

AntiHalluciNet: A Potential Auditing Tool of the Behavior of Deep Learning Denoising Models in Low-Dose Computed Tomography


Abstract
:1. Introduction
2. Materials and Methods
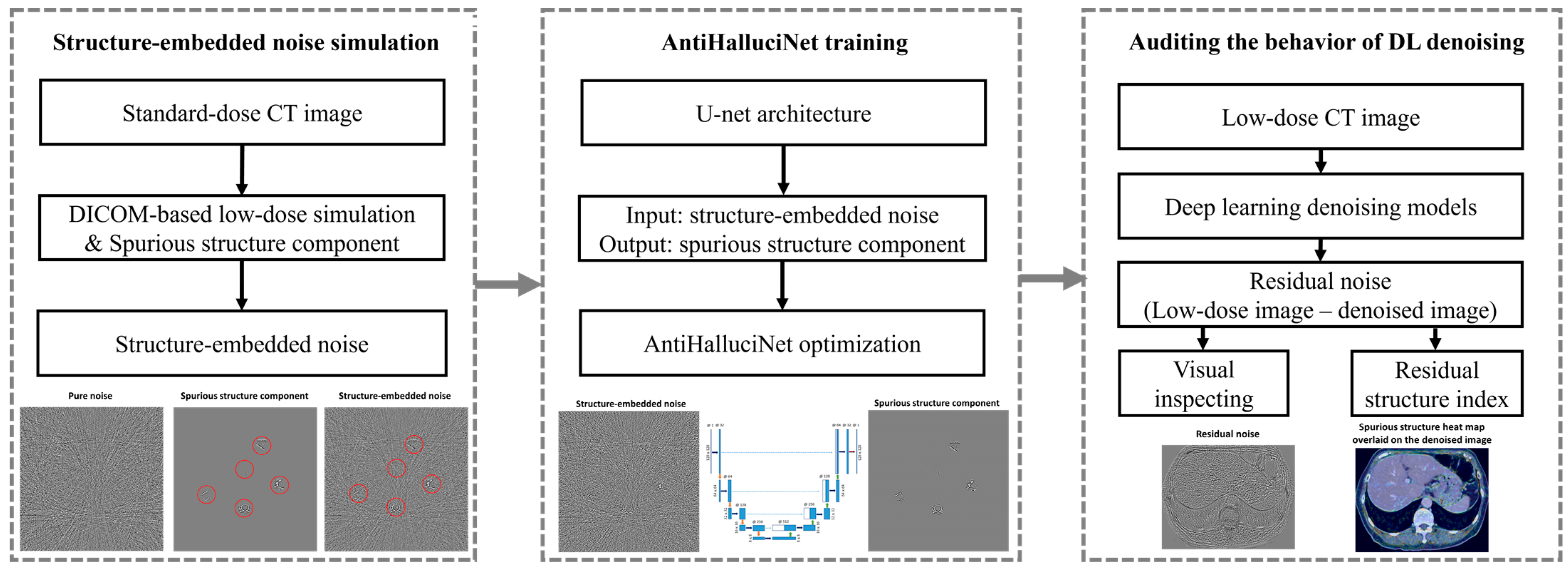
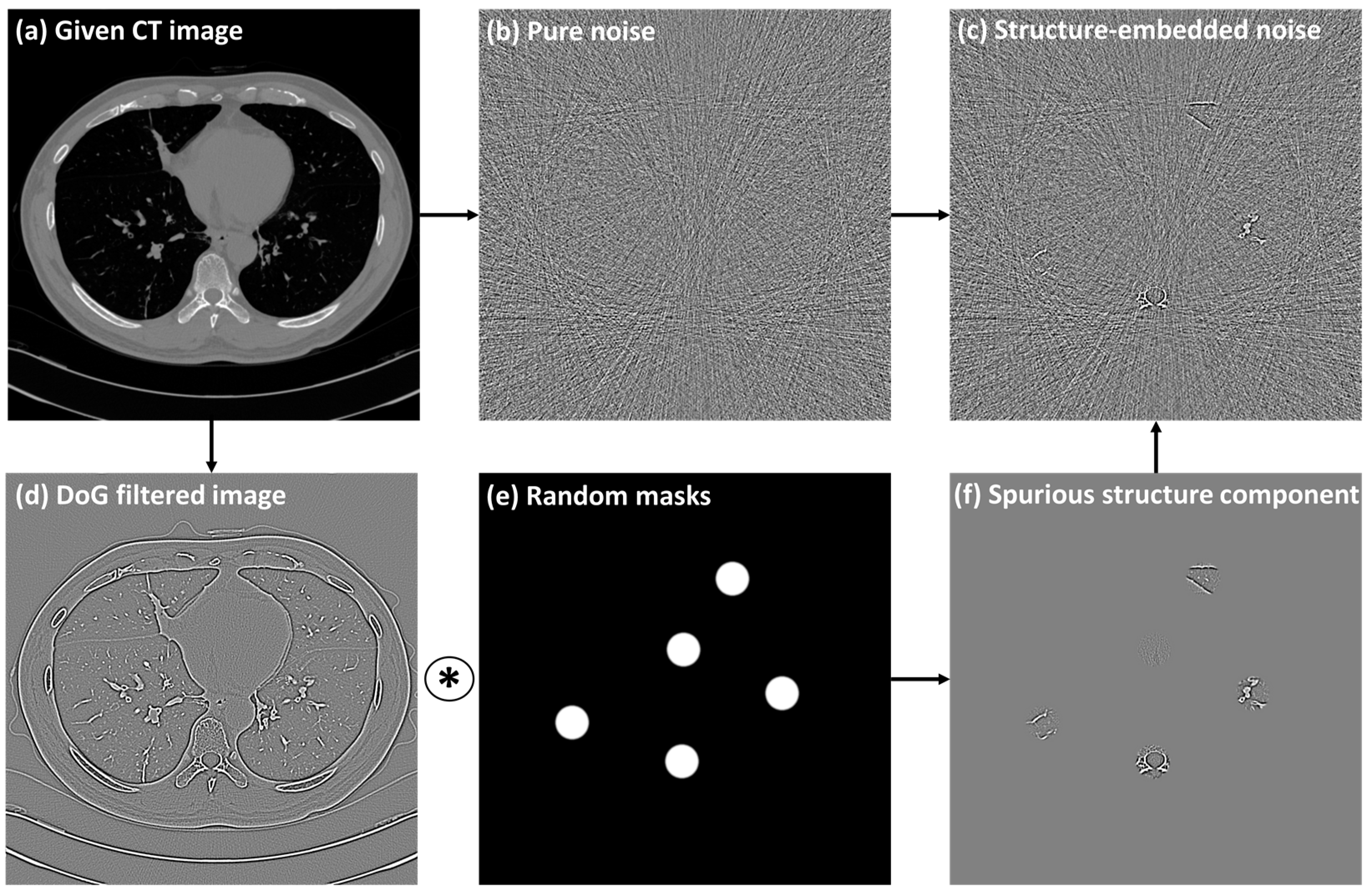
2.1. Generation of Paired Structure-Embedded and Pure Noise Images
2.1.1. Base Dataset
2.1.2. Generation of Simulated Low-Dose CT
2.1.3. Generation of Pure Noise Images
2.1.4. Generation of Structure-Embedded Noise Images
2.2. AntiHalluciNet
2.2.1. Training
2.2.2. Residual Structure Index
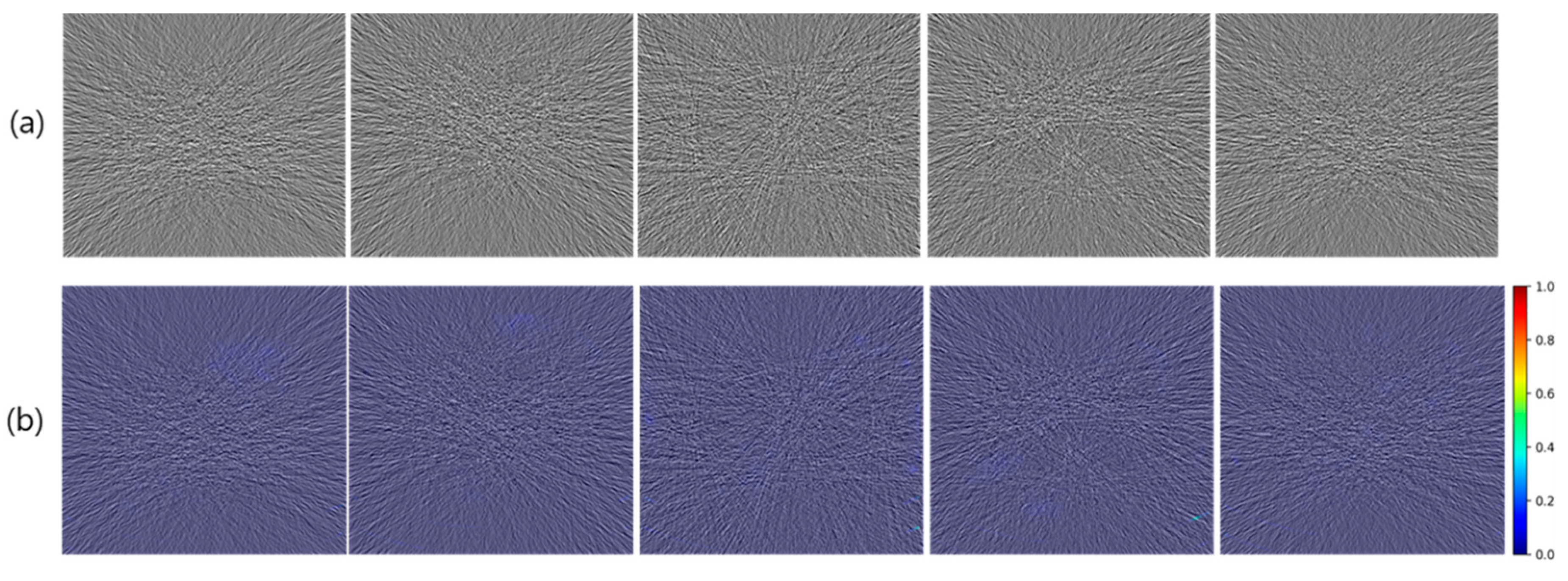
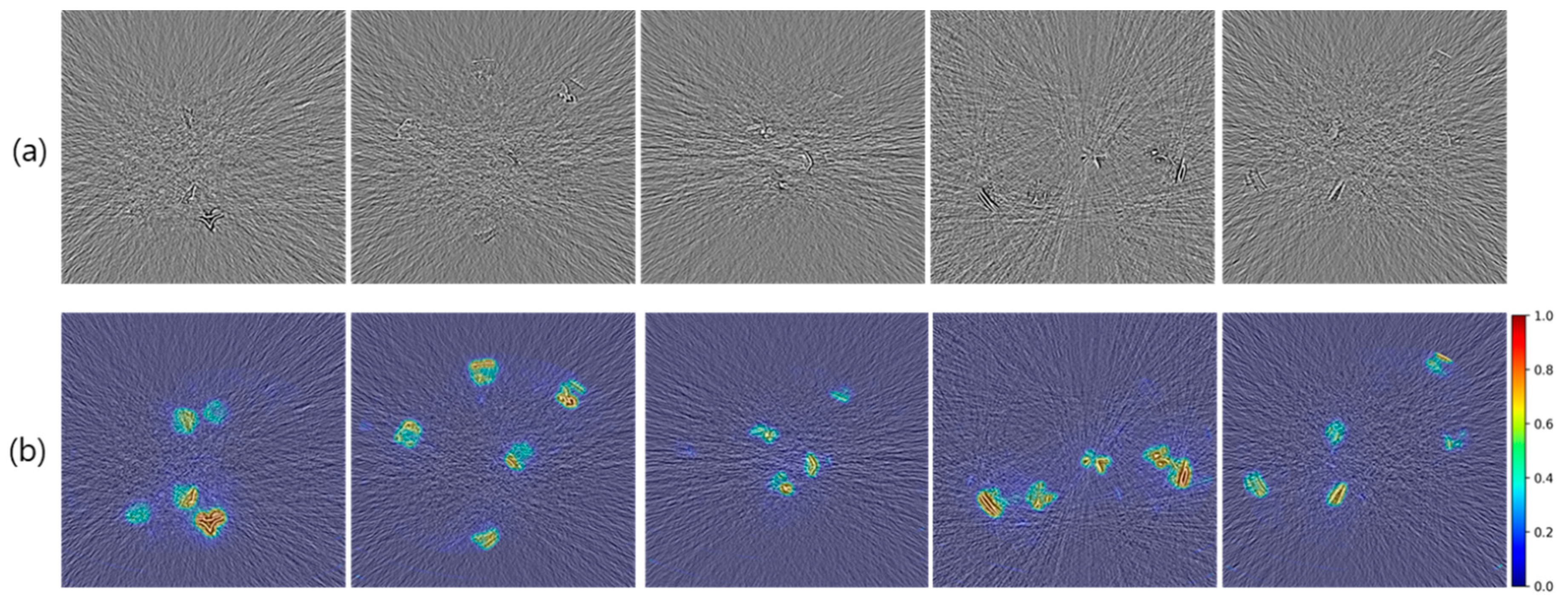
2.2.3. Performance Verification
2.2.4. Performance Comparison with SSIM
2.3. Auditing the Behavior of DL Denoising Models
2.3.1. DL Denoising Models
2.3.2. Real-World Evaluation Dataset
2.3.3. Auditing of DL Denoisers
3. Results
3.1. Generation of Structure-Embedded and Pure Noise Images
3.2. Verification of Prediction Performance with Heatmap
3.3. Verification of Prediction Performance with RSI Measurements
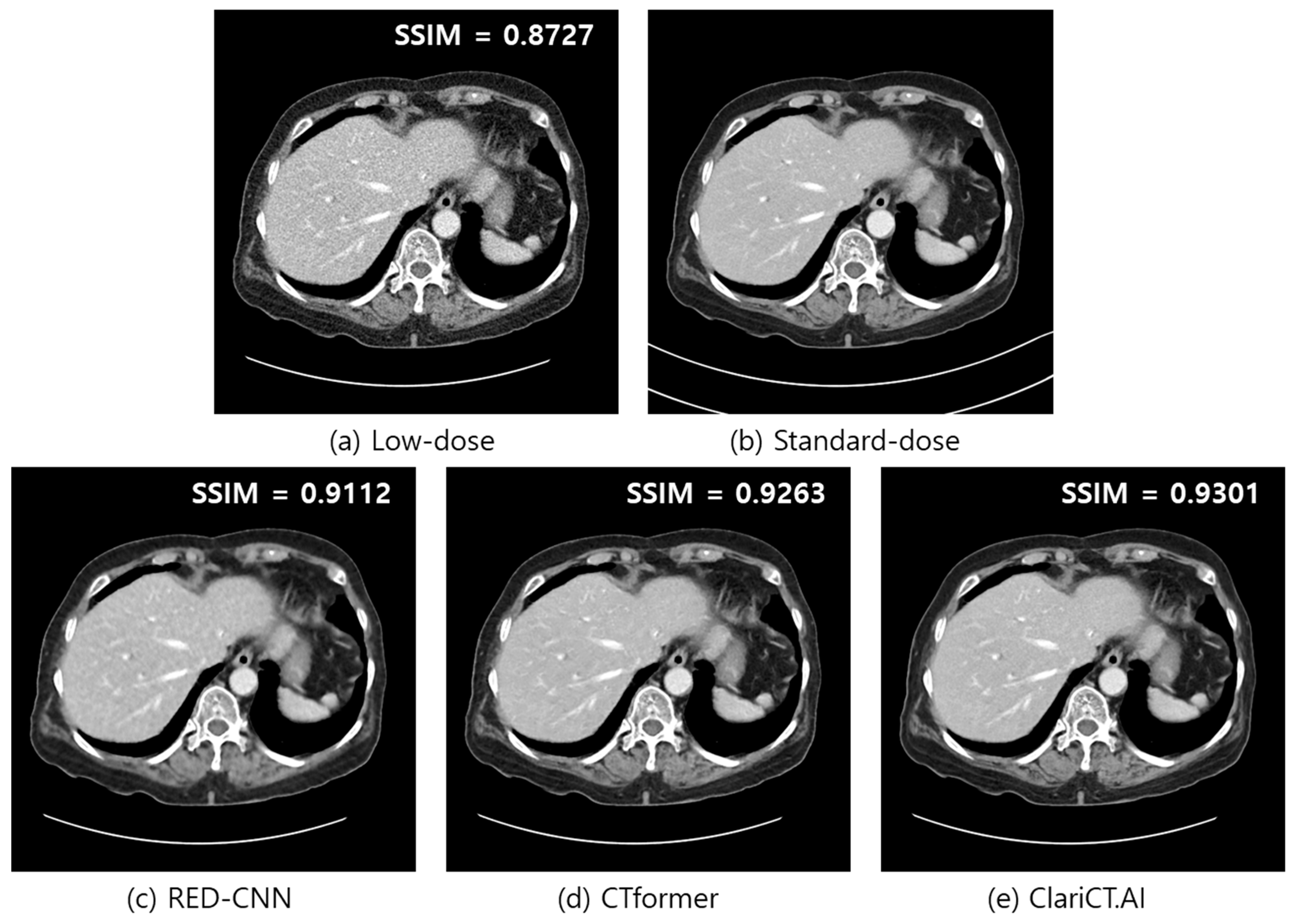
3.4. Performance Comparison with SSIM
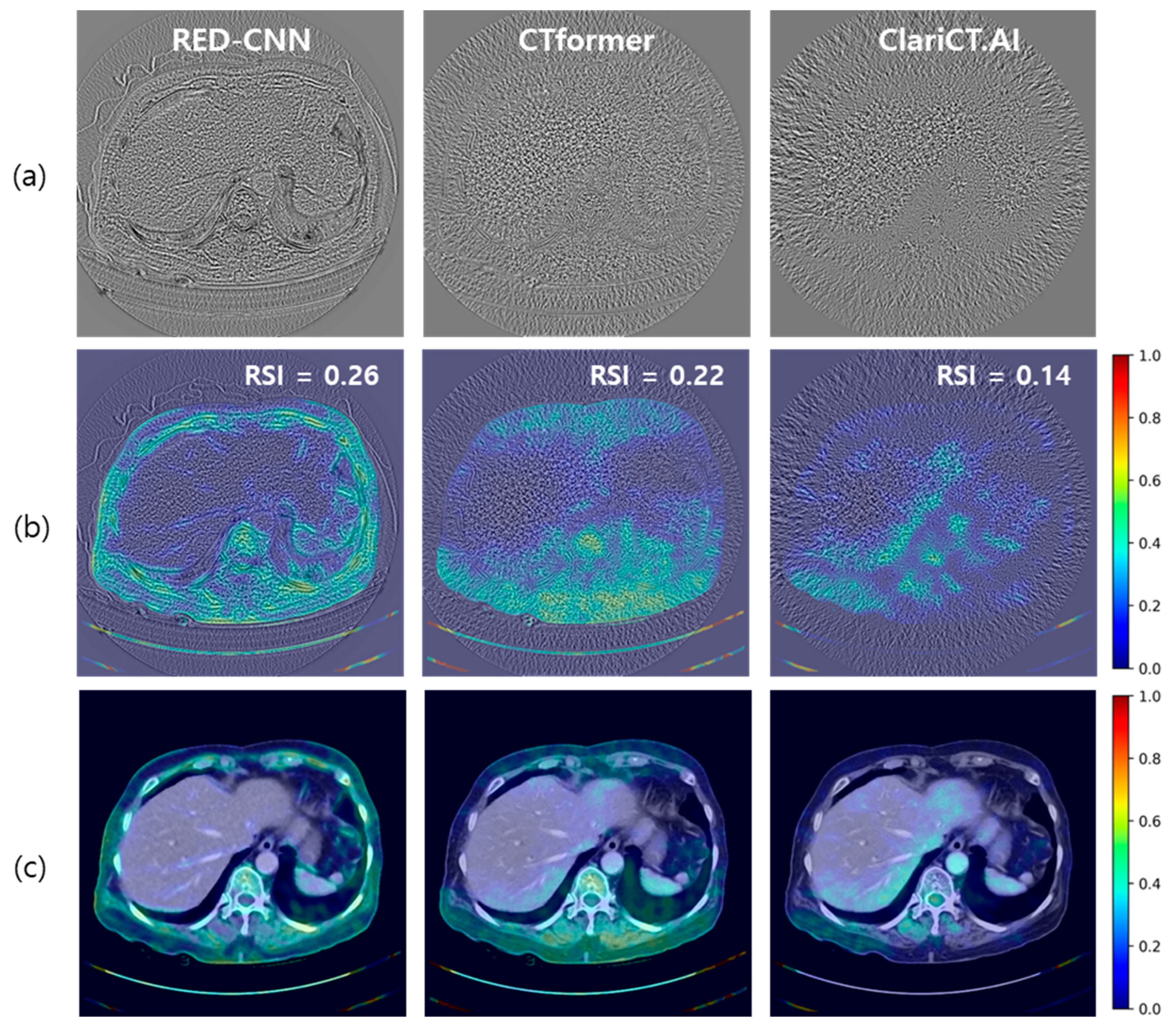
3.5. Auditing of DL Denoisers
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Smith-Bindman, R.; Miglioretti, D.L.; Larson, E.B. Rising Use of Diagnostic Medical Imaging in a Large Integrated Health System. Health Aff. 2008, 27, 1491–1502. [Google Scholar] [CrossRef] [PubMed]
