
In Vivo Verification of Treatment Source Dwell Times in Brachytherapy of Postoperative Endometrial Carcinoma: A Feasibility Study

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Analysis
2.2. Repeatability
2.3. Long-Term Stability
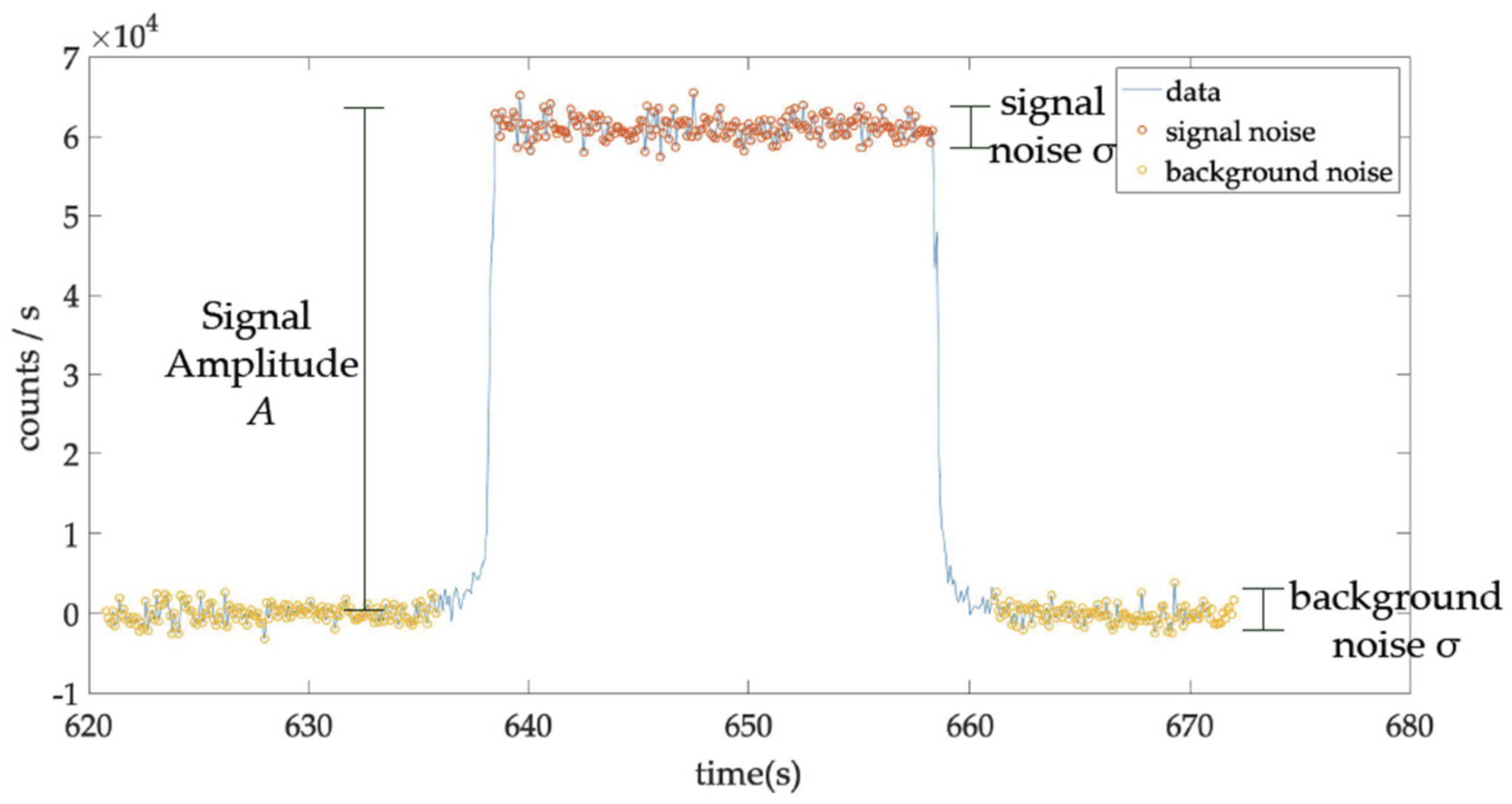
2.4. Signal-to-Noise Ratio
2.5. Linearity of PSD Total Counts with Dwell Time (Absorbed Dose)
2.6. Linearity of PSD Count Rate with Absorbed Dose Rate
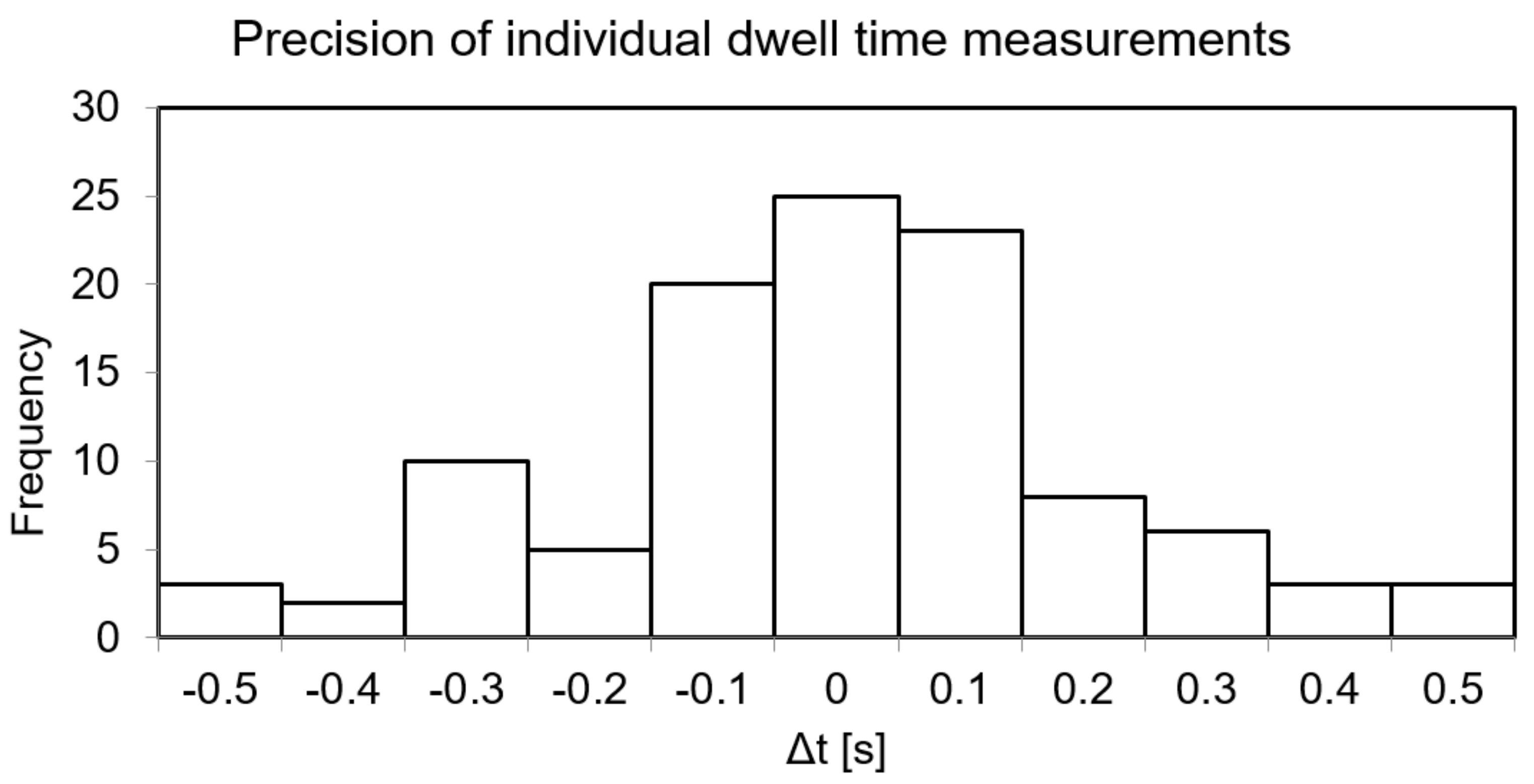
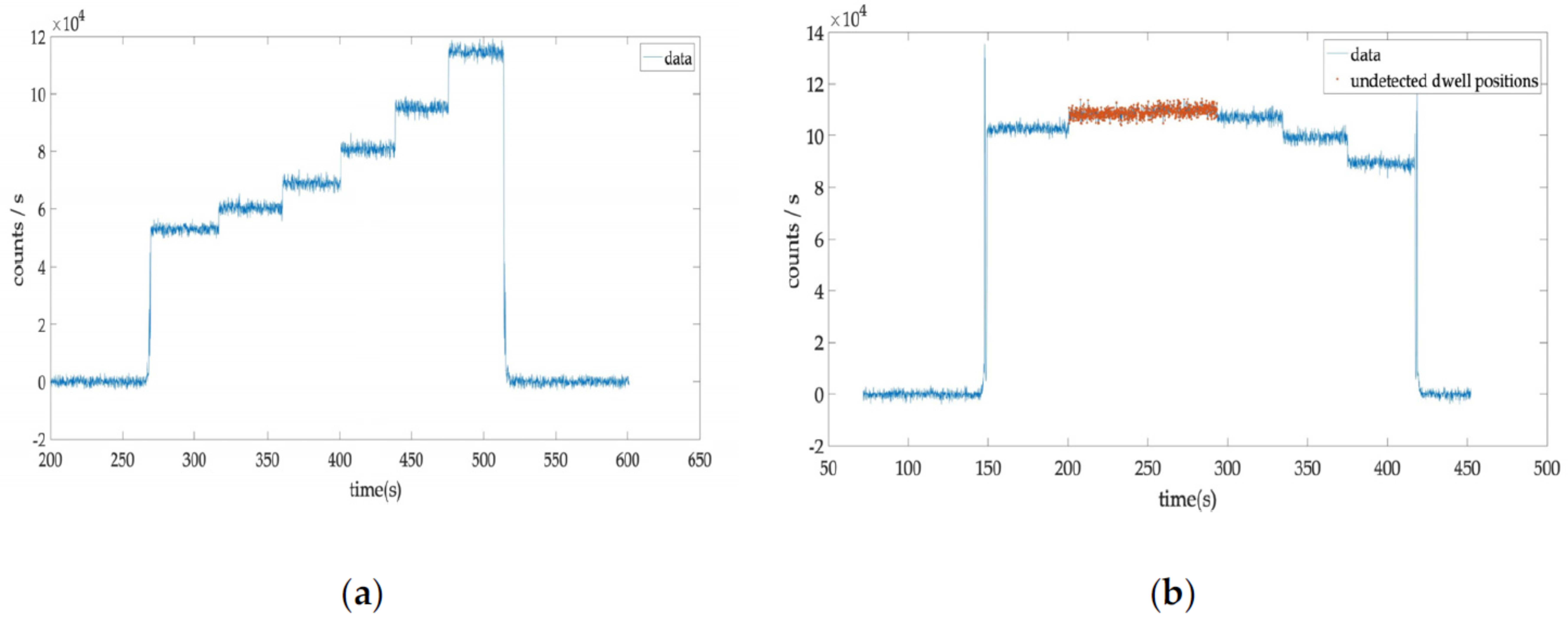
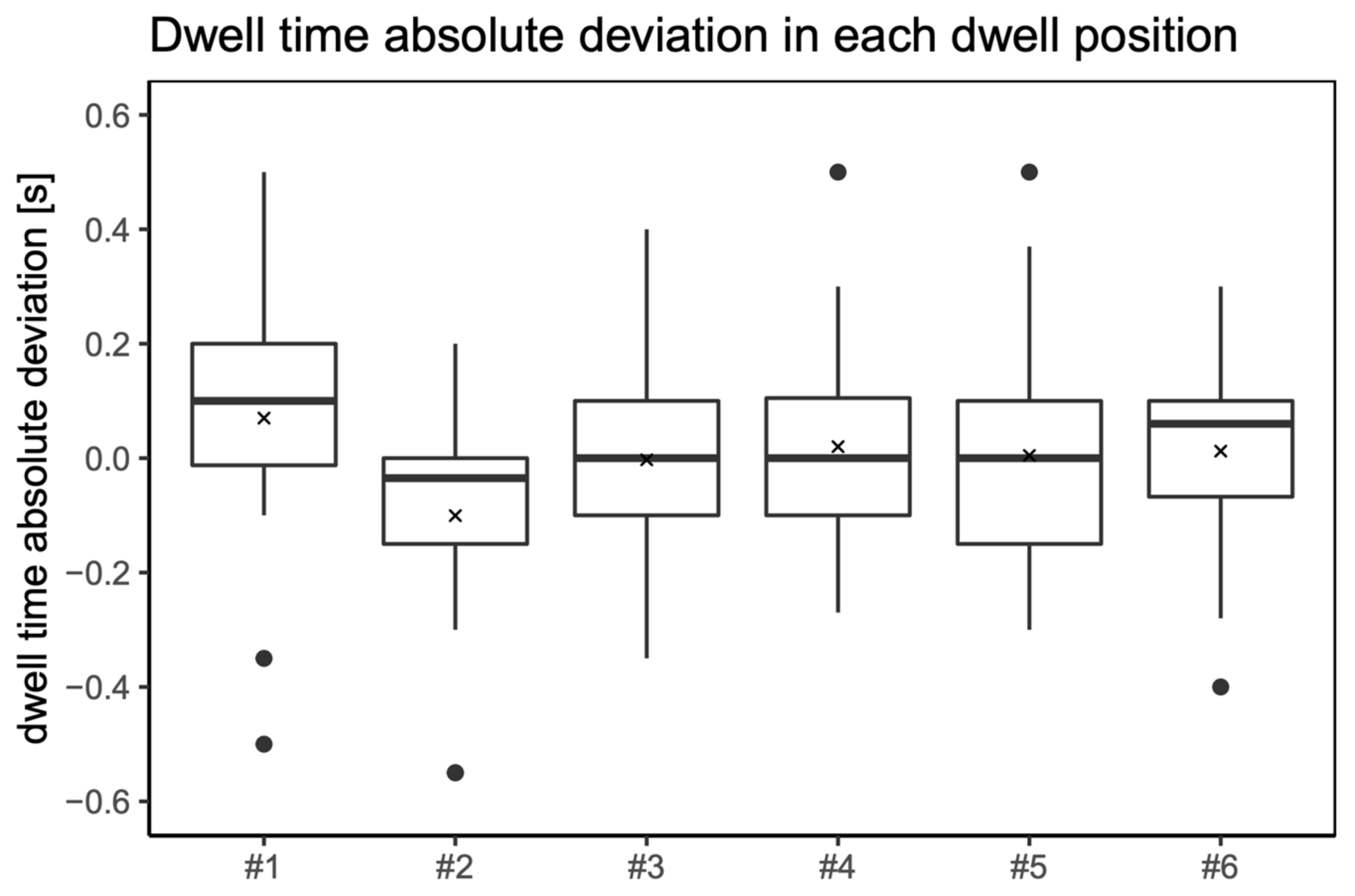
2.7. Precision of Dwell Time Measurements in Patient Treatments
2.8. Statistical Analysis
3. Results
3.1. Repeatability
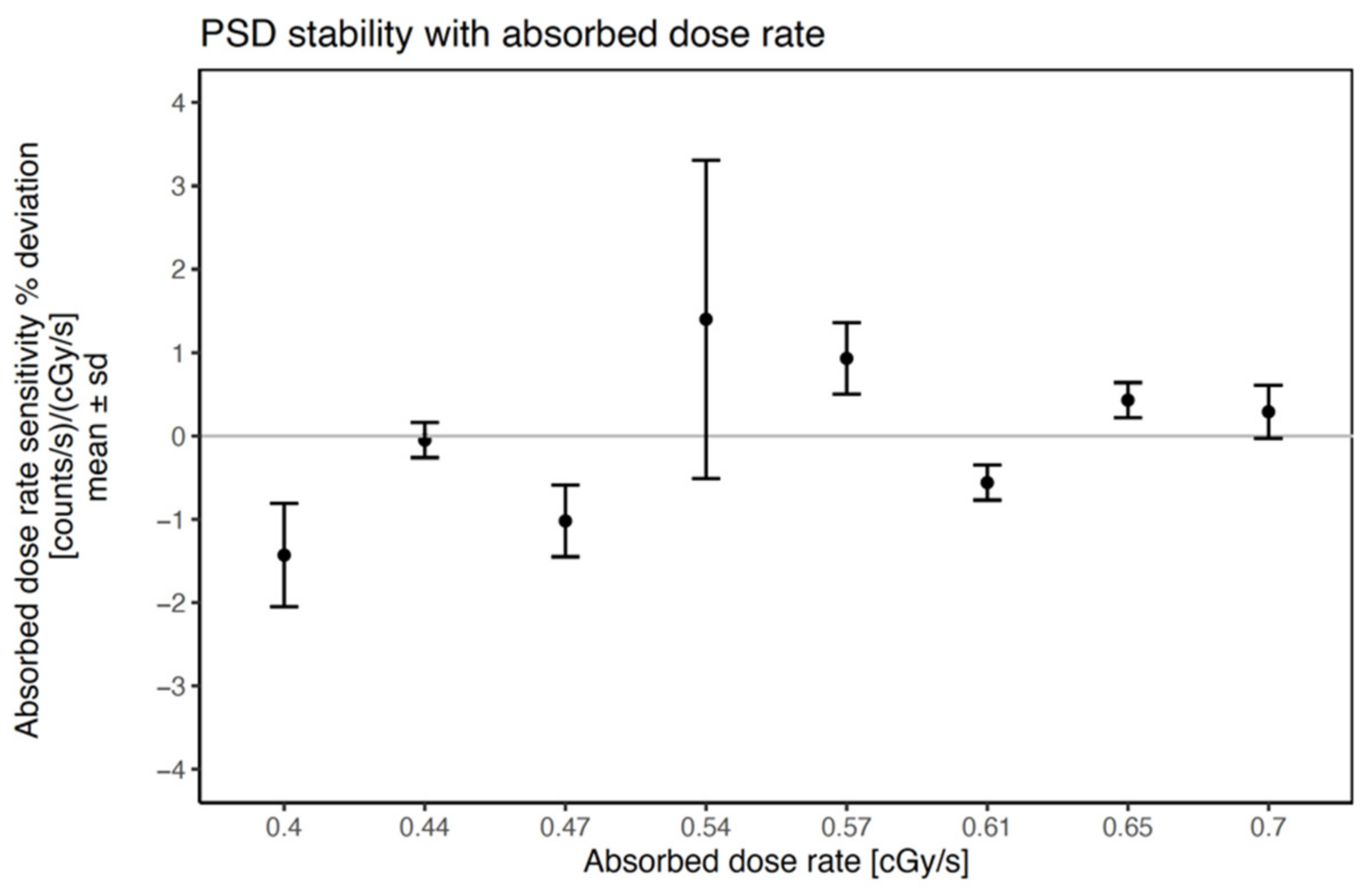
3.2. Long-Term Stability
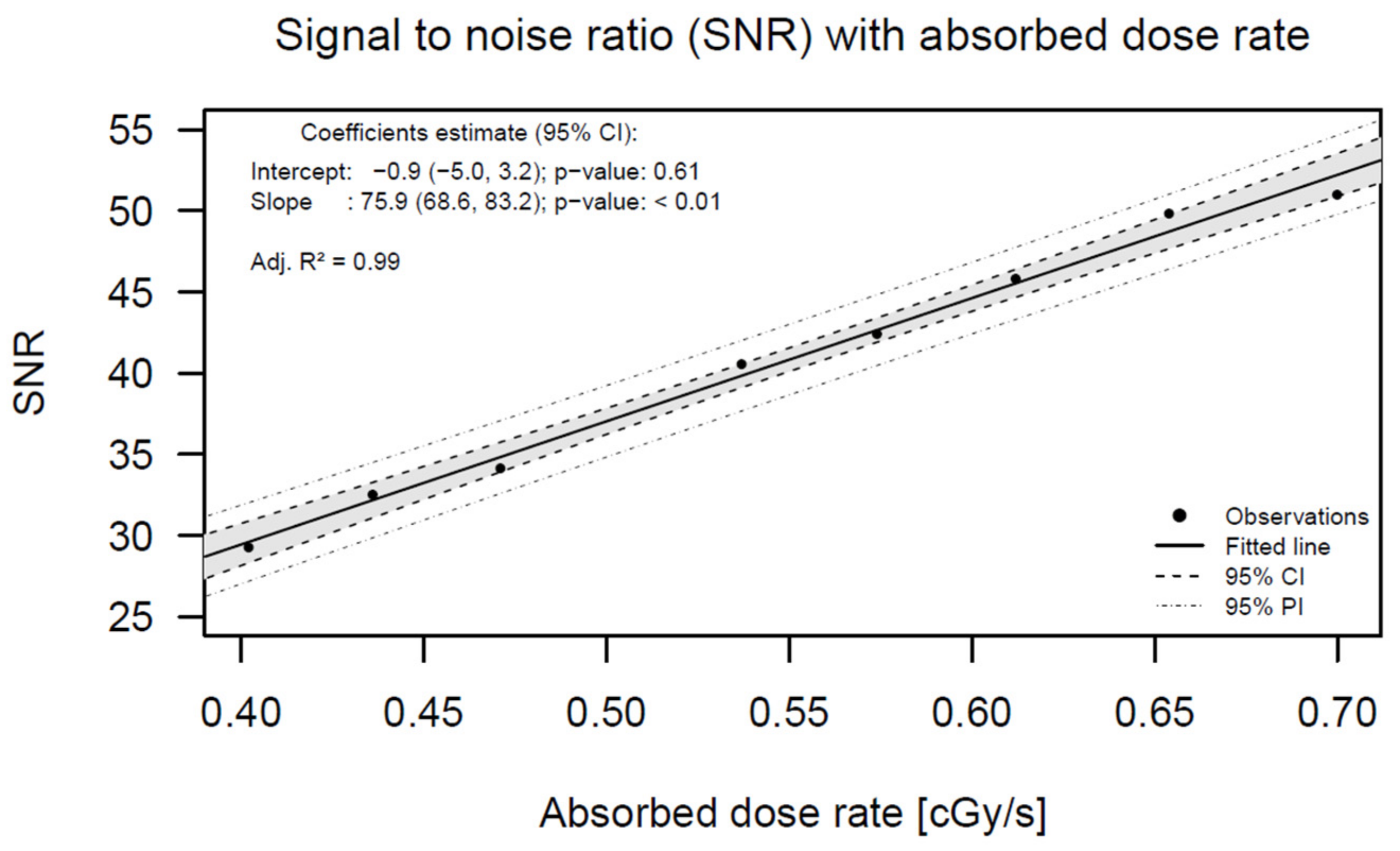
3.3. Signal-to-Noise Ratio (SNR)
3.4. Linearity of PSD Total Counts with Absorbed Dose
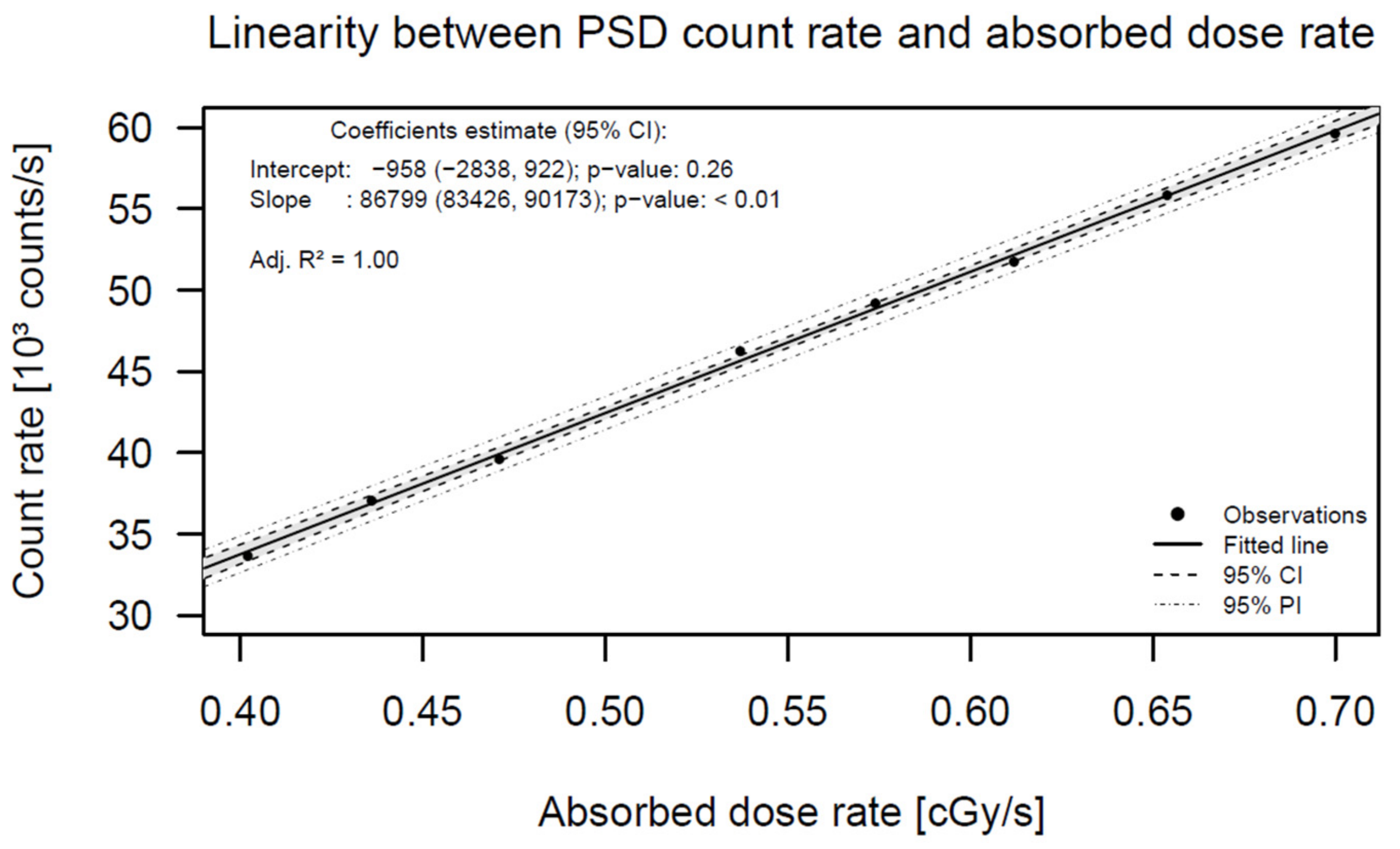
3.5. Linearity of PSD Count Rate with Absorbed Dose Rate
3.6. Precision of Dwell Time Measurements in Patient Treatments
4. Discussion
4.1. Repeatability
4.2. Long-Term Stability
4.3. Signal-to-Noise Ratio (SNR)
4.4. Linearity of PSD Total Counts with Absorbed Dose
4.5. Linearity of PSD Count Rate with Absorbed Dose Rate
4.6. Precision of Dwell Time Measurements in Patient Treatments
