
Predictive Factors of Recovery after an Acute Lateral Ankle Sprain: A Longitudinal Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Rationale
2.2. Participants
2.3. Procedure
2.4. Outcome Assessment
- Edema: To assess edema (joint swelling), we measured circumference (tape measure) of the ankle at the level of both malleoli and foot circumference, midway between the lateral malleolus and the base of the second metatarsal [21]. These measurements were repeated for both healthy and injured ankles. The selected values were the percent differences between sides;
- Joint mobility: Passive ankle ROM was measured with a manual goniometer (GIMA S.p.A, Gessate (MI), Italy). Both plantar and dorsal flexion were tested. Dorsal flexion was measured in both an extended knee position and a 90° flexed knee position [22]. These measurements were repeated for both healthy and injured ankles. The selected values were the percent differences between sides;
- Muscle strength: The maximum isometric muscle strength of the ankle’s plantar and dorsal flexor, invertor, and evertor was measured with a handheld dynamometer (microFET2 Hoggan Scientific, Salt Lake City, UT, USA). The foot was placed in a neutral position, and the examiner held the dynamometer stationary while the patient exerted maximal force against it. The dynamometer was positioned as recommended by Spink et al. [23]. Each measurement was taken three times and the maximum result was recorded. These measurements were repeated for both healthy and injured ankles. The selected values were the percent differences between sides;
- Self-reported pain: Pain was evaluated by means of a visual analogue scale (VAS) both at rest and while walking [24]. Each patient marked a point on a 10-cm line, ranging from zero for “no pain” to ten for “severe pain”;
- Self-reported physical function of the ankle: Ankle function was evaluated with the FAAM questionnaire, which is a valid and reliable self-report questionnaire for patients with foot and ankle disorders [25,26]. This questionnaire consists of 21 items concerning ADL and eight items concerning sports activities. The final score is represented as a percentage from 0 to 100, and a higher score indicates a higher functional level. The minimal clinically important difference is eight points for the ADL subscale and nine points for the sport subscale.
2.5. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Beynnon, B.D.; Renström, P.A.; Alosa, D.M.; Baumhauer, J.F.; Vacek, P.M. Ankle ligament injury risk factors: A prospective study of college athletes. J. Orthop. Res. 2001, 19, 213–220. [Google Scholar] [CrossRef]