- Brenner, D.J.; Hall, E.J. Computed Tomography—An Increasing Source of Radiation Exposure. N. Engl. J. Med. 2007, 357, 2277–2284. [Google Scholar] [CrossRef] [PubMed]
- Berrington De González, A.; Mahesh, M.; Kim, K.P.; Bhargavan, M.; Lewis, R.; Mettler, F.; Land, C. Projected Cancer Risks From Computed Tomographic Scans Performed in the United States in 2007. Arch Intern. Med. 2009, 169, 2071. [Google Scholar] [CrossRef] [PubMed]
- Smith-Bindman, R.; Lipson, J.; Marcus, R.; Kim, K.P.; Mahesh, M.; Gould, R.; Berrington De González, A.; Miglioretti, D.L. Radiation Dose Associated with Common Computed Tomography Examinations and the Associated Lifetime Attributable Risk of Cancer. Arch. Intern. Med. 2009, 169, 2078–2086. [Google Scholar] [CrossRef] [PubMed]
- Goo, H.W. CT Radiation Dose Optimization and Estimation: An Update for Radiologists. Korean J. Radiol. 2012, 13, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Liu, X.; Leng, S.; Kofler, J.M.; Ramirez-Giraldo, J.C.; Qu, M.; Christner, J.; Fletcher, J.G.; McCollough, C.H. Radiation Dose Reduction in Computed Tomography: Techniques and Future Perspective. Imaging Med. 2009, 1, 65. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Zhang, Y.; Kalra, M.K.; Lin, F.; Chen, Y.; Liao, P.; Zhou, J.; Wang, G. Low-Dose CT With a Residual Encoder-Decoder Convolutional Neural Network. IEEE Trans. Med. Imaging 2017, 36, 2524–2535. [Google Scholar] [CrossRef]
