Reconstruction of Complex Zygomatic Bone Defects Using Mirroring Coupled with EBM Fabrication of Titanium Implant

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
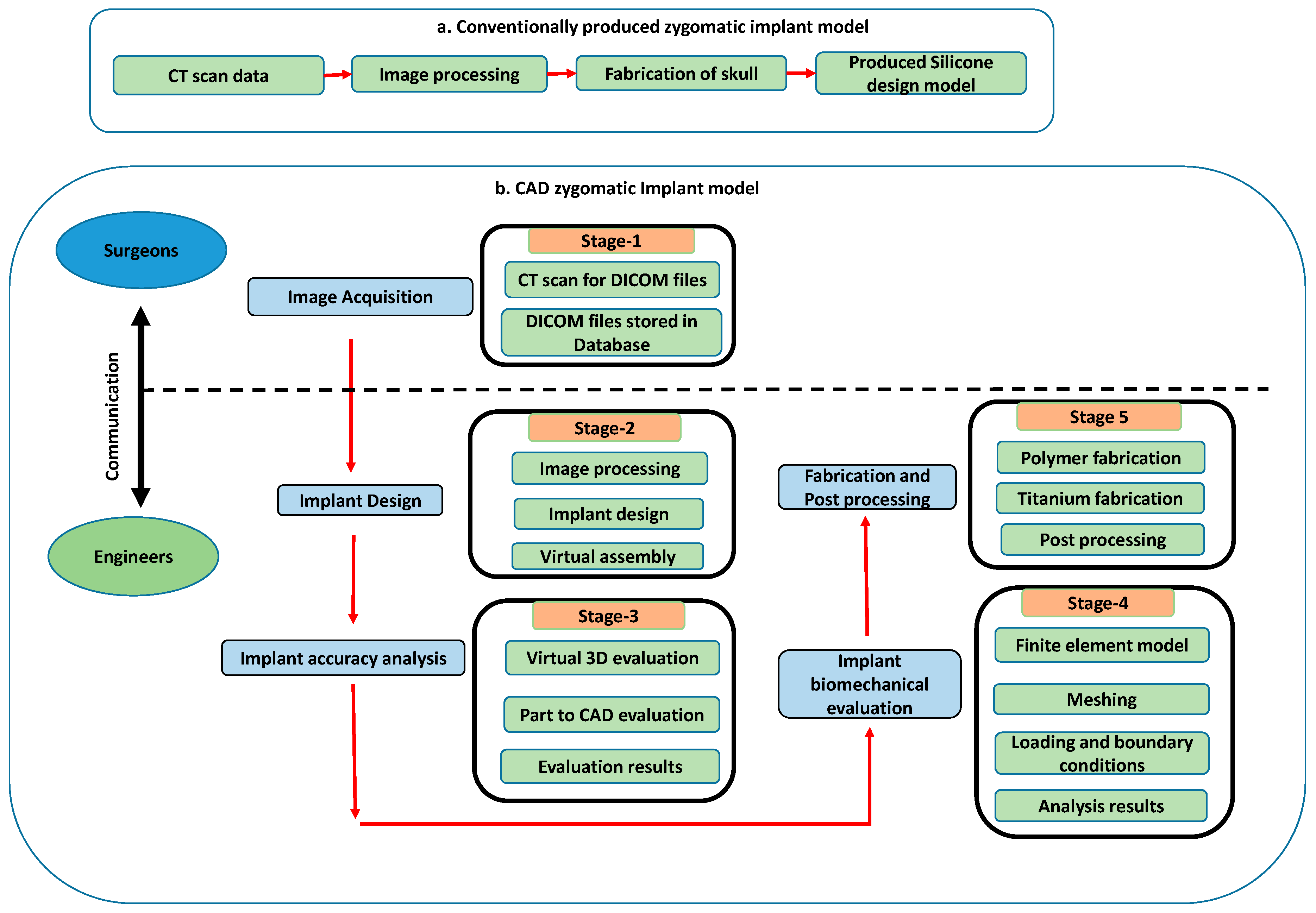
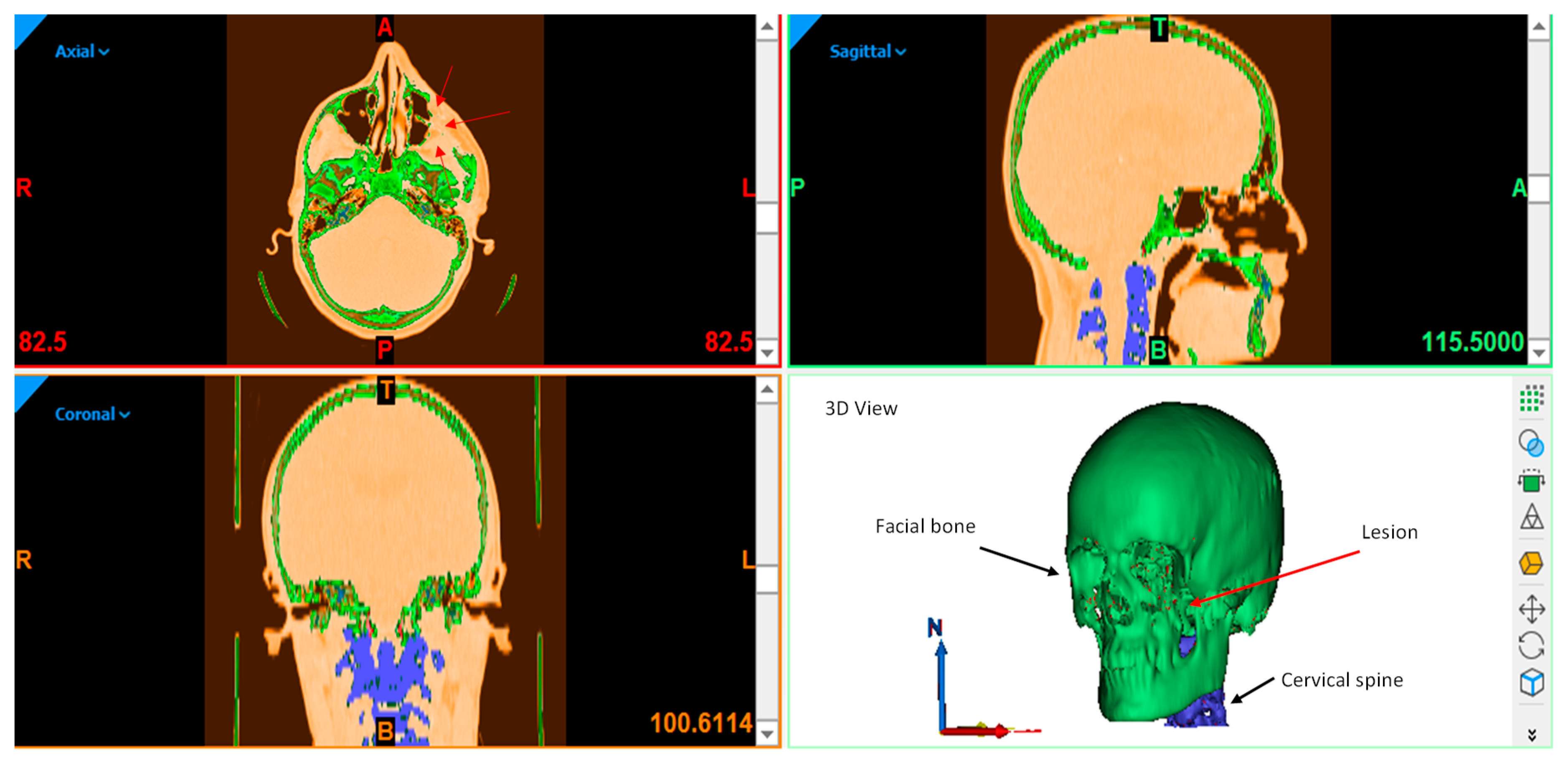
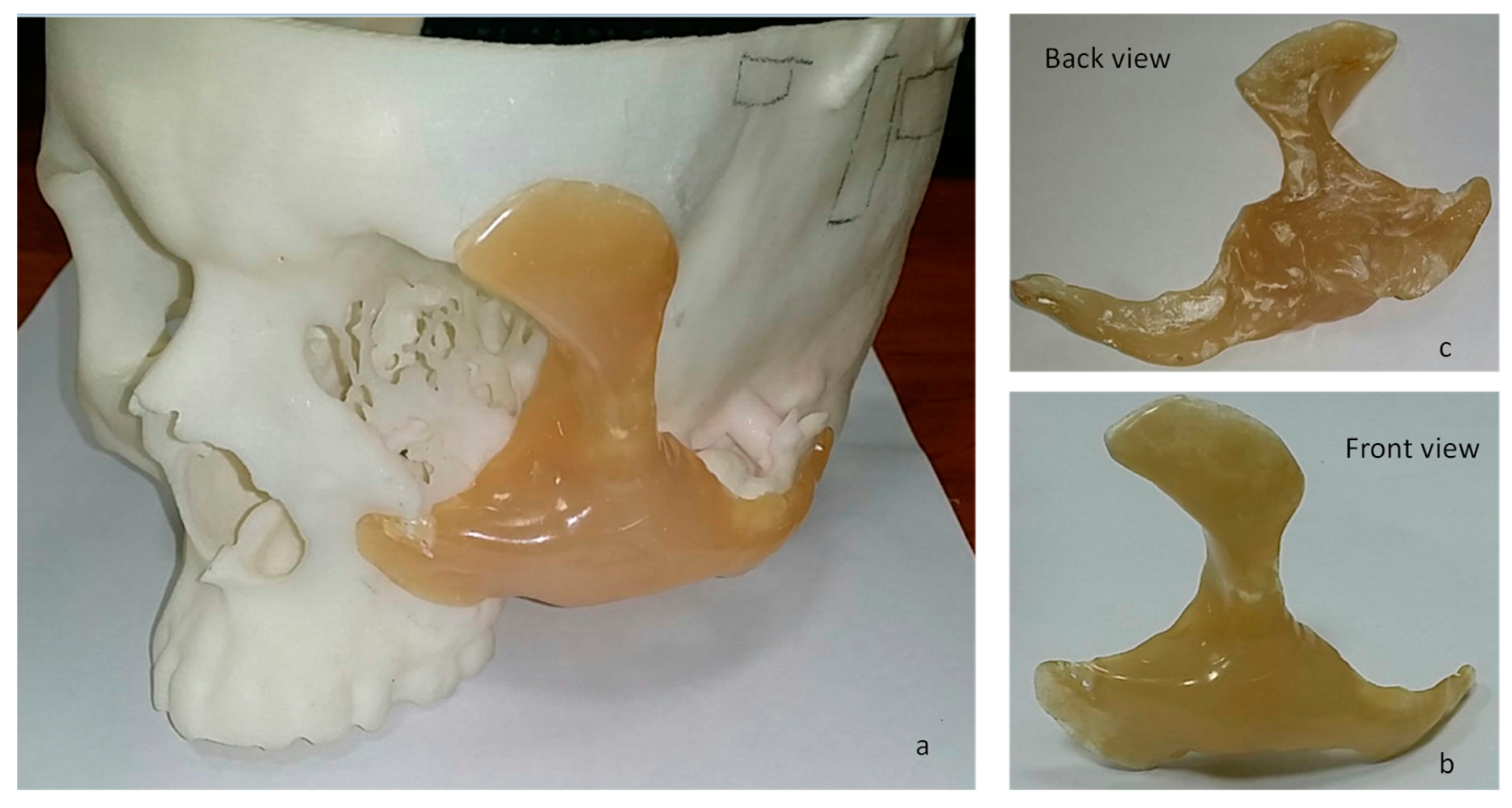
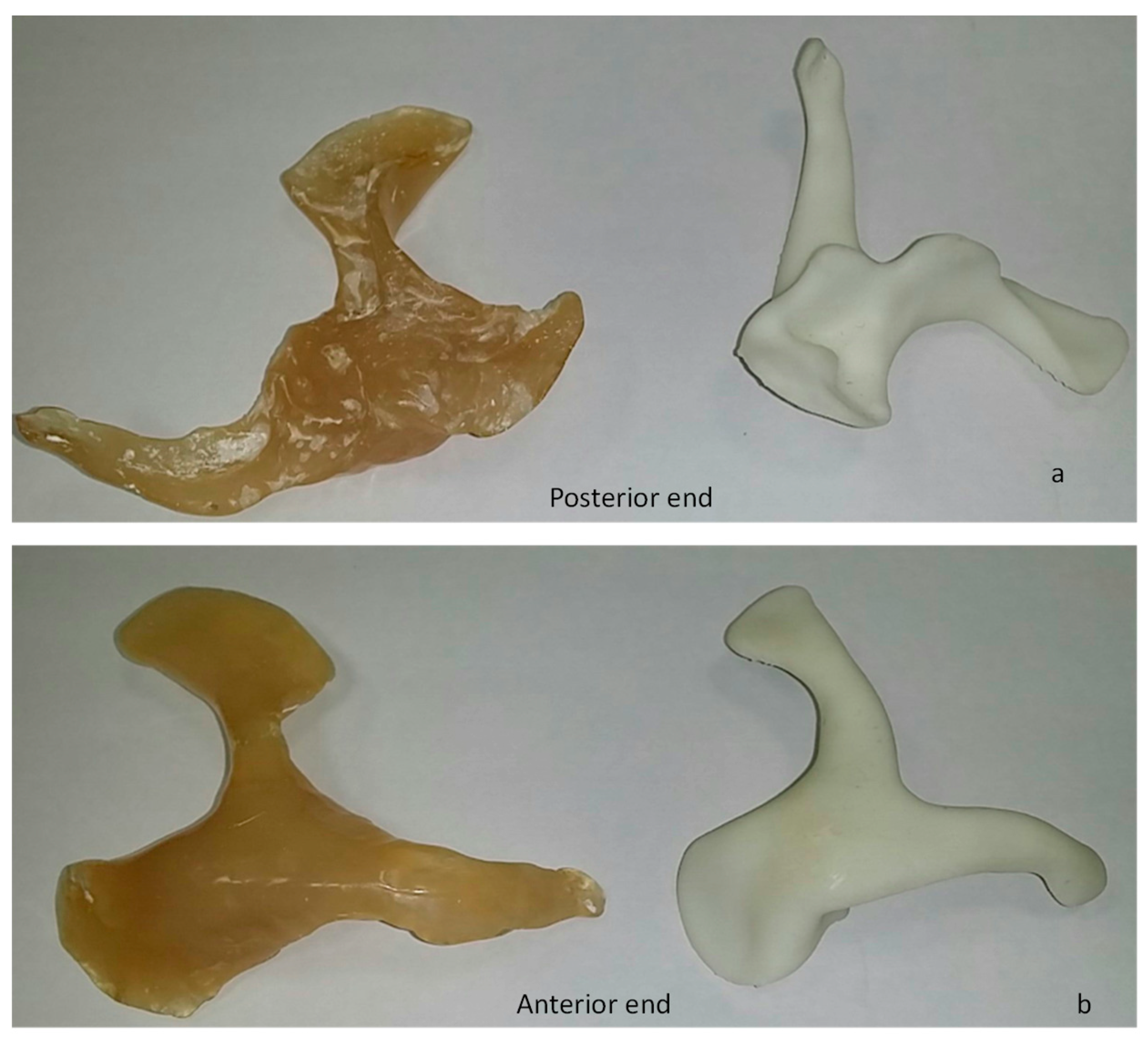
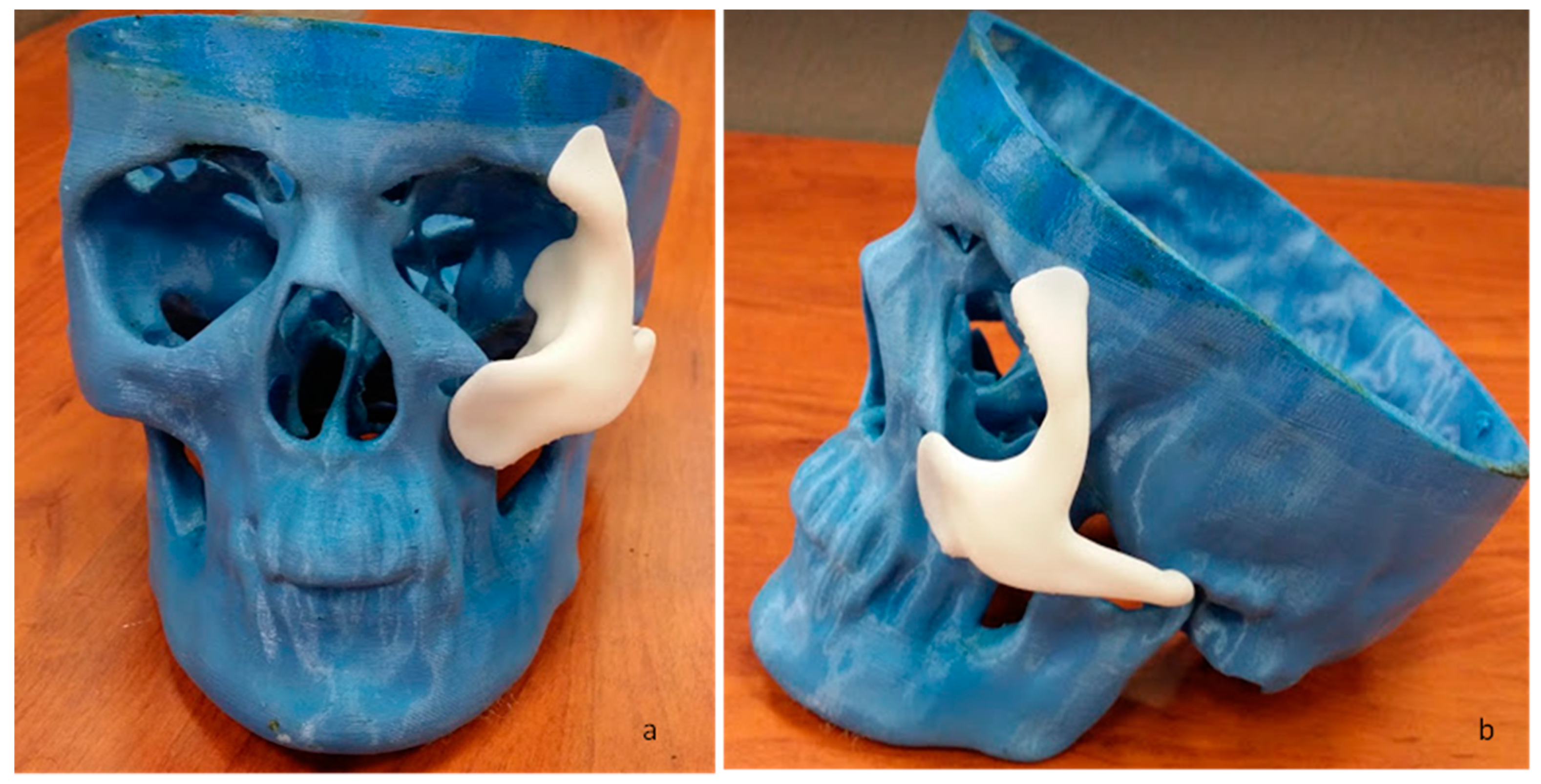
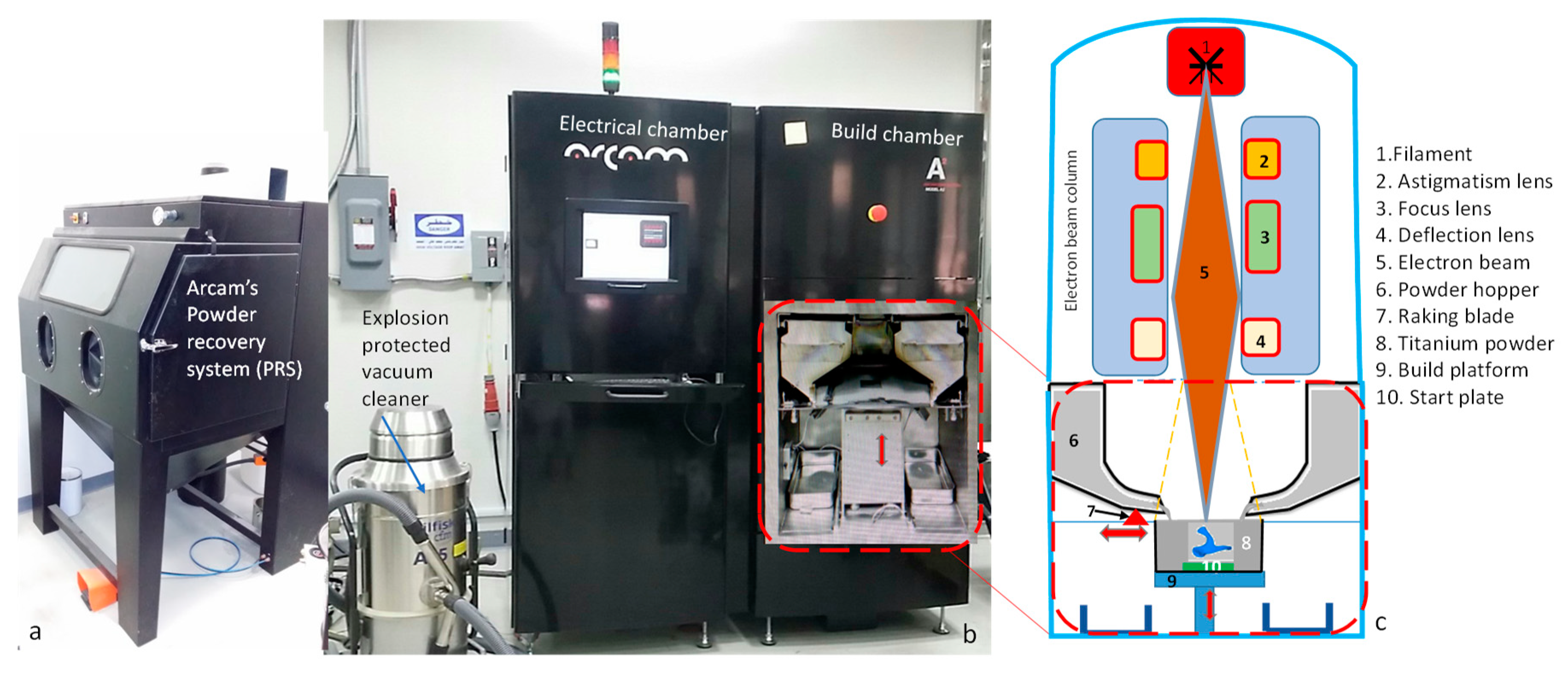
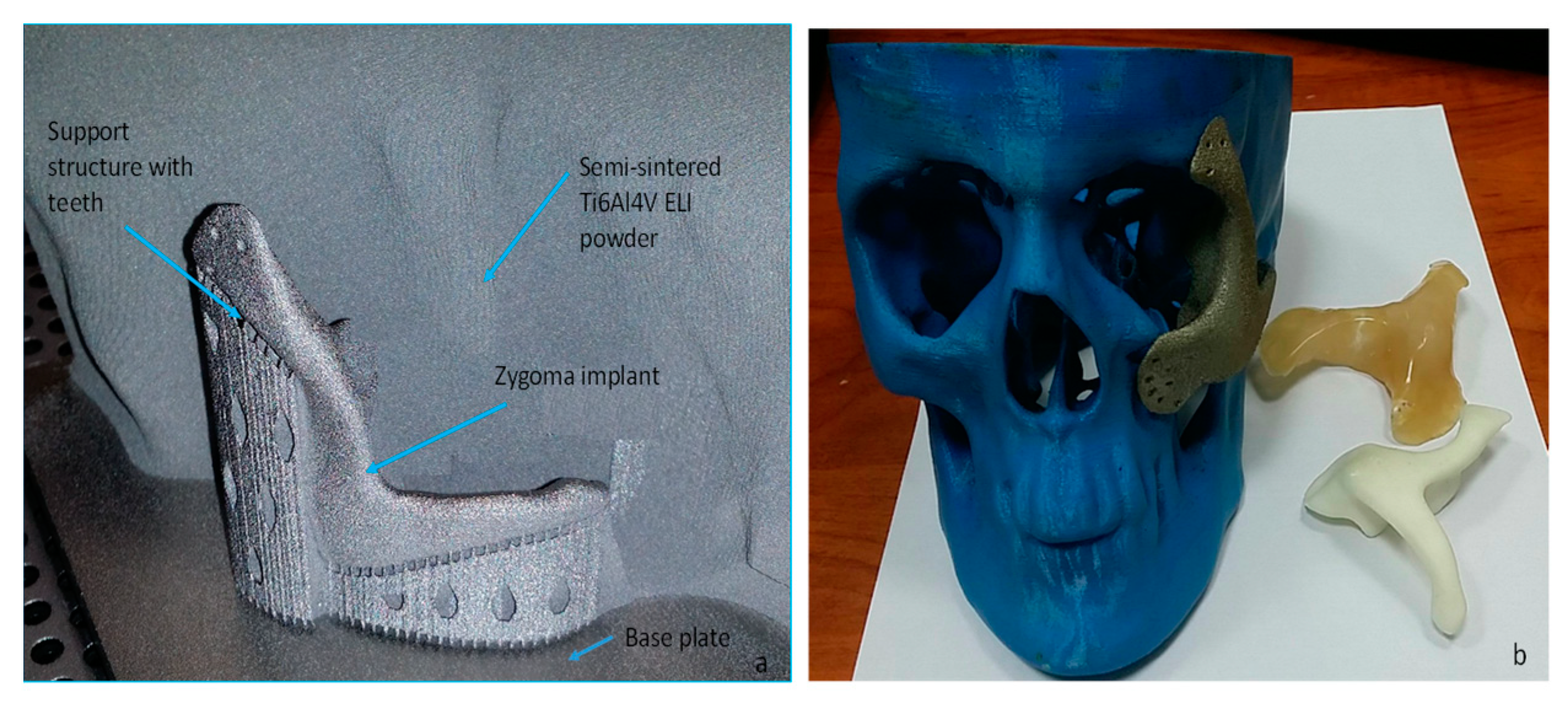
2.1. Implant Customization and Fabrication
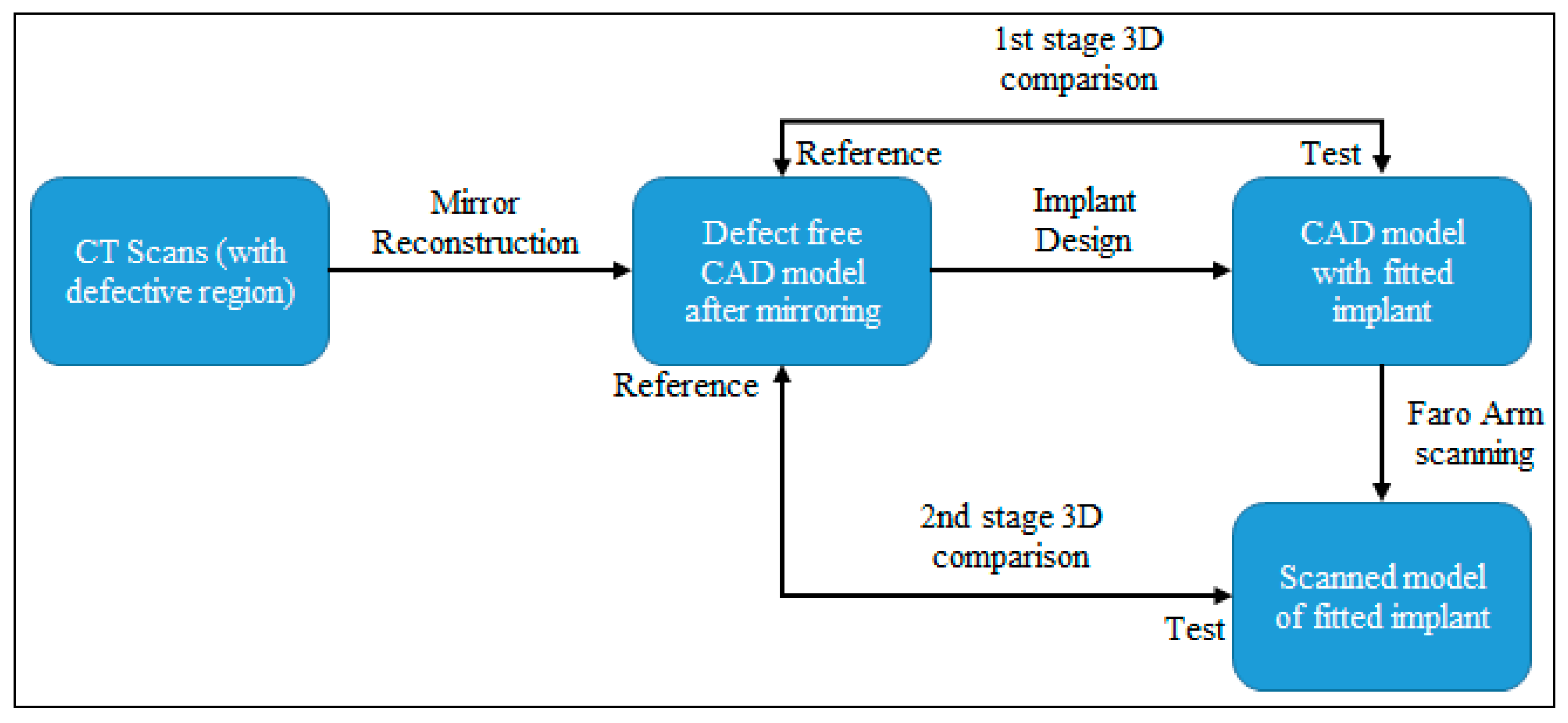
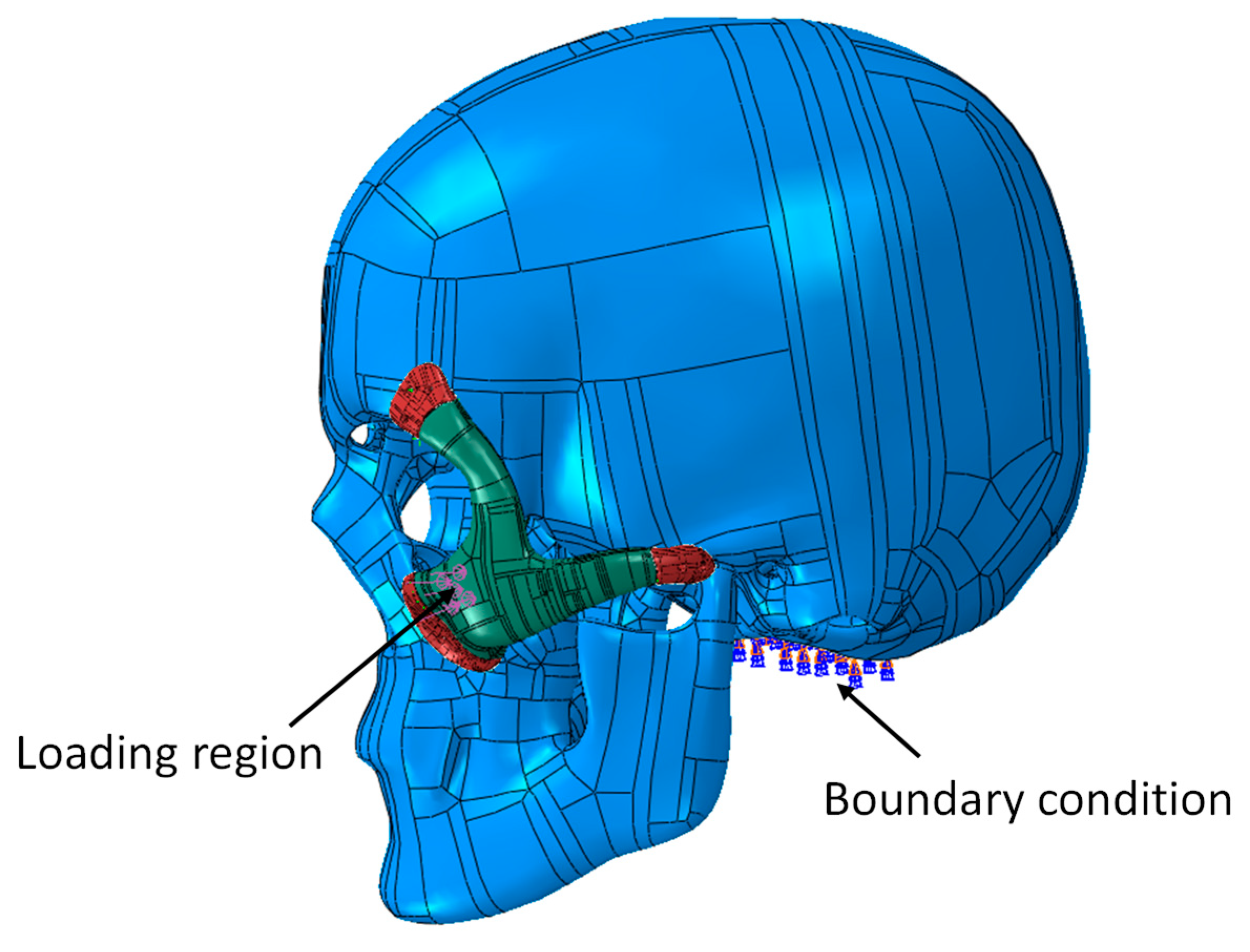
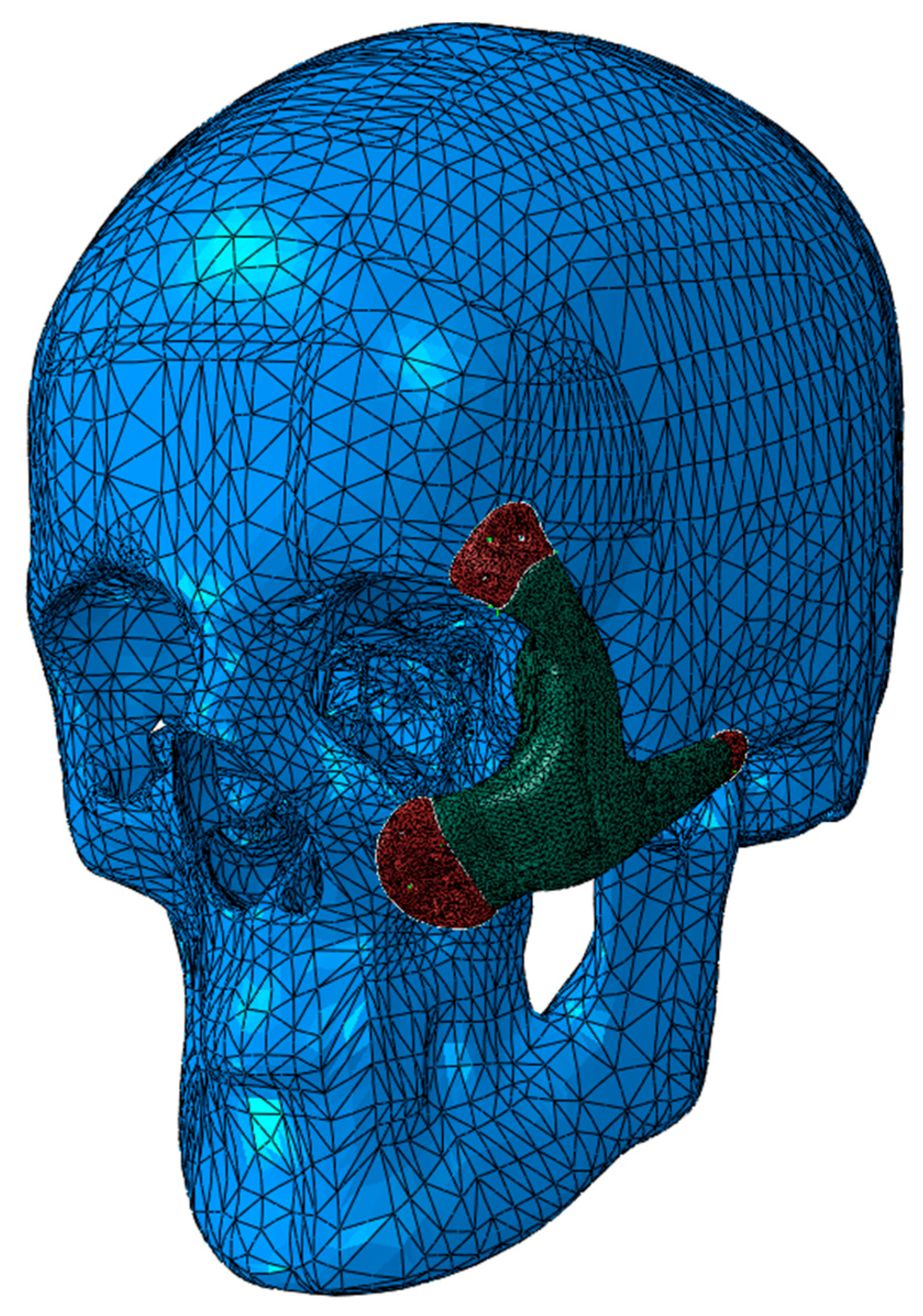
2.2. Evaluation
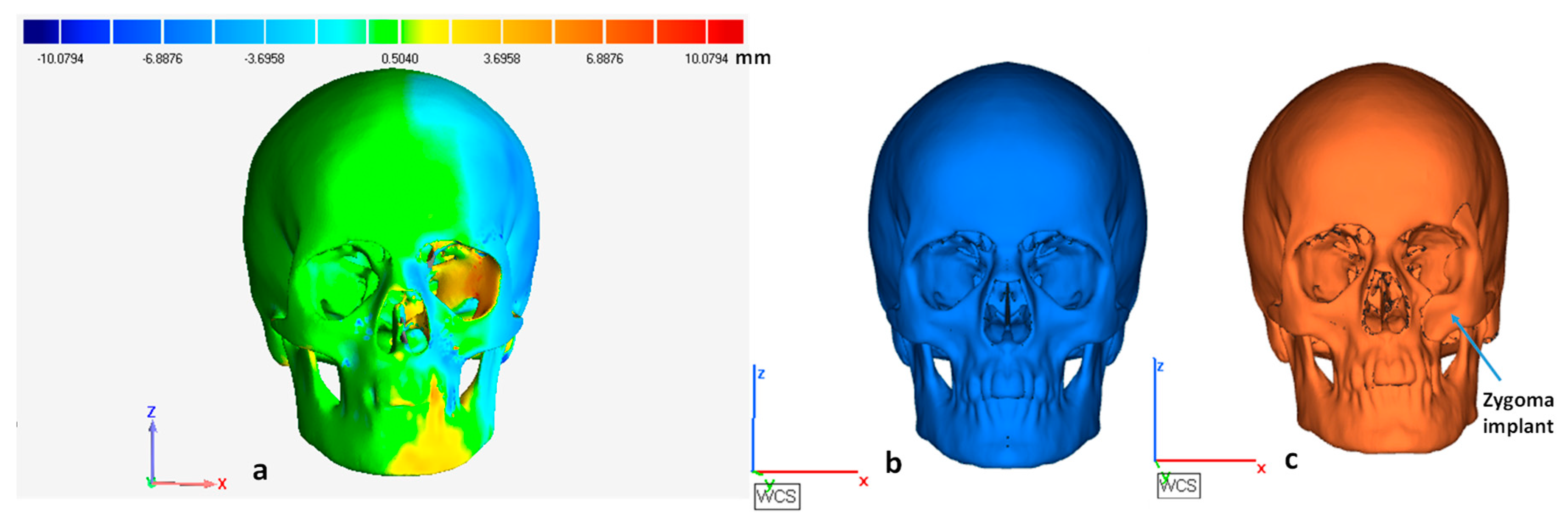
- First stage comparison before fabrication. In this stage, the tumor-free model after mirroring was taken as a reference and the skull model with the implant was considered as a test file. It was done to quantify the error from the mirroring stage.
- The second stage after fabrication. The 3D model obtained using the Faro platinum arm scanner (FARO, Lake Mary, FL, USA) was used to inspect the implant with the skull model. The 3D model obtained from a Faro arm scanner was considered as a test file and the tumor-free model after mirroring was fixed as the reference file. The test was aligned and superimposed on the error-free mirror model to analyze the deviation error.
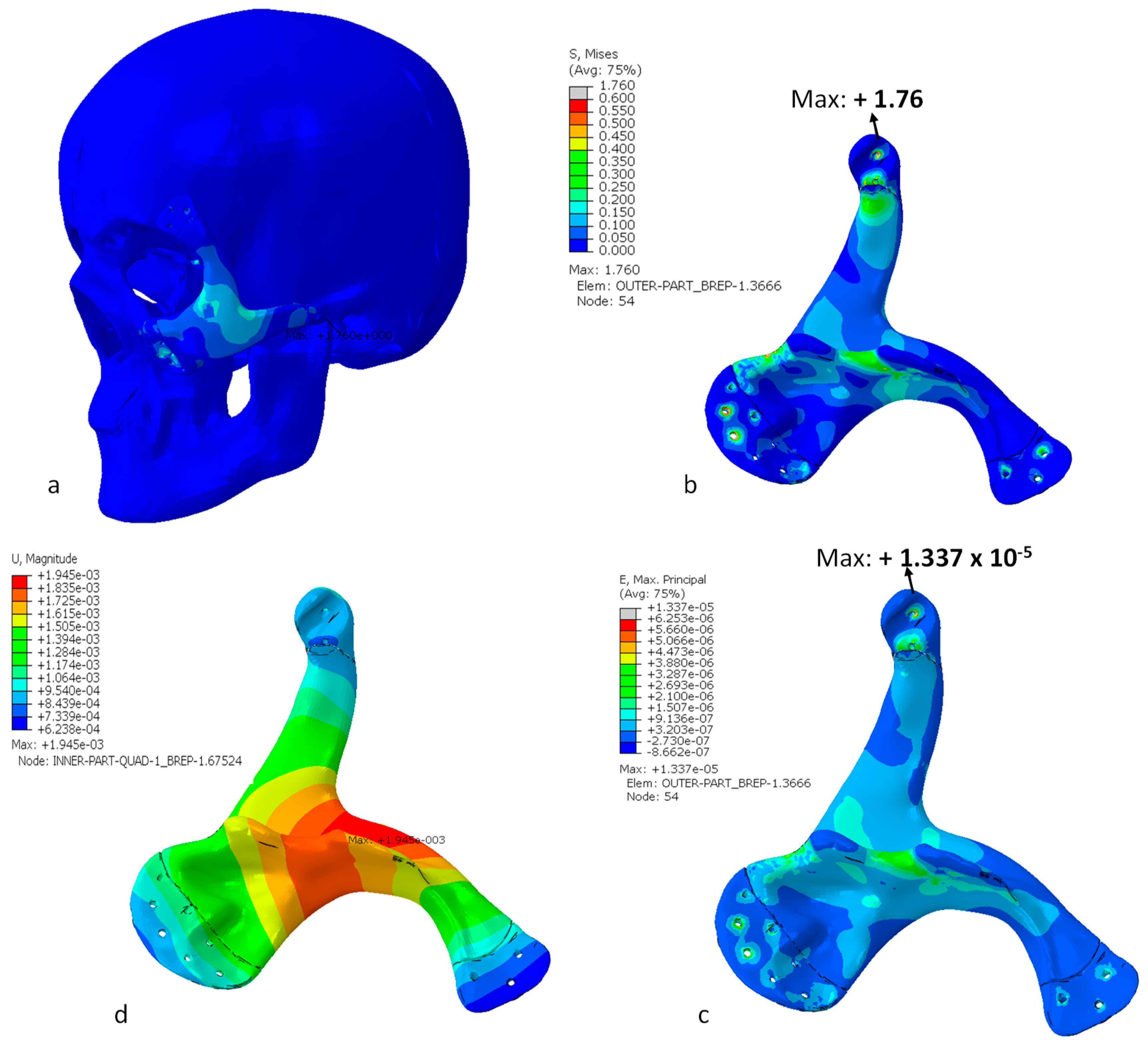
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Di, M.P.; Coburn, J.; Hwang, D.; Kelly, J.; Khairuzzaman, A.; Ricles, L. Additively manufactured medical products-the FDA perspective. 3D Print Med. 2016, 2, 1–6. [Google Scholar]
