



A Review of Surgical Bone Drilling and Drill Bit Heat Generation for Implantation


 , , ,
, , ,  and
and
Abstract
:1. Introduction
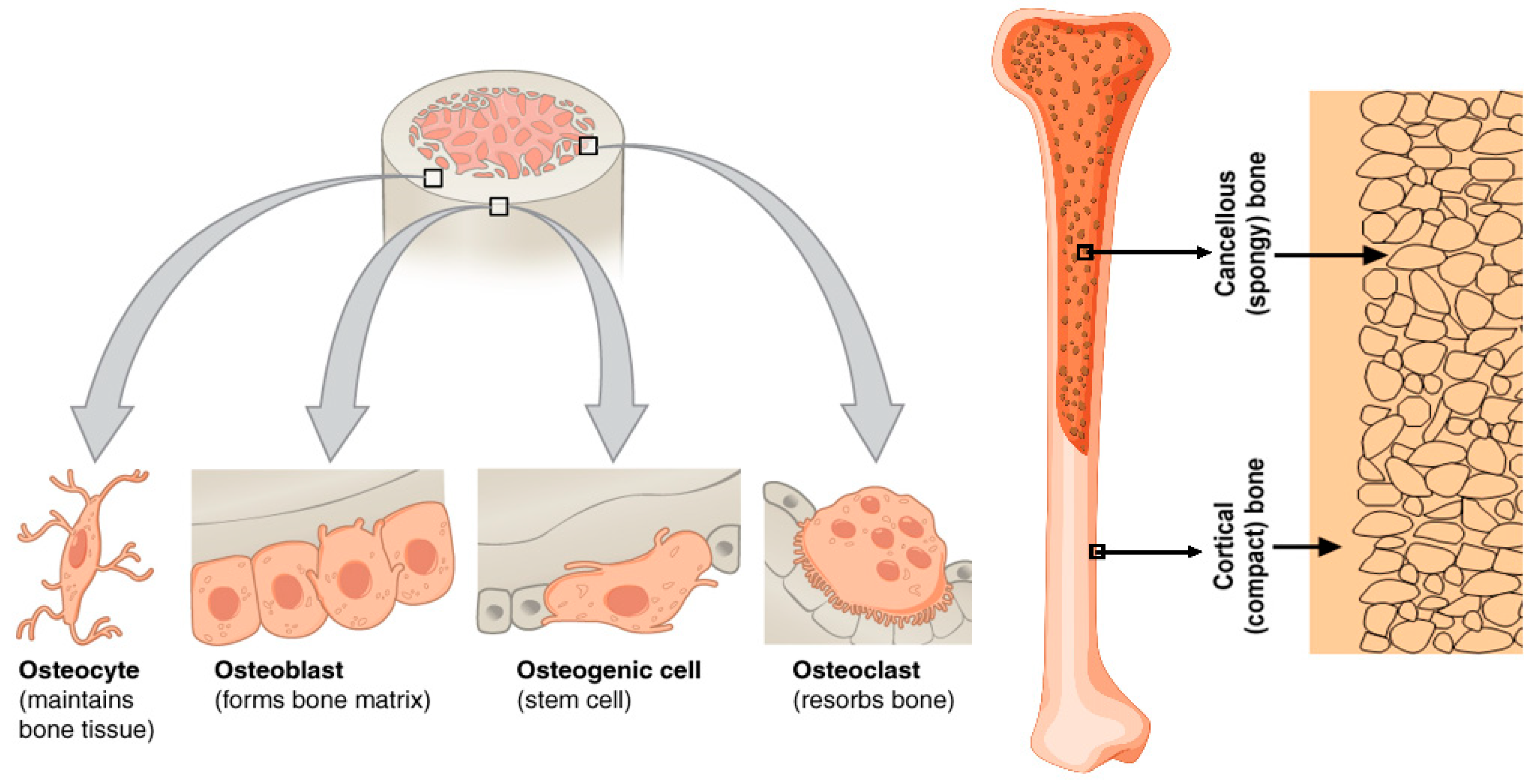
2. Bone Anatomy and Biomechanical Properties
3. Thermomechanical Properties of Bone Tissue
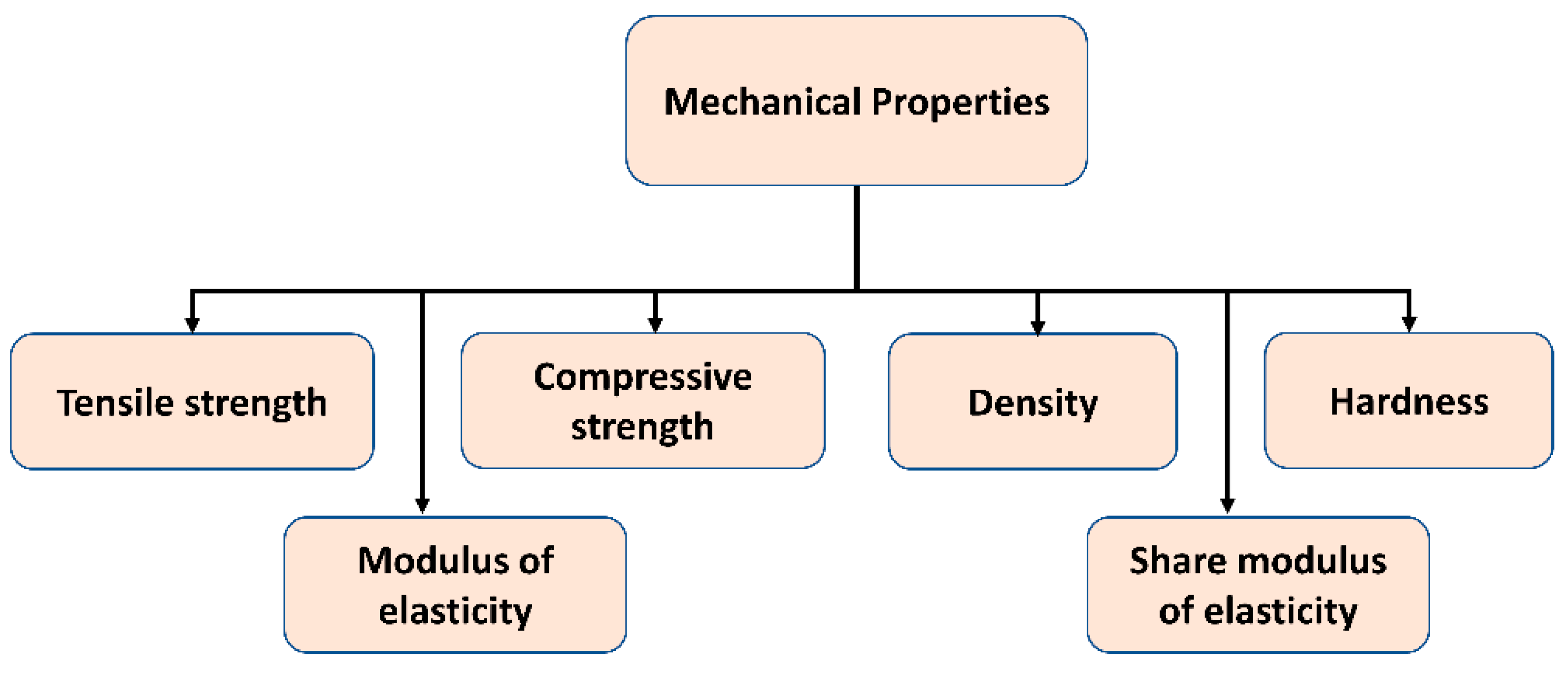
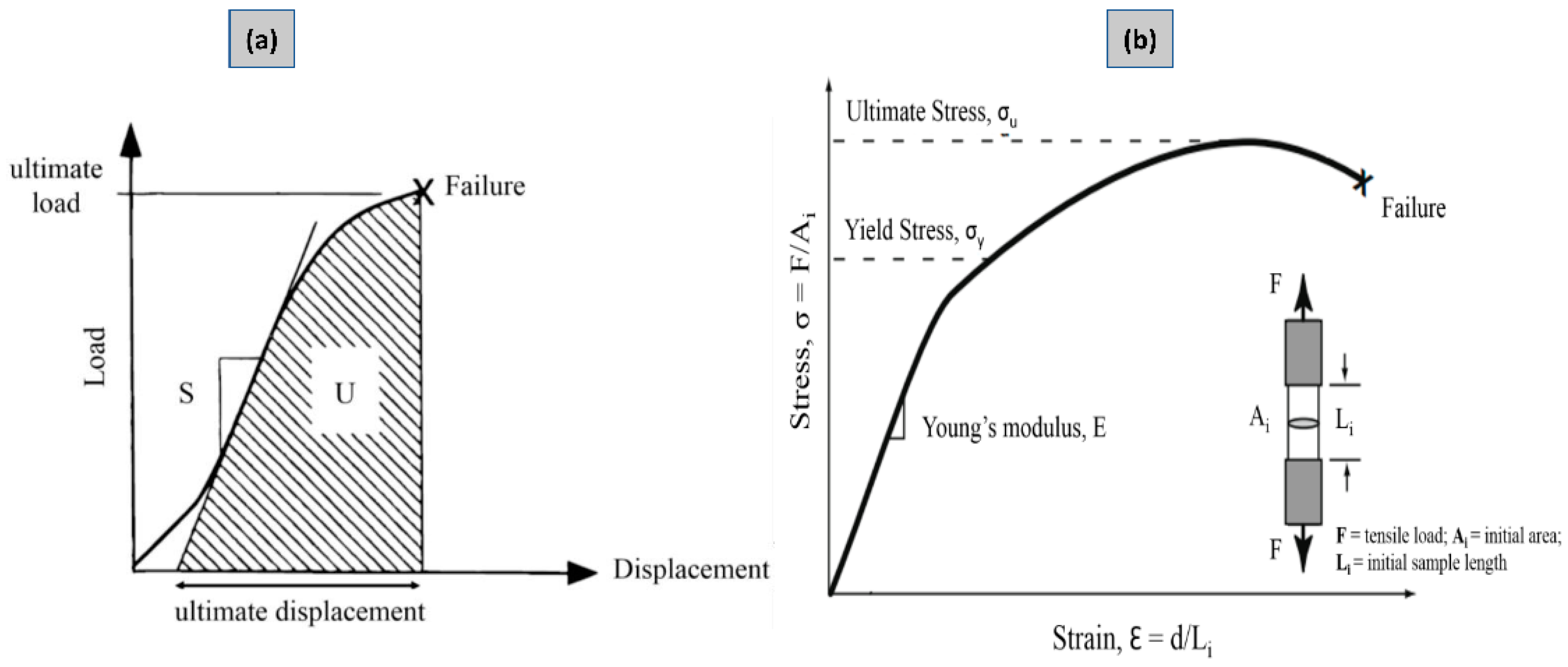
3.1. Mechanical Properties
3.2. Thermal Osteonecrosis Analysis
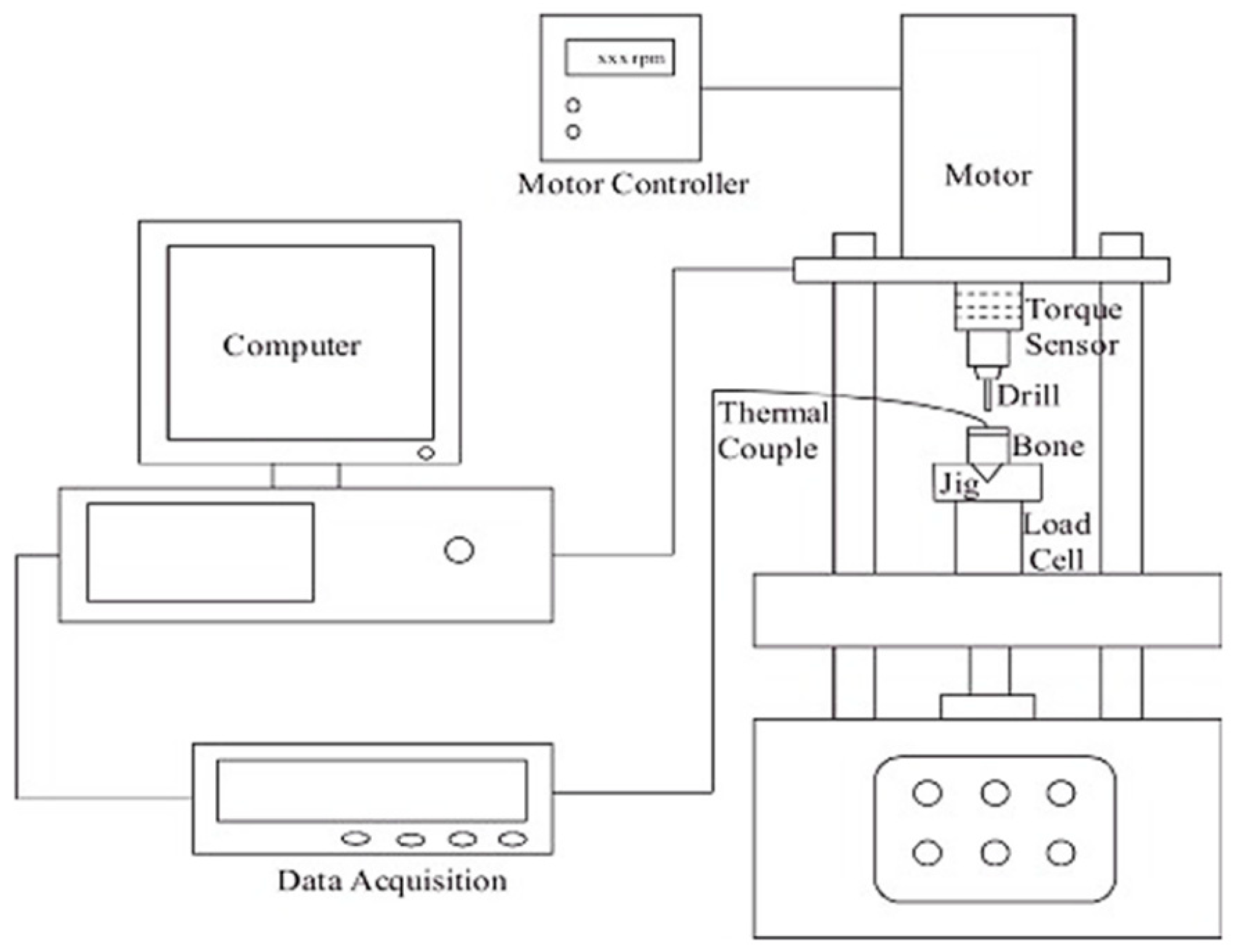
4. Surgical Bone Drilling Practice
5. Conventional and Non-Conventional Bone Drilling
- Researchers undertake numerous tests to determine the effect of various parameters (feed rate, drill bit shape, spindle speed, and bone structure) and output reactions (such as temperature, thrust force, surface roughness, and delamination).
- Conventional bone drilling raises the temperature of the bone, and a temperature greater than 47 °C is dangerous because it leads to thermal bone necrosis. Researchers have examined the influence of machining parameters on bone tissue thermal damage.
