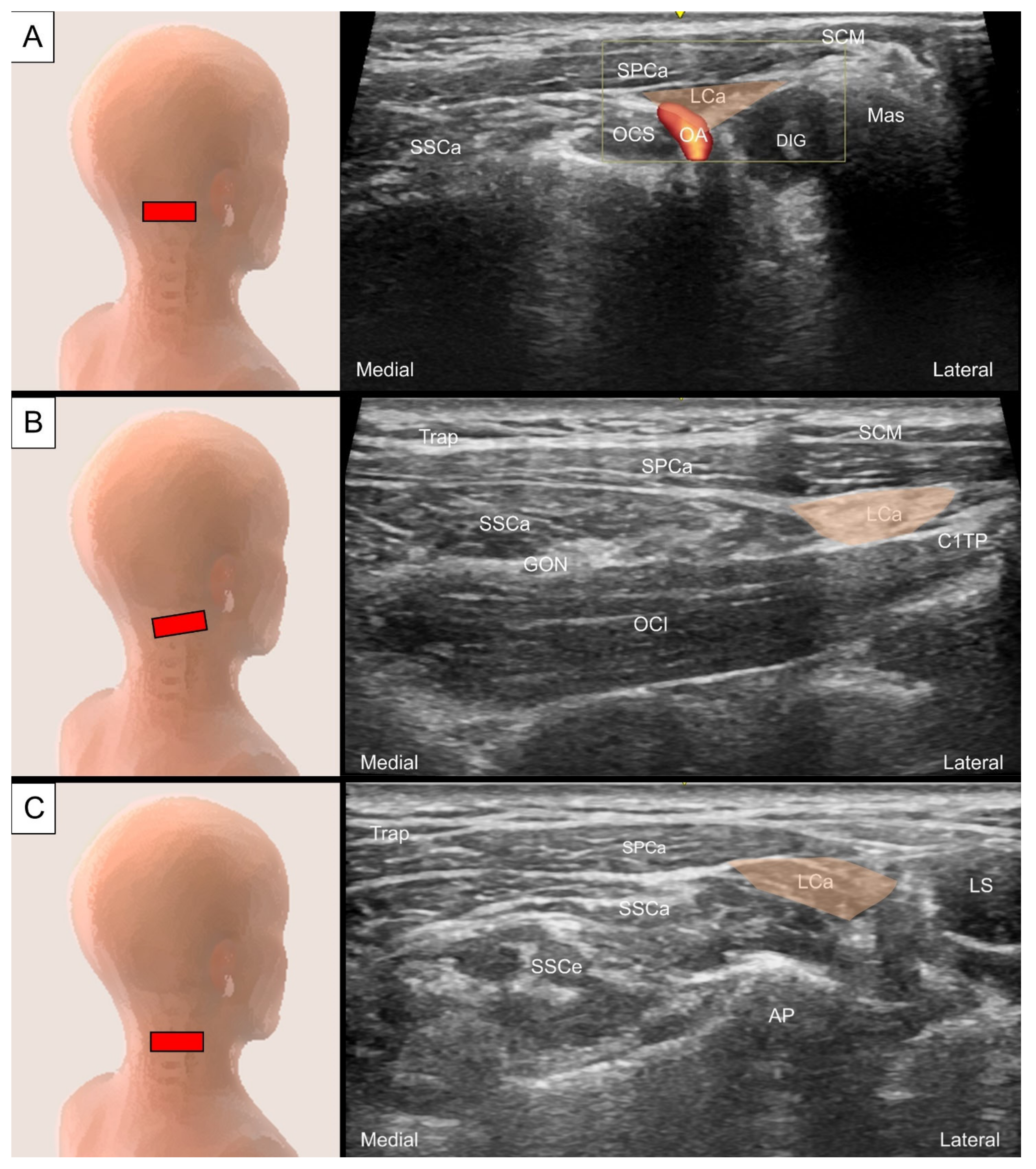
4.1. Splenius Capitis and Longissimus Capitis
4.1.1. Anatomy
4.1.2. Sonographic Scanning
4.1.3. Clinical Relevance
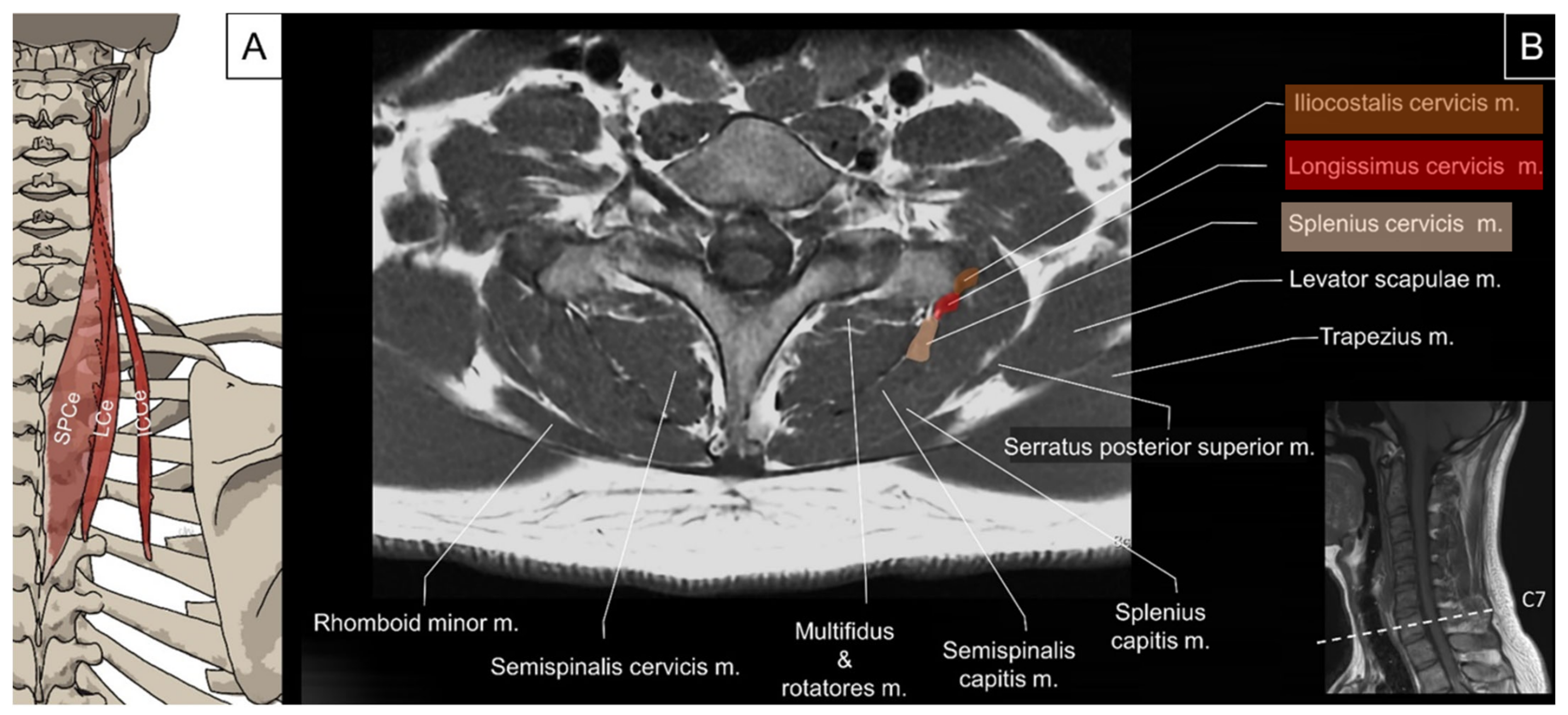
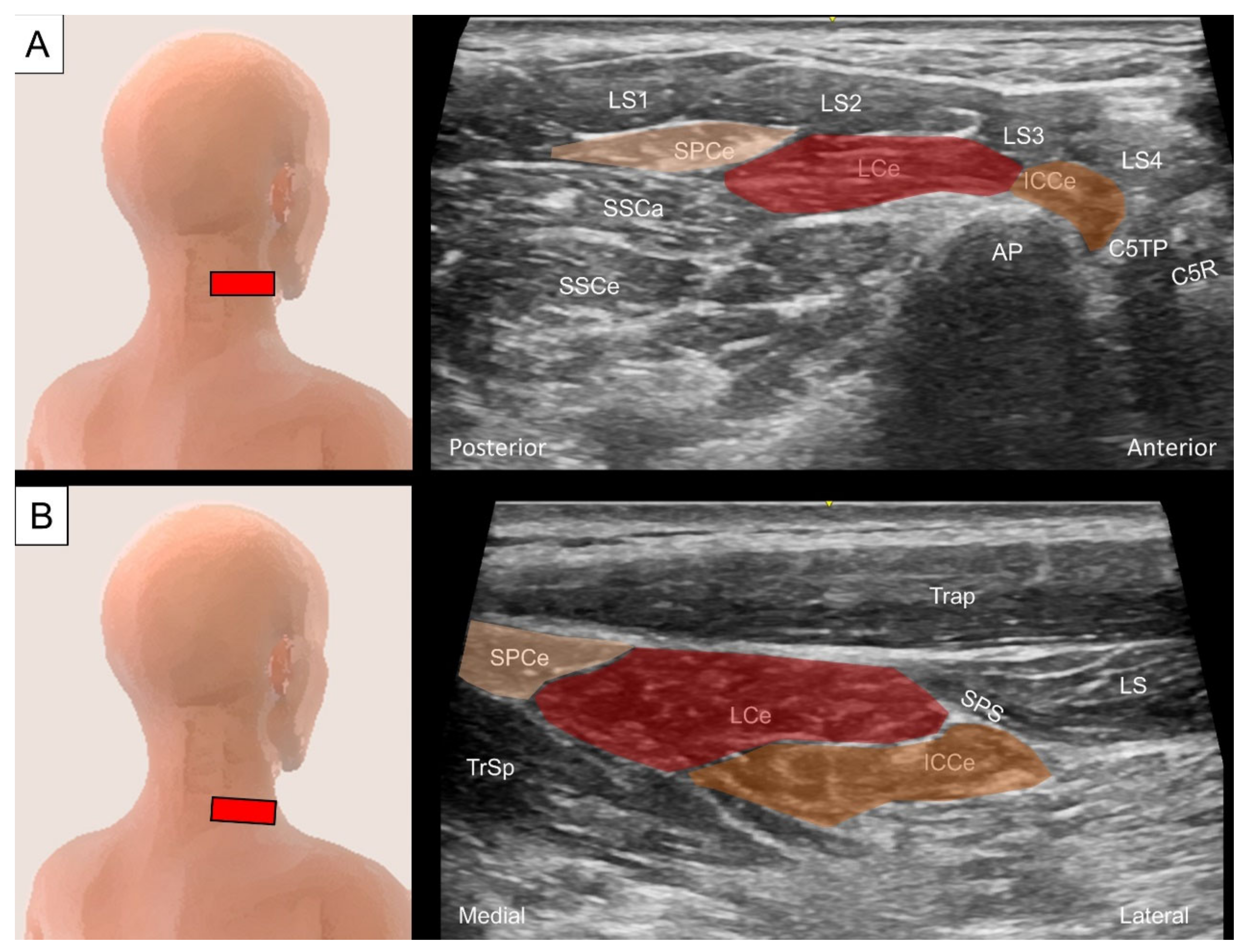
4.2. Iliocostalis/Longissimus/Splenius Cervicis
4.2.1. Anatomy
4.2.2. Sonographic Scanning
4.2.3. Clinical Relevance
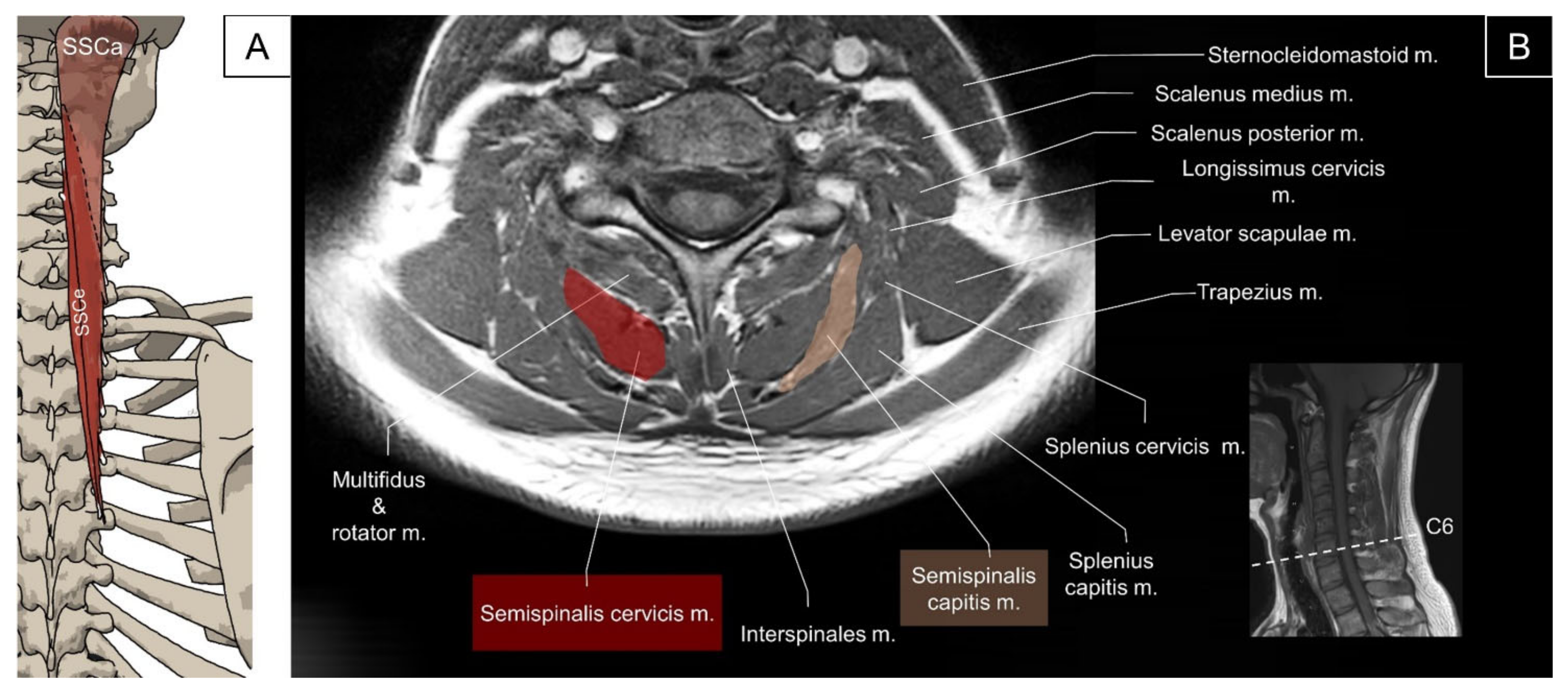
4.3. Transversospinalis (Semispinalis Capitis/Semispinalis Cervicis/Multifidus)
4.3.1. Anatomy
4.3.2. Sonographic Scanning
4.3.3. Clinical Relevance
5. Intrinsic Muscles of the Thoracic and Lumbar Regions
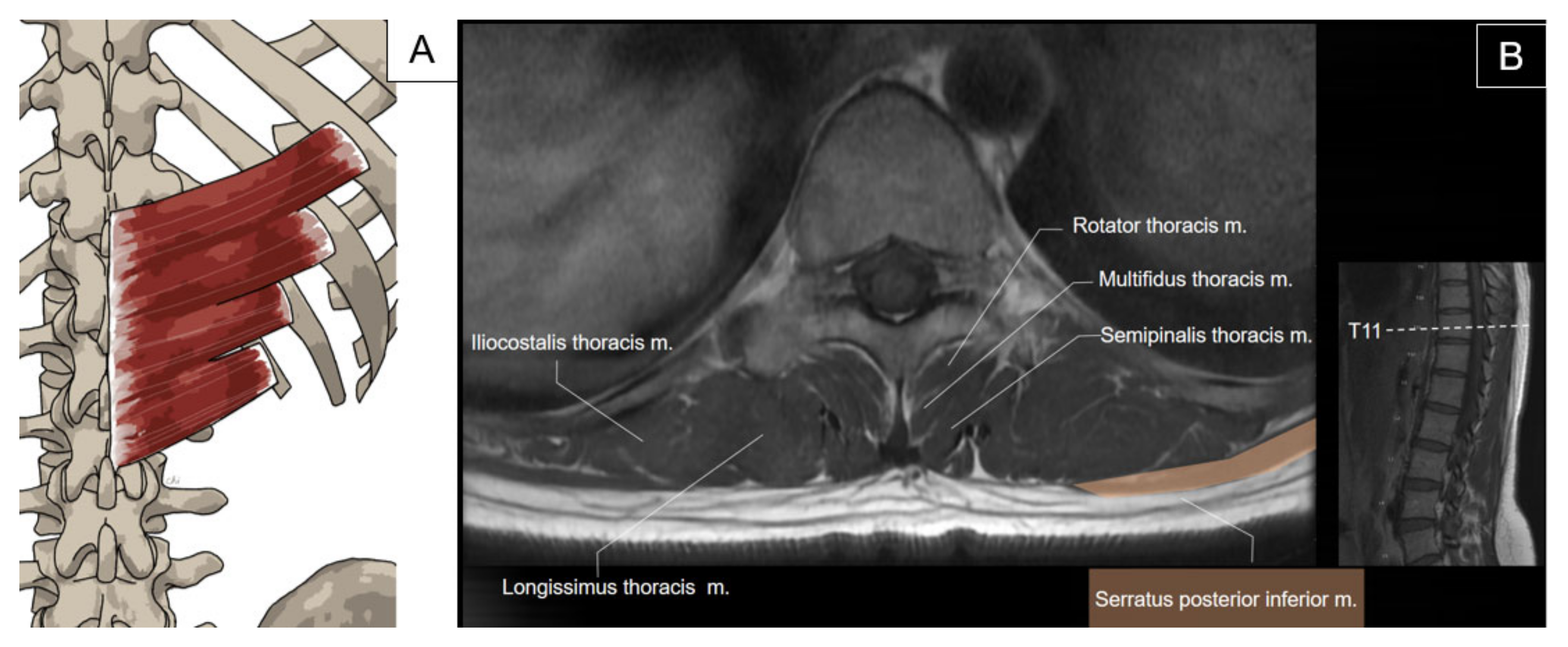
5.1. Iliocostalis Thoracis, Longissimus Thoracis, Semispinalis Thoracis, and Thoracic Multifidus
5.1.1. Anatomy
5.1.2. Sonographic Scanning
5.1.3. Clinical Relevance
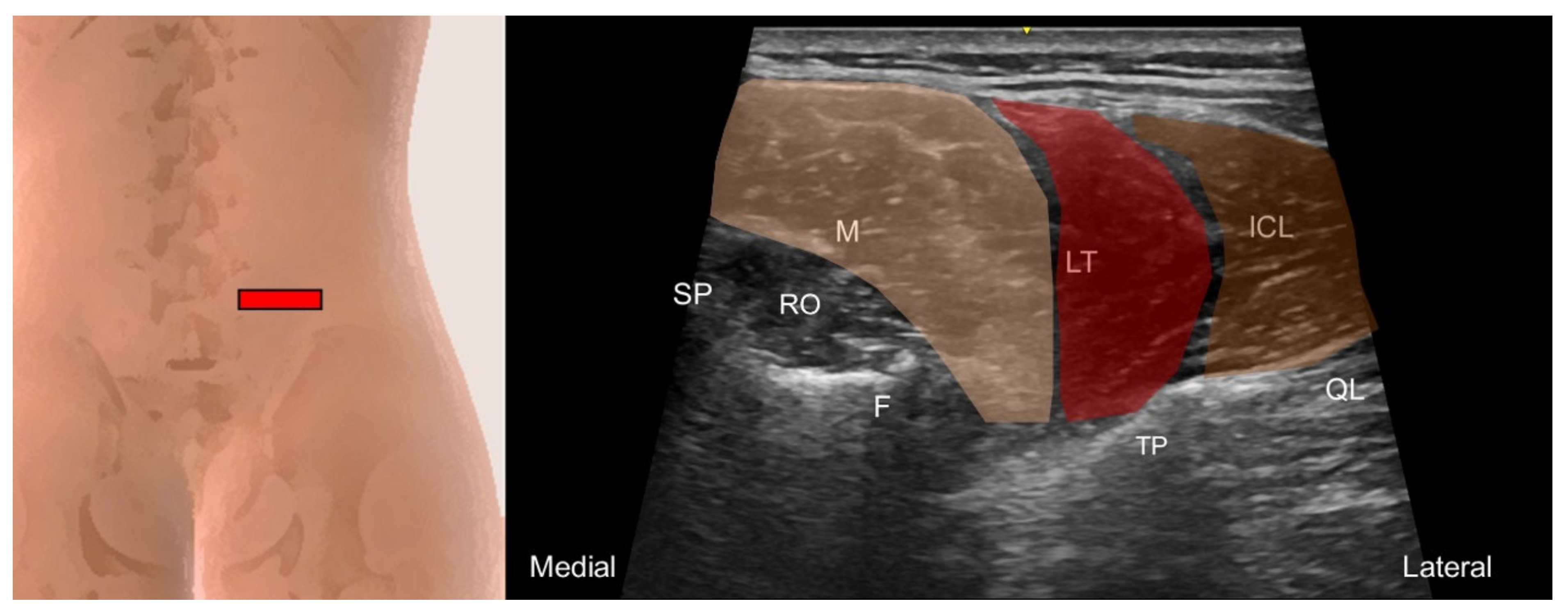
5.2. Iliocostalis Lumborum, Longissimus Thoracis, and Lumbar Multifidus
5.2.1. Anatomy
5.2.2. Sonographic Scanning
5.2.3. Clinical Relevance
6. Other Associated Muscles
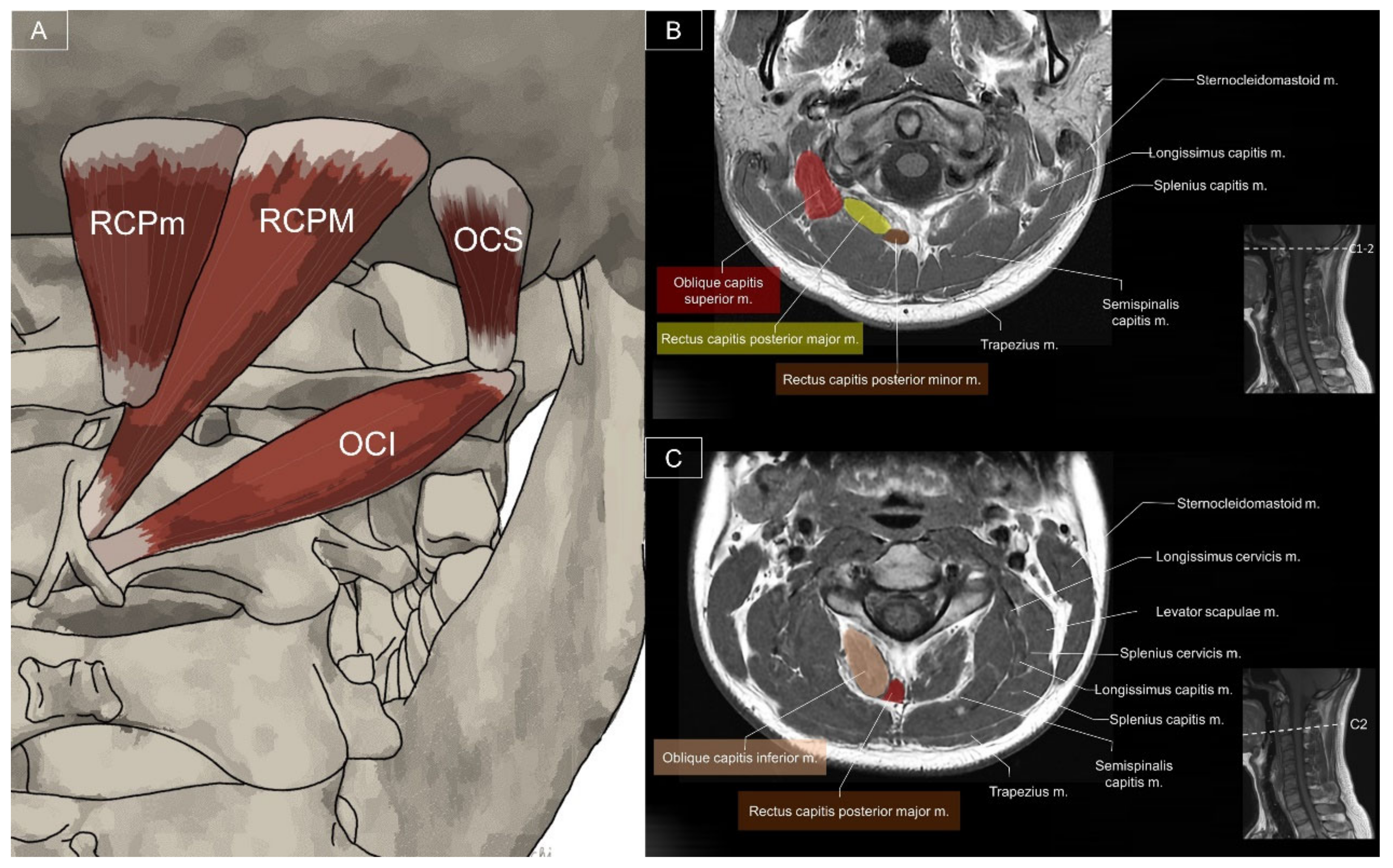
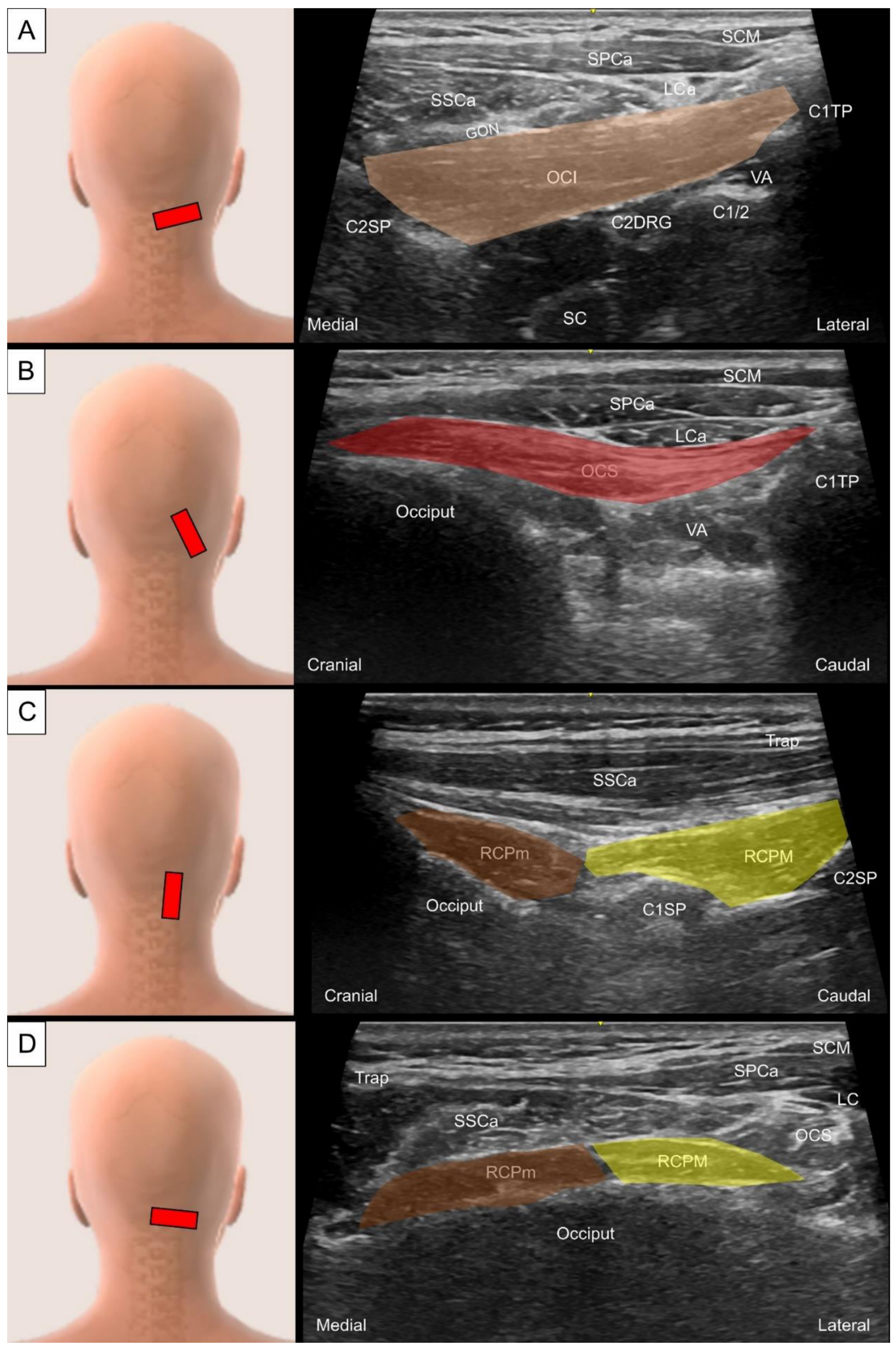
6.1. Sub-Occipital Muscles
6.1.1. Anatomy
6.1.2. Sonographic Scanning
6.1.3. Clinical Relevance
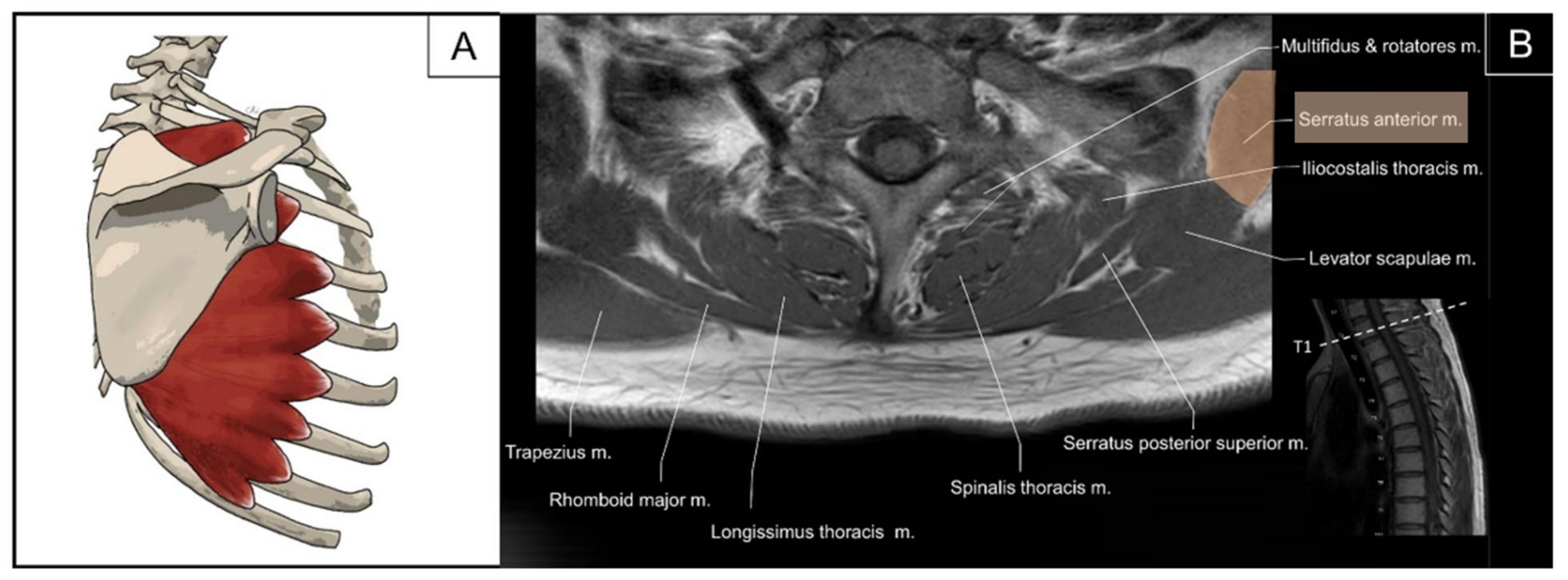
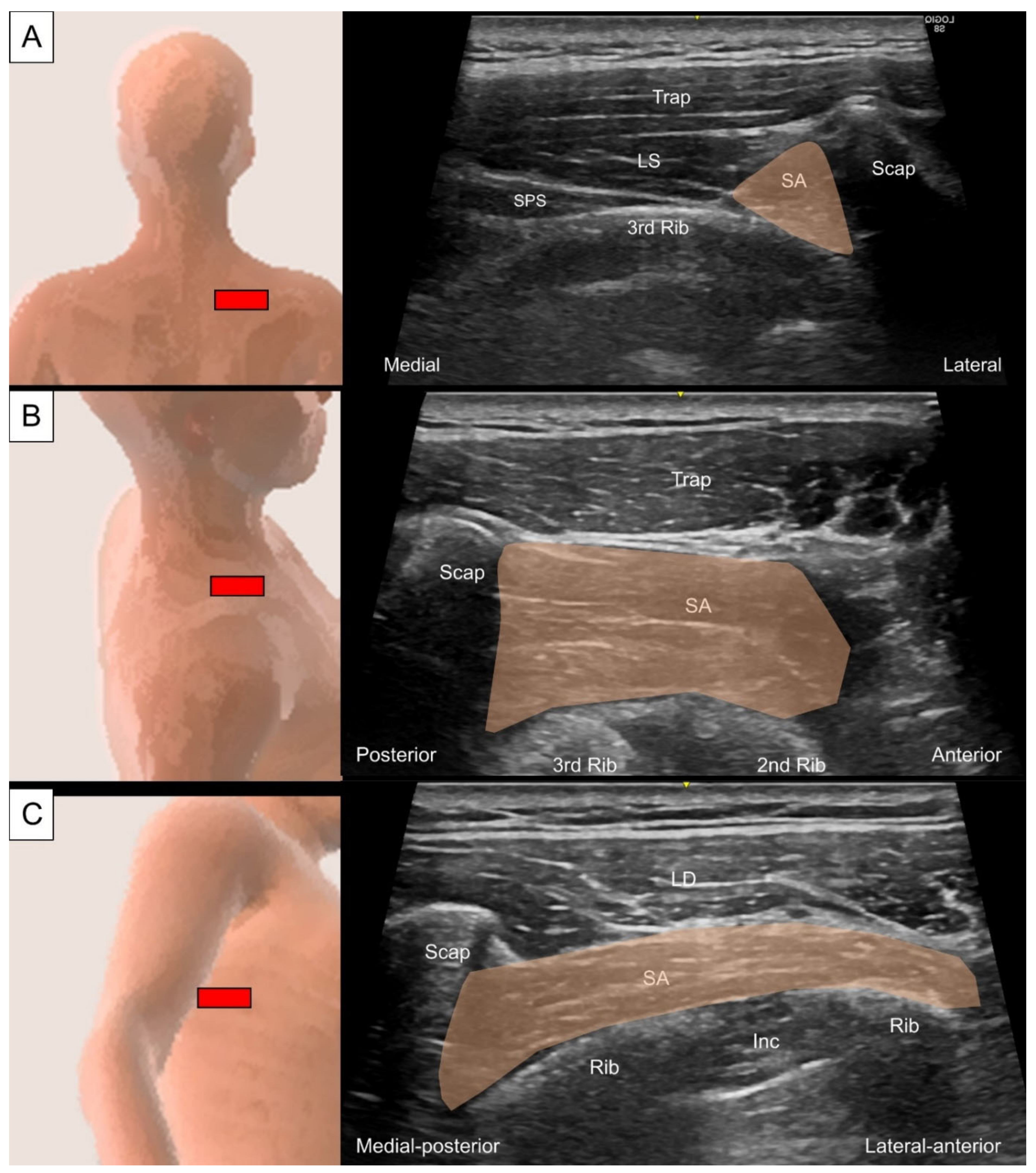
6.2. Serratus Anterior
6.2.1. Anatomy
6.2.2. Sonographic Scanning
6.2.3. Clinical Relevance
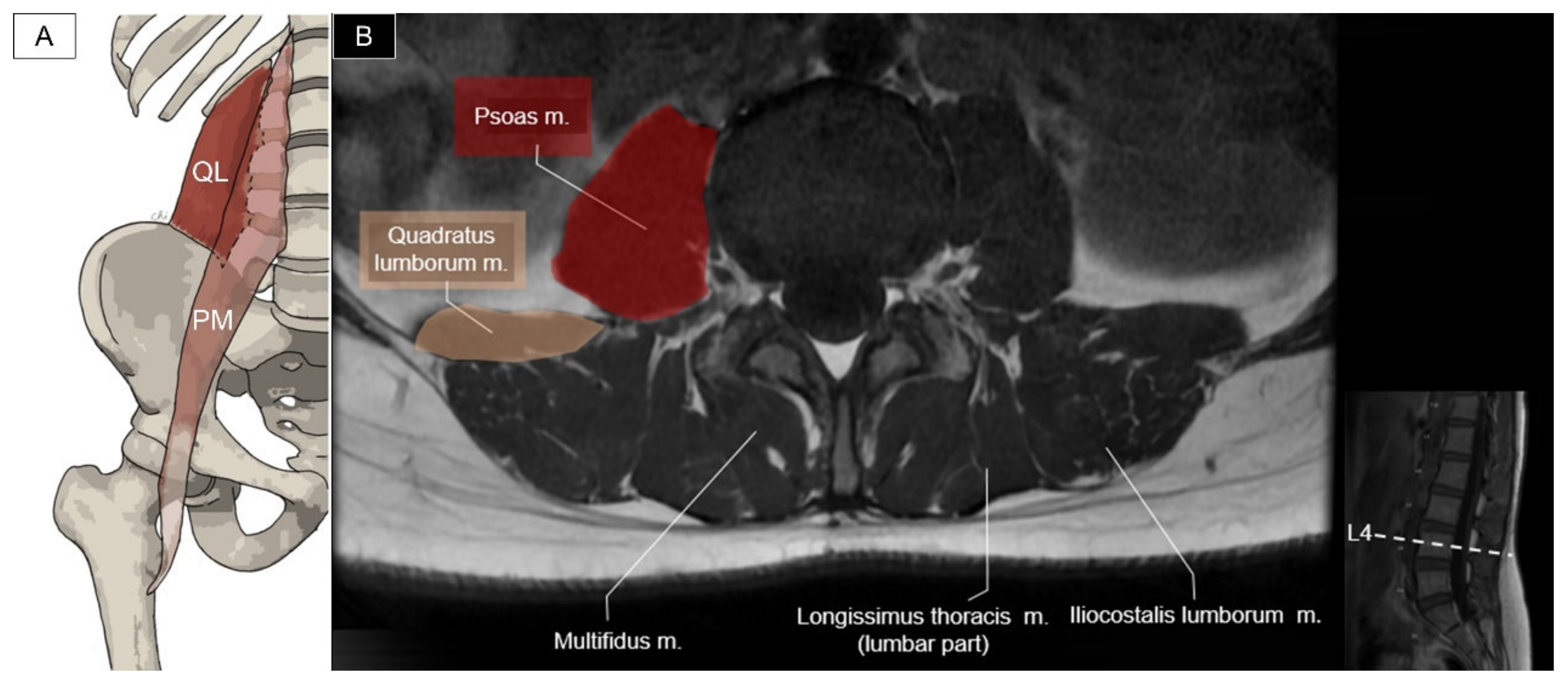
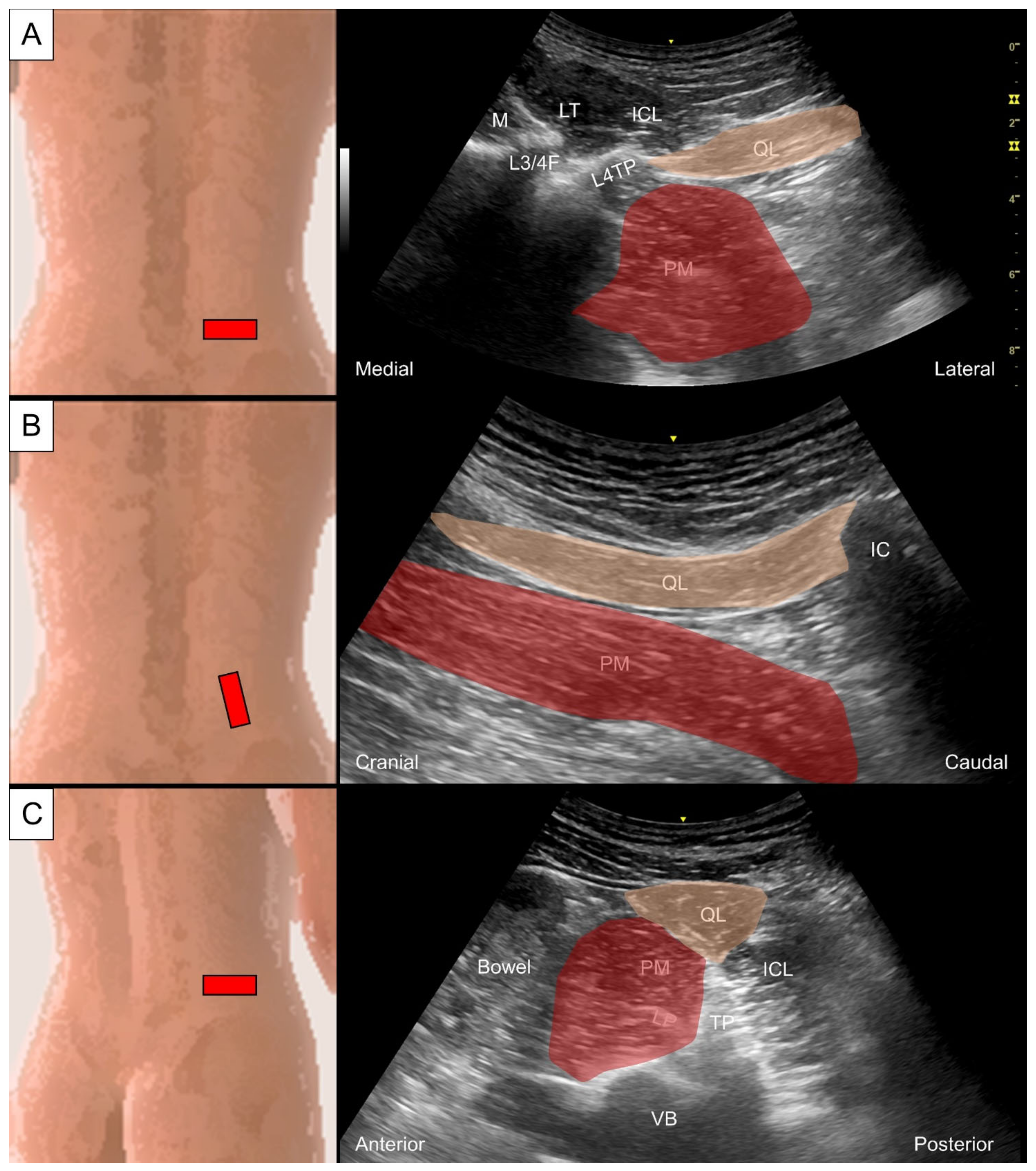
