1. Introduction
Transvaginal ultrasonography (TVUS) is the primary diagnostic modality in investigating endometriomas. Usually, this technique can provide enough information for adequate preoperative planning [
1]. However, endometriomas share some imaging features with functional hemorrhagic ovarian cysts (HOCs) [
2]. Correctly distinguishing the two lesions is vital not only to avoid unnecessary surgery [
3] but also because endometriomas are a sign of the presence of other endometriotic lesions at the pelvic and intestinal levels, which can cause a series of complications [
4]. As a result, the imaging distinction between the two lesions strongly impacts the course of both medical and surgical treatment [
5].
Since it was first described more than 25 years ago [
6], the classic “ground glass” appearance of endometriomas has been constantly reevaluated; because of this, researchers have assigned it different levels of diagnostic utility [
7,
8,
9,
10] and even integrated it into decision trees, along with other ultrasonographic, clinical, and biological parameters [
11]. The ultrasound (US) appearance of endometriomas is highly variable, being influenced by the time-lapse of blood degradation [
12]. Moreover, the US features of endometriomas overlap with other lesions such as dermoids, cystic adnexal lesions complicated by bleeding, and cystic ovarian neoplasms [
13]. Often, endometriomas and HOCs are indistinguishable, especially in the early stages [
2], as they share the characteristic of a cystic mass with bloody content [
14]. For these reasons, recent studies [
15] concluded that only 60% of endometriomas larger than 2 cm can be appropriately diagnosed with US.
Furthermore, the variety of ultrasound-based descriptors and scoring systems may cause confusion, particularly because their parameters are changeable, sophisticated, and frequently of arbitrary importance [
16,
17]. Furthermore, the interpretation of medical images is always subjective and observer-dependent [
18].
Computer-aided discrimination (CAD) systems have emerged in recent years and attempt to overcome these limitations and increase confidence in the US detection and characterization of ovarian masses [
19]. Some of the recently developed CAD techniques focus on the US identification of ovarian malignancies [
20,
21,
22,
23,
24] and mostly rely on texture analysis (TA) to autonomously detect the presence of a disease based on grayscale variations within TVUS images [
25]. TA is a method for extracting and processing parameters that describe pixel intensity and variation patterns, resulting in a quantitative and comprehensive representation of image content [
26,
27]. The basic concept of texture analysis of ultrasound images is that a diseased process that affects the tissue produces an altered signal, which gives textural features different values than those of the normal structure [
28].
This is the first study to provide an ultrasound-based texture characterization of endometriomas and HOCs. We investigated whether texture parameters could be used as an objective diagnostic criterion for distinguishing between the two lesions and whether these parameters were able to outperform the classic US features.
2. Materials and Methods
2.1. Study Group
This Health Insurance Portability and Accountability Act–compliant, a single-institution, retrospective pilot study, was approved by the institutional review board, and informed consent was waived because of its retrospective nature. From September 2017 to March 2019, a keyword search (using the terms “hemorrhagic + cyst”, alternatives and combinations) in the imaging database of our institution was conducted to identify TVUS images corresponding to ovarian cystic lesions. The keyword search resulted in 235 image reports. Each report was analyzed by one researcher, who excluded all studies that referred to previously documented ovarian malignant or benign tumors (other than endometriomas) (n = 57), lesions that were described as having features strongly suggesting malignancy (n = 31), and lesions that measured less than 2 cm (n = 28). The medical records of the remaining 119 patients were retrieved from the archive of our healthcare institution and investigated for disease-related data. Further, all patients that were transferred to another institution (n = 19) and all lesions that were not removed and did not undergo histopathological analysis were also excluded (n = 33). The US examinations of the remaining 67 patients were reviewed by one gynecologist who selected only B-mode images that were not affected by artifacts or technique errors. After applying these criteria, US images from 30 endometriomas and 26 hemorrhagic cysts were selected.