- Delamination studies: The primary purpose of these investigations is to alleviate delamination caused by bone hole drilling.
- Effects of tool materials, drill bit shape, and tool wear on the quality of holes and thrust forces induced during bone drilling.
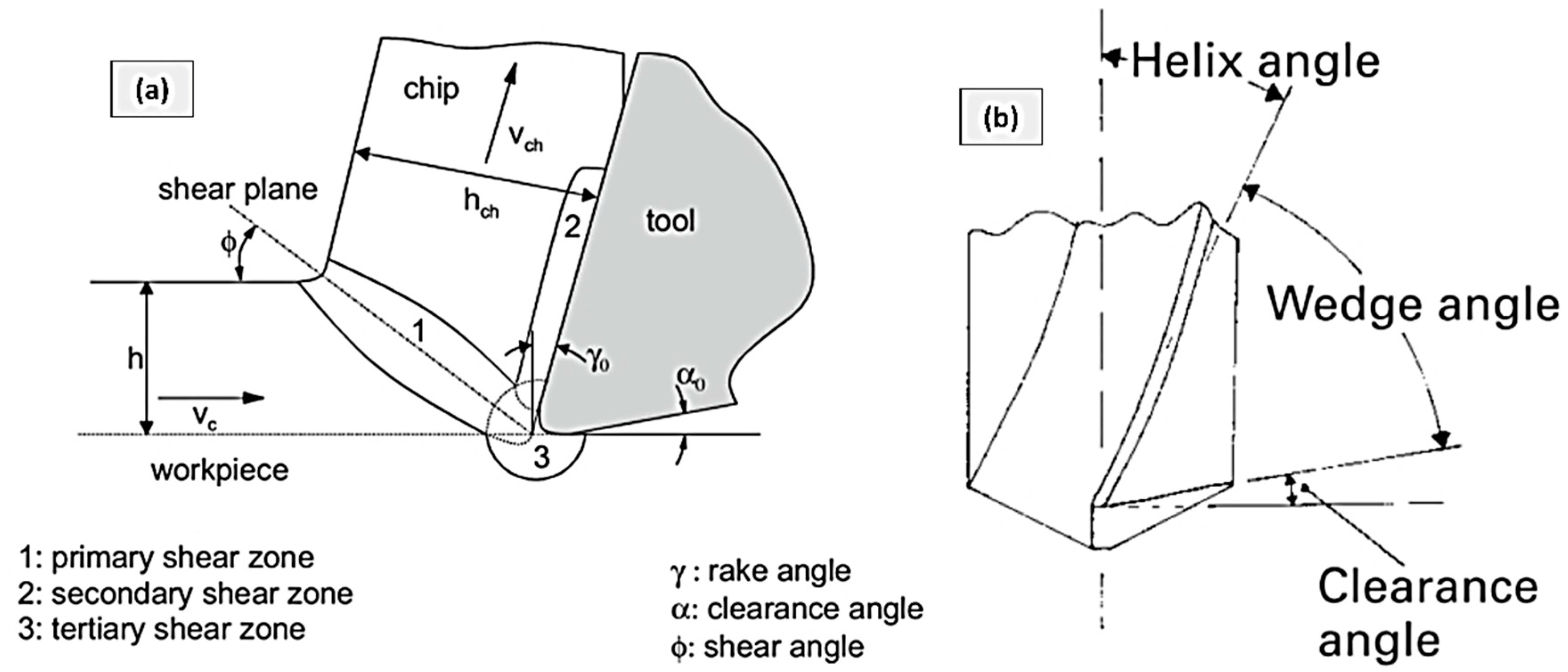
6. Bone Drilling Heat Generation
- The primary sources of heat are shear deformation of the work material (1), friction between the cutting chips from the work material and the rake face of the cutting tool (2), and friction between the cutting edge and the under surface of the work material that touches the relief face of the cutting tool (3).
- Secondly, the indirect heat sources are simply driven by friction between cutting chips, particularly between bone chips and flutes, or between bone chips and the drilled wall of the work material when travelling the flute.