- Kang, E.; Min, J.; Ye, J.C. A Deep Convolutional Neural Network Using Directional Wavelets for Low-Dose X-Ray CT Reconstruction. Med. Phys. 2017, 44, e360–e375. [Google Scholar] [CrossRef]
- Bao, P.; Sun, H.; Wang, Z.; Zhang, Y.; Xia, W.; Yang, K.; Chen, W.; Chen, M.; Xi, Y.; Niu, S.; et al. Convolutional Sparse Coding for Compressed Sensing CT Reconstruction. IEEE Trans. Med. Imaging 2019, 38, 2607–2619. [Google Scholar] [CrossRef]
- Lecun, Y.; Bengio, Y.; Hinton, G. Deep Learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef]
- Choi, H.; Chang, W.; Kim, J.H.; Ahn, C.; Lee, H.; Kim, H.Y.; Cho, J.; Lee, Y.J.; Kim, Y.H. Dose Reduction Potential of Vendor-Agnostic Deep Learning Model in Comparison with Deep Learning–Based Image Reconstruction Algorithm on CT: A Phantom Study. Eur. Radiol. 2022, 32, 1247–1255. [Google Scholar] [CrossRef] [PubMed]
- Nam, J.G.; Ahn, C.; Choi, H.; Hong, W.; Park, J.; Kim, J.H.; Goo, J.M. Image Quality of Ultralow-Dose Chest CT Using Deep Learning Techniques: Potential Superiority of Vendor-Agnostic Post-Processing over Vendor-Specific Techniques. Eur. Radiol. 2021, 31, 5139–5147. [Google Scholar] [CrossRef] [PubMed]
- Belthangady, C.; Royer, L.A. Applications, Promises, and Pitfalls of Deep Learning for Fluorescence Image Reconstruction. Nat. Methods 2019, 16, 1215–1225. [Google Scholar] [CrossRef] [PubMed]
