

The Effect of a Home-Based Tele-Exercise Training Program on the Quality of Life and Physical Performance in Breast Cancer Survivors



Abstract
:1. Introduction
2. Materials and Methods
2.1. Consent Form and Ethical Approval
2.2. Study Participants
2.3. Tele-Exercise Training Program
2.4. Data Collection
2.4.1. Somatometric Characteristics
2.4.2. Cardiorespiratory Fitness
2.4.3. Muscle Function
2.4.4. Quality of Life
2.4.5. Post-Traumatic Stress
2.4.6. Anxiety
2.5. Statistical Analysis
3. Results
3.1. Somatometric Characteristics
3.2. Cardiorespiratory Fitness
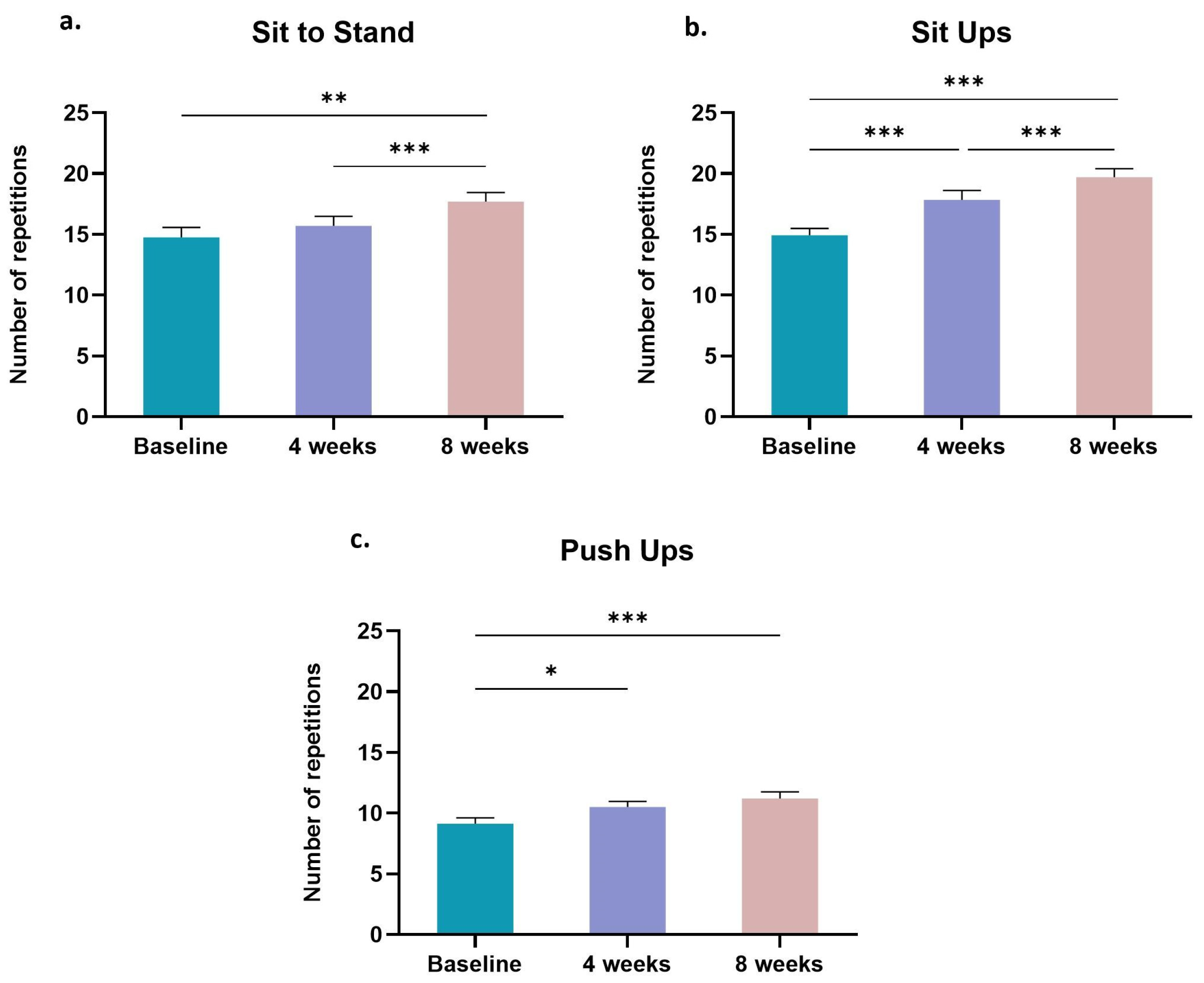
3.3. Muscle Function
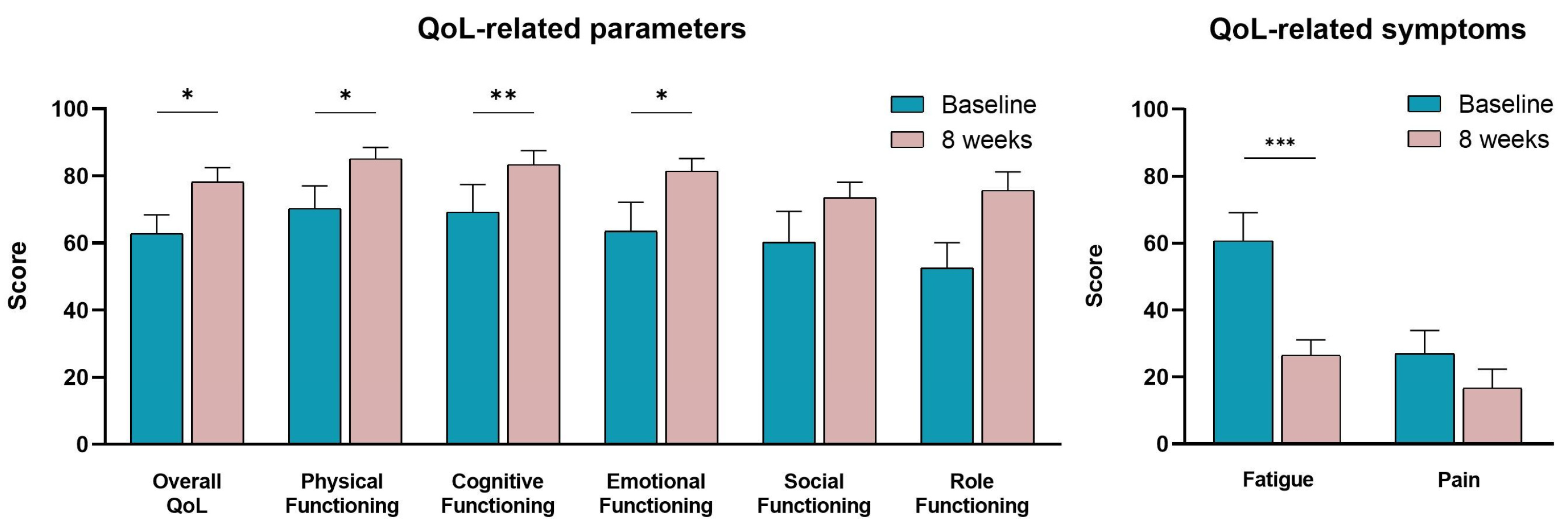
3.4. Quality of Life
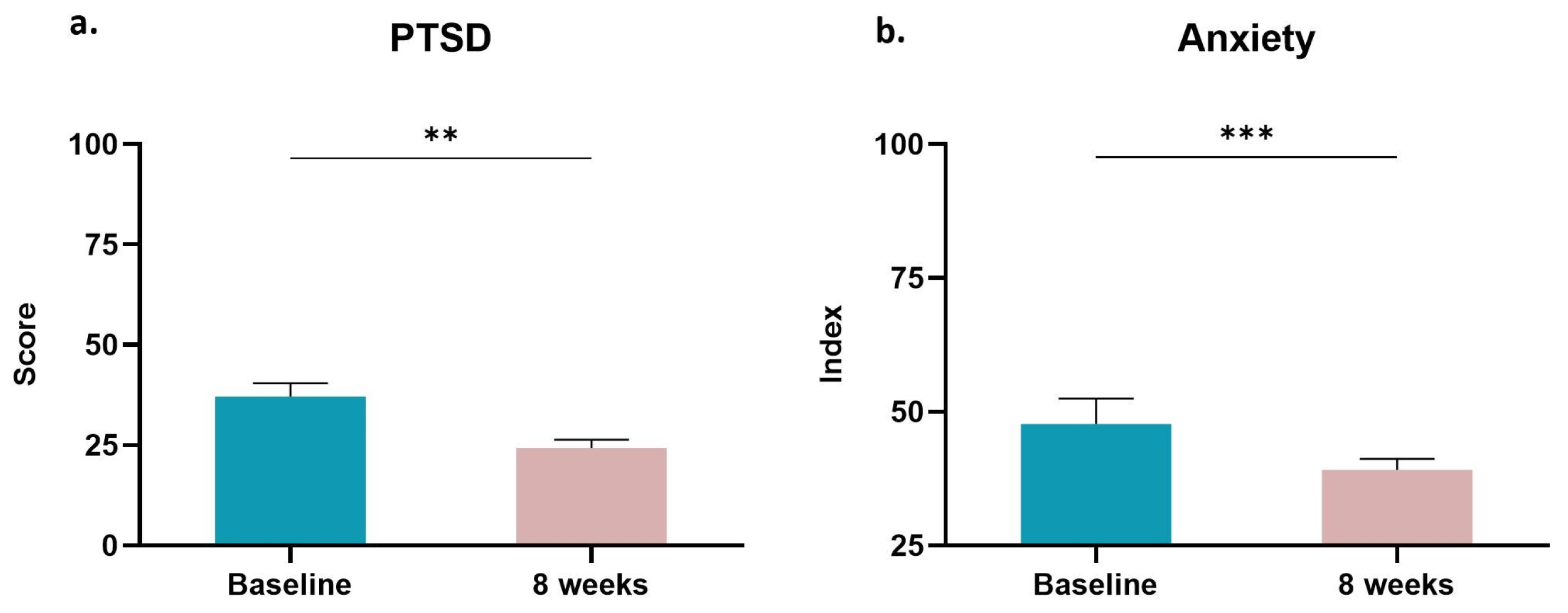
3.5. Post-Traumatic Stress and Anxiety
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Giaquinto, A.N.; Sung, H.; Miller, K.D.; Kramer, J.L.; Newman, L.A.; Minihan, A.; Jemal, A.; Siegel, R.L. Breast Cancer Statistics, 2022. CA Cancer J. Clin. 2022, 72, 524–541. [Google Scholar] [CrossRef] [PubMed]
- Papaoiconomou, E.; Lymperi, M.; Petraki, C.; Philippou, A.; Msaouel, P.; Michalopoulou, F.; Kafiri, G.; Vassilakos, G.; Zografos, G.; Koutsilieris, M. Kiss-1/GPR54 protein expression in breast cancer. Anticancer Res. 2014, 34, 1401–1407. [Google Scholar] [PubMed]
- Islami, F.; Goding Sauer, A.; Miller, K.D.; Siegel, R.L.; Fedewa, S.A.; Jacobs, E.J.; McCullough, M.L.; Patel, A.V.; Ma, J.; Soerjomataram, I.; et al. Proportion and number of cancer cases and deaths attributable to potentially modifiable risk factors in the United States. CA Cancer J. Clin. 2018, 68, 31–54. [Google Scholar] [CrossRef] [PubMed]
- Yfantis, A.; Sarafis, P.; Moisoglou, I.; Tolia, M.; Intas, G.; Tiniakou, I.; Zografos, K.; Zografos, G.; Constantinou, M.; Nikolentzos, A.; et al. How breast cancer treatments affect the quality of life of women with non-metastatic breast cancer one year after surgical treatment: A cross-sectional study in Greece. BMC Surg. 2020, 20, 210. [Google Scholar] [CrossRef]
- Lovelace, D.L.; McDaniel, L.R.; Golden, D. Long-Term Effects of Breast Cancer Surgery, Treatment, and Survivor Care. J. Midwifery Womens Health 2019, 64, 713–724. [Google Scholar] [CrossRef]