7. Characterization of Bone Drilling
7.1. Cutting Temperature
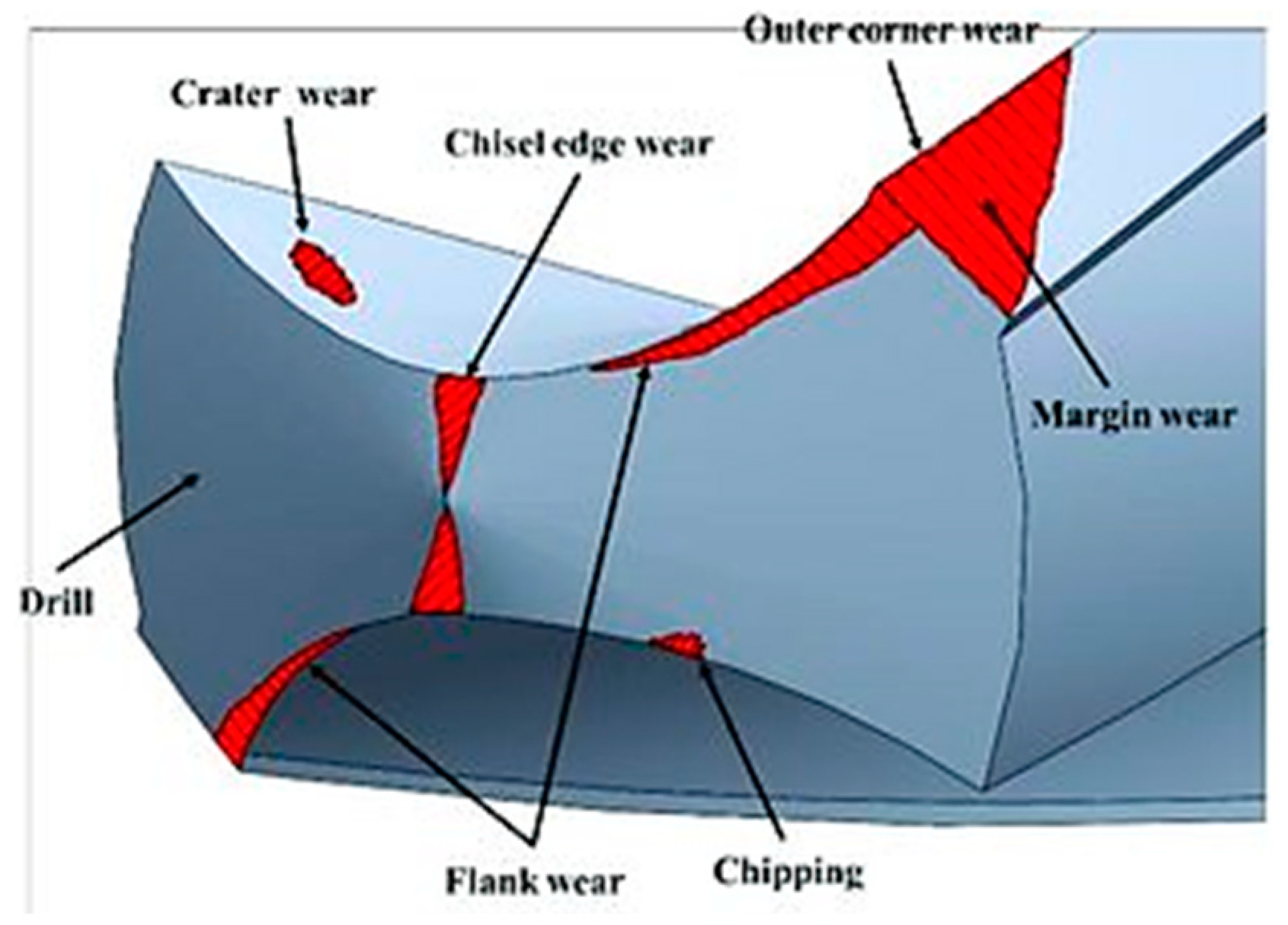
7.2. Cutting Tool Wear
7.3. Exposure Time
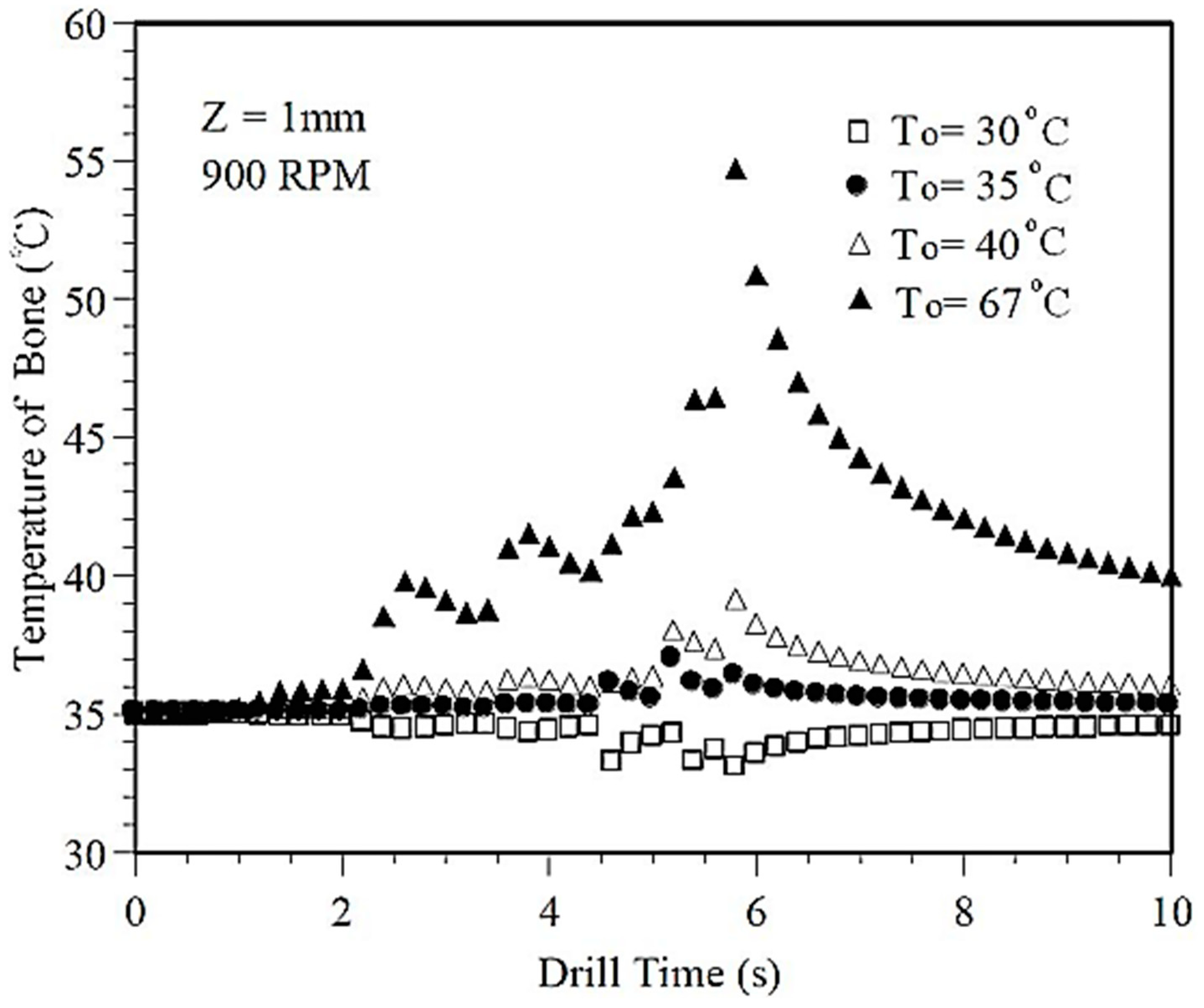
7.4. Initial Temperature of the Drill Bit
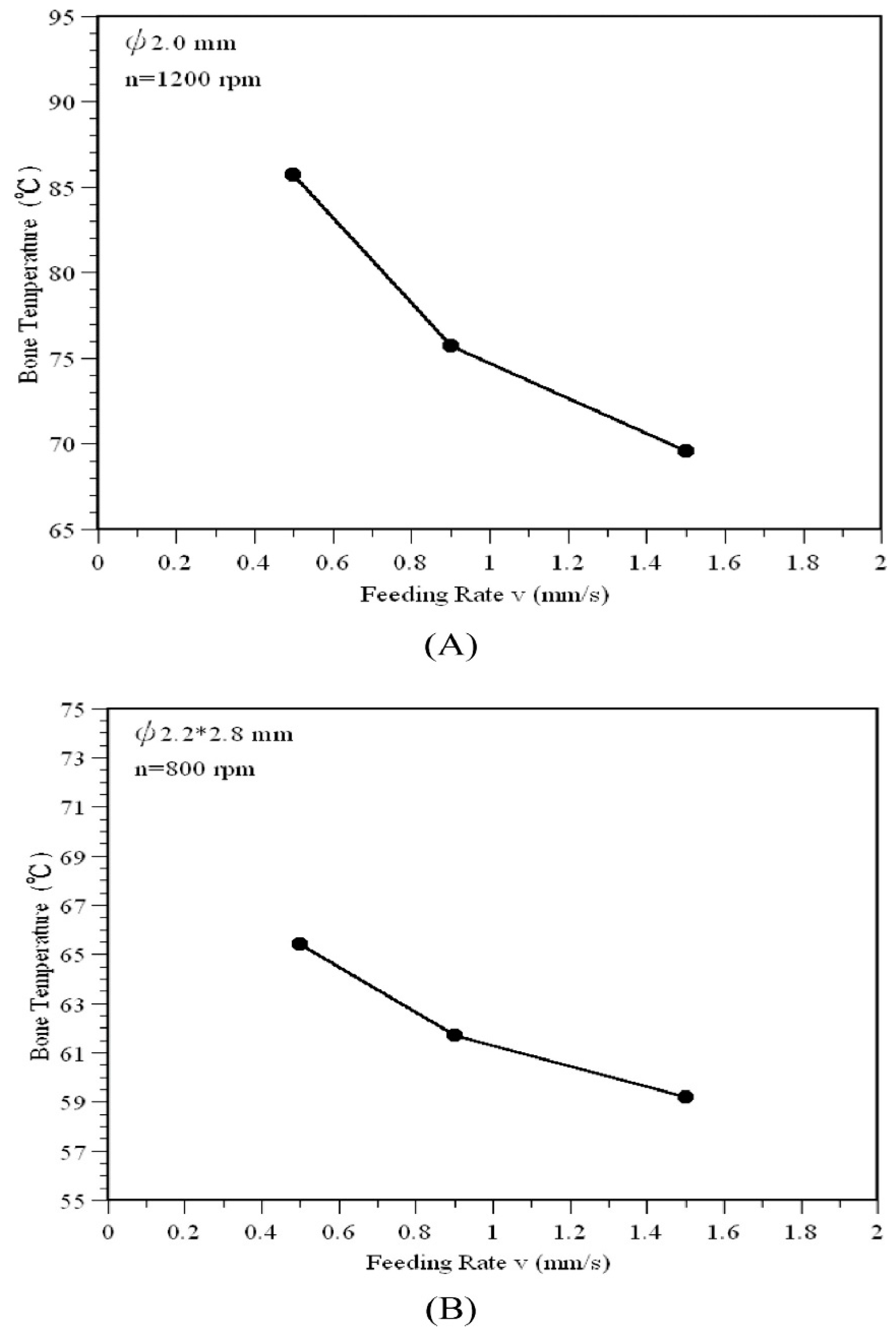
7.5. The Effect of Feed Rate
7.6. Drilling Speed
7.7. The Effect of Coolants
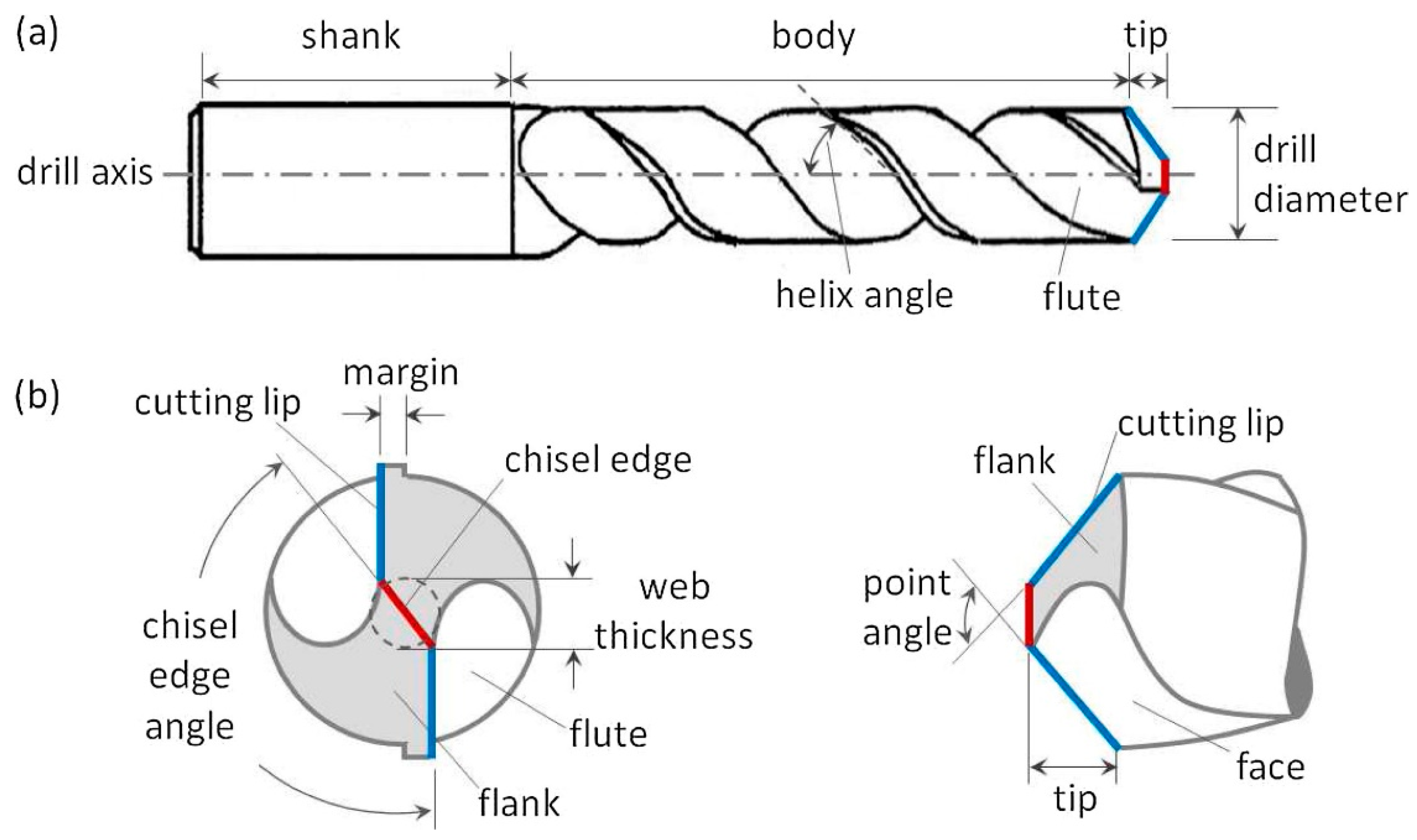
8. Surgical Drill Bit Geometry
8.1. Drill Diameter and Predrilling
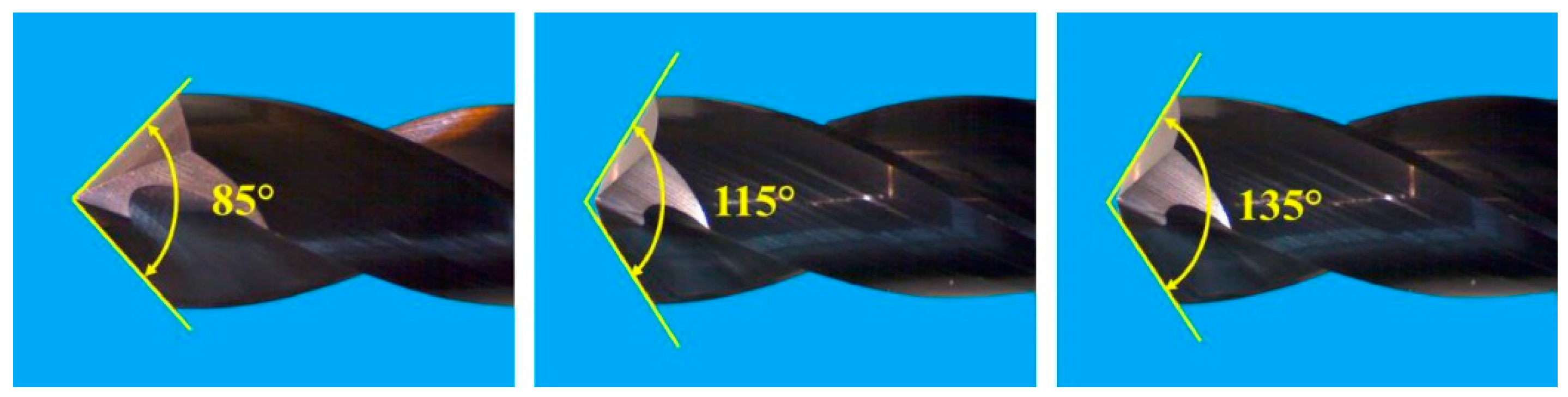
8.2. Point Angle
8.3. Drill Bit Helix Angle
8.4. Clearance Angle
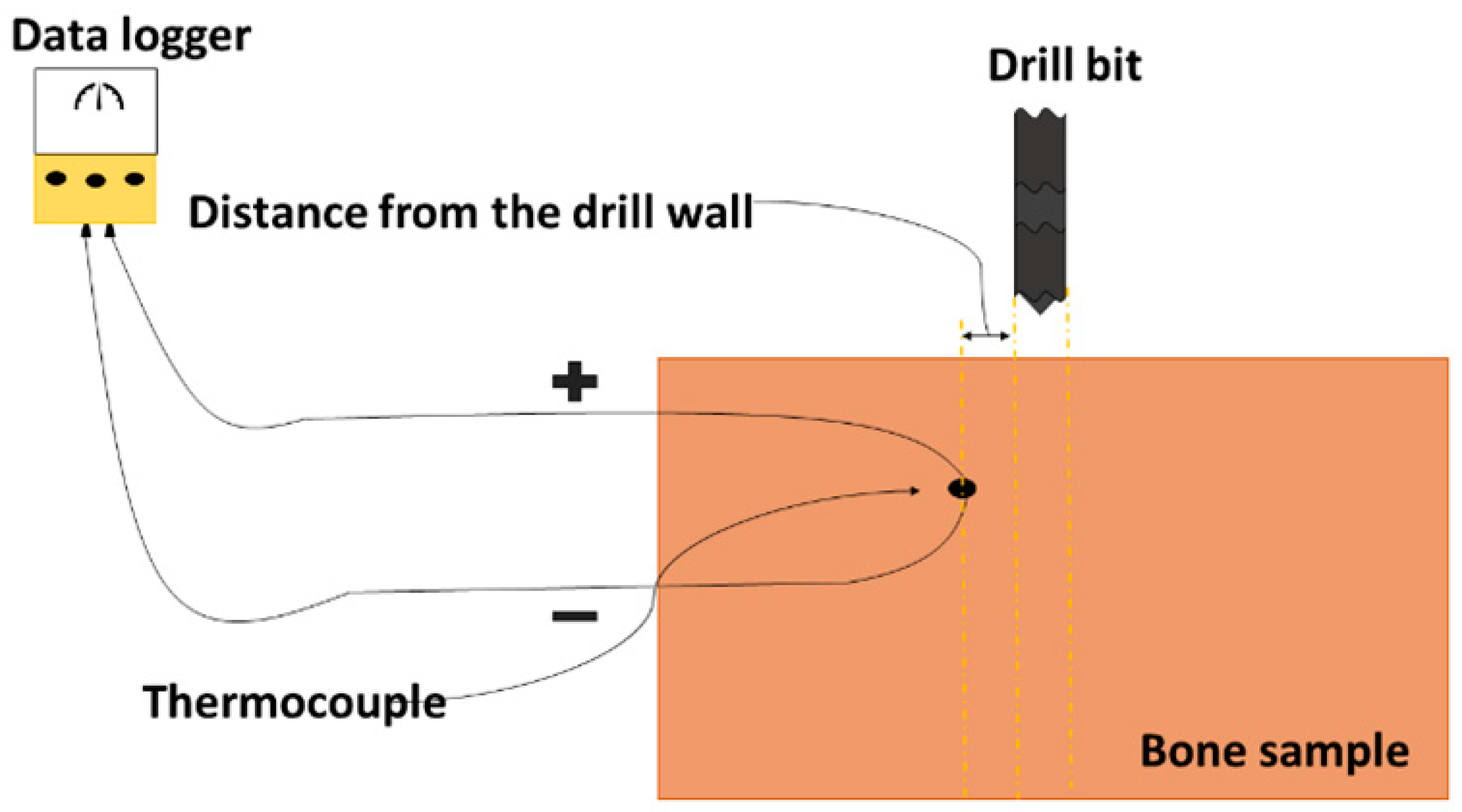
9. Temperature Measuring Method
10. Challenges in Bone Drilling
11. Summary: Future Directions/Guidelines
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hou, J.; Tamura, Y.; Lu, H.-Y.; Takahashi, Y.; Kasugai, S.; Nakata, H.; Kuroda, S. An In Vitro Evaluation of Selenium Nanoparticles on Osteoblastic Differentiation and Antimicrobial Properties against Porphyromonas Gingivalis. Nanomater 2022, 12, 1850. [Google Scholar] [CrossRef] [PubMed]
- Nicky, B.; Walsh, W.R. Drilling of bone: Practicality, limitations and complications associated with surgical drill-bits. Biomech. Appl. 2011, 4, 53–83. [Google Scholar]
- Akhbar, M.F.A.; Yusoff, A.R. Fast & Injurious: Reducing Thermal Osteonecrosis Regions in the Drilling of Human Bone with Multi-Objective Optimization. Meas. J. Int. Meas. Confed. 2020, 152, 107385. [Google Scholar]
- Islam, M.A.; Kamarrudin, N.S.; Suhaimi, M.F.F.; Daud, R.; Ibrahim, I.; Mat, F. Parametric Investigation on Different Bone Densities to Avoid Thermal Necrosis during Bone Drilling Process. J. Phys. Conf. Ser. 2021, 2051, 012033. [Google Scholar] [CrossRef]
- Crowninshield, R.D.; Pope, M.H. The Response of Compact Bone in Tension at Various Strain Rates. Ann. Biomed. Eng. 1974, 2, 217–225. [Google Scholar] [CrossRef]
- Hillery, M.T.; Shuaib, I. Temperature Effects in the Drilling of Human and Bovine Bone. J. Mater. Process. Technol. 1999, 92–93, 302–308. [Google Scholar] [CrossRef]
- Akhbar, M.F.A.; Yusoff, A.R. Comparison of Bone Temperature Elevation in Drilling of Human, Bovine and Porcine Bone. Procedia CIRP 2019, 82, 411–414. [Google Scholar] [CrossRef]
- Soriano, J.; Garay, A.; Aristimuño, P.; Arrazola, P.J. Study and improvement of surgical drill bit geometry for implant site preparation. Int. J. Adv. Manuf. Technol. 2014, 74, 615–627. [Google Scholar] [CrossRef]
- Chen, J.; Yuan, D.; Jiang, H.; Zhang, L.; Yang, Y.; Fu, Y.; Qian, N.; Jiang, F. Thermal Management of Bone Drilling Based on Rotating Heat Pipe. Energies 2022, 15, 35. [Google Scholar] [CrossRef]
- Can, M.; Koluaçik, S.; Bahçe, E.; Gokce, H.; Tecellioglu, F.S. Investigation of Thermal Damage in Bone Drilling: Hybrid Processing Method and Pathological Evaluation of Existing Methods. J. Mech. Behav. Biomed. Mater. 2021, 126, 105030. [Google Scholar] [CrossRef]
- Agarwal, R.; Gupta, V.; Singh, J. Additive Manufacturing-Based Design Approaches and Challenges for Orthopaedic Bone Screws: A State-of-the-Art Review. J. Braz. Soc. Mech. Sci. Eng. 2022, 44, 37. [Google Scholar] [CrossRef]
- Florencio-Silva, R.; Sasso, G.R.D.S.; Sasso-Cerri, E.; Simões, M.J.; Cerri, P.S. Biology of Bone Tissue: Structure, Function, and Factors That Influence Bone Cells. BioMed Res. Int. 2015, 2015, 421746. [Google Scholar] [CrossRef] [PubMed]
- Falk, D.; Aiello, L.; Dean, C. An Introduction to Human Evolutionary Anatomy. Man 1992, 27, 410. [Google Scholar] [CrossRef]
- Baker, G.F.; Tortora, G.J.; Nostakos, N.P.A. Principles of Anatomy and Physiology. Am. J. Nurs. 1976, 76, 477. [Google Scholar] [CrossRef]
- Currey, J.D. Effects of Differences in Mineralization on the Mechanical Properties of Bone. Philos. Trans. R. Soc. Lond. B. Biol. Sci. 1984, 304, 509–518. [Google Scholar] [PubMed]
- Lee, J.; Chavez, C.L.; Park, J. Parameters affecting mechanical and thermal responses in bone drilling: A review. J. Biomech. 2018, 71, 4–21. [Google Scholar] [CrossRef] [PubMed]
- 3 Bone Structure–Anatomy & Physiology. Available online: https://open.oregonstate.education/aandp/chapter/6-3-bone-structure (accessed on 30 June 2022).
- Ashwell, K.W.S. Concise Body Atlas: The Compact Guide to the Human Body; Quad Quarto Publishing Group: London, UK, 2017. [Google Scholar]
- Morgan, E.F.; Unnikrisnan, G.U.; Hussein, A.I. Bone Mechanical Properties in Healthy and Diseased States. Annu. Rev. Biomed. Eng. 2018, 20, 119–143. [Google Scholar] [CrossRef]
- Hikmawati, D.; Widiyanti, P.; Amrillah, T.; Astri Nia, W.; Firdania, I.T.; Abdullah, C.A.C. Study of Mechanical and Thermal Properties in Nano-Hydroxyapatite/Chitosan/Carboxymethyl Cellulose Nanocomposite-Based Scaffold for Bone Tissue Engineering: The Roles of Carboxymethyl Cellulose. Appl. Sci. 2020, 10, 6970. [Google Scholar]
