Mental Health Symptoms Related to Body Shape Idealization in Female Fitness Physique Athletes


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Ethics
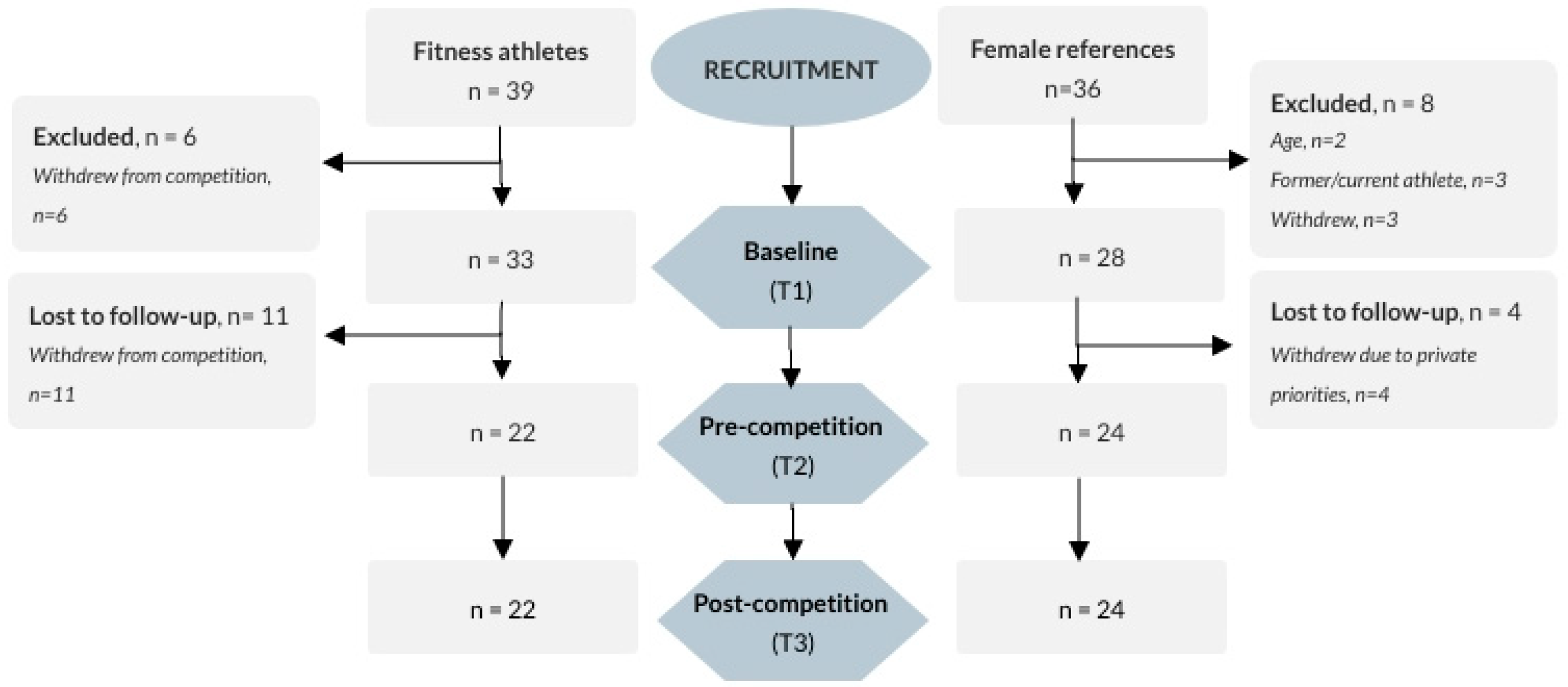
2.2. Participants
2.3. Questionnaires
2.3.1. Drive for Leanness (DL)
2.3.2. Drive for Muscularity (DM)
2.3.3. The Eating Disorder Examination Questionnaire (EDE-q)
2.3.4. The Binge Eating Scale (BES)
2.3.5. The Three-Factor Eating Questionnaire (TFE-q 21)
2.3.6. Reason for Exercise Inventory (REI)
2.3.7. The Exercise Dependence Scale (EDS)
2.3.8. The Child and Adolescent Perfectionism Scale (CAPS)
2.4. Statistics
3. Results
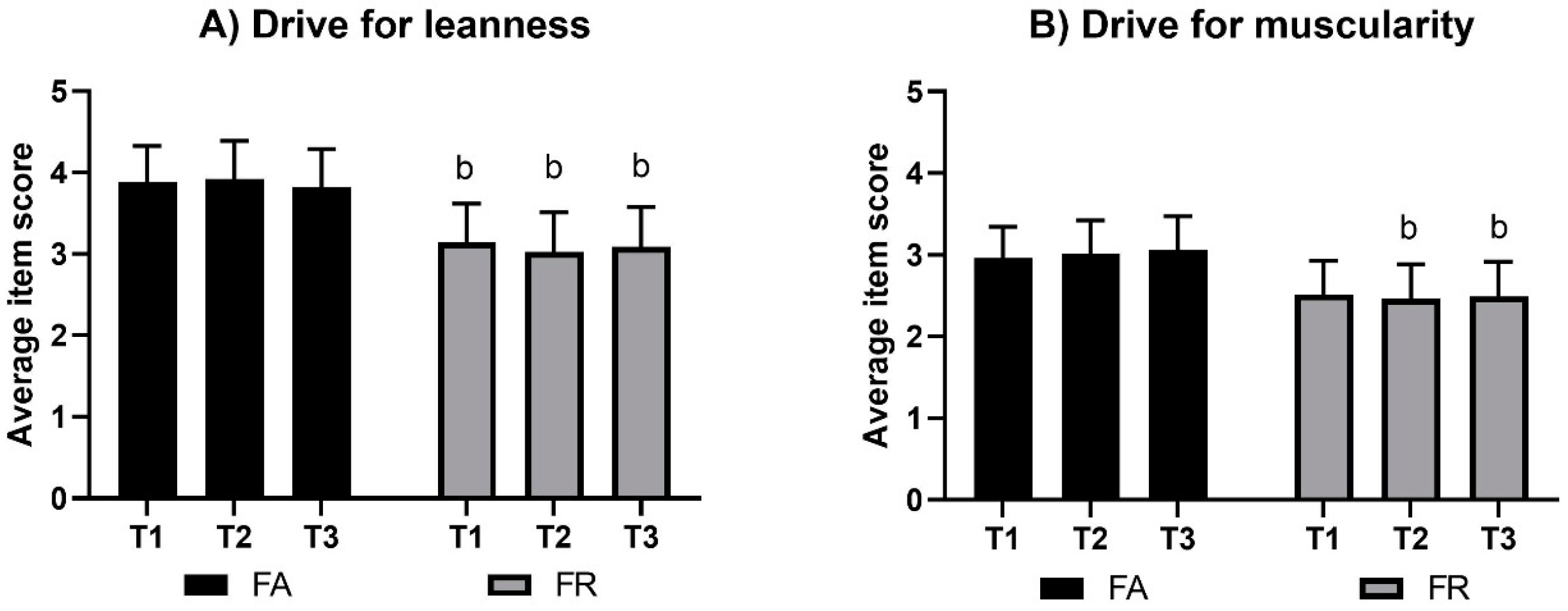
3.1. Drive for Leanness (DFL)
3.2. Drive for Muscularity (DM)
3.3. The Eating Disorder Examination Questionnaire (EDE-q)
3.3.1. Body Weight Concern (EDE-q)
3.3.2. Body Shape Concern (EDE-q)
3.3.3. Eating Restriction (EDE-q)
3.3.4. Eating Concern (EDE-q)
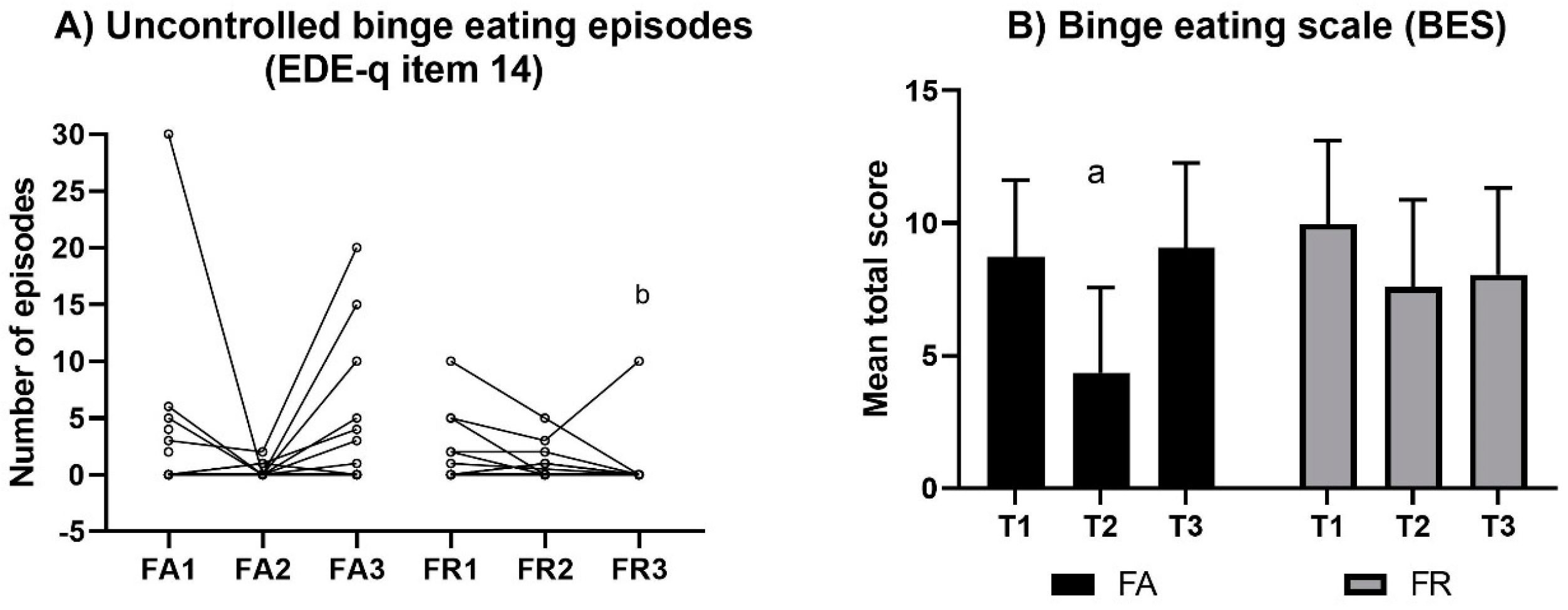
3.3.5. Binge Eating Episodes (EDE-q, Item 14)
3.3.6. Purging Episodes (EDE-q, Items 16–18)
3.4. Three-Factor Eating Questionnaire (TFE-q)
3.4.1. Intensity of Uncontrolled Eating (TFE-q)
3.4.2. Intensity of Cognitive Eating Restraint (TFE-q)
3.4.3. Intensity of Emotional Eating (TFE-q)
3.5. Symptoms of Binge Eating (BES)
3.6. Reasons for Exercise (REI)
3.7. Exercise Dependency (ExD)
3.8. Symptoms of Perfectionism (CAPS)
3.9. Correlates
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bakken, A. Ungdata. National Results on Adolescent Mental Health 2019; NOVA Report 9/19. 2019; NOVA, OsloMet: Oslo, Norway, 2019; p. 118. [Google Scholar]
- Rodriguez-Ayllon, M.; Cadenas-Sanchez, C.; Estevez-Lopez, F.; Munoz, N.E.; Mora-Gonzalez, J.; Migueles, J.H.; Molina-Garcia, P.; Henriksson, H.; Mena-Molina, A.; Martinez-Vizcaino, V.; et al. Role of Physical Activity and Sedentary Behavior in the Mental Health of Preschoolers, Children and Adolescents: A Systematic Review and Meta-Analysis. Sports Med. 2019, 49, 1383–1410. [Google Scholar] [CrossRef] [PubMed]
- Hausenblas, H.A.; Fallon, E.A. Exercise and body image: A meta-analysis. Psychol. Health 2006, 21, 33–47. [Google Scholar] [CrossRef]
- Collins, H.; Booth, J.N.; Duncan, A.; Fawkner, S.; Niven, A. The Effect of Resistance Training Interventions on ‘The Self’ in Youth: A Systematic Review and Meta-analysis. Sports Med. Open 2019, 5, 29. [Google Scholar] [CrossRef] [PubMed]