- Schmidt, M.E.; Scherer, S.; Wiskemann, J.; Steindorf, K. Return to work after breast cancer: The role of treatment-related side effects and potential impact on quality of life. Eur. J. Cancer Care 2019, 28, e13051. [Google Scholar] [CrossRef]
- Boscher, C.; Joly, F.; Clarisse, B.; Humbert, X.; Grellard, J.M.; Binarelli, G.; Tron, L.; Licaj, I.; Lange, M. Perceived Cognitive Impairment in Breast Cancer Survivors and Its Relationships with Psychological Factors. Cancers 2020, 12, 3000. [Google Scholar] [CrossRef]
- Yi, J.C.; Syrjala, K.L. Anxiety and Depression in Cancer Survivors. Med. Clin. North Am. 2017, 101, 1099–1113. [Google Scholar] [CrossRef]
- Natalucci, V.; Marini, C.F.; Flori, M.; Pietropaolo, F.; Lucertini, F.; Annibalini, G.; Vallorani, L.; Sisti, D.; Saltarelli, R.; Villarini, A.; et al. Effects of a Home-Based Lifestyle Intervention Program on Cardiometabolic Health in Breast Cancer Survivors during the COVID-19 Lockdown. J. Clin. Med. 2021, 10, 2678. [Google Scholar] [CrossRef]
- Kelly, D.L.; Yang, G.S.; Starkweather, A.R.; Siangphoe, U.; Alexander-Delpech, P.; Lyon, D.E. Relationships Among Fatigue, Anxiety, Depression, and Pain and Health-Promoting Lifestyle Behaviors in Women With Early-Stage Breast Cancer. Cancer Nurs. 2020, 43, 134–146. [Google Scholar] [CrossRef] [PubMed]
- Papadopetraki, A.; Maridaki, M.; Zagouri, F.; Dimopoulos, M.A.; Koutsilieris, M.; Philippou, A. Physical Exercise Restrains Cancer Progression through Muscle-Derived Factors. Cancers 2022, 14, 1892. [Google Scholar] [CrossRef] [PubMed]
- Adraskela, K.; Veisaki, E.; Koutsilieris, M.; Philippou, A. Physical Exercise Positively Influences Breast Cancer Evolution. Clin. Breast Cancer 2017, 17, 408–417. [Google Scholar] [CrossRef] [PubMed]
- Ntanasis-Stathopoulos, J.; Tzanninis, J.G.; Philippou, A.; Koutsilieris, M. Epigenetic regulation on gene expression induced by physical exercise. J. Musculoskelet Neuronal Interact. 2013, 13, 133–146. [Google Scholar]
- D’Ascenzi, F.; Anselmi, F.; Fiorentini, C.; Mannucci, R.; Bonifazi, M.; Mondillo, S. The benefits of exercise in cancer patients and the criteria for exercise prescription in cardio-oncology. Eur. J. Prev. Cardiol. 2021, 28, 725–735. [Google Scholar] [CrossRef]