- Abayazid, M.; Wicaksono, D.H.B.; Dankelman, J.; French, P.J. Modeling Heat Generation and Temperature Distribution for Temperature Sensing during Dental Surgical Drilling. In Proceedings of the SAFE 2009, Workshop on Microsystems, Materials, Technology and RF-devices and Sensors, Veldhoven, The Netherlands, 26–27 November 2009. [Google Scholar]
- Coulson-Thomas, Y.M.; Coulson-Thomas, V.J.; Norton, A.L.; Gesteira, T.F.; Cavalheiro, R.P.; Meneghetti, M.C.Z.; Martins, J.R.; Dixon, R.A.; Nader, H.B. The Identification of Proteoglycans and Glycosaminoglycans in Archaeological Human Bones and Teeth. PLoS ONE 2015, 10, e0131105. [Google Scholar] [CrossRef]
- Lin, X.; Patil, S.; Gao, Y.G.; Qian, A. The Bone Extracellular Matrix in Bone Formation and Regeneration. Front. Pharmacol. 2020, 11, 757. [Google Scholar] [CrossRef]
- Ashry, A.; Elattar, M.S.; Elsamni, O.A.; Soliman, I.S. Effect of Guiding Sleeve Design on Intraosseous Heat Generation During Implant Site Preparation (In Vitro Study). J. Prosthodont. 2022, 31, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Cui, Q.; Wang, R.; Faller, L.M.; Kan, T.; Jiang, X.; Zhu, F.; Zhu, W.; Liu, Y. Temperature Field in Bone During Robotic Dental Implant Drilling: Theoretical Models and In Vitro Experiments. J. Med. Biol. Eng. 2022, 42, 253–262. [Google Scholar] [CrossRef]
- Islam, M.A.; Kamarrudin, N.S.; Daud, R.; Ibrahim, I.; Rahman, A.; Mat, F. Temperature Measurement Methods in an Experimental Setup during Bone Drilling: A Brief Review on the Comparison of Thermocouple and Infrared Thermography. J. Phys. Conf. Ser. 2021, 2129, 12096. [Google Scholar] [CrossRef]
- Karmani, S. The Thermal Properties of Bone and the Effects of Surgical Intervention. Curr. Orthop. 2006, 20, 52–58. [Google Scholar] [CrossRef]
- Giasin, K.; Ayvar-Soberanis, S. Evaluation of Workpiece Temperature during Drilling of GLARE Fiber Metal Laminates Using Infrared Techniques: Effect of Cutting Parameters, Fiber Orientation and Spray Mist Application. Materials 2016, 9, 622. [Google Scholar] [CrossRef]
- Singh, R.P.; Pandey, P.M.; Mir, M.A.; Mridha, A.R. Thermal Changes during Drilling in Human Femur by Rotary Ultrasonic Bone Drilling Machine: A Histologic and Ultrastructural Study. J. Biomed. Mater. Res. Part B Appl. Biomater. 2021, 110, 1023–1033. [Google Scholar] [CrossRef]
- Amewoui, F.; Le Coz, G.; Bonnet, A.S.; Moufki, A. Bone Drilling: An Identification of Heat Sources. Comput. Methods Biomech. Biomed. Eng. 2020, 23, S10–S11. [Google Scholar] [CrossRef]
- Lee, J.E.; Huh, S.J.; Lee, H.J. Experimental Determination of Thermal Conductivity of Cortical Bone by Compensating Heat Loss in Parallel Plate Method. Int. J. Precis. Eng. Manuf. 2018, 19, 569–576. [Google Scholar] [CrossRef]
- Irandoust, S.; Müftü, S. The Interplay between Bone Healing and Remodeling around Dental Implants. Sci. Rep. 2020, 10, 4335. [Google Scholar] [CrossRef] [Green Version]
- Feldmann, A.; Wili, P.; Maquer, G.; Zysset, P. The thermal conductivity of cortical and cancellous bone. Eur. Cell. Mater. 2018, 35, 25–33. [Google Scholar] [CrossRef]
- De Tommasi, F.; Massaroni, C.; Grasso, R.F.; Carassiti, M.; Schena, E. Temperature Monitoring in Hyperthermia Treatments of Bone Tumors: State-of-the-Art and Future Challenges. Sensors 2021, 21, 5470. [Google Scholar] [CrossRef] [PubMed]
- Babbar, A.; Jain, V.; Gupta, D.; Agrawal, D. Finite Element Simulation and Integration of CEM43 °C and Arrhenius Models for Ultrasonic-Assisted Skull Bone Grinding: A Thermal Dose Model. Med. Eng. Phys. 2021, 90, 9–22. [Google Scholar] [CrossRef] [PubMed]
- Bai, W.; Pan, P.; Shu, L.; Yang, Y.; Zhang, J.; Xu, J.; Sugita, N. Design of a Self-Centring Drill Bit for Orthopaedic Surgery: A Systematic Comparison of the Drilling Performance. J. Mech. Behav. Biomed. Mater. 2021, 123, 104727. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-C.; Hsiao, C.-K.; Ciou, J.-S.; Tsai, Y.-J.; Tu, Y.-K. Effects of implant drilling parameters for pilot and twist drills on temperature rise in bone analog and alveolar bones. Med. Eng. Phys. 2016, 38, 1314–1321. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Robles-Linares, J.A.; Chen, L.; Liao, Z.; Shih, A.J.; Wang, C. Advances in Machining of Hard Tissues–From Material Removal Mechanisms to Tooling Solutions. Int. J. Mach. Tools Manuf. 2021, 172, 103838. [Google Scholar] [CrossRef]
- Guimarães, B.M.P.; Fernandes, C.M.D.S.; de Figueiredo, D.A.; da Silva, F.S.C.P.; Miranda, M.G.M. Cutting temperature measurement and prediction in machining processes: Comprehensive review and future perspectives. Int. J. Adv. Manuf. Technol. 2022, 120, 2849–2878. [Google Scholar] [CrossRef]
- Ali Akhbar, M.F.; Yusoff, A.R. Drilling of Bone: Effect of Drill Bit Geometries on Thermal Osteonecrosis Risk Regions. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2019, 233, 207–218. [Google Scholar] [CrossRef]
- Mohd, A.N.B.; Husain, M.K.B.A.; Sarip, S.B.; Ismail, R.B. Temperature Performance of Stainless Steel AISI420B Orthopedic Drill Bits Simulation Study. J. Adv. Res. Appl. Sci. Eng. Technol. 2022, 26, 78–96. [Google Scholar]