- Cruz, C.; Foi, A.; Katkovnik, V.; Egiazarian, K. Nonlocality-Reinforced Convolutional Neural Networks for Image Denoising. IEEE Signal Process Lett. 2018, 25, 1216–1220. [Google Scholar] [CrossRef]
- Bhadra, S.; Kelkar, V.A.; Brooks, F.J.; Anastasio, M.A. On Hallucinations in Tomographic Image Reconstruction. IEEE Trans. Med. Imaging 2021, 40, 3249. [Google Scholar] [CrossRef] [PubMed]
- Zeng, R.; Lin, C.Y.; Li, Q.; Jiang, L.; Skopec, M.; Fessler, J.A.; Myers, K.J. Performance of a Deep Learning-Based CT Image Denoising Method: Generalizability over Dose, Reconstruction Kernel, and Slice Thickness. Med. Phys. 2022, 49, 836–853. [Google Scholar] [CrossRef] [PubMed]
- Samei, E.; Bakalyar, D.; Boedeker, K.L.; Brady, S.; Fan, J.; Leng, S.; Myers, K.J.; Popescu, L.M.; Ramirez Giraldo, J.C.; Ranallo, F.; et al. Performance Evaluation of Computed Tomography Systems: Summary of AAPM Task Group 233. Med. Phys. 2019, 46, e735–e756. [Google Scholar] [CrossRef]
- Chow, L.S.; Rajagopal, H. Modified-BRISQUE as No Reference Image Quality Assessment for Structural MR Images. Magn. Reson. Imaging 2017, 43, 74–87. [Google Scholar] [CrossRef]
- Zhang, Z.; Dai, G.; Liang, X.; Yu, S.; Li, L.; Xie, Y. Can Signal-to-Noise Ratio Perform as a Baseline Indicator for Medical Image Quality Assessment. IEEE Access 2018, 6, 11534–11543. [Google Scholar] [CrossRef]