- de Viteri, V.S.; Fuentes, E. Titanium and Titanium Alloys as Biomaterials. Tribol. Fundam. Adv. InTech. 2013, 155–181. [Google Scholar]
- Balazic, M.; Kopac, J.; Jackson, M.J.; Ahmed, W. Review: Titanium and titanium alloy applications in medicine. IJNBM 2007, 1, 3. [Google Scholar] [CrossRef]
- Parthasarathy, J. 3D modeling, custom implants and its future perspectives in craniofacial surgery. Ann. Maxillofac. Surg. 2013, 4, 9. [Google Scholar] [CrossRef]
- Starch-Jensen, T.; Linnebjerg, L.B.; Jensen, J.D. Treatment of Zygomatic Complex Fractures with Surgical or Nonsurgical Intervention: A Retrospective Study. Int. J. Oral Maxillofac. Surg. 2018, 12, 377–387. [Google Scholar] [CrossRef]
- Lee, H.-S.; Choi, H.-M.; Choi, D.-S.; Jang, I.; Cha, B.-K. Bone thickness of the infrazygomatic crest area in skeletal Class III growing patients: A computed tomographic study. Imaging Sci. Dent. 2013, 43, 261–266. [Google Scholar] [CrossRef]
- Pryor McIntosh, L.; Strait, D.S.; Ledogar, J.A.; Smith, A.L.; Ross, C.F.; Wang, Q.; Opperman, L.A.; Dechow, P.C. Internal Bone Architecture in the Zygoma of Human and Pan. Anat. Rec. 2016, 299, 1704–1717. [Google Scholar] [CrossRef]
- Milne, N.; Fitton, L.C.; Kupczik KFagan, M.J.; O’Higgins, P. The role of the zygomaticomaxillary suture in modulating strain distribution within the skull of Macaca fascicularis. Homo J. Comp. Hum. Biol. 2009, 60, 281. [Google Scholar]