- Li, S.; Shu, L.; Kizaki, T.; Bai, W.; Terashima, M.; Sugita, N. Cortical Bone Drilling: A Time Series Experimental Analysis of Thermal Characteristics. J. Manuf. Process. 2021, 64, 606–619. [Google Scholar] [CrossRef]
- Akhbar, M.F.A.; Sulong, A.W. Surgical Drill Bit Design and Thermomechanical Damage in Bone Drilling: A Review. Ann. Biomed. Eng. 2021, 49, 29–56. [Google Scholar] [CrossRef]
- Motoyoshi, M.; Hirabayashi, M.; Uemura, M.; Shimizu, N. Recommended Placement Torque When Tightening an Orthodontic Mini-Implant. Clin. Oral Implants Res. 2006, 17, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Pandey, R.K.; Panda, S.S. Drilling of Bone: A Comprehensive Review. J. Clin. Orthop. Trauma 2013, 4, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jamil, M.; Rafique, S.; Khan, A.M.; Hegab, H.; Mia, M.; Gupta, M.K.; Song, Q. Comprehensive analysis on orthopedic drilling: A state-of-the-art review. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2020, 234, 537–561. [Google Scholar] [CrossRef]
- Nishanth, B.S.; Kulkarni, V.N.; Gaitonde, V.N. A Review on Conventional and Non-Conventional Machining of Titanium and Nickel Based Alloys. AIP Conf. Proc. 2019, 2200, 020091. [Google Scholar]
- Bohra, A.; Chandrasekaran, M.; Teyi, N. Bone Drilling Investigation and Possible Research: A State of the Art Review. AIP Conf. Proc. 2019, 2128, 050022. [Google Scholar]
- Dixit, U.S.; Pandey, P.M.; Verma, G.C. Ultrasonic-Assisted Machining Processes: A Review. Int. J. Mechatron. Manuf. Syst. 2019, 12, 227–254. [Google Scholar] [CrossRef]
- Davis, R.; Singh, A.; Jackson, M.J.; Coelho, R.T.; Prakash, D.; Charalambous, C.P.; Ahmed, W.; da Silva, L.R.R.; Lawrence, A.A. A Comprehensive Review on Metallic Implant Biomaterials and Their Subtractive Manufacturing. Int. J. Adv. Manuf. Technol. 2022, 120, 1473–1530. [Google Scholar] [CrossRef]
- Xue, Y.; Lofland, S.; Hu, X. Thermal Conductivity of Protein-Based Materials: A Review. Polymers 2019, 11, 456. [Google Scholar] [CrossRef] [Green Version]
- Samarasinghe, C.; Uddin, M.; Bari, S.; Xian, C. Temperature and Force Generation in Surgical Bone Drilling. AIP Conf. Proc. 2021, 2324, 060007. [Google Scholar]
- Soriano, J.; Garay, A.; Ishii, K.; Sugita, N.; Arrazola, P.J.; Mitsuishi, M. A New Surgical Drill Bit Concept for Bone Drilling Operations. Mater. Manuf. Process. 2013, 28, 1065–1070. [Google Scholar] [CrossRef]
- Sui, J.; Wang, C.; Sugita, N. Experimental Study of Temperature Rise during Bone Drilling Process. Med. Eng. Phys. 2020, 78, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Davidson, S.R.H.; James, D.F. Drilling in Bone: Modeling Heat Generation and Temperature Distribution. J. Biomech. Eng. 2003, 125, 305–314. [Google Scholar] [CrossRef]
- Lee, J.E.; Rabin, Y.; Ozdoganlar, O.B. A New Thermal Model for Bone Drilling with Applications to Orthopaedic Surgery. Med. Eng. Phys. 2011, 33, 1234–1244. [Google Scholar] [CrossRef] [PubMed]
- Sui, J.; Sugita, N.; Mitsuishi, M. Thermal Modeling of Temperature Rise for Bone Drilling with Experimental Validation. J. Manuf. Sci. Eng. Trans. ASME 2015, 137, 061008. [Google Scholar] [CrossRef]
- Zelenov, E.S. Experimental Investigation of the Thermophysical Properties of Compact Bone. Mech. Compos. Mater. 1986, 21, 759–762. [Google Scholar] [CrossRef]
- Hochscheidt, C.J.; Shimizu, R.H.; Andrighetto, A.R.; Moura, L.M.; Golin, A.L.; Hochscheidt, R.C. Thermal Variation during Osteotomy with Different Dental Implant Drills: A Standardized Study in Bovine Ribs. Implant Dent. 2017, 26, 73–79. [Google Scholar] [CrossRef]
- Mishra, S.K.; Chowdhary, R. Heat Generated by Dental Implant Drills During Osteotomy—A Review: Heat Generated by Dental Implant Drills. J. Indian Prosthodont. Soc. 2014, 14, 131. [Google Scholar] [CrossRef] [PubMed]
- Tuijthof, G.J.M.; Frühwirt, C.; Kment, C. Influence of Tool Geometry on Drilling Performance of Cortical and Trabecular Bone. Med. Eng. Phys. 2013, 35, 1165–1172. [Google Scholar] [CrossRef]
- Citation Mediouni, M.; Kucklick, T.; Poncet, S.; Madiouni, R.; Abouaomar, A.; Madry, H.; Cucchiarini, M.; Chopko, B.; Vaughan, N.; Arora, M.; et al. An Overview of Thermal Necrosis: Present and Future. Curr. Med. Res. Opin. 2019, 35, 1555–1562. [Google Scholar] [CrossRef]
- Salomó-Coll, O.; Auriol-Muerza, B.; Lozano-Carrascal, N.; Hernández-Alfaro, F.; Wang, H.L.; Gargallo-Albiol, J. Influence of Bone Density, Drill Diameter, Drilling Speed, and Irrigation on Temperature Changes during Implant Osteotomies: An in Vitro Study. Clin. Oral Investig. 2021, 25, 1047–1053. [Google Scholar] [CrossRef]
- Zhang, Y.; Xu, L.; Wang, C.; Chen, Z.; Han, S.; Chen, B.; Chen, J. Mechanical and Thermal Damage in Cortical Bone Drilling in Vivo. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2019, 233, 621–635. [Google Scholar] [CrossRef] [PubMed]
