
Indoor Airflow Dynamics in Compartmentalized Pneumology Units Equipped with Variable-Thickness MERV-13 Filters

 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Background
2.1. Filtration Systems for Indoor Environment
2.2. Brazilian Hospital Standards
- Level 0. Areas where the risk does not exceed that found in public and collective environments.
- Level 1. Areas in which no health risks related to air quality have been found, but some authorities, organizations, or researchers suggest that some risks should be considered.
- Level 2. Areas in which there is strong evidence of the risk of occurrence of health hazards related to air quality to their occupants or patients, who will use products manipulate in these areas based on well-delineated clinical or epidemiological experimental studies.
- Level 3. Areas where there is strong evidence of a high risk of air quality-related health hazards to their occupants or patients, who will use products manipulated in these areas, under well-delineated experimental, clinical, or epidemiological studies.
3. Methodology
3.1. Mathematical Formulation
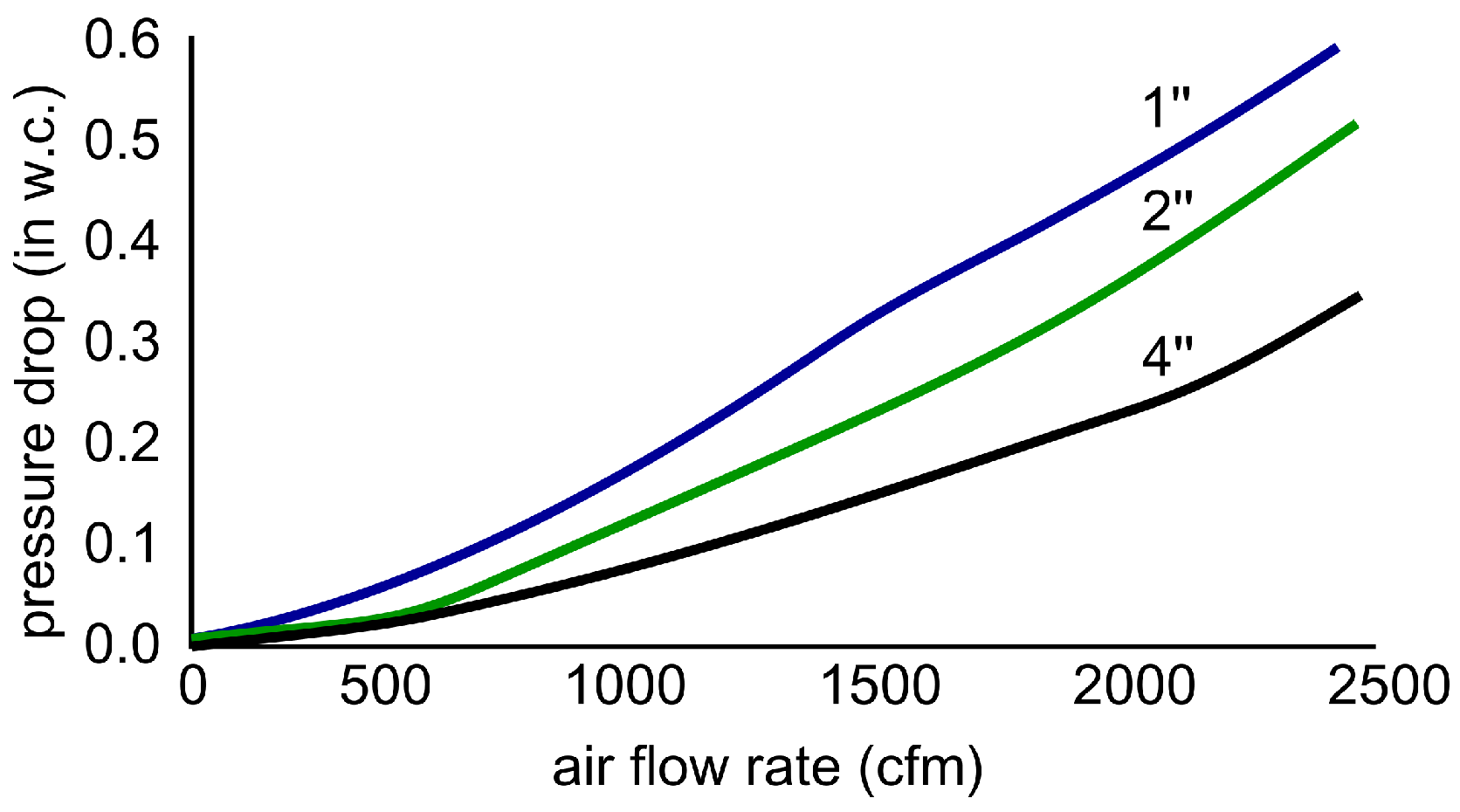
3.2. Filter Characterization
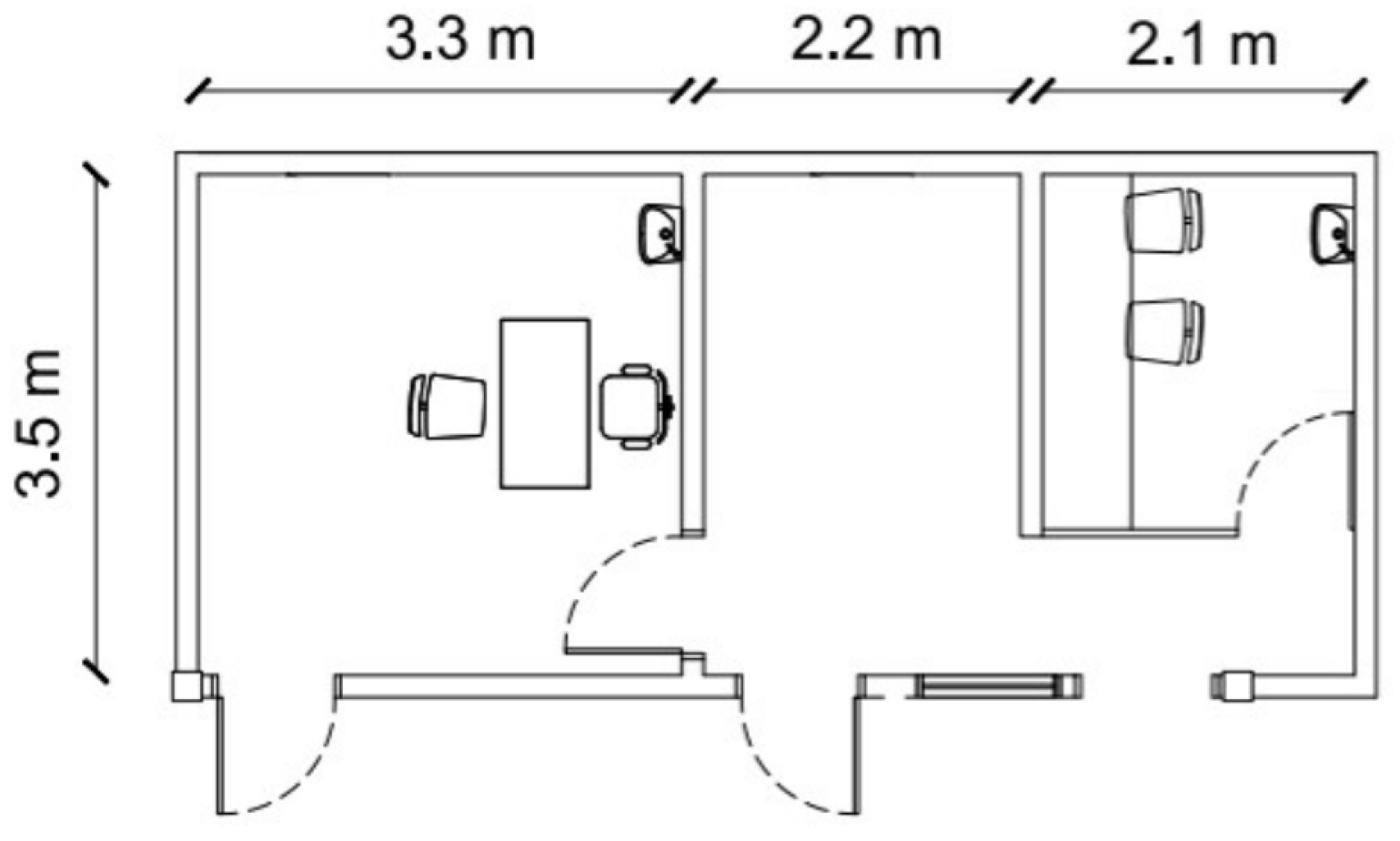
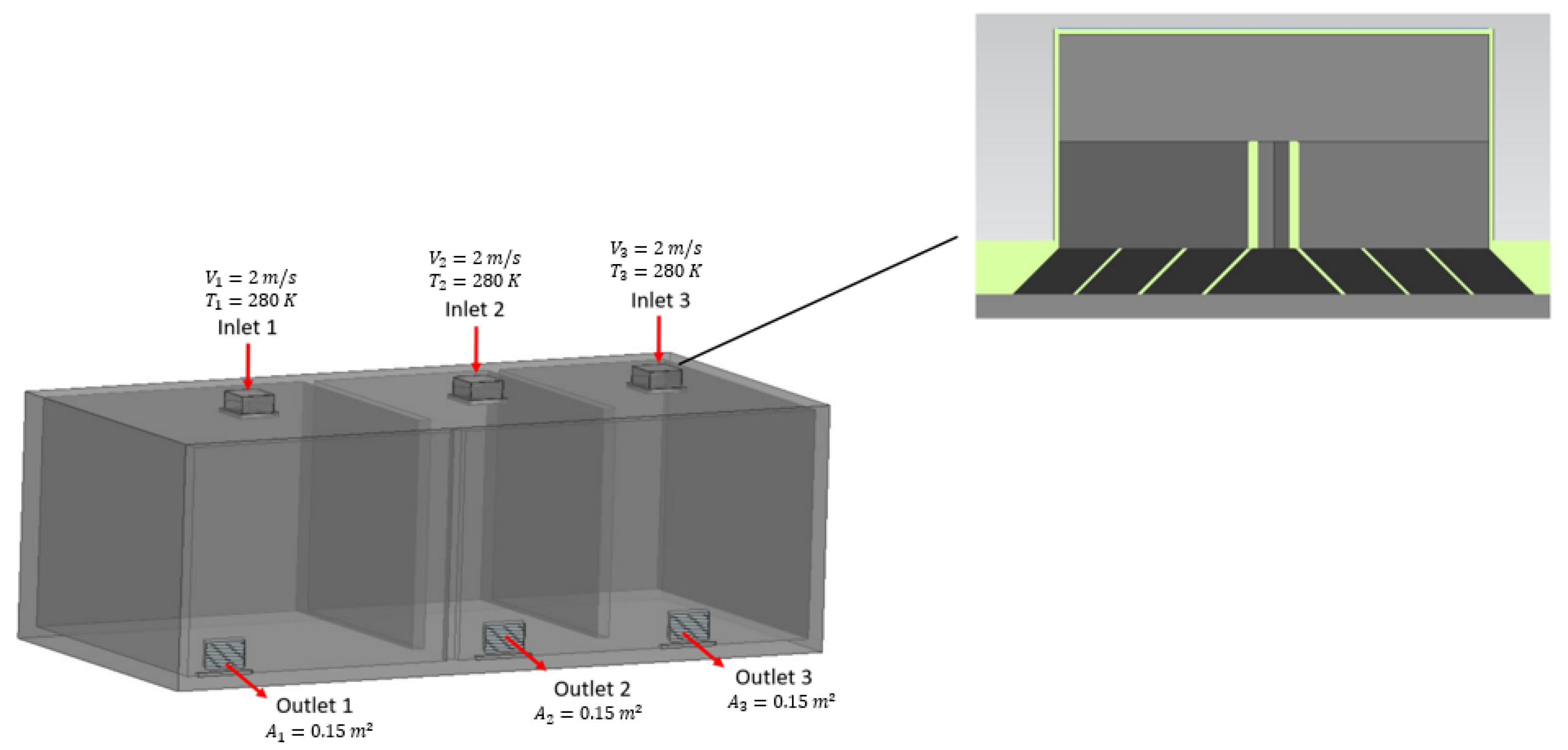
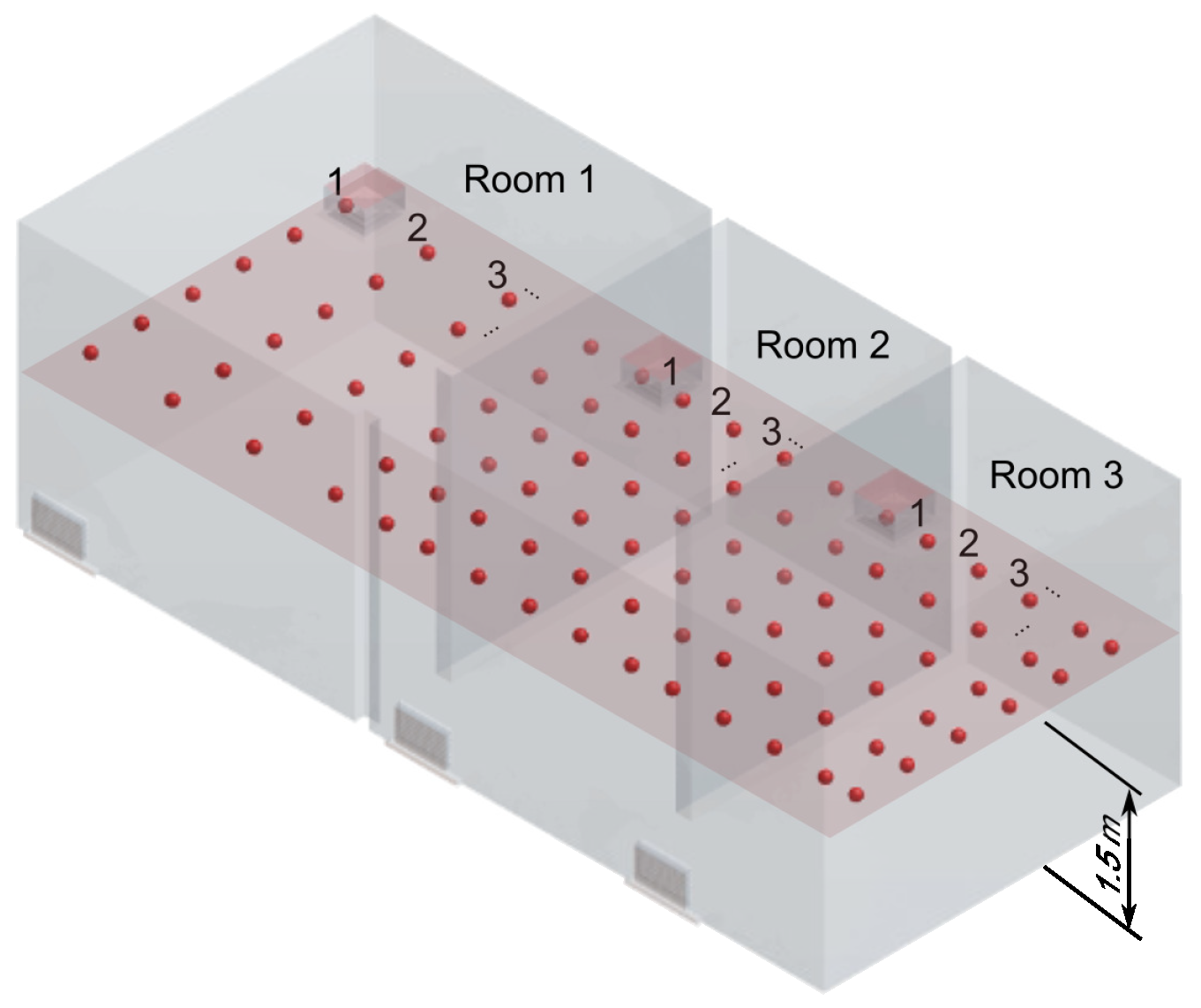