- Kandola, A.; Ashdown-Franks, G.; Stubbs, B.; Osborn, D.P.J.; Hayes, J.F. The association between cardiorespiratory fitness and the incidence of common mental health disorders: A systematic review and meta-analysis. J. Affect. Disord. 2019, 257, 748–757. [Google Scholar] [CrossRef]
- Gouttebarge, V.; Castaldelli-Maia, J.M.; Gorczynski, P.; Hainline, B.; Hitchcock, M.E.; Kerkhoffs, G.M.; Rice, S.M.; Reardon, C.L. Occurrence of mental health symptoms and disorders in current and former elite athletes: A systematic review and meta-analysis. Br. J. Sports Med. 2019, 53, 700–706. [Google Scholar] [CrossRef]
- Gouttebarge, V.; Jonkers, R.; Moen, M.; Verhagen, E.; Wylleman, P.; Kerkhoffs, G. The prevalence and risk indicators of symptoms of common mental disorders among current and former Dutch elite athletes. J. Sports Sci. 2017, 35, 2148–2156. [Google Scholar] [CrossRef]
- Rice, S.M.; Purcell, R.; De Silva, S.; Mawren, D.; McGorry, P.D.; Parker, A.G. The Mental Health of Elite Athletes: A Narrative Systematic Review. Sports Med. 2016, 46, 1333–1353. [Google Scholar] [CrossRef]
- Rosenvinge, J.H.; Sundgot-Borgen, J.; Pettersen, G.; Martinsen, M.; Stornæs, A.V.; Pensgaard, A.M. Are adolescent elite athletes less psychologically distressed than controls? A cross-sectional study of 966 Norwegian adolescents. Open Access J. Sports Med. 2018, 9, 115–123. [Google Scholar] [CrossRef]
- Reardon, C.L.; Hainline, B.; Aron, C.M.; Baron, D.; Baum, A.L.; Bindra, A.; Budgett, R.; Campriani, N.; Castaldelli-Maia, J.M.; Currie, A.; et al. Mental health in elite athletes: International Olympic Committee consensus statement. Br. J. Sports Med. 2019, 53, 667–699. [Google Scholar] [CrossRef]
- Steel, Z.; Marnane, C.; Iranpour, C.; Chey, T.; Jackson, J.W.; Patel, V.; Silove, D. The global prevalence of common mental disorders: A systematic review and meta-analysis 1980–2013. Int. J. Epidemiol. 2014, 43, 476–493. [Google Scholar] [CrossRef]
- Schaal, K.; Tafflet, M.; Nassif, H.; Thibault, V.; Pichard, C.; Alcotte, M.; Guillet, T.; El Helou, N.; Berthelot, G.; Simon, S.; et al. Psychological balance in high level athletes: Gender-based differences and sport-specific patterns. PLoS ONE 2011, 6, e19007. [Google Scholar] [CrossRef] [PubMed]
- Fortes, L.D.S.; Neves, C.M.; Filgueiras, J.F.; Almeida, S.S.; Ferreira, M.E.C. Body dissatisfaction, psychological commitment to exercise and eating behavior in young athletes from aesthetic sports. Rev. Bras. Cineantropometria Desempenho Hum. 2013, 15, 695–704. [Google Scholar]