- Foletti, J.M.; Martinez, V.; Haen, P.; Godio-Raboutet, Y.; Guyot LThollon, L. Finite element analysis of the human orbit. Behavior of titanium mesh for orbital floor reconstruction in case of trauma recurrence. J. Stomatol. Oral Maxillofac. Surg. 2019, 120, 91–94. [Google Scholar] [CrossRef]
- Parel, S.M.; Brånemark, P.I.; Ohrnell, L.O.; Svensson, B. Remote implant anchorage for the rehabilitation of maxillary defects. J. Prosthet. Dent. 2001, 86, 377–381. [Google Scholar] [CrossRef]
- Quatela, V.C.; Chow, J. Synthetic facial implants. Facial Plast. Surg. Clin. N. Am. 2008, 16, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Scolozzi, P. Maxillofacial reconstruction using polyetheretherketone patient-specific implants by ‘mirroring’ computational planning. Aesthetic Plast. Surg. 2012, 36, 660–665. [Google Scholar] [CrossRef] [PubMed]
- Ivy, E.J.; Lorenc, Z.P.; Aston, S.J. Malar augmentation with silicone implants. Plast. Reconstr. Surg. 1995, 96, 63–68. [Google Scholar] [CrossRef] [PubMed]
- El-Khayat, B.; Eley, K.A.; Shah, K.A.; Watt-Smith, S.R. Ewings sarcoma of the zygoma reconstructed with a gold prosthesis: A rare tumor and unique reconstruction. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 109, e5–e10. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, J.; Cornelius, C.P.; Groten, M.; Pröbster, L.; Pfannenberg, C.; Schwenzer, N. Orbital reconstruction with individually copy-milled ceramic implants. Plast. Reconstr. Surg. 1998, 101, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y. Orbital Defect Repair and Secondary Reconstruction of Enophthalmos with Mirror-Technique Fabricated Titanium Mesh. J. Oral Maxillofac. Surg. 2008, 66, 19–20. [Google Scholar] [CrossRef]
