


Effects of Different Nocturnal Lighting Stimuli on Melatonin, Sleep and Cognitive Performance of Workers in Confined Spaces


Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Conditions
2.2. Participant Selection
2.3. Experimental Protocol
2.4. Testing Methods
2.4.1. Collection and Processing of Saliva Melatonin Samples
2.4.2. Evaluation of Sleep Quality
2.4.3. Cognitive Ability Test
2.4.4. Karolinska Sleepiness Scale (KSS)
2.5. Data Analysis
3. Results
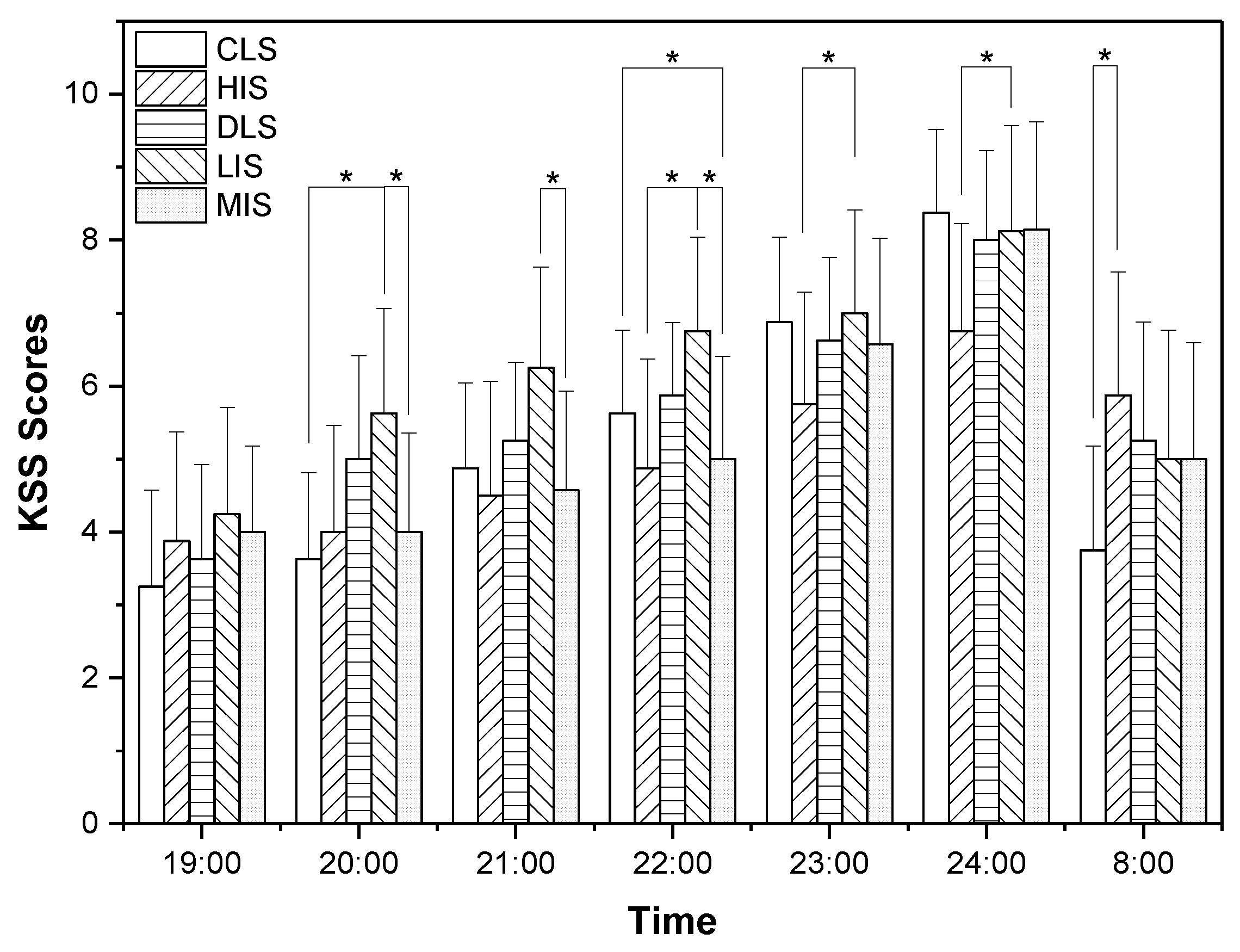
3.1. Evaluation of Subjective Sleepiness (KSS Scores)
3.2. Analysis of Melatonin
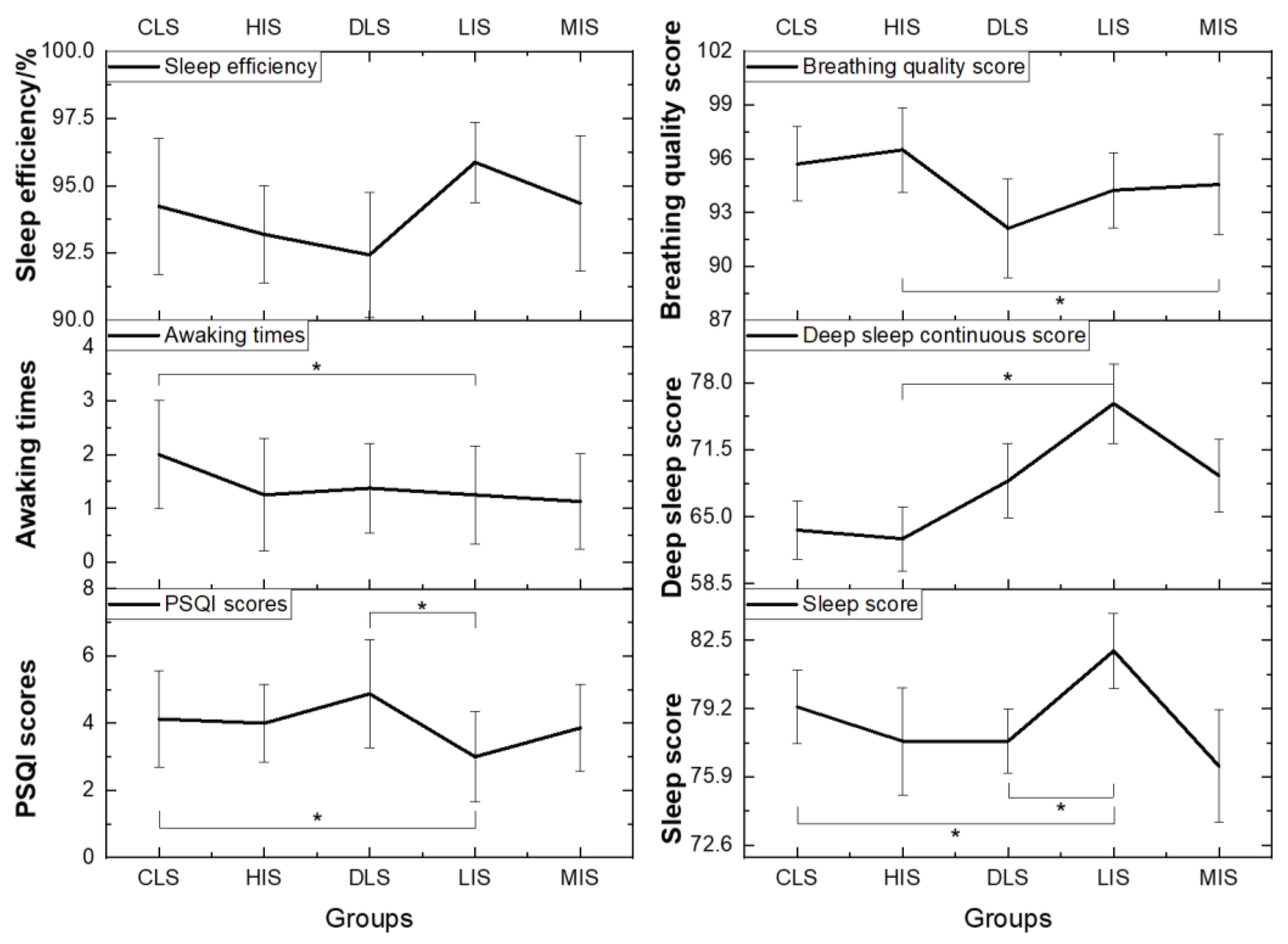
3.3. Evaluation of Sleep Quality
3.4. PVT Test
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lu, Y.; Yin, P.; Wang, J.; Yang, Y.; Li, F.; Yuan, H.; Li, S.; Long, Z.; Zhou, M. Light at night and cause-specific mortality risk in Mainland China: A nationwide observational study. BMC Med. 2023, 21, 95. [Google Scholar] [CrossRef]
- Lai, K.Y.; Sarkar, C.; Ni, M.Y.; Cheung, L.W.T.; Gallacher, J.; Webster, C. Exposure to light at night (LAN) and risk of breast cancer: A systematic review and meta-analysis. Sci. Total Environ. 2021, 762, 143159. [Google Scholar] [CrossRef]
- Stevens, R.G.; Hansen, J.; Costa, G.; Haus, E.; Kauppinen, T.; Aronson, K.J.; Castaño-Vinyals, G.; Davis, S.; Frings-Dresen, M.H.; Fritschi, L. Considerations of circadian impact for defining ‘shift work’in cancer studies: IARC Working Group Report. Occup. Environ. Med. 2011, 68, 154–162. [Google Scholar] [CrossRef]
- Haus, E.L.; Smolensky, M.H. Shift work and cancer risk: Potential mechanistic roles of circadian disruption, light at night, and sleep deprivation. Sleep Med. Rev. 2013, 17, 273–284. [Google Scholar] [CrossRef]