6.3. Quadratus Lumborum and Psoas Major
6.3.1. Anatomy
6.3.2. Sonographic Scanning
6.3.3. Clinical Relevance
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Modes, R.J.; Lafci Fahrioglu, S. Anatomy, Back; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Standring, S.; Gray, H. Gray’s Anatomy: The Anatomical Basis of Clinical Practice, 42nd ed.; Elsevier: Amsterdam, The Netherlands, 2021; Volume XVII, 1588p. [Google Scholar]
- Mazza, D.F.; Boutin, R.D.; Chaudhari, A.J. Assessment of Myofascial Trigger Points via Imaging: A Systematic Review. Am. J. Phys. Med. Rehabil. 2021, 100, 1003–1014. [Google Scholar] [CrossRef] [PubMed]
- Johnson, G.; Bogduk, N.; Nowitzke, A.; House, D. Anatomy and actions of the trapezius muscle. Clin. Biomech. 1994, 9, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Gerling, M.E.; Brown, S.H. Architectural analysis and predicted functional capability of the human latissimus dorsi muscle. J. Anat. 2013, 223, 112–122. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, J.M.; Simons, D.G. Travell, Simons & Simons’ Myofascial Pain and Dysfunction: The Trigger Point Manual, 3rd ed.; Wolters Kluwer Health: Philadelphia, PA, USA, 2019; Volume XXVII, 935p. [Google Scholar]
- Ricci, V.; Ozcakar, L. Ultrasound imaging of the upper trapezius muscle for safer myofascial trigger point injections: A case report. Phys. Sportsmed. 2019, 47, 247–248. [Google Scholar] [CrossRef]