- Moiduddin, K.; Mian, S.H.; Umer, U.; Alkhalefah, H. Fabrication and Analysis of a Ti6Al4V Implant for Cranial Restoration. Appl. Sci. 2019, 9, 2513. [Google Scholar] [CrossRef]
- Liu, Y.; Xu, L.; Zhu, H.; Liu, S.S.-Y. Technical procedures for template-guided surgery for mandibular reconstruction based on digital design and manufacturing. Biomed Eng. Online 2014, 13, 63. [Google Scholar] [CrossRef]
- Christensen, A.; Kircher, R.; Lippincott, A. Qualification of electron beam melted (EBM) Ti6Al4V-ELI for orthopaedic implant applications. In Medical Device Materials IV: Proceedings of the Materials and Processes for Medical Devices Conference; Jeremy, G., Ed.; ASM International: Cleveland, OH, USA, 2007; Volume 6, pp. 48–53. [Google Scholar]
- Niinomi, M. Recent research and development in titanium alloys for biomedical applications and healthcare goods. Sci. Technol. Adv. Mater. 2003, 4, 445. [Google Scholar] [CrossRef]
- Ehtemam-Haghighi, S.; Prashanth, K.G.; Attar, H.; Chaubey, A.K.; Cao, G.H.; Zhang, L.C. Evaluation of mechanical and wear properties of Ti xNb 7Fe alloys designed for biomedical applications. Mater. Des. 2016, 111, 592–599. [Google Scholar] [CrossRef]
- Huynh, V.; Ngo, N.K.; Golden, T.D. Surface Activation and Pretreatments for Biocompatible Metals and Alloys Used in Biomedical Applications. Int. J. Biomater. 2019, 2019, 21. [Google Scholar] [CrossRef] [PubMed]