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tanderup, K.; Kirisits, C.; Damato, A.L. Treatment delivery verification in brachytherapy: Prospects of technology innovation. Brachytherapy 2018, 17, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Guedea, F.; Venselaar, J.; Hoskin, P.; Hellebust, T.P.; Peiffert, D.; Londres, B.; Ventura, M.; Mazeron, J.-J.; Van Limbergen, E.; Pötter, R.; et al. Patterns of care for brachytherapy in Europe: Updated results. Radiother. Oncol. 2010, 97, 514–520. [Google Scholar] [CrossRef] [PubMed]
- SAFRON. A Newsletter on Patient Safety in Radiotherapy; IAEA: Vienna, Austria, 2017; Volume 3, pp. 1–4. [Google Scholar]
- Valentin, J. Prevention of high-dose-rate brachytherapy accidents. ICRP Publication 97. Ann ICRP 2005, 35, 1–51. [Google Scholar] [CrossRef] [PubMed]
- Tanderup, K.; Beddar, S.; Andersen, C.E.; Kertzscher, G.; Cygler, J.E. In vivo dosimetry in brachytherapy. Med. Phys. 2013, 40, 070902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kertzscher, G.; Rosenfeld, A.; Beddar, S.; Tanderup, K.; Cygler, J.E. In vivo dosimetry: Trends and prospects for brachytherapy. Br. J. Radiol. 2014, 87, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Beaulieu, L.; Beddar, S. Review of plastic and liquid scintillation dosimetry for photon, electron, and proton therapy. Phys. Med. Biol. 2016, 61, R305–R343. [Google Scholar] [CrossRef]
- Carrara, M.; Cutajar, D.; Alnaghy, S.; Espinoza, A.; Romanyukha, A.; Presilla, S.; Tenconi, C.; Cerrotta, A.; Fallai, C.; Safavi-Naeini, M.; et al. Semiconductor real-time quality assurance dosimetry in brachytherapy. Brachytherapy 2018, 17, 133–145. [Google Scholar] [CrossRef]