- Kim, C.H.; Chung, M.J.; Cha, Y.K.; Oh, S.; Kim, K.G.; Yoo, H. The Impact of Deep Learning Reconstruction in Low Dose Computed Tomography on the Evaluation of Interstitial Lung Disease. PLoS ONE 2023, 18, e0291745. [Google Scholar] [CrossRef]
- Wang, Z.; Bovik, A.C.; Sheikh, H.R.; Simoncelli, E.P. Image Quality Assessment: From Error Visibility to Structural Similarity. IEEE Trans. Image Process. 2004, 13, 600–612. [Google Scholar] [CrossRef] [PubMed]
- Mittal, A.; Soundararajan, R.; Bovik, A.C. Making a “completely Blind” Image Quality Analyzer. IEEE Signal Process Lett. 2013, 20, 209–212. [Google Scholar] [CrossRef]
- Mittal, A.; Moorthy, A.K.; Bovik, A.C. No-Reference Image Quality Assessment in the Spatial Domain. IEEE Trans. Image Process. 2012, 21, 4695–4708. [Google Scholar] [CrossRef] [PubMed]
- Venkatanath, N.; Praneeth, D.; Maruthi Chandrasekhar, B.H.; Channappayya, S.S.; Medasani, S.S. Blind Image Quality Evaluation Using Perception Based Features. In Proceedings of the 2015 21st National Conference on Communications, NCC, Mumbai, India, 27 February–1 March 2015. [Google Scholar] [CrossRef]
- Birch, P.; Mitra, B.; Bangalore, N.M.; Rehman, S.; Young, R.; Chatwin, C. Approximate Bandpass and Frequency Response Models of the Difference of Gaussian Filter. Opt. Commun. 2010, 283, 4942–4948. [Google Scholar] [CrossRef]