- Coquim, J.; Clemenzi, J.; Salahi, M.; Sherif, A.; Tavakkoli Avval, P.; Shah, S.; Schemitsch, E.H.; Shaghayegh Bagheri, Z.; Bougherara, H.; Zdero, R. Biomechanical Analysis Using FEA and Experiments of Metal Plate and Bone Strut Repair of a Femur Midshaft Segmental Defect. Biomed. Res. Int. 2018, 2018, 11. [Google Scholar] [CrossRef] [PubMed]
- Lemu, H.G. Virtual engineering in design and manufacturing. Adv. Manuf. 2014, 2, 289–294. [Google Scholar] [CrossRef]
- Shah, F.A.; Thomsen, P.; Palmquist, A. Osseointegration and current interpretations of the bone-implant interface. Acta Biomater. 2019, 84, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Wysocki, B.; Maj, P.; Sitek, R.; Buhagiar, J.; Kurzydłowski, K.; Święszkowski, W. Laser and Electron Beam Additive Manufacturing Methods of Fabricating Titanium Bone Implants. Appl. Sci. 2017, 7, 657. [Google Scholar] [CrossRef]
- Li, X.; Wang, C.; Zhang, W.; Li, Y. Fabrication and characterization of porous Ti6Al4V parts for biomedical applications using electron beam melting process. Mater. Lett. 2009, 63, 403–405. [Google Scholar] [CrossRef]
- Moiduddin, K.; Hammad Mian, S.; Alkindi, M.; Ramalingam, S.; Alkhalefah, H.; Alghamdi, O. An in vivo Evaluation of Biocompatibility and Implant Accuracy of the Electron Beam Melting and Commercial Reconstruction Plates. Metals 2019, 9, 1065. [Google Scholar] [CrossRef]
- Hoang, D.; Perrault, D.; Stevanovic, M.; Ghiassi, A. Surgical applications of three-dimensional printing: A review of the current literature & how to get started. Ann. Transl. Med. 2016, 4, 456. [Google Scholar]