2.2. Reference Standard
All included lesions underwent pathological analysis after surgical removal. For endometriomas, 12 lesions were removed and analyzed, along with subsequent diseases (uterine fibromatosis, n = 9; adenomyosis, n = 3). All HOCs underwent pathological analysis because they were included in the surgical specimen analyzed for another condition (atypical endometrial hyperplasia, n = 1; adnexal torsion, n = 2; uterine leiomyosarcoma, n = 2; mucinous cystadenoma, n =2; cystadenofibroma, n = 3; serous ovarian carcinoma, n = 3; serous cystadenomas, n = 3; ovarian teratoma, n = 4; uterine fibromatosis, n = 6).
For pathological analysis, a solution of 10% buffered formalin was used to fixate the surgical samples overnight. Further, using tissue processors, the samples were embedded in paraffin according to the standard protocol of the pathological anatomy laboratory of our institution. The resulting samples were sectioned at 5 µm and stained with hematoxylin and eosin. All resulting samples underwent examination by a pathologist with 9 years of experience in gynecological disease. Following the analysis workflow, a final diagnosis was possible in all the included cases.
2.3. Image Acquisition and Interpretation
All the included images were acquired by four gynecologists with at least 8 years of experience in gynecological ultrasound. All examinations were performed on the same machine (Aplio 300, Toshiba Medical Systems, Tokyo, Japan) using a dedicated endovaginal probe (4–10 MHz).
In the first step of image interpretation, each examination was reviewed by one researcher (R.A.Ș.) who was aware of the patients’ pathological findings, clinical outcomes, and final diagnoses. The medical data were cross-referenced with the images to ensure the selection of only the lesions that underwent pathological analysis. Respective lesions were marked, and only one image that was considered representative from each examination was retrieved and anonymized.
In the second step, the typical greyscale US characteristics of endometriomas (“a cyst with internal homogeneous low-level echoes, a perceptible …, no solid component, and a maximum of five locules for multilocular lesions”), as described by Collins et al. [
12], were quantified using anonymized images by another researcher (A.M.M.) who was also blinded to the patients’ outcomes. The homogeneous low-level echoes (or ground glass) appearance was considered if this was the dominant pattern in more than 90% of the lesion’s content. The lesions were considered to have a wall if a structure at least 2 mm thick that surrounded at least 50% of the visible portion of the cyst could be observed. Since only gray-scale images were retrieved, any structure that was adjacent to the walls was considered a solid component (including hyperechoic foci, papillary projections, and retracting clots). Furthermore, unilocular lesions were also considered to have a maximum of five locules.
2.4. Statistical Analysis
To quantify the information in a quantitative way, for each lesion, each ultrasound parameter was given the value of “1” if present or “0” if absent. A multiple regression (multivariate) analysis was conducted to investigate which ultrasound features could independently predict the presence of endometriomas. The analysis was conducted using the “enter” input model, which involved entering all variables into the model in one single step. A conventional p-value of less than 0.05 was used to determine the corresponding independent variables that contributed significantly to the differentiation of endometriomas from HOCs, whereas variables with a p-value of more than 0.01 were omitted. In addition, the coefficient of determination (R2, the proportion of the variation in the dependent variable explained by the regression model, measuring of the goodness of fit of the model), the R2-adjusted coefficient (the coefficient of determination adjusted for the number of independent variables in the regression model), the multiple correlation coefficient (measuring how tightly the data points clustered around the regression plane, calculated by taking the square root of the coefficient of determination), and the variance inflation factor (VIF, an indicator of multicollinearity) were calculated. After the analysis, the predicted values were saved and then used in a receiver operating characteristic (ROC) analysis to determine the prediction model’s ability to identify endometriomas. The ROC analysis was also used to test the ability of each ultrasound feature in the diagnosis of endometriomas. The DeLong et al. technique was used to compute the ROC curves, and the binomial exact confidence intervals for the areas under the curve (AUC) were stated. The optimal cut-off values for predicting patients with malignancies were determined using a common optimization step that maximized the Youden index (J). Specificity (Sp) and sensitivity (Se) were calculated from the same data, without other adjustments, using a 95% confidence interval (CI).