- Czajka, C.M.; Tran, E.; Cai, A.N.; DiPreta, J.A. Ankle Sprains and Instability. Med. Clin. N. Am. 2014, 98, 313–329. [Google Scholar] [CrossRef] [PubMed]
- Waterman, B.R.; Owens, B.D.; Davey, S.; Zacchilli, M.A.; Belmont, J.P.J. The Epidemiology of Ankle Sprains in the United States. J. Bone Jt. Surg. Am. Vol. 2010, 92, 2279–2284. [Google Scholar] [CrossRef] [Green Version]
- Shah, S.; Thomas, A.C.; Noone, J.M.; Blanchette, C.M.; Wikstrom, E.A. Incidence and Cost of Ankle Sprains in United States Emergency Departments. Sports Heal. A Multidiscip. Approach 2016, 8, 547–552. [Google Scholar] [CrossRef] [Green Version]
- Hootman, J.M.; Dick, R.; Agel, J. Epidemiology of Collegiate Injuries for 15 Sports: Summary and Recommendations for Injury Prevention Initiatives. J. Athl. Train. 2007, 42, 311–319. [Google Scholar] [PubMed]
- Doherty, C.; Delahunt, E.; Caulfield, B.; Hertel, J.; Ryan, J.; Bleakley, C.J. The Incidence and Prevalence of Ankle Sprain Injury: A Systematic Review and Meta-Analysis of Prospective Epidemiological Studies. Sports Med. 2014, 44, 123–140. [Google Scholar] [CrossRef] [PubMed]
- Rinonapoli, G.; Graziani, M.; Ceccarini, P.; Razzano, C.; Manfreda, F.; Caraffa, A. Epidemiology of injuries connected with dance: A critical review on epidemiology. Med. Glas 2020, 17, 256–264. [Google Scholar]
- McCriskin, B.J.; Cameron, K.L.; Orr, J.D.; Waterman, B.R. Management and prevention of acute and chronic lateral ankle instability in athletic patient populations. World J. Orthop. 2015, 6, 161–171. [Google Scholar] [CrossRef]
- Vuurberg, G.; Hoorntje, A.; Wink, L.M.; Van Der Doelen, B.F.W.; Bekerom, M.P.V.D.; Dekker, R.; Van Dijk, C.N.; Krips, R.; Loogman, M.C.M.; Ridderikhof, M.L.; et al. Diagnosis, treatment and prevention of ankle sprains: Update of an evidence-based clinical guideline. Br. J. Sports Med. 2018, 52, 956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maffulli, N.; Ferran, N.A. Management of Acute and Chronic Ankle Instability. J. Am. Acad. Orthop. Surg. 2008, 16, 608–615. [Google Scholar] [CrossRef] [Green Version]
- Doherty, C.; Bleakley, C.; Delahunt, E.; Holden, S. Treatment and prevention of acute and recurrent ankle sprain: An overview of systematic reviews with meta-analysis. Br. J. Sports Med. 2016, 51, 113–125. [Google Scholar] [CrossRef]
- Polzer, H.; Kanz, K.G.; Prall, W.C.; Haasters, F.; Ockert, B.; Mutschler, W.; Grote, S. Diagnosis and treatment of acute ankle injuries: Development of an evidence-based algorithm. Orthop. Rev. 2011, 4, e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiller, C.E.; Nightingale, E.J.; Raymond, J.; Kilbreath, S.L.; Burns, J.; Black, D.A.; Refshauge, K.M. Prevalence and Impact of Chronic Musculoskeletal Ankle Disorders in the Community. Arch. Phys. Med. Rehabil. 2012, 93, 1801–1807. [Google Scholar] [CrossRef] [PubMed]