- Lee, J.-W.; Fang, J.-J.; Chang, L.-R.; Yu, C.-K. Mandibular Defect Reconstruction with the Help of Mirror Imaging Coupled with Laser Stereolithographic Modeling Technique. J. Formos. Med. Assoc. 2007, 106, 244–250. [Google Scholar] [CrossRef]
- Kashi, A.; Saha, S. Mechanisms of failure of medical implants during long-term use. In Biointegration of Medical Implant Materials; Sharma, C.P., Ed.; Woodhead Publishing: Cambridge, UK, 2010; pp. 326–348. [Google Scholar]
- Singare, S.; Shenggui, C.; Sheng, L. The use of 3D printing technology in human defect reconstruction-a review of cases study. Med. Res. Innov. 2017, 1, 1–4. [Google Scholar] [CrossRef]
- Moiduddin, K.; Al-Ahmari, A.; Nasr, E.S.A.; Mian, S.H.; Al Kindi, M. A comparison study on the design of mirror and anatomy reconstruction technique in maxillofacial region. Technol. Health Care 2016, 24, 377–389. [Google Scholar] [CrossRef] [PubMed]
- Jardini, A.L.; Larosa, M.A.; Maciel Filho, R.; de Carvalho Zavaglia, C.A.; Bernardes, L.F.; Lambert, C.S.; Calderoni, D.R.; Kharmandayan, P. Cranial reconstruction: 3D biomodel and custom-built implant created using additive manufacturing. J. Cranio-Maxillofac. Surg. 2014, 42, 1877–1884. [Google Scholar] [CrossRef] [PubMed]
- Lütjering, G.; Williams, J.C. Titanium; Springer Science & Business Media: Berlin, Germany, 2007. [Google Scholar]
- Arcam, A. Arcam A2 Technical Specification. ARCAM A2 TECHNICAL DATA. 2019. Available online: http://www.arcam.com/wp-content/uploads/Arcam-A2.pdf (accessed on 23 May 2019).
- New! 50 µm Process for High Resolution and Surface Finish. 21 May 2012. Available online: http://www.arcam.com/new-50-um-process-for-high-resolution-and-surface-finish (accessed on 14 September 2019).