- Pedret, C.; Balius, R.; Idoate, F. Sonography and MRI of latissimus dorsi strain injury in four elite athletes. Skelet. Radiol. 2011, 40, 603–608. [Google Scholar] [CrossRef] [PubMed]
- Kulow, C.; Theopold, J.D.; Ehrlich, A.; Hobusch, C.; Steinke, H. Levator scapulae and rhomboid minor are united. Ann. Anat. Anat. Anz. 2022, 243, 151938. [Google Scholar] [CrossRef] [PubMed]
- Beger, O.; Dinç, U.; Beger, B.; Uzmansel, D.; Kurtoğlu, Z. Morphometric properties of the levator scapulae, rhomboid major, and rhomboid minor in human fetuses. Surg. Radiol. Anat. 2018, 40, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Ulkir, M.; Sargon, M.F. A case of individual variation of the rhomboid muscles. Folia Morphol. 2021, 80, 222–224. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.V.; Wu, W.T.; Mezian, K.; Nanka, O.; Ozcakar, L. Sonoanatomy of Muscles Attaching to the Medial Scapular Border (Levator Scapulae, Rhomboid Minor, and Serratus Anterior) Revisited. Am. J. Phys. Med. Rehabil. 2019, 98, e79–e80. [Google Scholar] [CrossRef]
- Lee, D.G.; Chang, M.C. Dorsal scapular nerve injury after trigger point injection into the rhomboid major muscle: A case report. J. Back Musculoskelet. Rehabil. 2018, 31, 211–214. [Google Scholar] [CrossRef]
- Chang, K.V.; Lin, C.P.; Lin, C.S.; Wu, W.T.; Karmakar, M.K.; Ozcakar, L. Sonographic tracking of trunk nerves: Essential for ultrasound-guided pain management and research. J. Pain Res. 2017, 10, 79–88. [Google Scholar] [CrossRef]