- Walsh, W.R.; Pelletier, M.H.; Bertollo, N.; Lovric, V.; Wang, T.; Morberg, P.; Parr, W.C.H.; Bergadano, D. Bone Ongrowth and Mechanical Fixation of Implants in Cortical and Cancellous Bone. J. Orthop. Surg. Res. 2020, 15, 177. [Google Scholar] [CrossRef]
- Singh, G.; Babbar, A.; Jain, V.; Gupta, D. Comparative statement for diametric delamination in drilling of cortical bone with conventional and ultrasonic assisted drilling techniques. J. Orthop. 2021, 25, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Amewoui, F.; Le Coz, G.; Bonnet, A.S.; Moufki, A. Bone drilling: A thermal model for bone temperature prediction. Comput. Methods Biomech. Biomed. Eng. 2019, 22, S305–S307. [Google Scholar] [CrossRef]
- Babbar, A.; Jain, V.; Gupta, D. In Vivo Evaluation of Machining Forces, Torque, and Bone Quality during Skull Bone Grinding. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2020, 234, 626–638. [Google Scholar] [CrossRef]
- Jain, P.; Khan, M.R. Selection of Suitable Pedicle Screw for Degenerated Cortical and Cancellous Bone of Human Lumbar Spine: A Finite Element Study. Int. J. Artif. Organs 2021, 44, 361–366. [Google Scholar] [CrossRef]
- Lundskog, J. Heat and bone tissue. An experimental investigation of the thermal properties of bone and threshold levels for thermal injury. Scand. J. Plast. Reconstr. Surg. 1972, 9, 1–80. [Google Scholar]
- Feldmann, A.; Wandel, J.; Zysset, P. Reducing temperature elevation of robotic bone drilling. Med. Eng. Phys. 2016, 38, 1495–1504. [Google Scholar] [CrossRef]
- Akhbar, M.F.A.; Yusoff, A.R. Drilling of Bone: Thermal Osteonecrosis Regions Induced by Drilling Parameters. Biomed. Phys. Eng. Express 2019, 5, 6. [Google Scholar] [CrossRef]
- Feldmann, A.; Gavaghan, K.; Stebinger, M.; Williamson, T.; Weber, S.; Zysset, P. Real-Time Prediction of Temperature Elevation During Robotic Bone Drilling Using the Torque Signal. Ann. Biomed. Eng. 2017, 45, 2088–2097. [Google Scholar] [CrossRef]
- Shakouri, E.; Hassanalideh, H.H.; Gholampour, S. Experimental investigation of temperature rise in bone drilling with cooling: A comparison between modes of without cooling, internal gas cooling, and external liquid cooling. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2017, 232, 45–53. [Google Scholar] [CrossRef] [Green Version]
- Kuppuswamy, R.; Christie-Taylor, B. Influence of Surgical Drill Geometry on Drilling Performance of Cortical and Trabecular Bone. In Advances in Forming, Machining and Automation; Springer: Berlin/Heidelberg, Germany, 2019; pp. 119–131. [Google Scholar]
- Sui, J.; Sugita, N. Experimental Study of Thrust Force and Torque for Drilling Cortical Bone. Ann. Biomed. Eng. 2019, 47, 802–812. [Google Scholar] [CrossRef] [PubMed]
- Akhbar, M.F.A.; Yusoff, A.R. Multi-Objective Optimization of Surgical Drill Bit to Minimize Thermal Damage in Bone-Drilling. Appl. Therm. Eng. 2019, 157, 113594. [Google Scholar] [CrossRef]
- Jeong, M.J.; Lee, S.W.; Jang, W.K.; Kim, H.J.; Seo, Y.H.; Kim, B.H. Prediction of Drill Bit Breakage Using an Infrared Sensor. Sensors 2021, 21, 2808. [Google Scholar] [CrossRef] [PubMed]
- Noorazizi, M.; Izamshah, R.; Kasim, M. Effects of Drill Geometry and Penetration Angle on Temperature and Holes Surfaces for Cortical Bovine Bone: An in Vitro Study. Procedia Eng. 2017, 184, 70–77. [Google Scholar] [CrossRef]
- Shu, L.; Li, S.; Terashima, M.; Bai, W.; Hanami, T.; Hasegawa, R.; Sugita, N. A novel self-centring drill bit design for low-trauma bone drilling. Int. J. Mach. Tools Manuf. 2020, 154, 103568. [Google Scholar] [CrossRef]
- Chen, Y.C.; Tu, Y.K.; Zhuang, J.Y.; Tsai, Y.J.; Yen, C.Y.; Hsiao, C.K. Evaluation of the Parameters Affecting Bone Temperature during Drilling Using a Three-Dimensional Dynamic Elastoplastic Finite Element Model. Med. Biol. Eng. Comput. 2017, 55, 1949–1957. [Google Scholar] [CrossRef]
- Dahibhate, R.V.; Jaju, S.B. Bone Drilling Parameters and Necrosis: An In Vitro Study. In Smart Technologies for Energy, Environment and Sustainable Development; Springer: Singapore, 2019; pp. 599–606. [Google Scholar]
- Delaisse, J.M.; Søe, K.; Andersen, T.L.; Rojek, A.M.; Marcussen, N. The Mechanism Switching the Osteoclast From Short to Long Duration Bone Resorption. Front. Cell Dev. Biol. 2021, 9, 644503. [Google Scholar] [CrossRef]
- Aghvami, M.; Brunski, J.B.; Tulu, U.S.; Chen, C.-H.; Helms, J.A. A Thermal and Biological Analysis of Bone Drilling. J. Biomech. Eng. 2018, 140, 101010. [Google Scholar] [CrossRef]
- Sarparast, M.; Ghoreishi, M.; Jahangirpoor, T.; Tahmasbi, V. Experimental and finite element investigation of high-speed bone drilling: Evaluation of force and temperature. J. Braz. Soc. Mech. Sci. Eng. 2020, 42, 349. [Google Scholar] [CrossRef]
- Fernandes, M.G.; Fonseca, E.M.; Jorge, R.N. Thermo-mechanical stresses distribution on bone drilling: Numerical and experimental procedures. Proc. Inst. Mech. Eng. Part L J. Mater. Des. Appl. 2017, 233, 637–646. [Google Scholar] [CrossRef] [Green Version]