2.5. Texture Analysis Protocol
The radiomics approach consisted of five steps: image pre-processing, lesion segmentation, feature extraction, feature selection, and prediction.
2.5.1. Image Pre-Processing and Segmentation
Images were retrieved in Digital Imaging and Communications in Medicine (DICOM) format and were further converted into Joint Photographic Experts Group format (JPG) and imported into a dedicated software (Topaz DeNoise AI, Topaz Labs, TX, USA) in which the negative impact of the speckle noise was reduced using a denoising technique based on convolutional neural networks [
29]. Afterward, images were reconverted into bitmap format and transferred to a dedicated texture analysis software (MaZda, Institute of Electronics, Technical University of Lodz, Lodz, Poland) [
30]. Using this program, the image grey levels were normalized based on the mean and three standard deviations of grey level intensities to reduce the contrast and brightness variations.
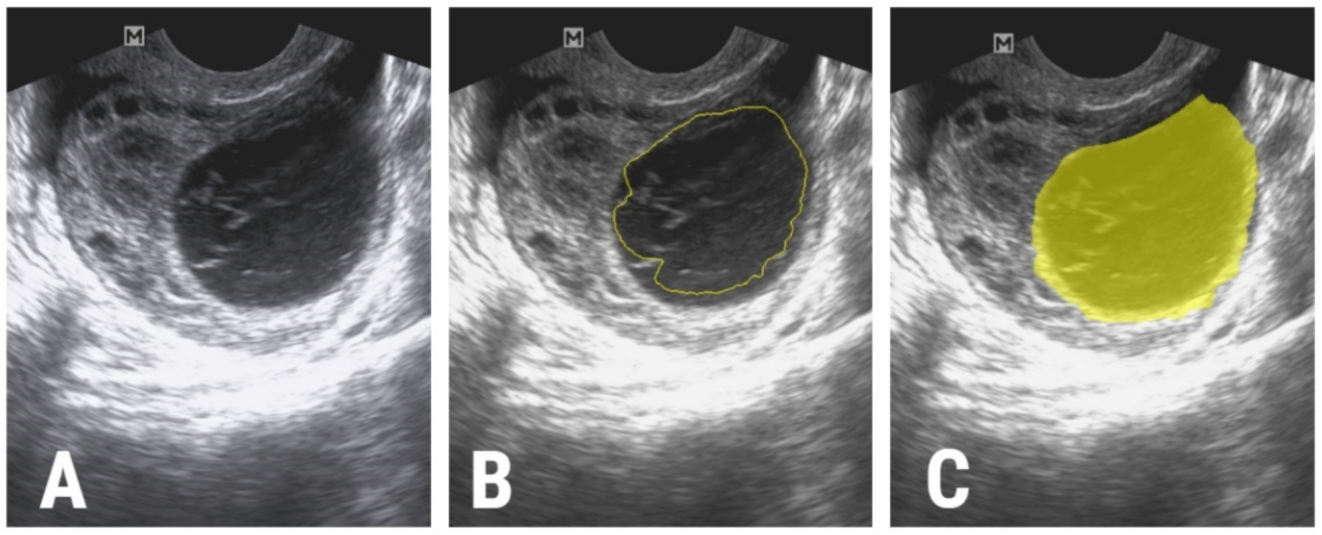
The image segmentation process was performed by a second researcher (P.A.Ș.) who was blinded to the outcomes of the patients. The researcher incorporated each lesion into a two-dimensional region of interest (ROI). The first step of the ROI definition process was performed semi-automatically. The researcher drew a circle inside each lesion and the software automatically delineated the structure of interest based on gradient and geometry coordinates. In the second step, if a complete overlap between the ROI and the structure’s contours was detected, the ROI was manually adjusted (
Figure 1).
2.5.2. Feature Extraction
The texture features (or parameters) were automatically extracted by the software after the definition and positioning of each ROI. From each lesion, a total of 275 parameters were computed [
31]. The parameters are described in
Table 1.