- Henry, J.P.; Munakomi, S. Anatomy, Head and Neck, Levator Scapulae Muscles; StatPearls: Treasure Island, FL, USA, 2024. [Google Scholar]
- Chang, K.V.; Lin, C.P.; Hung, C.Y.; Ozcakar, L.; Wang, T.G.; Chen, W.S. Sonographic Nerve Tracking in the Cervical Region: A Pictorial Essay and Video Demonstration. Am. J. Phys. Med. Rehabil. 2016, 95, 862–870. [Google Scholar] [CrossRef] [PubMed]
- Boswell, M.V.; Cole, B.E.; Weiner, R.S. Weiner’s Pain Management: A Practical Guide for Clinicians, 7th ed.; CRC Press: Boca Raton, FL, USA, 2006; p. 1612. [Google Scholar]
- Tang, T.Y.; Wu, C.H. Identifying the Dorsal Scapular Artery Optimizes the Safety and Precision of the Ultrasound-Guided 5-in-1 Injection. Am. J. Phys. Med. Rehabil. 2019, 98, e80–e81. [Google Scholar] [CrossRef] [PubMed]
- Vilensky, J.A.; Baltes, M.; Weikel, L.; Fortin, J.D.; Fourie, L.J. Serratus posterior muscles: Anatomy, clinical relevance, and function. Clin. Anat. 2001, 14, 237–241. [Google Scholar] [CrossRef] [PubMed]
- Elsharkawy, H.; El-Boghdadly, K.; Barrington, M. Quadratus Lumborum Block: Anatomical Concepts, Mechanisms, and Techniques. Anesthesiology 2019, 130, 322–335. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, C.; Harmon, D. A technical report on ultrasound-guided scapulocostal syndrome injection. Ir. J. Med. Sci. 2016, 185, 669–672. [Google Scholar] [CrossRef] [PubMed]