- Shin, H.C.; Yoon, Y.S. Bone Temperature Estimation during Orthopaedic Round Bur Milling Operations. J. Biomech. 2006, 39, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Ein-Afshar, M.J.; Shahrezaee, M.; Shahrezaee, M.H.; Sharifzadeh, S.R. Biomechanical Evaluation of Temperature Rising and Applied Force in Controlled Cortical Bone Drilling: An Animal in Vitro Study. Arch. Bone Jt. Surg. 2020, 8, 605–612. [Google Scholar] [PubMed]
- Wang, H.; Gao, X.; Wang, B.; Wang, M.; Liu, Y.; Zan, T.; Gao, P.; Liu, C. Evaluation of temperature distribution for bone drilling considering aging factor. Med. Nov. Technol. Devices 2022, 16, 100174. [Google Scholar] [CrossRef]
- Tahmasbi, V.; Ghoreishi, M.; Zolfaghari, M. Sensitivity Analysis of Temperature and Force in Robotic Bone Drilling Process Using Sobol Statistical Method. Biotechnol. Biotechnol. Equip. 2018, 32, 130–141. [Google Scholar] [CrossRef] [Green Version]
- Qasemi, M.; Tahmasbi, V.; Sheikhi, M.M.; Zolfaghari, M. An effect of osteon orientation in end milling operation of cortical bone based on FEM and experiment. J. Manuf. Process. 2022, 81, 141–154. [Google Scholar] [CrossRef]
- Tahmasbi, V.; Ghoreishi, M.; Zolfaghari, M. Investigation, Sensitivity Analysis, and Multi-Objective Optimization of Effective Parameters on Temperature and Force in Robotic Drilling Cortical Bone. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2017, 231, 1012–1024. [Google Scholar] [CrossRef]
- Saltelli, A.; Tarantola, S.; Chan, K.P.S. A Quantitative Model-Independent Method for Global Sensitivity Analysis of Model Output. Technometrics 1999, 41, 39–56. [Google Scholar] [CrossRef]
- Karalis, T.; Galanos, P. Research on the Mechanical Impedance of Human Bone by a Drilling Test. J. Biomech. 1982, 15, 561–581. [Google Scholar] [CrossRef]
- Natali, C.; Ingle, P.; Dowell, J. Orthopaedic Bone Drills-Can They Be Improved? Temperature Changes near the Drilling Face. J. Bone Jt. Surg. Ser. B 1996, 78, 357–362. [Google Scholar] [CrossRef]
- Eriksson, A.R.; Albrektsson, T.; Albrektsson, B. Heat Caused by Drilling Cortical Bone: Temperature Measured in Vivo in Patients and Animals. Acta Orthop. 1984, 55, 629–631. [Google Scholar] [CrossRef] [PubMed]
- Gholampour, S.; Deh, H.H.H. The Effect of Spatial Distances between Holes and Time Delays between Bone Drillings Based on Examination of Heat Accumulation and Risk of Bone Thermal Necrosis. Biomed. Eng. Online 2019, 18, 65. [Google Scholar] [CrossRef] [Green Version]
- Hassanalideh, H.H.; Gholampour, S. Finding the Optimal Drill Bit Material and Proper Drilling Condition for Utilization in the Programming of Robot-Assisted Drilling of Bone. CIRP J. Manuf. Sci. Technol. 2020, 31, 34–47. [Google Scholar] [CrossRef]
- Lempel, E.; Szalma, J. Effect of Spray Air Settings of Speed-Increasing Contra-Angle Handpieces on Intrapulpal Temperatures, Drilling Times, and Coolant Spray Pattern. Clin. Oral Investig. 2022, 26, 523–533. [Google Scholar] [CrossRef]
- Effatparvar, M.R.; Jamshidi, N.; Mosavar, A. Appraising Efficiency of OpSite as Coolant in Drilling of Bone. J. Orthop. Surg. Res. 2020, 15, 197. [Google Scholar] [CrossRef] [PubMed]
- Song, S.; Cheng, X.; Li, T.; Shi, M.; Zheng, G.; Liu, H. Experimental study of bone drilling by Kirschner wire. Med. Eng. Phys. 2022, 106, 103835. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, M.G.; Fonseca, E.M.; Jorge, R.N.; Manzanares, M.C.; Dias, M.I. Effect of drill speed on the strain distribution during drilling of bovine and human bones. J. Mech. Eng. Biomech. 2018, 2, 69–74. [Google Scholar] [CrossRef] [Green Version]
- Möhlhenrich, S.C.; Heussen, N.; Modabber, A.; Bock, A.; Hölzle, F.; Wilmes, B.; Danesh, G.; Szalma, J. Influence of Bone Density, Screw Size and Surgical Procedure on Orthodontic Mini-Implant Placement–Part B: Implant Stability. Int. J. Oral Maxillofac. Surg. 2021, 50, 565–572. [Google Scholar] [CrossRef]
- Timon, C.; Keady, C. Thermal Osteonecrosis Caused by Bone Drilling in Orthopedic Surgery: A Literature Review. Cureus 2019, 11, e5226. [Google Scholar] [CrossRef] [Green Version]
- Ghazali, M.; Roseiro, L.; Garruço, A.; Margalho, L.; Expedito, F. Pre-Drilling vs. Self-Drilling of Pin Bone Insertion—A Thermography Experimental Evaluation. Lect. Notes Comput. Vis. Biomech. 2018, 27, 1063–1068. [Google Scholar]
- Hein, C.; Inceoglu, S.; Juma, D.; Zuckerman, L. Heat Generation during Bone Drilling: A Comparison between Industrial and Orthopaedic Drill Bits. J. Orthop. Trauma 2017, 31, e55–e59. [Google Scholar] [CrossRef] [PubMed]