- Therriault-Proulx, F.; Briere, T.M.; Mourtada, F.; Aubin, S.; Beddar, S.; Beaulieu, L. A phantom study of an in vivo dosimetry system using plastic scintillation detectors for real-time verification of 192 Ir HDR brachytherapy. Med. Phys. 2011, 38, 2542–2551. [Google Scholar] [CrossRef] [Green Version]
- Bergau, P.F.L.; Schirmer, M.A.; Leha, A.; Leu, M.; Emons, G.; Hess, C.F.; Hille, A. The impact of rectal/bladder filling and applicator positioning on in vivo rectal dosimetry in vaginal cuff brachytherapy using an enhanced therapy setting. Brachytherapy 2019, 19, 168–175. [Google Scholar] [CrossRef]
- Belley, M.D.; Craciunescu, O.; Chang, Z.; Langloss, B.W.; Stanton, I.N.; Yoshizumi, T.T.; Therien, M.J.; Chino, J.P. Real-time dose-rate monitoring with gynecologic brachytherapy: Results of an initial clinical trial. Brachytherapy 2018, 17, 1023–1029. [Google Scholar] [CrossRef]
- Van Gellekom, M.P.R.; Canters, R.A.M.; Dankers, F.J.W.M.; Loopstra, A.; van der Steen-Banasik, E.M.; Haverkort, M.A.D. In vivo dosimetry in gynecological applications—A feasibility study. Brachytherapy 2018, 17, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Johansen, J.G.; Rylander, S.; Buus, S.; Bentzen, L.; Hokland, S.B.; Søndergaard, C.S.; With, A.K.M.; Kertzscher, G.; Tanderup, K. Time-resolved in vivo dosimetry for source tracking in brachytherapy. Brachytherapy 2018, 17, 122–132. [Google Scholar] [CrossRef] [PubMed]