- De Bruin, A.; Oudejans, R.R.; Bakker, F.C. Dieting and body image in aesthetic sports: A comparison of Dutch female gymnasts and non-aesthetic sport participants. Psychol. Sport Exerc. 2007, 8, 507–520. [Google Scholar] [CrossRef]
- Gotwals, J.K.; Stoeber, J.; Dunn, J.G.H.; Stoll, O. Are perfectionistic strivings in sport adaptive? A systematic review of confirmatory, contradictory, and mixed evidence. Can. Psychol. Can. 2012, 53, 263–279. [Google Scholar] [CrossRef]
- Stirling, A.; Kerr, G. Perceived vulnerabilities of female athletes to the development of disordered eating behaviours. Eur. J. Sport Sci. 2012, 12, 262–273. [Google Scholar] [CrossRef]
- Sundgot-Borgen, J.; Garthe, I. Elite athletes in aesthetic and Olympic weight-class sports and the challenge of body weight and body compositions. J. Sports Sci. 2011, 29, S101–S114. [Google Scholar] [CrossRef]
- Mountjoy, M.; Sundgot-Borgen, J.; Burke, L.; Ackerman, K.E.; Blauwet, C.; Constantini, N.; Lebrun, C.; Lundy, B.; Melin, A.; Meyer, N.; et al. International Olympic Committee (IOC) Consensus Statement on Relative Energy Deficiency in Sport (RED-S): 2018 Update. Int. J. Sport Nutr Exerc. Metab. 2018, 28, 316–331. [Google Scholar] [CrossRef]
- Hall, H.K.; Hill, A.P.; Appleton, P.R. Perfectionism: A Foundation for Sporting Excellence or an Uneasy Pathway Toward Purgatory? Human Kinetics: Champaign, IL, USA, 2012. [Google Scholar]
- Forsberg, S.; Lock, J. The relationship between perfectionism, eating disorders and athletes: A review. Minerva Pediatr. 2006, 58, 525–536. [Google Scholar]
- Limburg, K.; Watson, H.J.; Hagger, M.S.; Egan, S.J. The Relationship Between Perfectionism and Psychopathology: A Meta-Analysis. J. Clin. Psychol. 2017, 73, 1301–1326. [Google Scholar] [CrossRef]
- Vinkers, C.D.W.; Evers, C.; Adriaanse, M.A.; de Ridder, D.T.D. Body esteem and eating disorder symptomatology: The mediating role of appearance-motivated exercise in a non-clinical adult female sample. Eat. Behav. 2012, 13, 214–218. [Google Scholar] [CrossRef]
- Fuller-Tyszkiewicz, M.; Dias, S.; Krug, I.; Richardson, B.; Fassnacht, D. Motive—And appearance awareness-based explanations for body (dis)satisfaction following exercise in daily life. Br. J. Health Psychol. 2018, 23, 982–999. [Google Scholar] [CrossRef] [PubMed]