- Gribble, P.A.; Bleakley, C.M.; Caulfield, B.M.; Docherty, C.L.; Fourchet, F.; Fong, D.T.-P.; Hertel, J.; Hiller, C.E.; Kaminski, T.W.; McKeon, P.O.; et al. Evidence review for the 2016 International Ankle Consortium consensus statement on the prevalence, impact and long-term consequences of lateral ankle sprains. Br. J. Sports Med. 2016, 50, 1496–1505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Rijn, R.M.; Van Os, A.G.; Bernsen, R.M.; Luijsterburg, P.A.; Koes, B.W.; Bierma-Zeinstra, S.M. What Is the Clinical Course of Acute Ankle Sprains? A Systematic Literature Review. Am. J. Med. 2008, 121, 324–331.e7. [Google Scholar] [CrossRef] [PubMed]
- Van Ochten, J.M.; Mos, M.C.; Van Putte-Katier, N.; Oei, E.H.; Bindels, P.J.; Bierma-Zeinstra, S.M.; Van Middelkoop, M. Structural abnormalities and persistent complaints after an ankle sprain are not associated: An observational case control study in primary care. Br. J. Gen. Pr. 2014, 64, e545–e553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, J.Y.; Byrne, C.; Williams, M.A.; Keene, D.J.; Schlussel, M.M.; Lamb, S.E. Prognostic factors for recovery following acute lateral ankle ligament sprain: A systematic review. BMC Musculoskelet. Disord. 2017, 18, 421. [Google Scholar] [CrossRef] [Green Version]
- Punt, I.M.; Ziltener, J.-L.; Monnin, D.; Allet, L. Wii Fit™ exercise therapy for the rehabilitation of ankle sprains: Its effect compared with physical therapy or no functional exercises at all. Scand. J. Med. Sci. Sports 2015, 26, 816–823. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, S.R.; Bleakley, C.M.; Tully, M.A.; McDonough, S.M. Predicting Functional Recovery after Acute Ankle Sprain. PLoS ONE 2013, 8, e72124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wikstrom, E.A.; Brown, C.N. Minimum Reporting Standards for Copers in Chronic Ankle Instability Research. Sports Med. 2013, 44, 251–268. [Google Scholar] [CrossRef]
- Mawdsley, R.H.; Hoy, D.K.; Erwin, P.M. Criterion-Related Validity of the Figure-of-Eight Method of Measuring Ankle Edema. J. Orthop. Sports Phys. Ther. 2000, 30, 149–153. [Google Scholar] [CrossRef]
- Elveru, R.A.; Rothstein, J.M.; Lamb, R.L. Goniometric Reliability in a Clinical Setting. Phys. Ther. 1988, 68, 672–677. [Google Scholar] [CrossRef]
- Spink, M.J.; Fotoohabadi, M.R.; Menz, H.B. Foot and Ankle Strength Assessment Using Hand-Held Dynamometry: Reliability and Age-Related Differences. Gerontology 2010, 56, 525–532. [Google Scholar] [CrossRef]