- Won Kim, C.; Kim, J.H. Realistic Simulation of Reduced-Dose CT with Noise Modeling and Sinogram Synthesis Using DICOM CT Images. Med. Phys. 2014, 41, 011901. [Google Scholar] [CrossRef] [PubMed]
- Othman, A.E.; Brockmann, C.; Yang, Z.; Kim, C.; Afat, S.; Pjontek, R.; Nikoubashman, O.; Brockmann, M.A.; Nikolaou, K.; Wiesmann, M.; et al. Impact of Image Denoising on Image Quality, Quantitative Parameters and Sensitivity of Ultra-Low-Dose Volume Perfusion CT Imaging. Eur. Radiol. 2016, 26, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Hepp, T.; Othman, A.; Liebgott, A.; Kim, J.H.; Pfannenberg, C.; Gatidis, S. Effects of Simulated Dose Variation on Contrast-Enhanced CT-Based Radiomic Analysis for Non-Small Cell Lung Cancer. Eur. J. Radiol. 2020, 124, 108804. [Google Scholar] [CrossRef]
- Afat, S.; Brockmann, C.; Nikoubashman, O.; Müller, M.; Thierfelder, K.M.; Brockmann, M.A.; Nikolaou, K.; Wiesmann, M.; Kim, J.H.; Othman, A.E. Diagnostic Accuracy of Simulated Low-Dose Perfusion CT to Detect Cerebral Perfusion Impairment after Aneurysmal Subarachnoid Hemorrhage: A Retrospective Analysis. Radiology 2018, 287, 643–650. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation; Lecture Notes in Computer Science (including subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics); Springer: Berlin/Heidelberg, Germany, 2015; Volume 9351, pp. 234–241. [Google Scholar] [CrossRef]