- Kose, E.; Aydin, M.; Kose, O.; Aksu, M.G.; Sekban, G. The efficiency of a mixed exercise program on quality of life and fatigue levels in patients with breast cancer. Rev. Assoc. Med. Bras. 2021, 67, 1279–1285. [Google Scholar] [CrossRef]
- Salchow, J.L.; Strunk, M.A.; Niels, T.; Steck, J.; Minto, C.A.; Baumann, F.T. A Randomized Controlled Pilot Trial About the Influence of Kyusho Jitsu Exercise on Self-efficacy, Fear, Depression, and Distress of Breast Cancer Patients within Follow-Up Care. Integr. Cancer Ther. 2021, 20, 15347354211037955. [Google Scholar] [CrossRef]
- Maridaki, M.; Papadopetraki, A.; Karagianni, H.; Koutsilieris, M.; Philippou, A. The Assessment and Relationship Between Quality of Life and Physical Activity Levels in Greek Breast Cancer Female Patients under Chemotherapy. Sports 2020, 8, 32. [Google Scholar] [CrossRef]
- Anderson, E.; Shivakumar, G. Effects of exercise and physical activity on anxiety. Front. Psychiatry 2013, 4, 27. [Google Scholar] [CrossRef]
- Smith-Turchyn, J.; Allen, L.; Dart, J.; Lavigne, D.; Rooprai, S.; Dempster, H.; Trenholm, R.; Santa Mina, D.; Sabiston, C.M.; MacMillan, L.; et al. Characterizing the Exercise Behaviour, Preferences, Barriers, and Facilitators of Cancer Survivors in a Rural Canadian Community: A Cross-Sectional Survey. Curr. Oncol. 2021, 28, 3172–3187. [Google Scholar] [CrossRef]
- Galiano-Castillo, N.; Cantarero-Villanueva, I.; Fernandez-Lao, C.; Ariza-Garcia, A.; Diaz-Rodriguez, L.; Del-Moral-Avila, R.; Arroyo-Morales, M. Telehealth system: A randomized controlled trial evaluating the impact of an internet-based exercise intervention on quality of life, pain, muscle strength, and fatigue in breast cancer survivors. Cancer 2016, 122, 3166–3174. [Google Scholar] [CrossRef]
- Sagarra-Romero, L.; Butragueno, J.; Gomez-Bruton, A.; Lozano-Berges, G.; Vicente-Rodriguez, G.; Morales, J.S. Effects of an online home-based exercise intervention on breast cancer survivors during COVID-19 lockdown: A feasibility study. Support. Care Cancer 2022, 30, 6287–6297. [Google Scholar] [CrossRef] [PubMed]
- Vancini, R.L.; Borges Viana, R.; dos Santos Andrade, M.; Andre Barbosa de Lira, C.; Theodoros Nikolaidis, P.; Aparecido de Almeida, A.; Knechtle, B. YouTube as a source of information about physical exercise during COVID-19 outbreak. Int. J. Sport Stud. Health 2022, 4, e123312. [Google Scholar] [CrossRef]