- Bijur, P.E.; Silver, W.; Gallagher, E.J. Reliability of the Visual Analog Scale for Measurement of Acute Pain. Acad. Emerg. Med. 2001, 8, 1153–1157. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.L.; Irrgang, J.J.; Burdett, R.G.; Conti, S.F.; Van Swearingen, J.M. Evidence of Validity for the Foot and Ankle Ability Measure (FAAM). Foot Ankle Int. 2005, 26, 968–983. [Google Scholar] [CrossRef]
- Borloz, S.; Crevoisier, X.; Deriaz, O.; Ballabeni, P.; Martin, R.L.; Luthi, F. Evidence for validity and reliability of a french version of the FAAM. BMC Musculoskelet. Disord. 2011, 12, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breiman, L. Random Forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Hothorn, T.; Hornik, K.; Zeileis, A. Unbiased Recursive Partitioning: A Conditional Inference Framework. J. Comput. Graph. Stat. 2006, 15, 651–674. [Google Scholar] [CrossRef] [Green Version]
- Strobl, C.; Boulesteix, A.-L.; Zeileis, A.; Hothorn, T. Bias in random forest variable importance measures: Illustrations, sources and a solution. BMC Bioinform. 2007, 8, 25. [Google Scholar] [CrossRef] [Green Version]
- Strobl, C.; Hothorn, T.; Zeileis, A. Party On! R J. 2009, 1, 14–17. [Google Scholar] [CrossRef]
- Strobl, C.; Boulesteix, A.-L.; Kneib, T.; Augustin, T.; Zeileis, A. Conditional variable importance for random forests. BMC Bioinform. 2008, 9, 307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strobl, C.; Malley, J.; Tutz, G. An introduction to recursive partitioning: Rationale, application, and characteristics of classification and regression trees, bagging, and random forests. Psychol. Methods 2009, 14, 323–348. [Google Scholar] [CrossRef] [Green Version]
- Boulesteix, A.-L.; Janitza, S.; Hapfelmeier, A.; Van Steen, K.; Strobl, C. Letter to the Editor: On the term ’interaction’ and related phrases in the literature on Random Forests. Briefings Bioinform. 2015, 16, 338–345. [Google Scholar] [CrossRef] [PubMed]
- Van Middelkoop, M.; Van Rijn, R.M.; Verhaar, J.A.; Koes, B.W.; Bierma-Zeinstra, S.M. Re-sprains during the first 3 months after initial ankle sprain are related to incomplete recovery: An observational study. J. Physiother. 2012, 58, 181–188. [Google Scholar] [CrossRef] [Green Version]