- Beddar, A.S.; Law, S. Physics in Medicine & Biology Related content Water-equivalent plastic scintillation detectors for high-energy beam dosimetry: II. Properties and measurements energy beam dosimetry: I. Phys. Med. Biol. 1992, 37, 1901–1913. [Google Scholar] [PubMed]
- Wootton, L.; Beddar, S. Temperature dependence of BCF plastic scintillation detectors. Phys. Med. Biol. 2013, 58, 2955–2967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dimitriadis, A.; Patallo, I.S.; Billas, I.; Duane, S.; Nisbet, A.; Clark, C.H. Characterisation of a plastic scintillation detector to be used in a multicentre stereotactic radiosurgery dosimetry audit. Radiat. Phys. Chem. 2017, 140, 373–378. [Google Scholar] [CrossRef] [Green Version]
- Beddar, A.S.; Briere, T.M.; Mourtada, F.A.; Vassiliev, O.N.; Liu, H.H.; Mohan, R. Monte Carlo calculations of the absorbed dose and energy dependence of plastic scintillators. Med. Phys. 2005, 32, 1265–1269. [Google Scholar] [CrossRef]
- Fonseca, G.P.; Johansen, J.G.; Smith, R.L.; Beaulieu, L.; Beddar, S.; Kertzscher, G.; Verhaegen, F.; Tanderup, K. In vivo dosimetry in brachytherapy: Requirements and future directions for research, development, and clinical practice. Phys. Imaging Radiat. Oncol. 2020, 16, 1–11. [Google Scholar] [CrossRef]
- Moutinho, L.M.; Castro, I.F.C.; Peralta, L.; Abreu, M.C.; Veloso, J.F.C.A. Brachytherapy dosimeter with silicon photomultipliers. Nucl. Instrum. Methods Phys. Res. Sect. A Accel. Spectrometers Detect. Assoc. Equip. 2015, 787, 358–360. [Google Scholar] [CrossRef]