- Taketa, Y.; Irisawa, Y.; Fujitani, T. Ultrasound guided serrates posterior superior muscle block relieves interscapular myofascial pain. J. Clin. Anesth. 2018, 44, 10–11. [Google Scholar] [CrossRef] [PubMed]
- Henson, B.; Kadiyala, B.; Edens, M.A. Anatomy, Back, Muscles; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Brumpt, E.; Aubry, S.; Vuillier, F.; Tatu, L. Anatomo-sonographic identification of the longissimus capitis and splenius cervicis muscles: Principles for possible application to ultrasound-guided botulinum toxin injections in cervical dystonia. Surg. Radiol. Anat. 2021, 43, 909–915. [Google Scholar] [CrossRef]
- Hatano, Y.; Ota, N.; Noda, K.; Okada, Y.; Suzuki, Y.; Fukuyama, S.; Tanada, S.; Hashimoto, A.; Kondo, T.; Miyazaki, T.; et al. Surgical microanatomy of the occipital artery for suboccipital muscle dissection and intracranial artery reconstruction. Surg. Neurol. Int. 2019, 10, 127. [Google Scholar] [CrossRef]
- Kariya, K.; Usui, Y.; Higashi, N.; Nakamoto, T.; Shimbori, H.; Terada, S.; Takahashi, H.; Ueta, H.; Kitazawa, Y.; Sawanobori, Y.; et al. Anatomical basis for simultaneous block of greater and third occipital nerves, with an ultrasound-guided technique. J. Anesth. 2018, 32, 483–492. [Google Scholar] [CrossRef]
- Rivard, J.; Unsleber, C.; Schomacher, J.; Erlenwein, J.; Petzke, F.; Falla, D. Activation of the semispinalis cervicis and splenius capitis with cervical pulley exercises. Musculoskelet. Sci. Pract. 