For each lesion, the segmentation and extraction of texture parameters were repeated 1 week apart, and the process was carried out by the same researcher. The resulting values were used to evaluate the intra-reader agreement using the intraclass coefficient.
2.5.3. Feature Selection
In order to identify the best-suited texture parameters for differentiating between the two histopathological groups, three methods were applied successively. The first step comprised of applying three reduction methods (based on mutual information (MI), Fisher coefficients (F, the ratio of between-class to within-class variance), and the probability of classification error and average correlation coefficients (POE + ACC)) [
32]. Each of the three selection methods provided a set of ten unique parameters.
Second, the intraclass correlation coefficient (ICC) was calculated using the absolute agreement between the same rater for the all-subjects model, and average values along with the 95% confidence interval were reported. Features that demonstrated an ICC of below 0.85 were excluded from further analysis.
Third, the absolute values of the remaining parameters were compared between the two groups using the Mann–Whitney U test. The statistically significant level was set at a p-value of below 0.0016 after Bonferroni correction (which implied dividing the classic 0.05 level by 30, considering the 27 unique parameters that resulted after applying the reduction techniques as well as age and the two separate histopathological entities). All texture parameters that showed univariate analysis results below this threshold were excluded from further processing.
2.5.4. Class Prediction
To investigate which of the previously selected texture features were independent predictors of endometriomas, a multiple regression analysis was performed following the same computational method as was used for the ultrasound features. Furthermore, features with a VIF greater than 10
4 were withdrawn from further testing because a high VIF value indicates multicollinearity. The predicted values were saved and then used in an ROC analysis to determine the prediction model’s ability to identify endometriomas. The ROC analysis was also used to test the diagnostic utility of the features that were independently associated with endometriomas, following the same workflow as described for the ultrasound features. Statistical analysis was performed using a commercially available dedicated software, MedCalc version 14.8.1 (MedCalc Software, Mariakerke, Belgium). The workflow model is summarized in
Figure 2.
3. Results
Fifty-six patients (average age ± standard deviation: 38.27 ± 14.68 years; age range: 22–54 years) were included according to their final diagnosis. Patients were divided into an endometrioma group (n = 30) and an HOC group (n = 26).
When analyzing the gray-scale features, three out of four characteristics (internal homogeneous low-level echoes, a perceptible wall, and a maximum of five locules) were independently associated with endometriomas (
Table 2). The multivariate analysis showed a significance level of
p < 0.0001, an R
2 coefficient of determination of 0.3856, an adjusted R
2 value of 0.3384, and a multiple correlation coefficient of 0.621. The diagnostic performance of the three independent US features and the prediction model is displayed in
Table 3.
For the texture analysis, one variation of the difference of variance parameter (CN5D6DifVarnc) was selected by both the Fisher and POE + ACC methods, while two variations of the same feature (CN4D6DifVarnc and CH5D6DifVarnc) were highlighted by both the Fisher and MI methods. In total, 27 unique parameters resulted after applying the three reduction techniques. The results of the univariate analysis and intra-reader agreement evaluation are displayed in
Table 4.
Twenty parameters showed statistically significant results in the univariate analysis and underwent multiple regression analysis. The parameter CN4D6DifVarnc was excluded from the analysis because it had a VIF greater than 10
4. The multivariate analysis showed a significance level of
p < 0.001, an R
2 coefficient of determination of 0.435, an adjusted R
2 value of 0.427, and a multiple correlation coefficient of 0.634. The multiple regression analysis identified seven parameters as independent predictors of endometriomas (
Table 5).