- Tylka, T.L.; Homan, K.J. Exercise motives and positive body image in physically active college women and men: Exploring an expanded acceptance model of intuitive eating. Body Image 2015, 15, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Craft, B.B.; Carroll, H.A.; Lustyk, M.K.B. Gender Differences in Exercise Habits and Quality of Life Reports: Assessing the Moderating Effects of Reasons for Exercise. Int. J. Lib. Arts Soc. Sci. 2014, 2, 65–76. [Google Scholar] [PubMed]
- Jankauskiene, R.; Pajaujiene, S. Disordered eating attitudes and body shame among athletes, exercisers and sedentary female college students. J. Sports Med. Phys. Fit. 2012, 52, 92–101. [Google Scholar]
- Bachner-Melman, R.; Zohar, A.H.; Ebstein, R.P.; Elizur, Y.; Constantini, N. How anorexic-like are the symptom and personality profiles of aesthetic athletes? Med. Sci. Sports Exerc. 2006, 38, 628–636. [Google Scholar] [CrossRef]
- Prnjak, K.; Jukic, I.; Tufano, J.J. Perfectionism, Body Satisfaction and Dieting in Athletes: The Role of Gender and Sport Type. Sports 2019, 7, 181. [Google Scholar] [CrossRef]
- Hopkinson, R.A.; Lock, J. Athletics, perfectionism, and disordered eating. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2004, 9, 99–106. [Google Scholar] [CrossRef]
- International Federation of Body Building. Our Disciplines. 2019. Available online: https://ifbb.com/our-disciplines/ (accessed on 23 August 2019).
- Alwan, N.; Moss, S.L.; Elliott-Sale, K.J.; Davies, I.G.; Enright, K. A Narrative Review on Female Physique Athletes: The Physiological and Psychological Implications of Weight Management Practices. Int. J. Sport Nutr. Exerc. Metab. 2019, 29, 682–689. [Google Scholar] [CrossRef]
- Holland, G.; Tiggemann, M. “Strong beats skinny every time”: Disordered eating and compulsive exercise in women who post fitspiration on Instagram. Int. J. Eat. Disord. 2017, 50, 76–79. [Google Scholar] [CrossRef]
- Bratland-Sanda, S.; Sundgot-Borgen, J. Symptoms of Eating Disorders, Drive for Muscularity and Physical Activity Among Norwegian Adolescents. Eur. Eat. Disord. Rev. 2012, 20, 287–293. [Google Scholar] [CrossRef]
- Mathisen, T.F.; Heia, J.; Raustøl, M.; Sandeggen, M.; Fjellestad, I.; Sundgot-Borgen, J. Physical health & symptoms of relative energy deficiency in female fitness athletes. Scand. J. Med. Sci. Sports 2019. [Google Scholar] [CrossRef]
- Boepple, L.; Ata, R.N.; Rum, R.; Thompson, J.K. Strong is the new skinny: A content analysis of fitspiration websites. Body Image 2016, 17, 132–135. [Google Scholar] [CrossRef] [PubMed]
- Tiggemann, M.; Zaccardo, M. ‘Strong is the new skinny’: A content analysis of #fitspiration images on Instagram. J. Health Psychol. 2018, 23, 1003–1011. [Google Scholar] [PubMed]