2017, 30, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.P.; Wang, C.L.; Shau, Y.W.; Wang, S.F. Measurement of cervical multifidus contraction pattern with ultrasound imaging. J. Electromyogr. Kinesiol. 2009, 19, 391–397. [Google Scholar] [CrossRef]
- Rezasoltani, A.; Ahmadipoor, A.; Khademi-Kalantari, K.; Javanshir, K. The sign of unilateral neck semispinalis capitis muscle atrophy in patients with chronic non-specific neck pain. J. Back Musculoskelet. Rehabil. 2012, 25, 67–72. [Google Scholar] [CrossRef]
- Ricci, V.; Ozcakar, L. Ultrasound Imaging of the Paraspinal Muscles for Interscapular Pain After Back Massage. J. Sport. Rehabil. 2020, 29, 830–832. [Google Scholar] [CrossRef]
- Lonnemann, M.E.; Paris, S.V.; Gorniak, G.C. A morphological comparison of the human lumbar multifidus by chemical dissection. J. Man. Manip. Ther. 2008, 16, E84–E92. [Google Scholar] [CrossRef] [PubMed]
- Sánchez Romero, E.A.; Alonso Pérez, J.L.; Muñoz Fernández, A.C.; Battaglino, A.; Castaldo, M.; Cleland, J.A.; Villafañe, J.H. Reliability of Sonography Measures of the Lumbar Multifidus and Transversus Abdominis during Static and Dynamic Activities in Subjects with Non-Specific Chronic Low Back Pain. Diagnostics 2021, 11, 632. [Google Scholar] [CrossRef]
- Heidari, P.; Farahbakhsh, F.; Rostami, M.; Noormohammadpour, P.; Kordi, R. The role of ultrasound in diagnosis of the causes of low back pain: A review of the literature. Asian J. Sports Med. 2015, 6, e23803. [Google Scholar] [CrossRef] [PubMed]