- Rovirosa, A.; Ascaso, C.; Sánchez-Reyes, A.; Herreros, A.; Abellana, R.; Pahisa, J.; Lejarcegui, J.A.; Biete, A. Three or four fractions of 4–5 Gy per week in postoperative high-dose-rate brachytherapy for endometrial carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 418–423. [Google Scholar] [CrossRef]
- Zhang, Y.; Fornes, B.; Gómez, G.; Bentoldrà, I.; Carmona, C.; Herreros, A.; Sabater, S.; Nicolás, I.; Li, Y.; Sánchez, J.; et al. Eqd2 analyses of vaginal complications in exclusive brachytherapy for postoperative endometrial carcinoma. Cancers 2020, 12, 3059. [Google Scholar] [CrossRef]
- Zhang, Y.; Ascaso, C.; Herreros, A.; Sánchez, J.; Sabater, S.; del Pino, M.; Li, Y.; Gómez, G.; Torné, A.; Biete, A.; et al. Postoperative endometrial carcinoma treated with external beam irradiation plus vaginal-cuff brachytherapy. Is there a dose relationship with G2 vaginal complications? Rep. Pr. Oncol. Radiother. 2020, 25, 227–232. [Google Scholar] [CrossRef]
- Del Valle Aguilera, M.; Rovirosa, Á.; Ascaso, C.; Herreros, A.; Sánchez, J.; Garcia-Migue, J.; Cortes, S.; Agusti, E.; Camacho, C.; Zhang, Y.; et al. Late G2 vagina toxicity in post-operative endometrial carcinoma is associated with a 68 Gy dose equivalent to 2 Gy per fraction(α/β = 3 Gy) at 2cm3 of vagina. J. Contemp. Brachyther. 2018, 10, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Gomez, G.; Ascaso, C.; Herreros, A.; Fornes, B.; Mases, J.; Rochera, J.; Tagliaferri, L.; Sabater, S.; Torne, A.; et al. Preliminary results of a vaginal constraint for reducing G2 late vaginal complications after postoperative brachytherapy in endometrial cancer: A prospective analysis. Clin. Transl. Oncol. 2021, 24, 875–881. [Google Scholar] [CrossRef] [PubMed]