3.3. Problem Setting
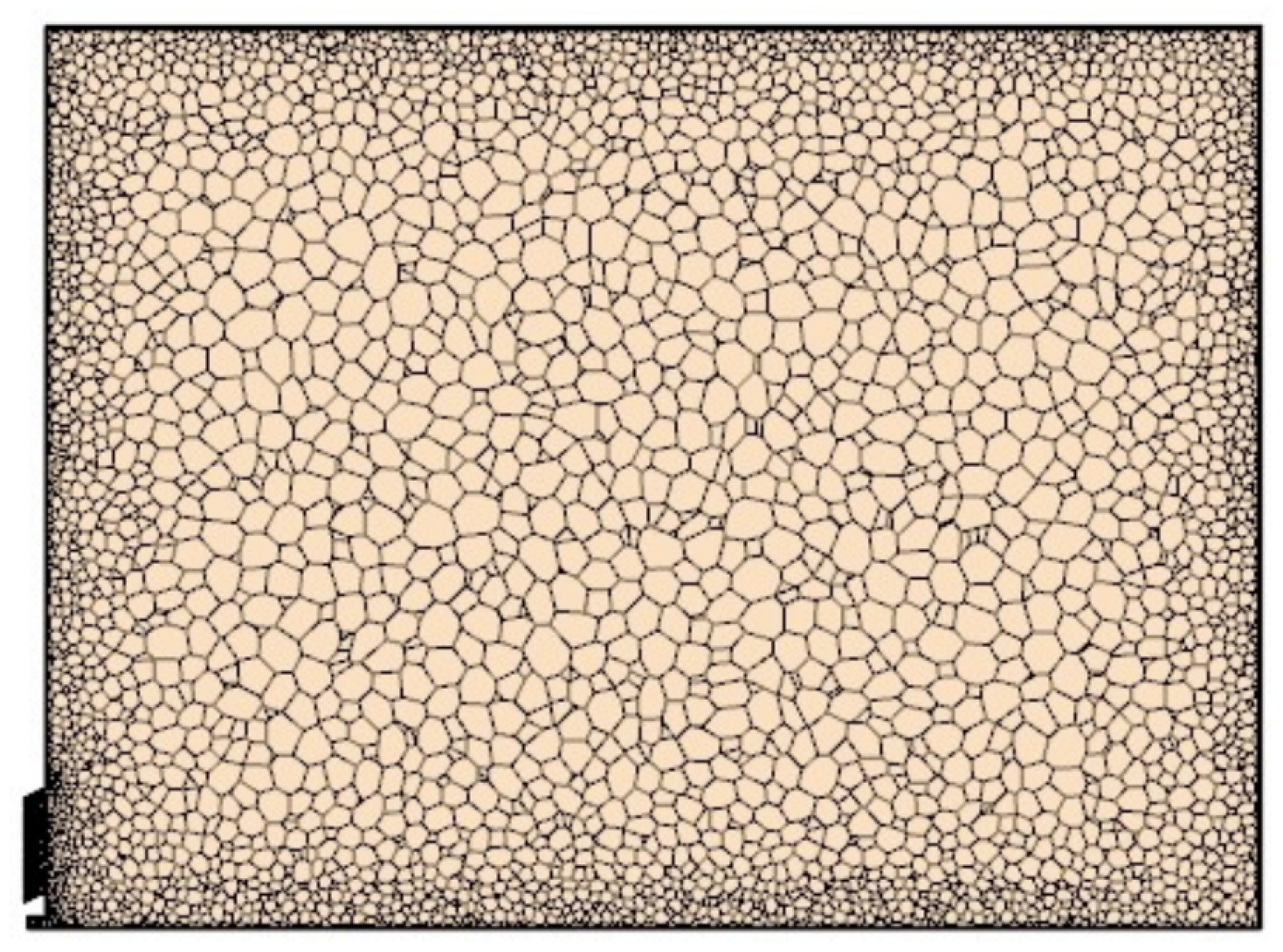
3.4. Discretization Procedures
4. Results and Discussion
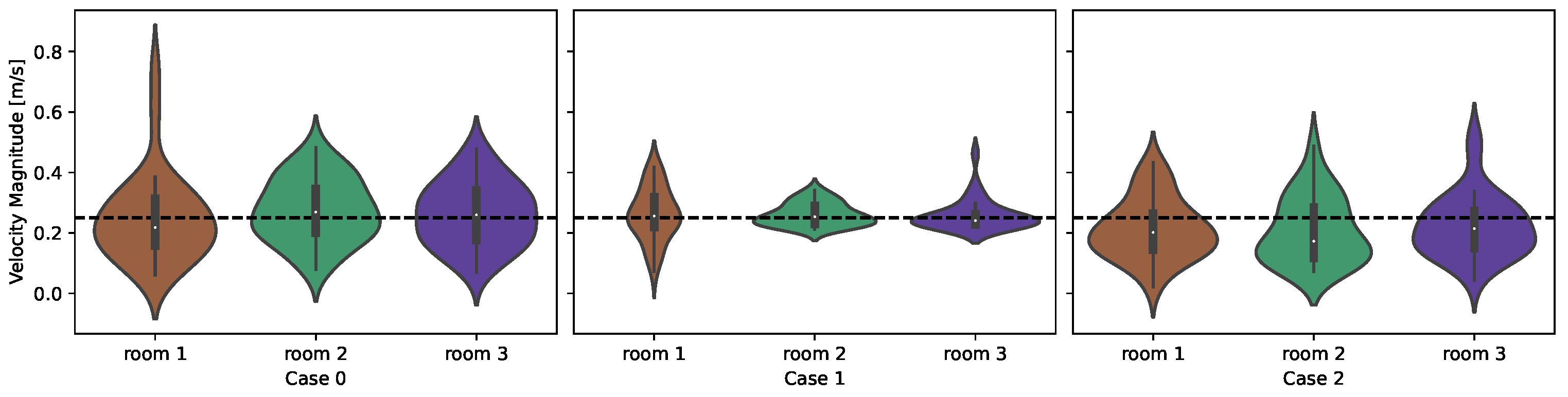
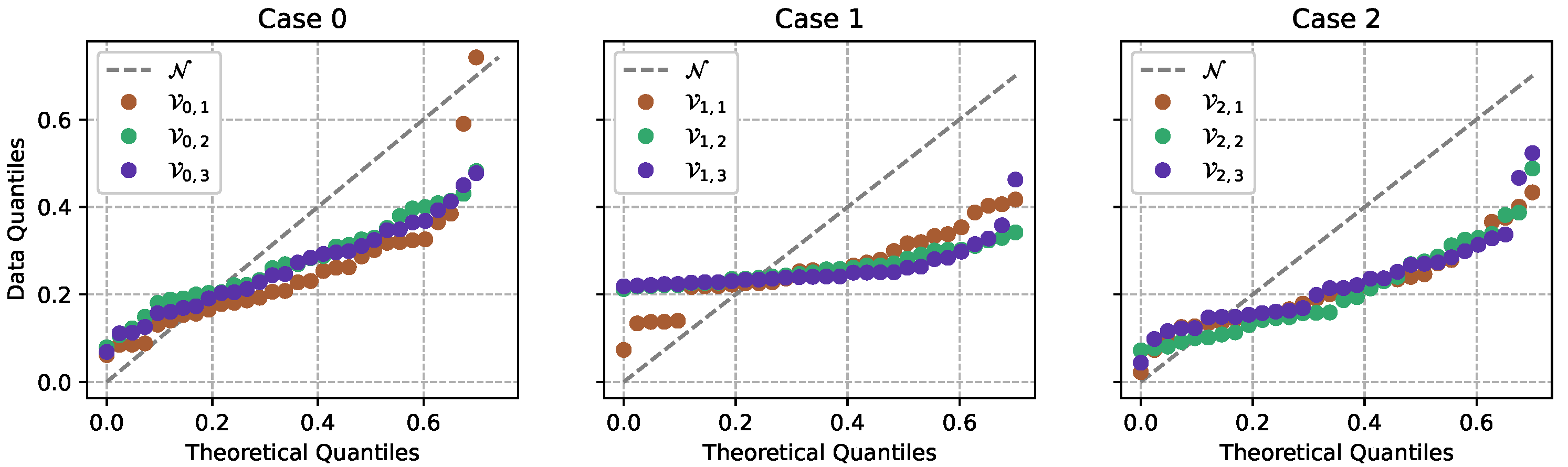
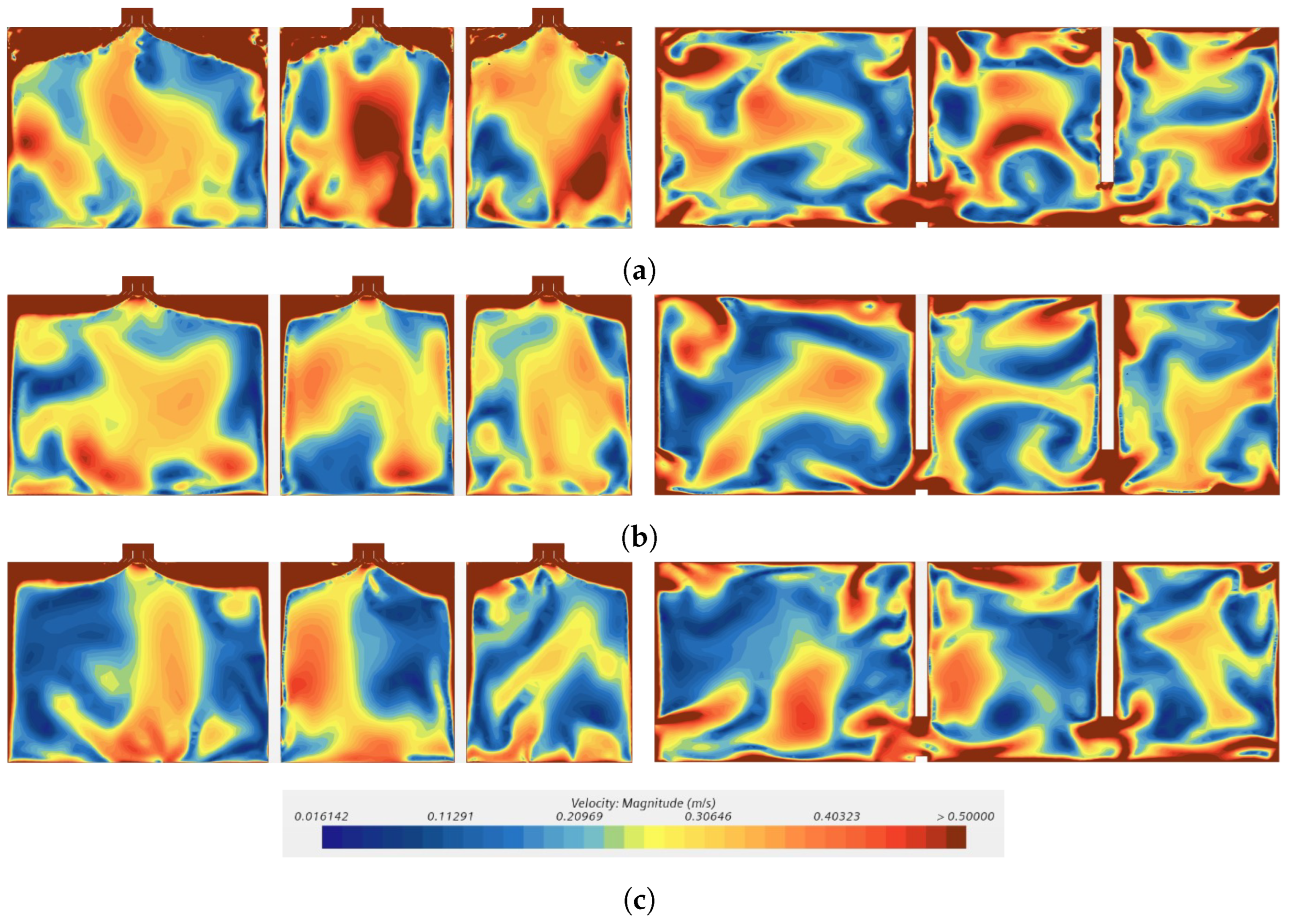
- Case 0: no device;
- Case 1: 1-inch device;
- Case 2: 2-inch device.