- Augustin, G.; Zigman, T.; Davila, S.; Udilljak, T.; Staroveski, T.; Brezak, D.; Babic, S. Cortical Bone Drilling and Thermal Osteonecrosis. Clin. Biomech. 2012, 27, 313–325. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R.; Singh, J.; Gupta, V. Prediction of temperature elevation in rotary ultrasonic bone drilling using machine learning models: An in-vitro experimental study. Med. Eng. Phys. 2022, 6, 103869. [Google Scholar] [CrossRef] [PubMed]
- Ashrith, H.S.; Doddamani, M. Point angle effect in drilling of syntactic foams. Compos. Part C Open Access 2021, 6, 100179. [Google Scholar] [CrossRef]
- Mali, V.; Warhatkar, H.; Pawade, R. Experimental Investigations into Assessment of Thrust Force and Temperature in Bone Drilling. Res. Sq. 2022, 1–18. [Google Scholar] [CrossRef]
- Liu, S.; Wu, D.; Zhao, J.; Yang, T.; Sun, J.; Gong, K. Novel crescent drill design and mechanistic force modeling for thrust force reduction in bone drilling. Med. Eng. Phys. 2022, 103, 103795. [Google Scholar] [CrossRef]
- Chen, Y.C.; Tu, Y.K.; Tsai, Y.J.; Tsai, Y.S.; Yen, C.Y.; Yang, S.C.; Hsiao, C.K. Assessment of Thermal Necrosis Risk Regions for Different Bone Qualities as a Function of Drilling Parameters. Comput. Methods Programs Biomed. 2018, 162, 253–261. [Google Scholar] [CrossRef]
- Hart, N.H.; Nimphius, S.; Rantalainen, T.; Ireland, A.; Siafarikas, A.; Newton, R.U. Mechanical Basis of Bone Strength: Influence of Bone Material, Bone Structure and Muscle Action. J. Musculoskelet. Neuronal Interact. 2017, 17, 114. [Google Scholar]
- Guglielmi, G.; Muscarella, S.; Bazzocchi, A. Integrated Imaging Approach to Osteoporosis: State-of-the-Art Review and Update. Radiographics 2011, 31, 1343–1364. [Google Scholar] [CrossRef]
- Safari, M.; Tahmasbi, V.; Hassanpour, P.; Zolfaghari, M. Experimental investigation, sensitivity analysis and optimization on the effect of drill bit’s point angle and helix angle on cortical bone drilling process temperature. J. Mech. Eng. 2022, 52, 11–19. [Google Scholar]
- Liu, C.; Wang, Z.; Gao, L.; Zhang, X.; Wang, G.; Yang, T.; Du, Y. A Novel Tool Wear Modeling Method in Drilling of Particle Reinforced Metal Matrix Composite. Int. J. Adv. Manuf. Technol. 2022, 119, 7089–7107. [Google Scholar] [CrossRef]
- Han, Y.; Lv, Q.; Song, Y.; Zhang, Q. Influence of parameters on temperature rise and chips morphology in low-frequency vibration-assisted bone drilling. Med. Eng. Phys. 2022, 103, 103791. [Google Scholar] [CrossRef]
- Mondal, N.; Mandal, S.; Mandal, M.C.; Das, S.; Haldar, B. ANN-FPA Based Modelling and Optimization of Drilling Burrs Using RSM and GA. In Global Congress on Manufacturing and Management; Springer International Publishing: Cham, Switzerland, 2022; pp. 180–195. [Google Scholar]
- Piska, M.; Yang, L.; Reed, M.; Saleh, M. Drilling Efficiency and Temperature Elevation of Three Types of Kirschner-Wire Point. J. Bone Jt. Surg. Ser. B 2002, 84, 137–140. [Google Scholar] [CrossRef]
- Agarwal, R.; Singh, R.P.; Gupta, V.; Singh, J. Influence of cutting force on temperature, microcracks and chip morphology during rotary ultrasonic bone drilling: An in-vitro study. J. Braz. Soc. Mech. Sci. Eng. 2022, 44, 301. [Google Scholar] [CrossRef]
- Zdero, R.; MacAvelia, T.; Janabi-Sharifi, F. Force and torque measurements of surgical drilling into whole bone. In Experimental Methods in Orthopaedic Biomechanics; Academic Press: Cambridge, MA, USA, 2017; pp. 85–100. [Google Scholar]

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Properties | Human Bone | Bovine Bone | Drill Bit |
|---|---|---|---|
| Density (kg m−3) | 2.10 × 103 | 2.10 × 103 | 7.99 × 103 |
| Young’s modulus (Pa) | 1.70 × 1010 | 2.20 × 1010 | 1.93 × 1011 |
| Shear modulus (Pa) | 3.00 × 106 | 3.00 × 106 | 9.70 × 108 |
| Tensile strength (Pa) | 2.00 × 108 | 2.50 × 108 | 5.79 × 108 |
| Yielding strength (Pa) | 1.10 × 108 | - | 6.08 × 108 |
| Poisson’s ratio | 0.40 | 0.33 | 0.30 |
| Specific heat (J kg−1 K−1) | 1.26 × 103 | 1.30 × 103 | 5.00 × 102 |
| Thermal conductivity (W m−1 K−1) | 3.80 × 10−1 | 3.00 × 10−1 | 1.70 × 10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Islam, M.A.; Kamarrudin, N.S.; Daud, R.; Mohd Noor, S.N.F.; Azmi, A.I.; Razlan, Z.M. A Review of Surgical Bone Drilling and Drill Bit Heat Generation for Implantation. Metals 2022, 12, 1900. https://doi.org/10.3390/met12111900
Islam MA, Kamarrudin NS, Daud R, Mohd Noor SNF, Azmi AI, Razlan ZM. A Review of Surgical Bone Drilling and Drill Bit Heat Generation for Implantation. Metals. 2022; 12(11):1900. https://doi.org/10.3390/met12111900
Chicago/Turabian StyleIslam, Md Ashequl, Nur Saifullah Kamarrudin, Ruslizam Daud, Siti Noor Fazliah Mohd Noor, Azwan Iskandar Azmi, and Zuradzman Mohamad Razlan. 2022. "A Review of Surgical Bone Drilling and Drill Bit Heat Generation for Implantation" Metals 12, no. 11: 1900. https://doi.org/10.3390/met12111900
APA StyleIslam, M. A., Kamarrudin, N. S., Daud, R., Mohd Noor, S. N. F., Azmi, A. I., & Razlan, Z. M. (2022). A Review of Surgical Bone Drilling and Drill Bit Heat Generation for Implantation. Metals, 12(11), 1900. https://doi.org/10.3390/met12111900