- Grazioli, E.; Cerulli, C.; Dimauro, I.; Moretti, E.; Murri, A.; Parisi, A. New strategy of home-based exercise during pandemic COVID-19 in breast cancer patients: A case study. Sustainability 2020, 12, 6940. [Google Scholar] [CrossRef]
- Gonzalo-Encabo, P.; Wilson, R.L.; Kang, D.W.; Normann, A.J.; Dieli-Conwright, C.M. Exercise oncology during and beyond the COVID-19 pandemic: Are virtually supervised exercise interventions a sustainable alternative? Crit. Rev. Oncol. Hematol. 2022, 174, 103699. [Google Scholar] [CrossRef]
- Spector, D.; Deal, A.M.; Amos, K.D.; Yang, H.; Battaglini, C.L. A pilot study of a home-based motivational exercise program for African American breast cancer survivors: Clinical and quality-of-life outcomes. Integr. Cancer Ther. 2014, 13, 121–132. [Google Scholar] [CrossRef]
- Shachar, S.S.; Williams, G.R. The Obesity Paradox in Cancer-Moving beyond BMI-Response. Cancer Epidemiol. Biomark. Prev. 2017, 26, 981. [Google Scholar] [CrossRef]
- Dieli-Conwright, C.M.; Sami, N.; Norris, M.K.; Wan, J.; Kumagai, H.; Kim, S.J.; Cohen, P. Effect of aerobic and resistance exercise on the mitochondrial peptide MOTS-c in Hispanic and Non-Hispanic White breast cancer survivors. Sci. Rep. 2021, 11, 16916. [Google Scholar] [CrossRef]
- But-Hadzic, J.; Dervisevic, M.; Karpljuk, D.; Videmsek, M.; Dervisevic, E.; Paravlic, A.; Hadzic, V.; Tomazin, K. Six-Minute Walk Distance in Breast Cancer Survivors—A Systematic Review with Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 2591. [Google Scholar] [CrossRef]
- Stefani, L.; Giorgio, G.; Klika, R. Clinical Implementation of Exercise Guidelines for Cancer Patients: Adaptation of ACSM’s Guidelines to the Italian Model. J. Funct. Morphol. Kinesiol. 2017, 2, 4. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Fayers, P.; Bottomley, A.; EORTC Quality of Life Group; Quality of Life Unit. Quality of life research within the EORTC-the EORTC QLQ-C30. European Organisation for Research and Treatment of Cancer. Eur. J. Cancer 2002, 38 (Suppl. S4), S125–S133. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Wang, L.; Jia, X.; Li, Z.; Mu, H.; Liu, X.; Peng, B.; Li, A.; Fan, L. Prevalence and correlates of symptoms of post-traumatic stress disorder among Chinese healthcare workers exposed to physical violence: A cross-sectional study. BMJ Open 2017, 7, e016810. [Google Scholar] [CrossRef]