4.1. Statistical Analysis
4.2. Hydrodynamic Analysis
4.3. Numerical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Chakraborty, I.; Maity, P. COVID-19 outbreak: Migration, effects on society, global environment and prevention. Sci. Total Environ. 2020, 728, 138882. [Google Scholar] [CrossRef]
- CDC. Scientific Brief: SARS-CoV-2 Transmission. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/sars-cov-2-transmission.html (accessed on 10 February 2022).
- Alrebi, O.F.; Obeidat, B.; Abdallah, I.A.; Darwish, E.F.; Amhamed, A. Airflow dynamics in an emergency department: A CFD simulation study to analyse COVID-19 dispersion. Alex. Eng. J. 2022, 61, 3435–3445. [Google Scholar] [CrossRef]
- Ding, J.; Yu, C.W.; Cao, S.J. HVAC systems for environmental control to minimize the COVID-19 infection. Indoor Built Environ. 2020, 29, 1195–1201. [Google Scholar] [CrossRef]
- Liu, Y.; Ning, Z.; Chen, Y.; Guo, M.; Liu, Y.; Gali, N.K.; Sun, L.; Duan, Y.; Cai, J.; Westerdah, D.; et al. Aerodynamic analysis of SARS-CoV-2 in two Wuhan hospitals. Nature 2020, 582, 557–560. [Google Scholar] [CrossRef]
- Machado, A.A. Infecção pelo vírus Influenza A (H1N1) de origem suína: Como reconhecer, diagnosticar e prevenir. J. Bras. Pneumol. 2009, 35, 464–469. [Google Scholar] [CrossRef] [PubMed]
- Schwartzmann, P.V.; Volpe, G.J.; Vilar, F.C.; Moriguti, J.C. Pneumonia comunitária e pneumonia hospitalar em adultos. Medicina (Ribeirão Preto) 2010, 43, 238–248. [Google Scholar] [CrossRef]
- Eslami, H.; Jalili, M. The role of environmental factors to transmission of SARS-CoV-2 (COVID-19). AMB Express 2020, 10, 92. [Google Scholar] [CrossRef]
- Kwon, T.; Gaudreault, N.N.; Richt, J.A. Environmental stability of SARS-CoV-2 on different types of surfaces under indoor and seasonal climate conditions. Pathogens 2021, 10, 227. [Google Scholar] [CrossRef]
- Stadnytskyi, V.; Bax, C.E.; Bax, A.; Anfinrud, P. The airborne lifetime of small speech droplets and their potential importance in SARS-CoV-2 transmission. Proc. Natl. Acad. Sci. USA 2020, 117, 11875–11877. [Google Scholar] [CrossRef]
- Wang, J.; Tang, K.; Feng, K.; Lv, W. High Temperature and High Humidity Reduce the Transmission of COVID-19. BMJ Open 2020, 3551767, 2020b. Available online: https://www.researchgate.net/publication/339873481_High_Temperature_and_High_Humidity_Reduce_the_Transmission_of_COVID-19 (accessed on 3 February 2023). [CrossRef]
- Satheesan, M.K.; Mui, K.W.; Wong, L.T. A numerical study of ventilation strategies for infection risk mitigation in general inpatient wards. In Proceedings of the Building Simulation, Loughborough, UK, 21–22 September 2020; Springer: Berlin/Heidelberg, Germany, 2020; pp. 1–10. [Google Scholar]
- Bourouiba, L. The fluid dynamics of disease transmission. Annu. Rev. Fluid Mech. 2020, 53, 473–508. [Google Scholar] [CrossRef]
- Löhner, R.; Antil, H.; Idelsohn, S.; Oñate, E. Detailed simulation of viral propagation in the built environment. Comput. Mech. 2020, 66, 1093–1107. [Google Scholar] [CrossRef] [PubMed]
- Vuorinen, V.; Aarnio, M.; Alava, M.; Alopaeus, V.; Atanasova, N.; Auvinen, M.; Balasubramanian, N.; Bordbar, H.; Erästö, P.; Grande, R.; et al. Modelling aerosol transport and virus exposure with numerical simulations in relation to SARS-CoV-2 transmission by inhalation indoors. Saf. Sci. 2020, 130, 104866. [Google Scholar] [CrossRef] [PubMed]
- Al-Baghdadi, M.A.S. CFD analysis of spread COVID-19 with air conditioning systems. Int. J. Energy Environ. 2021, 12, 63–73. [Google Scholar]
- Barbosa, B.P.P.; de Carvalho Lobo Brum, N. Ventilation mode performance against airborne respiratory infections in small office spaces: Limits and rational improvements for COVID-19. J. Braz. Soc. Mech. Sci. Eng. 2021, 43, 316. [Google Scholar] [CrossRef]
- Ren, C.; Zhu, H.C.; Cao, S.J. Ventilation Strategies for Mitigation of Infection Disease Transmission in an Indoor Environment: A Case Study in Office. Buildings 2022, 12, 180. [Google Scholar] [CrossRef]
- Zhang, J.; Huntley, D.; Fox, A.; Gerhardt, B.; Vatine, A.; Cherne, J. Study of viral filtration performance of residential HVAC filters. ASHRAE J. 2020, 62, 26–32. [Google Scholar]
- ASHRAE. Filtration/Disinfection. 2021. Available online: https://www.ashrae.org/technical-resources/filtration-disinfection (accessed on 10 February 2022).