- Smolak, L.; Murnen, S.K. Drive for leanness: Assessment and relationship to gender, gender role and objectification. Body Image 2008, 5, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Tod, D.; Hall, G.; Edwards, C. Gender invariance and correlates of the Drive for Leanness Scale. Body Image 2012, 9, 555–558. [Google Scholar] [CrossRef]
- McCreary, D.R.; Sasse, D.K. An exploration of the drive for muscularity in adolescent boys and girls. J. Am. Coll. Health 2000, 48, 297–304. [Google Scholar] [CrossRef]
- McCreary, D.R.; Sasse, D.K.; Saucier, D.M.; Dorsch, K.D. Measuring the drive for muscularity: Factorial validity of the drive for muscularity scale in men and women. Psychol. Men Masc. 2004, 5, 49. [Google Scholar] [CrossRef]
- Fairburn, C.; Beglin, S. Eating Disorder Examination Questionnaire (EDE-Q 6.0), in Cognitive Behavior Therapy and Eating Disorders; Fairburn, C., Ed.; Guildford Press: New York, NY, USA, 2008; pp. 309–313. [Google Scholar]
- Freitas, S.R.; Lopes, C.S.; Appolinario, J.C.; Coutinho, W. The assessment of binge eating disorder in obese women: A comparison of the binge eating scale with the structured clinical interview for the DSM-IV. Eat. Behav. 2006, 7, 282–289. [Google Scholar] [CrossRef]
- Gormally, J.; Black, S.; Daston, S.; Rardin, D. The assessment of binge eating severity among obese persons. Addict. Behav. 1982, 7, 47–55. [Google Scholar] [CrossRef]
- Stunkard, A.J.; Messick, S. The three-factor eating questionnaire to measure dietary restraint, disinhibition and hunger. J. Psychosom. Res. 1985, 29, 71–83. [Google Scholar] [CrossRef]
- Anglé, S.; Engblom, J.; Eriksson, T.; Kautiainen, S.; Saha, M.T.; Lindfors, P.; Lehtinen, M.; Rimpelä, A. Three factor eating questionnaire-R18 as a measure of cognitive restraint, uncontrolled eating and emotional eating in a sample of young Finnish females. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silberstein, L.R.; Striegel-Moore, R.H.; Timko, C.; Rodin, J. Behavioral and psychological implications of body dissatisfaction: Do men and women differ? Sex. Roles 1988, 19, 219–232. [Google Scholar] [CrossRef]
- Hausenblas, H.A.; Downs, D.S. How much is too much? The development and validation of the exercise dependence scale. Psychol. Health 2002, 17, 387–404. [Google Scholar] [CrossRef]
- Flett, G.L.; Hewitt, P.; Boucher, D.; Davidson, L.A.; Munro, Y. The Child-Adolescent Perfectionism Scale: Development, Validation, and Association with Adjustment. J. Psychoeduc. Assess. 2000, in press. [Google Scholar]