- Umer, U.; Ameen, W.; Abidi, M.H.; Moiduddin, K.; Alkhalefah, H.; Alkahtani, M.; Al-Ahmari, A. Modeling the Effect of Different Support Structures in Electron Beam Melting of Titanium Alloy Using Finite Element Models. Metals 2019, 9, 806. [Google Scholar] [CrossRef]
- Mian, S.H.; Mannan, M.A.; Al-Ahmari, A.M. The influence of surface topology on the quality of the point cloud data acquired with laser line scanning probe. Sens. Rev. 2014, 34, 255–265. [Google Scholar] [CrossRef]
- El-Anwar, M.I.; Mohammed, M.S. Comparison between two low profile attachments for implant mandibular overdentures. J. Genet. Eng. Biotechnol. 2014, 12, 45–53. [Google Scholar] [CrossRef] [Green Version]
- Arcam, Ti6Al4V ELI Titanium Alloy, Ti6Al4V ELI Titanium Alloy. Available online: http://www.arcam.com/wp-content/uploads/Arcam-Ti6Al4V-ELI-Titanium-Alloy.pdf (accessed on 23 September 2019).
- Nagasao, M.; Nagasao, T.; Imanishi, Y.; Tomita, T.; Tamaki, T.; Ogawa, K. Experimental evaluation of relapse-risks in operated zygoma fractures. Auris. Nasus. Larynx. 2009, 36, 168–175. [Google Scholar] [CrossRef]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Materials | Young’s Modulus (GPa) | Poisson’s Ratio | Yield Strength (MPa) |
|---|---|---|---|
| Cortical bone | 13.7 | 0.3 | 122 |
| Zygomatic implant (Ti-6Al-4V ELI) | 120 | 0.3 | 930 |
| Comparison | Models | AVG Deviation (mm) | Root Mean Square Error (RMSE) (mm) |
|---|---|---|---|