- Kingma, D.P.; Ba, J.L. Adam: A Method for Stochastic Optimization. In Proceedings of the 3rd International Conference on Learning Representations, ICLR 2015–Conference Track Proceedings, San Diego, CA, USA, 7–9 May 2015. [Google Scholar]
- Prakash, P.; Kalra, M.K.; Kambadakone, A.K.; Pien, H.; Hsieh, J.; Blake, M.A.; Sahani, D.V. Reducing Abdominal CT Radiation Dose with Adaptive Statistical Iterative Reconstruction Technique. Investig. Radiol. 2010, 45, 202–210. [Google Scholar] [CrossRef]
- Mileto, A.; Guimaraes, L.S.; McCollough, C.H.; Fletcher, J.G.; Yu, L. State of the Art in Abdominal CT: The Limits of Iterative Reconstruction Algorithms. Radiology 2019, 293, 491–503. [Google Scholar] [CrossRef]
- Solomon, J.; Mileto, A.; Ramirez-Giraldo, J.C.; Samei, E. Diagnostic Performance of an Advanced Modeled Iterative Reconstruction Algorithm for Low-Contrast Detectability with a Third-Generation Dual-Source Multidetector CT Scanner: Potential for Radiation Dose Reduction in a Multireader Study. Radiology 2015, 275, 735–745. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Fan, F.; Wu, Z.; Liu, R.; Wang, F.; Yu, H. CTformer: Convolution-Free Token2Token Dilated Vision Transformer for Low-Dose CT Denoising. Phys. Med. Biol. 2023, 68, 065012. [Google Scholar] [CrossRef] [PubMed]
- ClariPi Inc ClariCT.AI. Available online: https://www.accessdata.fda.gov/cdrh_docs/pdf21/K212074.pdf (accessed on 22 October 2023).