- Hoque, M.N.; Hannan, A.; Imran, S.; Alam, M.A.; Matubber, B.; Saha, S.M. Anxiety and Its Determinants among Undergraduate Students during E-learning in Bangladesh Amid Covid-19. J. Affect. Disord. Rep. 2021, 6, 100241. [Google Scholar] [CrossRef] [PubMed]
- Reeves, M.M.; Terranova, C.O.; Winkler, E.A.H.; McCarthy, N.; Hickman, I.J.; Ware, R.S.; Lawler, S.P.; Eakin, E.G.; Demark-Wahnefried, W. Effect of a Remotely Delivered Weight Loss Intervention in Early-Stage Breast Cancer: Randomized Controlled Trial. Nutrients 2021, 13, 4091. [Google Scholar] [CrossRef] [PubMed]
- Dieli-Conwright, C.M.; Courneya, K.S.; Demark-Wahnefried, W.; Sami, N.; Lee, K.; Buchanan, T.A.; Spicer, D.V.; Tripathy, D.; Bernstein, L.; Mortimer, J.E. Effects of Aerobic and Resistance Exercise on Metabolic Syndrome, Sarcopenic Obesity, and Circulating Biomarkers in Overweight or Obese Survivors of Breast Cancer: A Randomized Controlled Trial. J. Clin. Oncol. 2018, 36, 875–883. [Google Scholar] [CrossRef]
- Ochi, E.; Tsuji, K.; Narisawa, T.; Shimizu, Y.; Kuchiba, A.; Suto, A.; Jimbo, K.; Takayama, S.; Ueno, T.; Sakurai, N.; et al. Cardiorespiratory fitness in breast cancer survivors: A randomised controlled trial of home-based smartphone supported high intensity interval training. BMJ Support. Palliat. Care 2022, 12, 33–37. [Google Scholar] [CrossRef]
- Dieli-Conwright, C.M.; Courneya, K.S.; Demark-Wahnefried, W.; Sami, N.; Lee, K.; Sweeney, F.C.; Stewart, C.; Buchanan, T.A.; Spicer, D.; Tripathy, D.; et al. Aerobic and resistance exercise improves physical fitness, bone health, and quality of life in overweight and obese breast cancer survivors: A randomized controlled trial. Breast Cancer Res. 2018, 20, 124. [Google Scholar] [CrossRef]
- Lee, M.K.; Lee, D.H.; Park, S.; Kim, S.I.; Jeon, J.Y. Relationship between resting heart rate and metabolic risk factors in breast cancer patients. Clin. Chim. Acta 2018, 486, 104–109. [Google Scholar] [CrossRef]
- Lee, D.H.; Park, S.; Lim, S.M.; Lee, M.K.; Giovannucci, E.L.; Kim, J.H.; Kim, S.I.; Jeon, J.Y. Resting heart rate as a prognostic factor for mortality in patients with breast cancer. Breast Cancer Res. Treat. 2016, 159, 375–384. [Google Scholar] [CrossRef]