- George, T.; Tadi, P. Anatomy, Head and Neck, Suboccipital Muscles; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Lung, K.; St Lucia, K.; Lui, F. Anatomy, Thorax, Serratus Anterior Muscles; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Vargas-Schaffer, G.; Nowakowsky, M.; Eghtesadi, M.; Cogan, J. Ultrasound-Guided Trigger Point Injection for Serratus Anterior Muscle Pain Syndrome: Description of Technique and Case Series. A&A Practice 2015, 5, 99–102. [Google Scholar] [CrossRef]
- Bordoni, B.; Varacallo, M. Anatomy, Abdomen and Pelvis, Quadratus Lumborum; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Siccardi, M.A.; Tariq, M.A.; Valle, C. Anatomy, Bony Pelvis and Lower Limb, Psoas Major; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Nielsen, M.V.; Bendtsen, T.F.; Borglum, J. Superiority of ultrasound-guided Shamrock lumbar plexus block. Minerva Anestesiol. 2018, 84, 115–121. [Google Scholar] [CrossRef]
- Barreto Silva, A.; Malheiro, N.; Oliveira, B.; Pereira, D.; Antunes, F.; Borges, J.; Cunha, A.C. Efficacy of ultrasound-guided infiltration with levobupivacaine and triamcinolone for myofascial pain syndrome of the quadratus lumborum: A retrospective observational study. Braz. J. Anesth. Anesthesiol. 2021, 73, 718–724. [Google Scholar] [CrossRef]