The ROC analysis showed that the prediction model exceeded the individual diagnostic ability of all independent features in terms of both sensitivity and specificity (
Table 6,
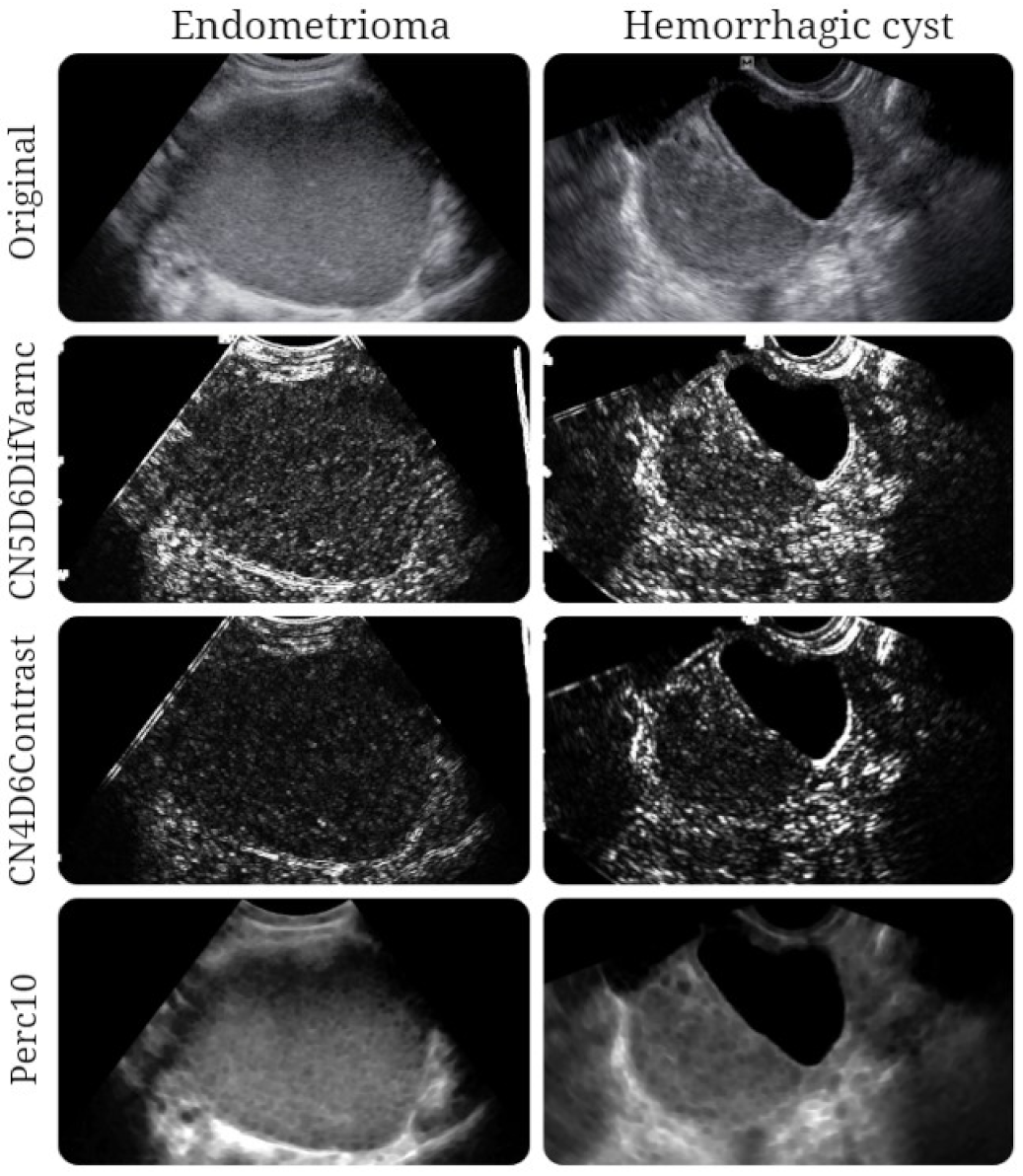
Figure 3). The texture maps that display the distribution of selected texture features in images from each entity are shown in
Figure 4.