- Gell, N.M.; Dittus, K.; Caefer, J.; Martin, A.; Bae, M.; Patel, K.V. Remotely delivered exercise to older rural cancer survivors: A randomized controlled pilot trial. J. Cancer Surviv. 2022, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Gorzelitz, J.S.; Stoller, S.; Costanzo, E.; Gangnon, R.; Koltyn, K.; Dietz, A.T.; Spencer, R.J.; Rash, J.; Cadmus-Bertram, L. Improvements in strength and agility measures of functional fitness following a telehealth-delivered home-based exercise intervention in endometrial cancer survivors. Support. Care Cancer 2022, 30, 447–455. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Lee, M.K.; Lee, D.H.; Kang, D.W.; Min, J.H.; Lee, J.W.; Chu, S.H.; Cho, M.S.; Kim, N.K.; Jeon, J.Y. Effects of a 12-week home-based exercise program on quality of life, psychological health, and the level of physical activity in colorectal cancer survivors: A randomized controlled trial. Support. Care Cancer 2019, 27, 2933–2940. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Liu, Y.; Jiang, J.; Peng, X.; Hu, X. Effect of telehealth interventions on quality of life in cancer survivors: A systematic review and meta-analysis of randomized controlled trials. Int. J. Nurs. Stud. 2021, 122, 103970. [Google Scholar] [CrossRef]
- De Luca, V.; Minganti, C.; Borrione, P.; Grazioli, E.; Cerulli, C.; Guerra, E.; Bonifacino, A.; Parisi, A. Effects of concurrent aerobic and strength training on breast cancer survivors: A pilot study. Public Health 2016, 136, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Paulo, T.R.S.; Rossi, F.E.; Viezel, J.; Tosello, G.T.; Seidinger, S.C.; Simoes, R.R.; de Freitas, R., Jr.; Freitas, I.F., Jr. The impact of an exercise program on quality of life in older breast cancer survivors undergoing aromatase inhibitor therapy: A randomized controlled trial. Health Qual. Life Outcomes 2019, 17, 17. [Google Scholar] [CrossRef]
- Schmitz, K.H.; Troxel, A.B.; Dean, L.T.; DeMichele, A.; Brown, J.C.; Sturgeon, K.; Zhang, Z.; Evangelisti, M.; Spinelli, B.; Kallan, M.J.; et al. Effect of Home-Based Exercise and Weight Loss Programs on Breast Cancer-Related Lymphedema Outcomes Among Overweight Breast Cancer Survivors: The WISER Survivor Randomized Clinical Trial. JAMA Oncol. 2019, 5, 1605–1613. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Duration: 55–60 min | ||