- Sun, S.; Cao, W.; Ge, Y.; Ran, J.; Sun, F.; Zeng, Q.; Guo, M.; Huang, J.; Lee, R.S.-Y.; Tian, L. Outdoor light at night and risk of coronary heart disease among older adults: A prospective cohort study. Eur. Heart J. 2021, 42, 822–830. [Google Scholar] [CrossRef] [PubMed]
- Stefani, O.; Cajochen, C. Should we re-think regulations and standards for lighting at workplaces? A practice review on existing lighting recommendations. Front. Psychiatry 2021, 12, 652161. [Google Scholar] [CrossRef] [PubMed]
- CIE S 017/E:2020; ILV: International Lighting Vocabulary, 2nd ed. CIE Central Bureau: Vienna, Austria, 2020.
- Lowden, A.; Kecklund, G. Considerations on how to light the night-shift. Light. Res. Technol. 2021, 53, 437–452. [Google Scholar] [CrossRef]
- Hou, D.; He, S.; Dai, C.; Chen, S.; Chen, H.; Lin, Y. Lighting scheme recommendation for interior workplace to adjust the phase-advance jet lag. Build. Environ. 2021, 198, 107913. [Google Scholar] [CrossRef]
- Houser, K.; Boyce, P.; Zeitzer, J.; Herf, M. Human-centric lighting: Myth, magic or metaphor? Light. Res. Technol. 2021, 53, 97–118. [Google Scholar] [CrossRef]
- Wang, T.; Li, J.; Wang, Y.; Dai, S.; Shao, R.; Hao, L. Active interventions of dynamic lighting on human circadian rhythm and sleep quality in confined spaces. Build. Environ. 2022, 226, 109766. [Google Scholar] [CrossRef]
- Vethe, D.; Scott, J.; Engstrøm, M.; Salvesen, Ø.; Sand, T.; Olsen, A.; Morken, G.; Heglum, H.S.; Kjørstad, K.; Faaland, P.M.; et al. The evening light environment in hospitals can be designed to produce less disruptive effects on the circadian system and improve sleep. Sleep 2021, 44, 194. [Google Scholar] [CrossRef]