4. Discussion
Our results showed that the majority of the included endometriomas (
n = 23) expressed low-level internal echoes, while this indicator was encountered in less than 30% of HOCs (
n = 7). As expected, this feature was the most distinctive sign of endometriomas, as previously described since the first research was conducted in the field (
Table 7). However, we were unable to find a study that specifically aimed to address the distinction between endometriomas and HOCs based on grey-level ultrasound features, with most research focusing on distinguishing endometriomas from other ovarian tumors (sometimes including HOCs) [
7,
11]. In our study, the low-level internal echoes (or ground glass appearance) showed similar sensitivity (74.19%) but lower specificity for the diagnosis of endometriomas compared with the most recent research in the field (73% Se; 94% Sp) [
11]. Moreover, when other features were added to the model, the overall sensitivity did not increase.
Hemorrhagic ovarian cysts are caused by bleeding inside functional cysts that are spontaneously resorbed [
2]. They also progress slowly through different stages of acute hemorrhage, clot development, and retraction, resulting in a shifting sonographic appearance until they fully resolve in 6 weeks or shrink significantly in size [
33]. In the early stages, they appear as solid masses with thin walls. Furthermore, their content may express variable echogenicity with reticular strands. When the clot retracts, its attachment to the wall can mimic a papillary projection, and a fluid layer also develops within the cyst [
34].
At the beginning of their formation, the US appearance of endometriomas can be indistinguishable from that of HOCs. In time, as the bleeding becomes chronic, endometriomas build up more hemorrhagic debris [
2], which is responsible for their classic US appearance (of a “unilocular cyst with fluid content expressing ground glass echogenicity” or “ground glass”) [
35,
36]. However, further research [
11] demonstrated that less than 50% of endometriomas exhibit these characteristics, with even lower rates in the postmenopausal population. This is most likely because endometriomas express cyclic bleeding, which results in different time stages of blood degradation, thereby generating variable US appearance [
37].
In practice, the grayscale imaging of endometriomas and HOCs can be identical due to bleeding features of different ages, making distinction difficult [
2]. On one hand, sonographic observation of fibrin strands and/or retracting clots within an adnexal cyst reflects a recent episode of hemorrhage [
35]. Due to the cyclic bleeding characteristic of endometriomas, the appearance of fibrin stands can easily mimic the features of an HOC [
38]. On the other hand, HOCs can also demonstrate diffuse low-level internal echoes [
7], most likely because in some cases, they do not regress and instead accumulate various quantities of intracellular deoxyhemoglobin and methemoglobin [
39].
Considering the information above, together with the subjective nature of the interpretation of US images, a clear differentiation between the two lesion types can be performed only through microscopic evaluation [
40]. The cell population found within endometriomas consists of degenerate erythrocytes, hemosiderin-laden macrophages, and endometrial and epithelial cells [
41,
42,
43,
44]. Functional hemorrhagic cysts’ content is composed of a mixture of blood products along with plasma proteins, mucopolysaccharides, and hyaluronic acid [
45], and these lesions also have rich cellularity [
43]. It is possible that all the histopathological characteristics are reflected within US images, subtly influencing the pixel intensity and distribution, which may be detected and quantified through texture parameters.
Our results showed that five variations of the difference of variance parameter were independent predictors of endometriomas (CN5D6DifVarnc, CV5D6DifVarnc, CZ3D6DifVarnc, CZ4D6DifVarnc, and CZ5D6DifVarnc). The variance is a measure of contrast severity, which can be used to create descriptors of relative smoothness. [
46]. The difference of variance measures the variance of the difference of grey level values (reflecting the randomness within an image [
47,
48]. In all scenarios, this feature exhibited higher values for HOCs than for endometriomas.
The contrast parameter shows the local variations present in an image, expressing higher values when an image contains a large number of pixels with different grey level values [
47]. We obtained higher values for the HOCs than for endometriomas.
The first-order histogram parameters (mean, standard deviation, variance, skewness, kurtosis, and percentiles) reflect the value of the pixel intensity, without considering the spatial relations between the pixels [
49]. The percentile number (
n) is the point in the histogram where
n% of the pixel values are found to the left [
50]. A percentile, in other words, is the highest grey level value at which a given percentage of the pixels in an image are contained [
51]. This signifies that 10% of the pixels within images were distributed under higher values for endometriomas than for HOCs.