- Flett, G.L.; Hewitt, P.; Besser, A.; Su, C.; Vaillancourt, T.; Boucher, D.; Munro, Y.; Davidson, L.A.; Gale, O. The Child–Adolescent Perfectionism Scale: Development, Psychometric Properties, and Associations with Stress, Distress, and Psychiatric Symptoms. J. Psychoeduc. Assess. 2016, 34, 634–652. [Google Scholar] [CrossRef]
- Frost, R.O.; Marten, P.; Lahart, C.; Rosenblate, R. The dimensions of perfectionism. Cogn. Ther. Res. 1990, 14, 449–468. [Google Scholar] [CrossRef]
- Vicent, M.; Rubio-Aparicio, M.; Sanchez-Meca, J.; Gonzalvez, C. A reliability generalization meta-analysis of the child and adolescent perfectionism scale. J. Affect. Disord. 2019, 245, 533–544. [Google Scholar] [CrossRef] [Green Version]
- Curran, T.; Hill, A.P. Perfectionism is increasing over time: A meta-analysis of birth cohort differences from 1989 to 2016. Psychol. Bull. 2019, 145, 410–429. [Google Scholar] [CrossRef]
- Martinsen, M.; Sundgot-Borgen, J. Higher Prevalence of Eating Disorders among Adolescent Elite Athletes than Controls. Med. Sci. Sports Exerc. 2013, 45, 1188–1197. [Google Scholar] [CrossRef] [Green Version]
- Flett, G.; Flett, G.; Hewitt, P.L.; Boucher, D.J.; Davidson, L.A.; Munro, Y. Normative Data for Child-Adolescent Perfectionism Scale Subscales of Self-Oriented Perfectionism and Socially Prescribed Perfectionism for Community and Psychiatric Patients; Hewitt Lab, The University of British Columbia: Vancouver, BC, Canada, 2000. [Google Scholar]
- Stornæs, A.V.; Rosenvinge, J.H.; Sundgot-Borgen, J.; Pettersen, G.; Friborg, O. Profiles of Perfectionism Among Adolescents Attending Specialized Elite- and Ordinary Lower Secondary Schools: A Norwegian Cross-Sectional Comparative Study. Front. Psychol. 2019, 10, 2039. [Google Scholar] [CrossRef] [Green Version]
- Downey, C.A.; Reinking, K.R.; Gibson, J.M.; Cloud, J.A.; Chang, E.C. Perfectionistic cognitions and eating disturbance: Distinct mediational models for males and females. Eat. Behav. 2014, 15, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Karazsia, B.T.; Murnen, S.K.; Tylka, T.L. Is Body Dissatisfaction Changing Across Time? A Cross-Temporal Meta-Analysis. Psychol. Bull. 2017, 143, 293–320. [Google Scholar] [CrossRef] [PubMed]