- Berson, D.M.; Dunn, F.A.; Takao, M. Phototransduction by retinal ganglion cells that set the circadian clock. Science 2002, 295, 1070–1073. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, M.; Din, N.S.B.M.; Tharumalay, R.D.; Che Din, N.; Ibrahim, N.; Amit, N.; Farah, N.M.; Osman, R.A.; Abdul Hamid, M.F.; Ibrahim, I.A. The effects of circadian rhythm disruption on mental health and physiological responses among shift workers and general population. Int. J. Environ. Res. Public Health 2020, 17, 7156. [Google Scholar] [CrossRef] [PubMed]
- Gou, Z.; Gou, B.; Liao, W.; Bao, Y.; Deng, Y. Integrated lighting ergonomics: A review on the association between non-visual effects of light and ergonomics in the enclosed cabins. Build. Environ. 2023, 243, 110616. [Google Scholar] [CrossRef]
- Khalsa, S.B.S.; Jewett, M.E.; Cajochen, C.; Czeisler, C.A. A phase response curve to single bright light pulses in human subjects. J. Physiol. 2003, 549, 945–952. [Google Scholar] [CrossRef] [PubMed]
- Minors, D.S.; Waterhouse, J.M.; Wirz-Justice, A. A human phase-response curve to light. Neurosci. Lett. 1991, 133, 36–40. [Google Scholar] [CrossRef]
- Gabel, V.; Maire, M.; Reichert, C.F.; Chellappa, S.L.; Schmidt, C.; Hommes, V.; Viola, A.U.; Cajochen, C. Effects of artificial dawn and morning blue light on daytime cognitive performance, well-being, cortisol and melatonin levels. Chronobiol. Int. 2013, 30, 988–997. [Google Scholar] [CrossRef]
- Souman, J.L.; Tinga, A.M.; Te Pas, S.F.; Van Ee, R.; Vlaskamp, B.N. Acute alerting effects of light: A systematic literature review. Behav. Brain Res. 2018, 337, 228–239. [Google Scholar] [CrossRef]