- Mousavi, E.S.; Kananizadeh, N.; Martinello, R.A.; Sherman, J.D. COVID-19 outbreak and hospital air quality: A systematic review of evidence on air filtration and recirculation. Environ. Sci. Technol. 2020, 55, 4134–4147. [Google Scholar] [CrossRef] [PubMed]
- ANVISA. COVID-19: Tudo Sobre Máscaras Faciais de Proteção. 2020. Available online: https://www.gov.br/anvisa/pt-br/assuntos/noticias-anvisa/2020/covid-19-tudo-sobre-mascaras-faciais-de-protecao (accessed on 10 February 2022).
- Chia, P.Y.; Coleman, K.K.; Tan, Y.K.; Ong, S.W.X.; Gum, M.; Lau, S.K.; Lim, X.F.; Lim, A.S.; Sutjipto, S.; Lee, P.H.; et al. Detection of air and surface contamination by SARS-CoV-2 in hospital rooms of infected patients. Nat. Commun. 2020, 11, 2800. [Google Scholar] [CrossRef]
- López-Rebollar, B.M.; Posadas-Bejarano, A.; García-Pulido, D.; Torres-Maya, A.; Díaz-Delgado, C. Proposal of a Mask and Its Performance Analysis with CFD for an Enhanced Aerodynamic Geometry That Facilitates Filtering and Breathing against COVID-19. Fluids 2021, 6, 408. [Google Scholar] [CrossRef]
- Siemens Digital Industries Software. Simcenter STAR-CCM+ User Guide, version 2021.1. In Adaptive Mesh Refinement for Overset Meshes; Siemens: Berlin, Germany, 2021; pp. 3067–3070. [Google Scholar]
- ANVISA. Resolução n. 9, de 16 de Janeiro de 2003; Technical Report; Ministério da Saúde: Brasília, Brazil, 2003.
- ABNT. NBR-7256, Tratamento de ar em Estabelecimento Assistenciais de Saúde (EAS): Requisitos Para Projetos e Execução das Instalações; Associação Brasileira de Normas técnicas: Rio de Janeiro, Brazil, 2005. [Google Scholar]
- ABNT. Instalação de Ar-Condicionado—Sistemas Centrais e Unitários—Parte 2: Parâmetros de Conforto Térmico; Technical Report; Brazilian Technical Standards Association: Rio de Janeiro, Brazil, 2008. [Google Scholar]
- ABNT. Instalação de Ar-Condicionado—Sistemas Centrais e Unitários—Parte 3: Qualidade do Ar Interior; Technical Report; Brazilian Technical Standards Association: Rio de Janeiro, Brazil, 2008. [Google Scholar]
- NC. Specification for Filters, Air (HVAC). 2017. Available online: https://files.nc.gov/ncdoa/pandc/Documents/BidAttachments/s4130-1.pdf (accessed on 10 February 2022).
- ASHRAE. Handbook—Heating, Ventilating and Air Conditioning Systems; American Society of Heating, Refrigerating and Air Conditioning Engineers: New York, NY, USA, 2008. [Google Scholar]
- ANSI/ASHRAE Standard 52.2-2017; Method of Testing General Ventilation Air-Cleaning Devices for Removal Efficiency by Particle Size. ASHRAE: New York, NY, USA, 2017.