Although it was expected that endometriomas would show a higher degree of echogenic randomness because of the multitude of contained elements, the parameters indicating these characteristics showed higher values for HOCs. This observation is in accordance with the literature, which indicates that HOCs have more complex and heterogenous content on TVUS (probably because they more often express fine linear strands and retracting clots) [
52].
In the current study, the texture model was able to diagnose endometriomas with almost perfect rates: 100% Se (CI, 88.4–100%) and 100% Sp (CI, 75.3–100%). In a similar study, based on magnetic resonance (MRI) images [
53], the texture model was able to distinguish endometriomas from HOCs with similar rates, showing a sensitivity of 100% (CI, 85.8–100%) and a specificity of 100% (CI, 71.5–100%). Once again, this model [
53] outperformed the classic MRI features of endometriomas (“T2 shading”, 75.86% Se and 35.71% Sp and “T2 dark spots”, 55.17% Se and 64.29% Sp). However, the current model comprised different texture parameters (five variations of difference of variance, image contrast, and 10th percentile) compared to those extracted from MRI images (which included mostly variations of entropy) [
53]. The high accuracy rates accomplished by both models could indicate that TA is feasible in distinguishing the two lesions in both types of imaging examinations. However, these excellent results may be influenced by the reduction techniques (especially the Fisher method); although they provide the most distinguishing parameters, these parameters are highly correlated [
32], and they could therefore influence the diagnostic value of the prediction model [
54]. In order to at least partially counteract this effect, in addition to the Fisher method, two other selection methods were used that did not provide parameters with a high degree of correlation (POE + ACC and Mutual Information). Moreover, parameters that showed statistical significance in the univariate analysis but also demonstrated a VIF >10
4 were excluded from the final model.
Because the ultrasound features of the two lesions may overlap, sometimes the diagnosis cannot be straightforward. Our TA model may be useful in providing more confidence in the diagnosis of a newly discovered bleeding ovarian lesion. Moreover, if this approach is further validated, it could offer an alternative to more expensive and time-consuming approaches for characterizing adnexal lesions, such as MRI examinations. However, the role of MRI in the characterization of endometriomas will not be diminished since some lesions could remain inapparent to TVUS despite the visualization of the ovaries because of their location or the presence of periovarian adhesions [
55].
Our study had several limitations. Due to the retrospective design and the decision to include only pathologically proven lesions, the study may possess selection and verification bias. In the final step of patient selection, all lesions below 2 cm (
n = 33) were excluded. This threshold was necessary to provide a sufficient area for the software to analyze and extract the pixel pattern. Therefore, the study population was relatively low. The small population was also due to the limited time approved for this research by the ethics committee and the strict exclusion and inclusion criteria. The menstrual phase, CA-125 levels, and menopausal status were not reported since they were inconsistently mentioned in the retrieved medical data. Few of the selected patients had Doppler images stored in our database; therefore, only grey scale images were selected. For this reason, other classic features of endometriomas, such as no internal vascularity and avascular internal nodules [
12], could not be quantified. However, the use of color Doppler imaging does not improve the diagnostic accuracy of transvaginal ultrasonography alone in the diagnosis of ovarian endometrioma [
56]. On the other hand, it is documented that the presence of intracystic vascularization poses doubts about malignancy [
57]. However, this was not the case for selected lesions, as the pathological analysis did not raise suspicions of malignancy in any case. A limitation was that one investigator was aware of the final diagnoses of the lesions. However, since many patients had several adnexal lesions at the time of the US evaluation, this strategy was necessary for selecting only documented lesions. This researcher was not involved in the image segmentation, statistical analysis, or reporting of the results after this point. Considering these limitations and the pilot nature of this research, the presented TA model for discriminating endometriomas from HOCs requires prospective research for both validation and establishment of its clinical utility compared with the classic imaging methods.


 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}