- Johansen, J.; Kertzscher, G.; Jørgensen, E.; Rylander, S.; Bentzen, L.; Hokland, S.; Søndergaard, C.; With, A.; Buus, S.; Tanderup, K. Dwell time verification in brachytherapy based on time resolved in vivo dosimetry. Phys. Med. 2019, 60, 156–161. [Google Scholar] [CrossRef]
- Fonseca, G.P.; Landry, G.; Reniers, B.; Hoffmann, A.; A Rubo, R.; Antunes, P.C.G.; Yoriyaz, H.; Verhaegen, F. The contribution from transit dose for 192Ir HDR brachytherapy treatments. Phys. Med. Biol. 2014, 59, 1831–1844. [Google Scholar] [CrossRef] [PubMed]
- Debnath, S.B.C.; Ferre, M.; Tonneau, D.; Fauquet, C.; Tallet, A.; Goncalves, A.; Darreon, J. High resolution small-scale inorganic scintillator detector: HDR brachytherapy application. Med. Phys. 2021, 48, 1485–1496. [Google Scholar] [CrossRef]
- Jørgensen, E.B.; Johansen, J.G.; Overgaard, J.; Piché-Meunier, D.; Tho, D.; Rosales, H.M.L.; Tanderup, K.; Beaulieu, L.; Kertzscher, G.; Beddar, S. A high-Z inorganic scintillator–based detector for time-resolved in vivo dosimetry during brachytherapy. Med. Phys. 2021, 48, 7382–7398. [Google Scholar] [CrossRef]
- Sahoo, N. Measurement of transit time of a remote after-loading high dose rate brachytherapy source. Med. Phys. 2001, 28, 1786–1790. [Google Scholar] [CrossRef]
- Rickey, D.W.; Sasaki, D.; Bews, J. A quality assurance tool for high-dose-rate brachytherapy. Med. Phys. 2010, 37, 2525–2532. [Google Scholar] [CrossRef]