| 1st session | 2nd session | |
| 5 min | Warm up | Warm up |
| 15 min | Aerobic Dance (70–80% HRmax) | Aerobic Dance (70–80% HRmax) |
| ~30 min | 4 sets × 10–12 reps × 4 exercises engaging major muscle groups * (45 s rest between exercises, 60 s rest between sets) | 5 sets × 15 s × 4 exercises engaging major muscle groups * (25 s rest between exercises, 90 s rest between sets) |
| 5 min | Breathing Exercises | Breathing Exercises |
| 5 min | Cool down (flexibility exercises for all the major muscle groups) | Cool down (flexibility exercises for all the major muscle groups) |
| Breast Cancer Survivors | Baseline | 4 Weeks | 8 Weeks |
|---|---|---|---|
| Age (yrs) | 58.31 ± 3.13 | ||
| Height (cm) | 165.50 ± 1.48 | ||
| Body Mass (kg) | 70.35 ± 2.07 | 70.08 ± 2.03 | 68.88 ± 1.89 |
| Body Mass Index (kg/m2) | 25.68 ± 0.62 | 25.58 ± 0.60 | 25.15 ± 0.58 |
| Waist Circumference (cm) | 96.54 ± 1.84 | 95.12 ± 1.91 | 92.31 ± 1.72 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andrioti, A.; Papadopetraki, A.; Maridaki, M.; Philippou, A. The Effect of a Home-Based Tele-Exercise Training Program on the Quality of Life and Physical Performance in Breast Cancer Survivors. Sports 2023, 11, 102. https://doi.org/10.3390/sports11050102
Andrioti A, Papadopetraki A, Maridaki M, Philippou A. The Effect of a Home-Based Tele-Exercise Training Program on the Quality of Life and Physical Performance in Breast Cancer Survivors. Sports. 2023; 11(5):102. https://doi.org/10.3390/sports11050102
Chicago/Turabian StyleAndrioti, Andreana, Argyro Papadopetraki, Maria Maridaki, and Anastassios Philippou. 2023. "The Effect of a Home-Based Tele-Exercise Training Program on the Quality of Life and Physical Performance in Breast Cancer Survivors" Sports 11, no. 5: 102. https://doi.org/10.3390/sports11050102
APA StyleAndrioti, A., Papadopetraki, A., Maridaki, M., & Philippou, A. (2023). The Effect of a Home-Based Tele-Exercise Training Program on the Quality of Life and Physical Performance in Breast Cancer Survivors. Sports, 11(5), 102. https://doi.org/10.3390/sports11050102