| 1st Stage (virtual evaluation using Geomagics®) | Zygomatic mirror and zygomatic with implant (3D comparison) | 1.65/–1.55 | 2.38 |
| Zygomatic mirror and zygomatic with implant (2D comparison on Implant region) | 0.86/–0.97 | 1.28 | |
| 2nd Stage (physical model evaluation using Faro arm scanner) | Zygomatic mirror and zygomatic with implant (3D comparison) | 1.82/–3.86 | 4.25 |
| Zygomatic mirror and zygomatic with implant (2D comparison on Implant region) | 1.40/–1.79 | 1.96 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moiduddin, K.; Hammad Mian, S.; Umer, U.; Ahmed, N.; Alkhalefah, H.; Ameen, W. Reconstruction of Complex Zygomatic Bone Defects Using Mirroring Coupled with EBM Fabrication of Titanium Implant. Metals 2019, 9, 1250. https://doi.org/10.3390/met9121250
Moiduddin K, Hammad Mian S, Umer U, Ahmed N, Alkhalefah H, Ameen W. Reconstruction of Complex Zygomatic Bone Defects Using Mirroring Coupled with EBM Fabrication of Titanium Implant. Metals. 2019; 9(12):1250. https://doi.org/10.3390/met9121250
Chicago/Turabian StyleMoiduddin, Khaja, Syed Hammad Mian, Usama Umer, Naveed Ahmed, Hisham Alkhalefah, and Wadea Ameen. 2019. "Reconstruction of Complex Zygomatic Bone Defects Using Mirroring Coupled with EBM Fabrication of Titanium Implant" Metals 9, no. 12: 1250. https://doi.org/10.3390/met9121250
APA StyleMoiduddin, K., Hammad Mian, S., Umer, U., Ahmed, N., Alkhalefah, H., & Ameen, W. (2019). Reconstruction of Complex Zygomatic Bone Defects Using Mirroring Coupled with EBM Fabrication of Titanium Implant. Metals, 9(12), 1250. https://doi.org/10.3390/met9121250