- Henn, A.T.; Taube, C.O.; Vocks, S.; Hartmann, A.S. Body Image as Well as Eating Disorder and Body Dysmorphic Disorder Symptoms in Heterosexual, Homosexual, and Bisexual Women. Front. Psychiatry 2019, 10, 531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tod, D.; Edwards, C.; Hall, G. Drive for leanness and health-related behavior within a social/cultural perspective. Body Image 2013, 10, 640–643. [Google Scholar] [CrossRef]
- Lang, B.; Rancourt, D. Drive for leanness: Potentially less maladaptive compared to drives for thinness and muscularity. Eat. Weight Disord. 2019, 1–11. [Google Scholar] [CrossRef]
- Homan, K. Athletic-ideal and thin-ideal internalization as prospective predictors of body dissatisfaction, dieting, and compulsive exercise. Body Image 2010, 7, 240–245. [Google Scholar] [CrossRef]
- Kelley, C.C.; Neufeld, J.M.; Musher-Eizenman, D.R. Drive for thinness and drive for muscularity: Opposite ends of the continuum or separate constructs? Body Image 2010, 7, 74–77. [Google Scholar] [CrossRef]
- Robinson, L.; Prichard, I.; Nikolaidis, A.; Drummond, C.; Drummond, M.; Tiggemann, M. Idealised media images: The effect of fitspiration imagery on body satisfaction and exercise behaviour. Body Image 2017, 22, 65–71. [Google Scholar] [CrossRef]
- Buckley, G.L.; Hall, L.E.; Lassemillante, A.C.M.; Ackerman, K.E.; Belski, R. Retired Athletes and the Intersection of Food and Body: A Systematic Literature Review Exploring Compensatory Behaviours and Body Change. Nutrients 2019, 11, 1395. [Google Scholar] [CrossRef] [Green Version]
- Keski-Rahkonen, A.; Mustelin, L. Epidemiology of eating disorders in Europe: Prevalence, incidence, comorbidity, course, consequences, and risk factors. Curr. Opin. Psychiatry 2016, 29, 340–345. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | Female Athletes, n = 33 | Female References, n = 28 | p-Level, Effect Size (g) |
|---|---|---|---|
| Age, years | 28.4 (5.6) | 30.2 (6.0) | 0.23 |
| BMI, kg × m−2 | 22.6 (2.0) | 23.1 (2.8) | 0.42 |
| Bodyfat, % | 24.6 (5.9) | 28.4 (5.7) | 0.02, g = 0.65 |
| Previous eating disorder *, n (%) | 9 (28%) | 3 (11%) | 0.09 |
| Current eating disorder *, n (%) | 2 (6%) | 1 (4%) | 0.89 |
| EDE-q, total score | 1.3 (0.8) | 1.0 (1.1) | 0.30 |
| REI Subscale | Fitness Athletes | Female References | ||||
|---|---|---|---|---|---|---|
| T1 n = 33 | T2 n = 22 | T3 n = 22 | T1 n = 28 | T2 n = 24 | T3 n = 24 | |
| Weight control | 2.3 (1.8, 2.8) | ns | ns | 2.4 (1.8, 2.9) | ns | ns |
| Fitness function | 4.5 (4.1, 5.0) | ns | ns | 4.4 (3.9, 4.9) | ns | ns |