- Sconfienza, L.M.; Perrone, N.; Lacelli, F.; Lentino, C.; Serafini, G. Ultrasound-guided injection of botulinum toxin A in the treatment of iliopsoas spasticity. J. Ultrasound 2008, 11, 113–117. [Google Scholar] [CrossRef] [PubMed]



























Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hung, C.-Y.; Wang, B.; Chang, H.-C.; Wu, W.-T.; Liu, P.-T.; Chang, K.-V.; Su, D.C.-J.; Mezian, K.; Ricci, V.; Özçakar, L. Pictorial Essay on Ultrasound and Magnetic Resonance Imaging of Paraspinal Muscles for Myofascial Pain Syndrome. Life 2024, 14, 499. https://doi.org/10.3390/life14040499
Hung C-Y, Wang B, Chang H-C, Wu W-T, Liu P-T, Chang K-V, Su DC-J, Mezian K, Ricci V, Özçakar L. Pictorial Essay on Ultrasound and Magnetic Resonance Imaging of Paraspinal Muscles for Myofascial Pain Syndrome. Life. 2024; 14(4):499. https://doi.org/10.3390/life14040499
Chicago/Turabian StyleHung, Chen-Yu, Bow Wang, Hsiang-Chi Chang, Wei-Ting Wu, Ping-Tang Liu, Ke-Vin Chang, Daniel Chiung-Jui Su, Kamal Mezian, Vincenzo Ricci, and Levent Özçakar. 2024. "Pictorial Essay on Ultrasound and Magnetic Resonance Imaging of Paraspinal Muscles for Myofascial Pain Syndrome" Life 14, no. 4: 499. https://doi.org/10.3390/life14040499
APA StyleHung, C. -Y., Wang, B., Chang, H. -C., Wu, W. -T., Liu, P. -T., Chang, K. -V., Su, D. C. -J., Mezian, K., Ricci, V., & Özçakar, L. (2024). Pictorial Essay on Ultrasound and Magnetic Resonance Imaging of Paraspinal Muscles for Myofascial Pain Syndrome. Life, 14(4), 499. https://doi.org/10.3390/life14040499