- Vandewalle, G.; Dijk, D.-J. Neuroimaging the Effects of Light on Non-Visual Brain Functions. 2012, pp. 171–178. Available online: https://orbi.uliege.be/bitstream/2268/149604/1/Vandewalle_Dijk_2013_book%20chapter.pdf (accessed on 7 November 2012).
- Mårtensson, B.; Pettersson, A.; Berglund, L.; Ekselius, L. Bright white light therapy in depression: A critical review of the evidence. J. Affect. Disord. 2015, 182, 1–7. [Google Scholar] [CrossRef]
- Griepentrog, J.E.; Labiner, H.E.; Gunn, S.R.; Rosengart, M.R. Bright environmental light improves the sleepiness of nightshift ICU nurses. Crit. Care 2018, 22, 295. [Google Scholar] [CrossRef]
- Figueiro, M.; Nagare, R.; Price, L. Non-visual effects of light: How to use light to promote circadian entrainment and elicit alertness. Light. Res. Technol. 2018, 50, 38–62. [Google Scholar] [CrossRef] [PubMed]
- Figueiro, M.; Steverson, B.; Heerwagen, J.; Yucel, R.; Roohan, C.; Sahin, L.; Kampschroer, K.; Rea, M. Light, entrainment and alertness: A case study in offices. Light. Res. Technol. 2020, 52, 736–750. [Google Scholar] [CrossRef]
- Stefani, O.; Freyburger, M.; Veitz, S.; Basishvili, T.; Meyer, M.; Weibel, J.; Kobayashi, K.; Shirakawa, Y.; Cajochen, C. Changing color and intensity of LED lighting across the day impacts on circadian melatonin rhythms and sleep in healthy men. J. Pineal Res. 2021, 70, e12714. [Google Scholar] [CrossRef]
- Ru, T.; Kompier, M.E.; Chen, Q.; Zhou, G.; Smolders, K.C. Temporal tuning of illuminance and spectrum: Effect of a full-day dynamic lighting pattern on well-being, performance and sleep in simulated office environment. Build. Environ. 2023, 228, 109842. [Google Scholar] [CrossRef]
- CIE S 026/E:2018; CIE System for Metrology of Optical Radiation for ipRGC-Influenced Responses to Light. CIE Central Bureau: Vienna, Austria, 2018.