- Menon, G.V.; Carlone, M.C.; Sloboda, R.S. Transit dose contributions to intracavitary and interstitial PDR brachytherapy treatments. Phys. Med. Biol. 2008, 53, 3447–3462. [Google Scholar] [CrossRef]
- Wong, T.P.Y.; Fernando, W.; Johnston, P.N.; Bubb, I.F. Transit dose of an Ir-192 high dose rate brachytherapy stepping source. Phys. Med. Biol. 2001, 46, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Guiral, P.; Ribouton, J.; Jalade, P.; Wang, R.; Galvan, J.-M.; Lu, G.-N.; Pittet, P.; Rivoire, A.; Gindraux, L. Design and testing of a phantom and instrumented gynaecological applicator based on GaN dosimeter for use in high dose rate brachytherapy quality assurance. Med. Phys. 2016, 43, 5240–5251. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, G.P.; Voncken, R.; Hermans, J.; Verhaegen, F. Time-resolved QA and brachytherapy applicator commissioning: Towards the clinical implementation. Brachytherapy 2021, 21, 128–137. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Detector Acquisition Frequency [Hz] | Nominal Dwell Time [s] | Time Average Deviation [s] | Maximum Time Deviation [s] | RSD 1 Count Rate [%] | RSD 1 Total Counts [%] | RSD 1 Measured Dwell Time [%] |
|---|---|---|---|---|---|---|
| 10 | 300 | −0.04 | −0.10 | 0.27 | 1.17 | 0.02 |
| 30 | −0.02 | −0.10 | 0.22 | 0.29 | 0.14 | |
| 10 | −0.02 | −0.20 | 0.50 | 1.38 | 0.79 | |
| 20 | 10 | 0.00 | −0.10 | 0.32 | 5.59 | 0.58 |
| 3 | 0.06 | 0.15 | 0.43 | 2.45 | 1.89 | |