- Ma, Y.; Hu, X.; Wu, D. The permeability of glass fiber mat and its influence on the filling time of RTM process. In Proceedings of the Eleventh International Conference on Composite Materials, Gold Coast, QLD, Australia, 14–18 July 1997; pp. 14–18. [Google Scholar]
- ABNT. NBR-16101, Filtros para Partículas em Suspensão no ar—Terminação da Eficiência para Filtros Grossos; Médios e Finos: São Paulo, Brazil, 2012. [Google Scholar]
- Date, A.W. Introduction to Computational Fluid Dynamics; Cambridge University Press: Cambridge, UK, 2005. [Google Scholar]
- Mase, G.T.; Smelser, R.E.; Mase, G.E. Continuum Mechanics for Engineers; CRC Press: Boca Raton, FL, USA, 2009. [Google Scholar]
- Zhong, W.; Ji, X.; Li, C.; Fang, J.; Liu, F. Determination of permeability and inertial coefficients of sintered metal porous media using an isothermal chamber. Appl. Sci. 2018, 8, 1670. [Google Scholar] [CrossRef]
- Belforte, G.; Raparelli, T.; Viktorov, V.; Trivella, A. Permeability and inertial coefficients of porous media for air bearing feeding systems. J. Tribol. 2007, 124, 705–711. [Google Scholar] [CrossRef]
- Malalasekera, W.; Versteeg, H. An Introduction to Computational Fluid Dynamics: The Finite Volume Method; Prentice Hall: Harlow, UK, 2007; p. 1995. [Google Scholar]
- Wang, S.K.; Wang, S.K. Handbook of Air Conditioning and Refrigeration; McGraw-Hill: New York, NY, USA, 2000; Volume 49. [Google Scholar]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MERV | Efficiency | Typical Contaminant | Applications | Filter Class |
|---|---|---|---|---|
| 20 | Not Applied | ≤ diameter | Clean rooms | HEPA/ULPA |
| 19 | Not Applied | Viruses | Radioactive materials | Effic. ≤ 99.999% |
| 18 | Not Applied | Sea Salt | Pharmaceutical industries | Types A, C, D and F |
| 17 | Not Applied | Combustion fumes | Surgical centers | Not applied |
| 16 | Not Applied | to | Hospitals | Bag filters |
| 15 | >95% | All bacteria | General surgeries | Not applied |
| 14 | 90 to 95% | Cigarette smoke | Smokers’ lounges | Not applied |
| 13 | 80 a 90% | Cooking oil/paint | Commercial buildings | Not applied |
| 12 | 70 to 75% | to | Residences (top conditions for air circulation) | Filter bags |
| 11 | 60 to 65% | Legionella | Commercial buildings | Not applied |
| 10 | 50 to 55% | Lead/charcoal dust | Hospital laboratories | Not applied |
| 9 | 40 to 45% | Car emissions | Not applied | Not applied |
| 8 | 30 to 35% | to | Commercial buildings | Pleated filters |
| 7 | 25 to 30% | Mold | Residences | Not applied |
| 6 | <20% | Spores | Industrial places | Disposable filters |
| 5 | <20% | Cement | Paint booth | Not applied |
| 4 | <20% | > | Minimal filtration | Disposable filters |
| 3 | <20% | Spanish moss | Residences | Washable filters |
| 2 | <20% | Paint spray powders | Window air conditioners | Electrostatics |
| 1 | <20% | Sanding powders | Not applied | Not applied |
| Efficiency Level | Lower |  | Higher | ||||||
|---|---|---|---|---|---|---|---|---|---|
| NBR 16101/2012 | G1 | G2 | G3 | G4 | M5 | M6 | F7 | F8 | F9 |
| MERV 62.1 | 1 | 2–4 | 5–6 | 7–8 | 9–10 | 11–12 | 13 | 14 | 15 |
| NBR 7256/2005 applications | Not applied | Not applied | Image examination room | Outpatient care | Not applied | Not applied | Pneumology procedure room | Low-risk operating room | High-risk operating room |
| Risk level | - | - | 1 | 1 | - | - | 1 | 2 | 3 |
| Boundary | Property | BC | Value |
|---|---|---|---|
| Intake grilles | Velocity | Dirichlet | |
| Intake grilles | Temperature | Dirichlet | |
| Exhaust grilles | Pressure | Dirichlet | |
| Doors and walls | Velocity (no-slip) | Dirichlet | |
| Doors and walls | Temperature (no-flux) | Neumann |
| h | |||
|---|---|---|---|
| 0.025 m | 57,121,034 | 0.1511 | 75.33 |
| 0.050 m | 13,609,162 | 0.1523 | 75.83 |
| 0.100 m | 7,319,700 | 0.1514 | 75.39 |
| 0.200 m | 6,552,371 | 0.1572 | 75.41 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Araújo Alves, C.G.; Junior, J.T.C.; Da Silva Neto, F.B.; Anjos, G.R.; Dos Santos, M.D.; Peixoto de Oliveira, G. Indoor Airflow Dynamics in Compartmentalized Pneumology Units Equipped with Variable-Thickness MERV-13 Filters. Buildings 2023, 13, 1072. https://doi.org/10.3390/buildings13041072
Araújo Alves CG, Junior JTC, Da Silva Neto FB, Anjos GR, Dos Santos MD, Peixoto de Oliveira G. Indoor Airflow Dynamics in Compartmentalized Pneumology Units Equipped with Variable-Thickness MERV-13 Filters. Buildings. 2023; 13(4):1072. https://doi.org/10.3390/buildings13041072
Chicago/Turabian StyleAraújo Alves, Camilo Gustavo, José Tadeu C. Junior, Francisco Bernardino Da Silva Neto, Gustavo R. Anjos, Moisés Dantas Dos Santos, and Gustavo Peixoto de Oliveira. 2023. "Indoor Airflow Dynamics in Compartmentalized Pneumology Units Equipped with Variable-Thickness MERV-13 Filters" Buildings 13, no. 4: 1072. https://doi.org/10.3390/buildings13041072
APA StyleAraújo Alves, C. G., Junior, J. T. C., Da Silva Neto, F. B., Anjos, G. R., Dos Santos, M. D., & Peixoto de Oliveira, G. (2023). Indoor Airflow Dynamics in Compartmentalized Pneumology Units Equipped with Variable-Thickness MERV-13 Filters. Buildings, 13(4), 1072. https://doi.org/10.3390/buildings13041072