- Schlangen, L.J. CIE Position Statement on Non-Visual Effects of Light: Recommending Proper Light at the Proper Time; CIE Central Bureau: Vienna, Austria, 2019. [Google Scholar]
- WELL-Building-Standard, v2 Pilot. Circadian Lighting Design. 2022. Available online: https://v2.wellcertified.com/en/wellv2/light/feature/3 (accessed on 15 June 2022).
- Brown, T.; Brainard, G.; Cajochen, C.; Czeisler, C.; Hanifin, J.; Lockley, S.; Lucas, R.; Munch, M.; O’Hagan, J.; Peirson, S. Recommendations for Healthy Daytime, Evening, and Night-Time Indoor Light Exposure. 2020. Available online: https://www.preprints.org/manuscript/202012.0037/v1 (accessed on 1 December 2020).
- GB 50034-2013; Ministry-of-Housing-and-Urban-Rural-Development, Standard for Lighting Design of Buildings. China Architecture and Building Press: Beijing, China, 2013.
- Figueiro, M. A working threshold for acute nocturnal melatonin suppression from “white” light sources used in architectural applications. J. Carcinog. Mutagen. 2013, 4, 150. [Google Scholar]
- Rea, M.S.; Figueiro, M.G.; Bierman, A.; Bullough, J.D. Circadian light. J. Circadian Rhythm. 2010, 8, 1–10. [Google Scholar] [CrossRef]
- Liu, H.; Yao, Z.; Fu, Y. Research status and development trend of bio-regenerative life support system for deep space exploration. J. Deep Space Explor. 2020, 7, 489. [Google Scholar]
- Tafforin, C. The Mars-500 crew in daily life activities: An ethological study. Acta Astronaut. 2013, 91, 69–76. [Google Scholar] [CrossRef]
- Meng, C.; Wang, W.; Hao, Z.; Liu, H. Investigation on the influence of isolated environment on human psychological and physiological health. Sci. Total Environ. 2020, 716, 136972. [Google Scholar] [CrossRef]
- Lowden, A.; Akerstedt, T. Assessment of a new dynamic light regimen in a nuclear power control room without windows on quickly rotating shiftworkers—Effects on health, wakefulness, and circadian alignment: A pilot study. Chronobiol. Int. 2012, 29, 641–649. [Google Scholar] [CrossRef]
- Nie, J.; Zhou, T.; Chen, Z.; Dang, W.; Jiao, F.; Zhan, J.; Chen, Y.; Chen, Y.; Pan, Z.; Kang, X.; et al. Investigation on entraining and enhancing human circadian rhythm in closed environments using daylight-like LED mixed lighting. Sci. Total Environ. 2020, 732, 139334. [Google Scholar] [CrossRef]
- Zhang, Z.; Henzmann, S.; Hugli, G.; Qi, M.; Chen, W.; Lu, C.; Khatami, R. Validation of wearable sleep monitoring device based on cardiopulmonary coupling and accelerometer with comparison to polysomnography in adults. In Proceedings of the 4th Congress of the European Academy of Neurology, Lisbon, Portugal, 16–19 June 2018; European Journal of Neurology: Lisbon, Portugal, 2018; p. 385. [Google Scholar]
- Carpenter, J.S.; Andrykowski, M.A. Psychometric evaluation of the Pittsburgh sleep quality index. J. Psychosom. Res. 1998, 45, 5–13. [Google Scholar] [CrossRef]
- Thomann, J.; Baumann, C.R.; Landolt, H.-P.; Werth, E. Psychomotor vigilance task demonstrates impaired vigilance in disorders with excessive daytime sleepiness. J. Clin. Sleep Med. 2014, 10, 1019–1024. [Google Scholar] [CrossRef] [PubMed]
- Basner, M.; Mollicone, D.; Dinges, D.F. Validity and sensitivity of a brief psychomotor vigilance test (PVT-B) to total and partial sleep deprivation. Acta Astronaut. 2011, 69, 949–959. [Google Scholar] [CrossRef]