- McCollough, C.H.; Bartley, A.C.; Carter, R.E.; Chen, B.; Drees, T.A.; Edwards, P.; Holmes, D.R.; Huang, A.E.; Khan, F.; Leng, S.; et al. Low-Dose CT for the Detection and Classification of Metastatic Liver Lesions: Results of the 2016 Low Dose CT Grand Challenge. Med. Phys. 2017, 44, e339–e352. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.; Cho, E.; Kim, W.; Choi, H.; Beck, K.S.; Yoon, H.J.; Baek, J.; Choi, J.H. No-Reference Perceptual CT Image Quality Assessment Based on a Self-Supervised Learning Framework. Mach. Learn Sci. Technol. 2022, 3, 045033. [Google Scholar] [CrossRef]
- Gao, Q.; Li, S.; Zhu, M.; Li, D.; Bian, Z.; Lyu, Q.; Zeng, D.; Ma, J. Blind CT Image Quality Assessment via Deep Learning Framework. In Proceedings of the 2019 IEEE Nuclear Science Symposium and Medical Imaging Conference, NSS/MIC, Manchester, UK, 26 October–2 November 2019. [Google Scholar] [CrossRef]
- Li, S.; He, J.; Wang, Y.; Liao, Y.; Zeng, D.; Bian, Z.; Ma, J. Blind CT Image Quality Assessment via Deep Learning Strategy: Initial Study. Med. Imaging 2018, 10577, 293–297. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scanner 1 | Scanner 2 | Scanner 3 | Scanner 4 | |
|---|---|---|---|---|
| Number of cases (Train/Val) | 35/5 | 35/5 | 35/5 | 35/5 |
| Tube voltage (kV) | 120 | 100 | 100 | 100 |
| Mean tube current (mAs) | 135.4 ± 25.3 | 150.2 ± 24.7 | 149.7 ± 28.1 | 152.3 ± 30.6 |
| Reconstruction kernel | Standard | B | B30f | FC08 |
| Slice thickness (mm) | 2.5 mm | 3 mm | 3 mm | 3 mm |
| ROIs with Embedded Structure | ROIs without Structure | p-Value * | |
|---|---|---|---|
| 25% dose simulation | 0.36 ± 0.29 | 0.01 ± 0.02 | <0.001 |
| 50% dose simulation | 0.57 ± 0.31 | 0.02 ± 0.02 | <0.001 |
| 75% dose simulation | 0.83 ± 0.25 | 0.03 ± 0.03 | <0.001 |
| SSIM ↑↑ | RSI ↓↓ | |
|---|---|---|
| 25% mixing | 0.9333 ± 0.0133 | 0.27 ± 0.08 |
| 50% mixing | 0.9490 ± 0.0130 | 0.41 ± 0.08 |
| 75% mixing | 0.9579 ± 0.0146 | 0.48 ± 0.08 |
| 100% mixing | 0.9603 ± 0.0169 | 0.52 ± 0.07 |
| RSI ↓↓ | FR-IQA | NR-IQA | |
|---|---|---|---|
| SSIM ↑↑ | NIQE ↓↓ | ||
| RED-CNN | 0.28 ± 0.06 | 0.8725 ± 0.0279 | 9.58 ± 0.32 |
| CTformer | 0.21 ± 0.06 | 0.8917 ± 0.0254 | 9.93 ± 0.30 |
| ClariCT.AI | 0.15 ± 0.03 | 0.9005 ± 0.0248 | 9.06 ± 0.27 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahn, C.; Kim, J.H. AntiHalluciNet: A Potential Auditing Tool of the Behavior of Deep Learning Denoising Models in Low-Dose Computed Tomography. Diagnostics 2024, 14, 96. https://doi.org/10.3390/diagnostics14010096
Ahn C, Kim JH. AntiHalluciNet: A Potential Auditing Tool of the Behavior of Deep Learning Denoising Models in Low-Dose Computed Tomography. Diagnostics. 2024; 14(1):96. https://doi.org/10.3390/diagnostics14010096
Chicago/Turabian StyleAhn, Chulkyun, and Jong Hyo Kim. 2024. "AntiHalluciNet: A Potential Auditing Tool of the Behavior of Deep Learning Denoising Models in Low-Dose Computed Tomography" Diagnostics 14, no. 1: 96. https://doi.org/10.3390/diagnostics14010096
APA StyleAhn, C., & Kim, J. H. (2024). AntiHalluciNet: A Potential Auditing Tool of the Behavior of Deep Learning Denoising Models in Low-Dose Computed Tomography. Diagnostics, 14(1), 96. https://doi.org/10.3390/diagnostics14010096