| Mood regulation | 4.8 (4.2, 5.4) - | 4.2 (3.5, 4.9) p = 0.005 g = 0.5 | ns | 5.0 (4.3, 5.6) - | 4.2 (3.5, 4.9) p = 0.001 g = 0.8 | 4.3 (3.7, 5.0) p = 0.002 g = −0.1 |
| Health enhancement | 4.8 (4.3, 5.3) | ns | ns | 4.8 (4.3, 5.3) | ns - | ns - |
| Attractiveness | 3.4 (2.8, 4.0) - | 2.9 (2.2, 3.5) p = 0.008 g = 0.5 | ns | 3.0 (2.4, 3.6) | ns | ns |
| Enjoyment | 4.1 (3.6, 4.6) - | ns | ns | 3.8 (3.2, 4.4) - | 4.3 (3.7, 4.9) p = 0.01 g = −0.6 | ns |
| Figure toning | 3.7 (3.1, 4.2) $ - | 3.8 (3.2, 4.5) * ns | 4.0 (3.3, 4.6) # ns | 2.8 (2.2, 3.5) $ - | 2.9 (2.3, 3.6) * ns | 2.9 (2.2, 3.5) # ns |
| Correlations | EDE-q | BES | UE | EE | CR | EC | ER | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T1 | T2 | T3 | T1 | T2 | T3 | T1 | T2 | T3 | T1 | T2 | T3 | T1 | T2 | T3 | T1 | T2 | T3 | T1 | T2 | T3 | ||
| DFL | FA | 0.4 0.01 | 0.6 0.002 | 0.6 0.003 | 0.5 0.01 | 0.5 0.002 | 0.6 0.008 | 0.7 0.001 | 0.5 0.01 | 0.4 0.01 | ||||||||||||
| FR | 0.5 0.007 | 0.7 <0.001 | 0.6 0.002 | 0.6 0.002 | 0.6 0.002 | 0.6 0.001 | 0.5 0.01 | 0.6 0.005 | 0.6 0.002 | 0.5 0.003 | 0.6 0.002 | 0.5 0.006 | 0.5 0.01 | |||||||||
| DM | FA | −0.5 0.009 | −0.6 0.007 | −0.5 0.004 | −0.6 0.001 | −0.5 0.01 | −0.6 0.001 | |||||||||||||||
| FR | −0.5 0.005 | −0.7 <0.001 | −0.7 <0.001 | −0.8 <0.001 | −0.6 0.007 | −0.7 0.001 | −0.5 0.01 | −0.6 0.001 | −0.8 <0.001 | −0.7 <0.001 | −0.6 0.003 | −0.6 0.002 | ||||||||||
| C-self | FA | 0.5 0.004 | .5 .006 | 0.6 <0.001 | 0.5 0.009 | |||||||||||||||||
| FR | 0.5 0.007 | |||||||||||||||||||||
| C-social | FA | 0.6 0.002 | 0.5 0.003 | 0.6 0.006 | 0.6 0.004 | 0.6 0.004 | ||||||||||||||||
| FR | 0.5 0.008 | 0.5 0.01 | ||||||||||||||||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mathisen, T.F.; Sundgot-Borgen, J. Mental Health Symptoms Related to Body Shape Idealization in Female Fitness Physique Athletes. Sports 2019, 7, 236. https://doi.org/10.3390/sports7110236
Mathisen TF, Sundgot-Borgen J. Mental Health Symptoms Related to Body Shape Idealization in Female Fitness Physique Athletes. Sports. 2019; 7(11):236. https://doi.org/10.3390/sports7110236
Chicago/Turabian StyleMathisen, Therese Fostervold, and Jorunn Sundgot-Borgen. 2019. "Mental Health Symptoms Related to Body Shape Idealization in Female Fitness Physique Athletes" Sports 7, no. 11: 236. https://doi.org/10.3390/sports7110236
APA StyleMathisen, T. F., & Sundgot-Borgen, J. (2019). Mental Health Symptoms Related to Body Shape Idealization in Female Fitness Physique Athletes. Sports, 7(11), 236. https://doi.org/10.3390/sports7110236