- Kaida, K.; Takahashi, M.; Åkerstedt, T.; Nakata, A.; Otsuka, Y.; Haratani, T.; Fukasawa, K. Validation of the Karolinska sleepiness scale against performance and EEG variables. Clin. Neurophysiol. 2006, 117, 1574–1581. [Google Scholar] [CrossRef]
- Rajaratnam, S.M.; Middleton, B.; Stone, B.M.; Arendt, J.; Dijk, D.J. Melatonin advances the circadian timing of EEG sleep and directly facilitates sleep without altering its duration in extended sleep opportunities in humans. J. Physiol. 2004, 561, 339–351. [Google Scholar] [CrossRef] [PubMed]
- Sletten, T.L.; Magee, M.; Murray, J.M.; Gordon, C.J.; Lovato, N.; Kennaway, D.J.; Gwini, S.M.; Bartlett, D.J.; Lockley, S.W.; Lack, L.C. Efficacy of melatonin with behavioural sleep-wake scheduling for delayed sleep-wake phase disorder: A double-blind, randomised clinical trial. PLoS Med. 2018, 15, e1002587. [Google Scholar] [CrossRef]
- Falcón, J.; Torriglia, A.; Attia, D.; Viénot, F.; Gronfier, C.; Behar-Cohen, F.; Martinsons, C.; Hicks, D. Exposure to artificial light at night and the consequences for flora, fauna, and ecosystems. Front. Neurosci. 2020, 14, 1183. [Google Scholar] [CrossRef] [PubMed]
- Gooley, J.J.; Chamberlain, K.; Smith, K.A.; Khalsa, S.B.S.; Rajaratnam, S.M.; Van Reen, E.; Zeitzer, J.M.; Czeisler, C.A.; Lockley, S.W. Exposure to room light before bedtime suppresses melatonin onset and shortens melatonin duration in humans. J. Clin. Endocrinol. Metab. 2011, 96, E463–E472. [Google Scholar] [CrossRef]
- Dumont, M.; Beaulieu, C. Light exposure in the natural environment: Relevance to mood and sleep disorders. Sleep Med. 2007, 8, 557–565. [Google Scholar] [CrossRef]
- Xiao, H.; Cai, H.; Li, X. Non-visual effects of indoor light environment on humans: A review✰. Physiol. Behav. 2021, 228, 113195. [Google Scholar] [CrossRef] [PubMed]
- Khademagha, P.; Aries, M.; Rosemann, A.; Van Loenen, E. Implementing non-image-forming effects of light in the built environment: A review on what we need. Build. Environ. 2016, 108, 263–272. [Google Scholar] [CrossRef]
- Rea, M.S.; Nagare, R.; Figueiro, M.G. Relative light sensitivities of four retinal hemi-fields for suppressing the synthesis of melatonin at night. Neurobiol. Sleep Circadian Rhythm. 2021, 10, 100066. [Google Scholar] [CrossRef]
- Glickman, G.; Hanifin, J.P.; Rollag, M.D.; Wang, J.; Cooper, H.; Brainard, G.C. Inferior retinal light exposure is more effective than superior retinal exposure in suppressing melatonin in humans. J. Biol. Rhythm. 2003, 18, 71–79. [Google Scholar] [CrossRef]
- Lasko, T.A.; Kripke, D.F.; Elliot, J.A. Melatonin suppression by illumination of upper and lower visual fields. J. Biol. Rhythm. 1999, 14, 122–125. [Google Scholar] [CrossRef] [PubMed]
- Figueiro, M.; Kalsher, M.; Steverson, B.; Heerwagen, J.; Kampschroer, K.; Rea, M. Circadian-effective light and its impact on alertness in office workers. Light. Res. Technol. 2019, 51, 171–183. [Google Scholar] [CrossRef]
- Smolders, K.; De Kort, Y.; van den Berg, S.M. Daytime light exposure and feelings of vitality: Results of a field study during regular weekdays. J. Environ. Psychol. 2013, 36, 270–279. [Google Scholar] [CrossRef]
- Hubalek, S.; Brink, M.; Schierz, C. Office workers’ daily exposure to light and its influence on sleep quality and mood. Light. Res. Technol. 2010, 42, 33–50. [Google Scholar] [CrossRef]