- Kemler, E.; Thijs, K.M.; Badenbroek, I.; Van De Port, I.G.L.; Hoes, A.W.; Backx, F.J.G. Long-term prognosis of acute lateral ankle ligamentous sprains: High incidence of recurrences and residual symptoms. Fam. Pr. 2016, 33, 596–600. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.W.; Gansneder, B.M. Measures of Functional Limitation as Predictors of Disablement in Athletes with Acute Ankle Sprains. J. Orthop. Sports Phys. Ther. 2000, 30, 528–535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cross, K.M.; Worrell, T.W.; Leslie, J.E.; Khalid, R.V.V. The Relationship Between Self-Reported and Clinical Measures and the Number of Days to Return to Sport Following Acute Lateral Ankle Sprains. J. Orthop. Sports Phys. Ther. 2002, 32, 16–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Bie, R.; De Vet, H.; Wildenberg, F.V.D.; Lenssen, T.; Knipschild, P. The Prognosis of Ankle Sprains. Int. J. Sports Med. 1997, 18, 285–289. [Google Scholar] [CrossRef]
- Van Der Wees, P.; Hendriks, E.; Van Beers, H.; Van Rijn, R.; Dekker, J.; De Bie, R. Validity and responsiveness of the ankle function score after acute ankle injury. Scand. J. Med. Sci. Sports 2010, 22, 170–174. [Google Scholar] [CrossRef]
- Lorenzo-Sánchez-Aguilera, C.; Rodríguez-Sanz, D.; Gallego-Izquierdo, T.; Lázaro-Navas, I.; Plaza-Rodríguez, J.; Navarro-Santana, M.; Pecos-Martín, D. Neuromuscular Mechanosensitivity in Subjects with Chronic Ankle Sprain: A Cross-Sectional Study. Pain Med. 2020, 21, 1991–1998. [Google Scholar] [CrossRef]
- Briet, J.P.; Houwert, R.M.; Hageman, M.G.; Hietbrink, F.; Ring, D.C.; Verleisdonk, E.J.J. Factors associated with pain intensity and physical limitations after lateral ankle sprains. Injury 2016, 47, 2565–2569. [Google Scholar] [CrossRef]
- Pierik, J.; Ijzerman, M.; Gaakeer, M.; Vollenbroek-Hutten, M.; van Vugt, A.; Doggen, C. Incidence and prognostic factors of chronic pain after isolated musculoskeletal extremity injury. Eur. J. Pain 2015, 20, 711–722. [Google Scholar] [CrossRef] [Green Version]
- Crombez, G.; Eccleston, C.; Van Damme, S.; Vlaeyen, J.W.; Karoly, P. Fear-Avoidance Model of Chronic Pain. Clin. J. Pain 2012, 28, 475–483. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variables | Recovered (n = 27) | Not Recovered (n = 25) | ||
|---|---|---|---|---|
| n | Mean (SD) or % | n | Mean (SD) or % | |
| Age (year) | 27 | 34 (9) | 25 | 36 (12) |
| BMI (kg/m2) | 27 | 26.2 (4.3) | 25 | 26.0 (4.3) |
| Sex | 27 | 25 | ||
| Male | 16 | 59% | 13 | 52% |
| Female | 11 | 41% | 12 | 48% |
| Severity | 27 | 25 | ||
| Grade I | 18 | 67% | 15 | 30% |
| Grade II | 9 | 33% | 10 | 40% |
| Previous sprain | 27 | 24 | ||
| Yes | 16 | 59% | 16 | 67% |
| No | 11 | 41% | 8 | 33% |
| Sport practice | 27 | 25 | ||
| Yes | 23 | 85% | 19 | 76% |
| No | 4 | 15% | 6 | 24% |
| High-load sport | 27 | 24 | ||
| Yes | 14 | 52% | 11 | 46% |
| No | 9 | 48% | 13 | 54% |