| 1 | 0.04 | 0.10 | 1.03 | 9.22 | 4.19 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herreros, A.; Pérez-Calatayud, J.; Ballester, F.; Barrera-Gómez, J.; Abellana, R.; Melo, J.; Moutinho, L.; Tagliaferri, L.; Rovirosa, Á. In Vivo Verification of Treatment Source Dwell Times in Brachytherapy of Postoperative Endometrial Carcinoma: A Feasibility Study. J. Pers. Med. 2022, 12, 911. https://doi.org/10.3390/jpm12060911
Herreros A, Pérez-Calatayud J, Ballester F, Barrera-Gómez J, Abellana R, Melo J, Moutinho L, Tagliaferri L, Rovirosa Á. In Vivo Verification of Treatment Source Dwell Times in Brachytherapy of Postoperative Endometrial Carcinoma: A Feasibility Study. Journal of Personalized Medicine. 2022; 12(6):911. https://doi.org/10.3390/jpm12060911
Chicago/Turabian StyleHerreros, Antonio, José Pérez-Calatayud, Facundo Ballester, Jose Barrera-Gómez, Rosa Abellana, Joana Melo, Luis Moutinho, Luca Tagliaferri, and Ángeles Rovirosa. 2022. "In Vivo Verification of Treatment Source Dwell Times in Brachytherapy of Postoperative Endometrial Carcinoma: A Feasibility Study" Journal of Personalized Medicine 12, no. 6: 911. https://doi.org/10.3390/jpm12060911
APA StyleHerreros, A., Pérez-Calatayud, J., Ballester, F., Barrera-Gómez, J., Abellana, R., Melo, J., Moutinho, L., Tagliaferri, L., & Rovirosa, Á. (2022). In Vivo Verification of Treatment Source Dwell Times in Brachytherapy of Postoperative Endometrial Carcinoma: A Feasibility Study. Journal of Personalized Medicine, 12(6), 911. https://doi.org/10.3390/jpm12060911