- Hsu, Z.Y.; Moskowitz, D.; Young, S.N. The influence of light administration on interpersonal behavior and affect in people with mild to moderate seasonality. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2014, 48, 92–101. [Google Scholar] [CrossRef]
- Revell, V.L.; Skene, D.J. Light-induced melatonin suppression in humans with polychromatic and monochromatic light. Chronobiol. Int. 2007, 24, 1125–1137. [Google Scholar] [CrossRef]
- Chellappa, S.L.; Steiner, R.; Blattner, P.; Oelhafen, P.; Götz, T.; Cajochen, C. Non-visual effects of light on melatonin, alertness and cognitive performance: Can blue-enriched light keep us alert? PLoS ONE 2011, 6, e16429. [Google Scholar] [CrossRef] [PubMed]
- Chellappa, S.L.; Viola, A.U.; Schmidt, C.; Bachmann, V.; Gabel, V.; Maire, M.; Reichert, C.F.; Valomon, A.; Landolt, H.-P.; Cajochen, C. Light modulation of human sleep depends on a polymorphism in the clock gene Period3. Behav. Brain Res. 2014, 271, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Knaier, R.; Schäfer, J.; Rossmeissl, A.; Klenk, C.; Hanssen, H.; Höchsmann, C.; Cajochen, C.; Schmidt-Trucksäss, A. Prime time light exposures do not seem to improve maximal physical performance in male elite athletes, but enhance end-spurt performance. Front. Physiol. 2017, 8, 264. [Google Scholar] [CrossRef] [PubMed]
- Giménez, M.C.; Stefani, O.; Cajochen, C.; Lang, D.; Deuring, G.; Schlangen, L.J. Predicting melatonin suppression by light in humans: Unifying photoreceptor-based equivalent daylight illuminances, spectral composition, timing and duration of light exposure. J. Pineal Res. 2022, 72, e12786. [Google Scholar] [CrossRef]
- Pandi-Perumal, S.R.; Smits, M.; Spence, W.; Srinivasan, V.; Cardinali, D.P.; Lowe, A.D.; Kayumov, L. Dim light melatonin onset (DLMO): A tool for the analysis of circadian phase in human sleep and chronobiological disorders. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2007, 31, 1–11. [Google Scholar] [CrossRef]
- Brown, T.M. Melanopic illuminance defines the magnitude of human circadian light responses under a wide range of conditions. J. Pineal Res. 2020, 69, e12655. [Google Scholar] [CrossRef]
- Mills, J. Circadian rhythms during and after three months in solitude underground. J. Physiol. 1964, 174, 217–231. [Google Scholar] [CrossRef]
- Broadway, J.; Arendt, J.; Folkard, S. Bright light phase shifts the human melatonin rhythm during the Antarctic winter. Neurosci. Lett. 1987, 79, 185–189. [Google Scholar] [CrossRef]
- Höhn, C.; Schmid, S.R.; Plamberger, C.P.; Bothe, K.; Angerer, M.; Gruber, G.; Pletzer, B.; Hoedlmoser, K. Preliminary results: The impact of smartphone use and short-wavelength light during the evening on circadian rhythm, sleep and alertness. Clocks Sleep 2021, 3, 66–86. [Google Scholar] [CrossRef]
- Vethe, D.; Drews, H.J.; Scott, J.; Engstrøm, M.; Heglum, H.S.A.; Grønli, J.; Wisor, J.; Sand, T.; Lydersen, S.; Kjørstad, K. Evening light environments can be designed to consolidate and increase the duration of REM-sleep. Sci. Rep. 2022, 12, 8719. [Google Scholar] [CrossRef]
- Ricketts, E.J.; Joyce, D.S.; Rissman, A.J.; Burgess, H.J.; Colwell, C.S.; Lack, L.C.; Gradisar, M. Electric lighting, adolescent sleep and circadian outcomes, and recommendations for improving light health. Sleep Med. Rev. 2022, 64, 101667. [Google Scholar] [CrossRef]
- Sahin, L.; Figueiro, M. A 24-h lighting scheme to promote alertness and circadian entrainment in railroad dispatchers on rotating shifts: A field study. Light. Res. Technol. 2022, 54, 441–457. [Google Scholar] [CrossRef]