| Measurements | Recovered (n = 27) | Not Recovered (n = 25) | ||
|---|---|---|---|---|
| n | Median (1st and 3rd Quartiles) or % | n | Median (1st and 3rd Quartiles) or % | |
| Edema (%) | ||||
| Ankle | 27 | 4.1 (−3.0 – 10.6) | 24 | 2.1 (−3.9 – 8.8) |
| Foot | 27 | 2.0 (−4.1 – 8.5) | 24 | 2.1 (−6.0 – 6.3) |
| Range of motion (%) | ||||
| Dorsiflexion | 25 | −16.7 (−33.3 – −6.9) | 25 | −25.0 (−60.0 – 0.0) |
| Dorsiflexion 90° | 27 | −16.7 (−27.6 – −4.9) | 25 | −20.0 (−40.0 – −9.7) |
| Plantar flexion | 27 | −16.7 (−22.0 – −5.6) | 25 | −9.1 (−18.4 – 0.0) |
| Strength (%) | ||||
| Dorsiflexion | 27 | −20.0 (−27.1 – −2.3) | 25 | −13.3 (−33.7 – −7.2) |
| Plantar flexion | 27 | −14.0 (−20.3 – −1.6) | 25 | −15.3 (−31.9 – −1.5) |
| Inversion | 27 | −9.9 (−43.6 – −2.5) | 25 | −12.8 (−43.2 – −5.4) |
| Eversion | 27 | −22.1 (−37.1 – −6.9) | 25 | −15.4 (−23.0 – −2.7) |
| Pain (VAS 0–10) | ||||
| Rest | 27 | 0.2 (0.0 – 1.0) | 25 | 0.5 (0.0 – 2.0) |
| Walking | 27 | 1.1 (0.1 – 2.0) | 25 | 2.4 (1.5 – 4.9) |
| Ankle function (0–100) | ||||
| FAAM ADL | 27 | 86.9 (71.9 – 94.6) | 25 | 73.8 (61.9 – 86.3) |
| FAAM Sport | 27 | 46.9 (28.1 – 72.5) | 25 | 40.6 (12.5 – 56.3) |
| Intervention | ||||
| Physical therapy | 12 | 44% | 9 | 36% |
| Wii fit™ | 5 | 19% | 10 | 40% |
| No treatment | 10 | 37% | 6 | 24% |
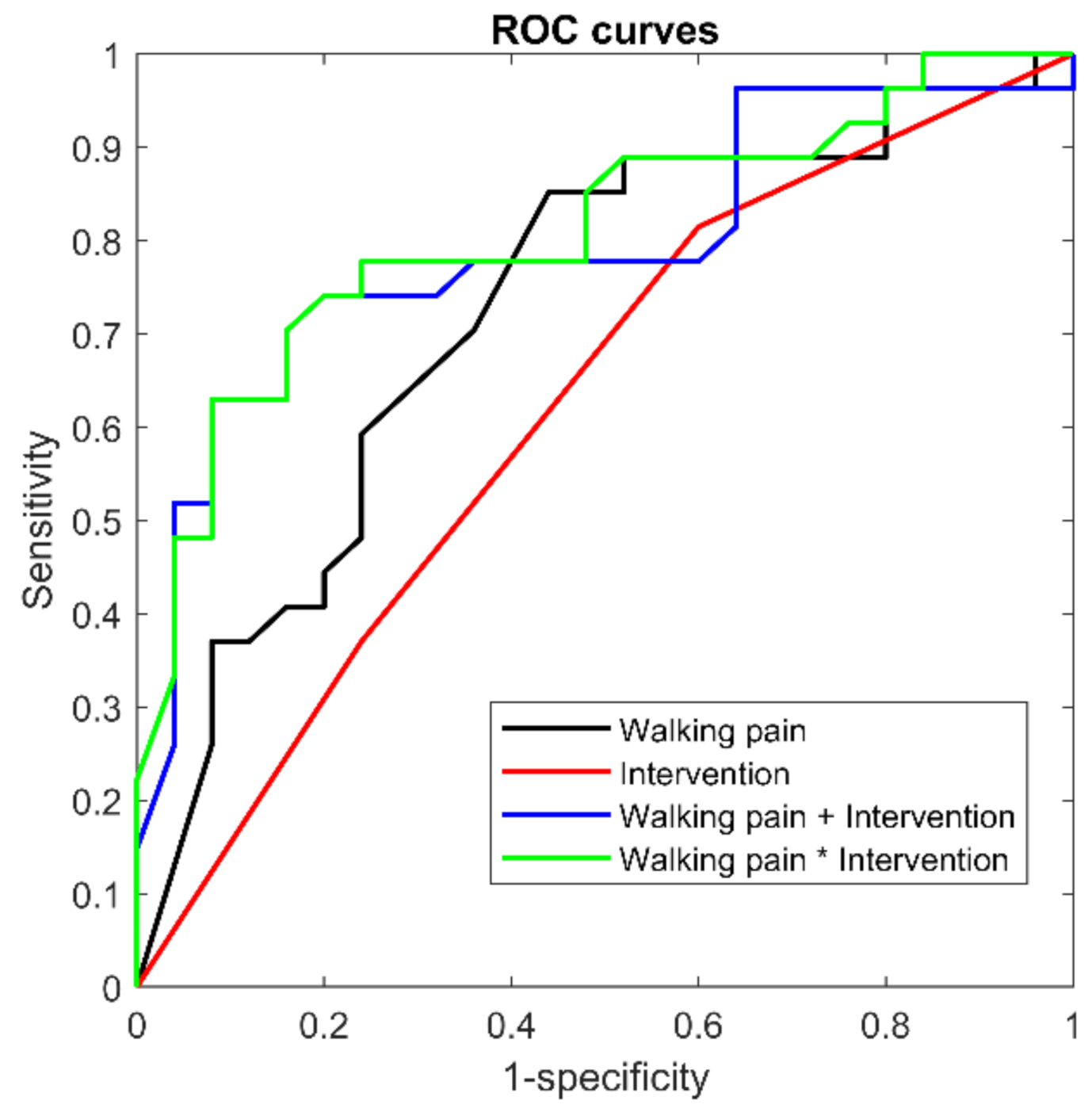
| n = 52 | Model | BIC | AUC | AUC CI | |
|---|---|---|---|---|---|
| Simple regressions | walking pain | 72.9 | 0.73 | 0.57 | 0.85 |
| intervention | 80.8 | 0.62 | 0.45 | 0.75 | |
| Multivariable regressions | without interaction | 77.1 | 0.79 | 0.65 | 0.90 |
| (pain and intervention) | with interaction | 79.0 | 0.81 | 0.66 | 0.91 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Terrier, P.; Piotton, S.; Punt, I.M.; Ziltener, J.-L.; Allet, L. Predictive Factors of Recovery after an Acute Lateral Ankle Sprain: A Longitudinal Study. Sports 2021, 9, 41. https://doi.org/10.3390/sports9030041
Terrier P, Piotton S, Punt IM, Ziltener J-L, Allet L. Predictive Factors of Recovery after an Acute Lateral Ankle Sprain: A Longitudinal Study. Sports. 2021; 9(3):41. https://doi.org/10.3390/sports9030041
Chicago/Turabian StyleTerrier, Philippe, Sébastien Piotton, Ilona M. Punt, Jean-Luc Ziltener, and Lara Allet. 2021. "Predictive Factors of Recovery after an Acute Lateral Ankle Sprain: A Longitudinal Study" Sports 9, no. 3: 41. https://doi.org/10.3390/sports9030041
APA StyleTerrier, P., Piotton, S., Punt, I. M., Ziltener, J.-L., & Allet, L. (2021). Predictive Factors of Recovery after an Acute Lateral Ankle Sprain: A Longitudinal Study. Sports, 9(3), 41. https://doi.org/10.3390/sports9030041