- Schledermann, K.; Bjørner, T.; West, A.; Hansen, T. Evaluation of staff’s perception of a circadian lighting system implemented in a hospital. Build. Environ. 2023, 242, 110488. [Google Scholar] [CrossRef]
- Van de Putte, E.; Kindt, S.; Bracke, P.; Stevens, M.; Vansteenkiste, M.; Vandevivere, L.; Ryckaert, W.R. The influence of integrative lighting on sleep and cognitive functioning of shift workers during the morning shift in an assembly plant. Appl. Ergon. 2022, 99, 103618. [Google Scholar] [CrossRef]
- Schlangen, L.J.; Price, L.L. The lighting environment, its metrology, and non-visual responses. Front. Neurol. 2021, 12, 624861. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Westland, S. Effect of long-wavelength light on electroencephalogram and subjective alertness. Light. Res. Technol. 2020, 52, 763–774. [Google Scholar] [CrossRef]
- Lin, J.; Westland, S.; Cheung, V. Effect of intensity of short-wavelength light on electroencephalogram and subjective alertness. Light. Res. Technol. 2020, 52, 413–422. [Google Scholar] [CrossRef]
- van Duijnhoven, J.; Aarts, M.; Rosemann, A.; Kort, H. Ambiguities regarding the relationship between office lighting and subjective alertness: An exploratory field study in a Dutch office landscape. Build. Environ. 2018, 142, 130–138. [Google Scholar] [CrossRef]
- Phillips, A.J.; Vidafar, P.; Burns, A.C.; McGlashan, E.M.; Anderson, C.; Rajaratnam, S.M.; Lockley, S.W.; Cain, S.W. High sensitivity and interindividual variability in the response of the human circadian system to evening light. Proc. Natl. Acad. Sci. USA 2019, 116, 12019–12024. [Google Scholar] [CrossRef]
- Daneault, V.; Dumont, M.; Massé, É.; Vandewalle, G.; Carrier, J. Light-sensitive brain pathways and aging. J. Physiol. Anthropol. 2016, 35, 9. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Light Scenes | CCT/K | Illuminance of Working Plane/lx | Vertical Illuminance at the Eyes/lx | Melanopic EDI/lx | Circadian Stimulus, CS |
|---|---|---|---|---|---|
| current lighting scene (CLS) | 6000 | 151.53 | 63.31 | 56.50 | 0.10 |
| high intervention scene (HIS) | 6000 | 3415.96 | 1255.80 | 1171.25 | 0.60 |
| design lighting scene (DLS) | 6000 | 333.34 | 129.85 | 124.10 | 0.20 |
| low intervention scene (LIS) | 2700 | 103.97 | 43.68 | 19.65 | 0.05 |
| medium intervention scene (MIS) | 6000 | 531.77 | 215.25 | 202.28 | 0.30 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, T.; Shao, R.; Hao, L. Effects of Different Nocturnal Lighting Stimuli on Melatonin, Sleep and Cognitive Performance of Workers in Confined Spaces. Buildings 2023, 13, 2112. https://doi.org/10.3390/buildings13082112
Wang T, Shao R, Hao L. Effects of Different Nocturnal Lighting Stimuli on Melatonin, Sleep and Cognitive Performance of Workers in Confined Spaces. Buildings. 2023; 13(8):2112. https://doi.org/10.3390/buildings13082112
Chicago/Turabian StyleWang, Tongyue, Rongdi Shao, and Luoxi Hao. 2023. "Effects of Different Nocturnal Lighting Stimuli on Melatonin, Sleep and Cognitive Performance of Workers in Confined Spaces" Buildings 13, no. 8: 2112. https://doi.org/10.3390/buildings13082112
APA StyleWang, T., Shao, R., & Hao, L. (2023). Effects of Different Nocturnal Lighting Stimuli on Melatonin, Sleep and Cognitive Performance of Workers in Confined Spaces. Buildings, 13(8), 2112. https://doi.org/10.3390/buildings13082112