Predictive Accuracy of COVID-19 World Health Organization (WHO) Severity Classification and Comparison with a Bayesian-Method-Based Severity Score (EPI-SCORE)

 , ,
, ,  , ,
, , 
Abstract
:1. Introduction
2. Results
2.1. Characteristics of Patients Following WHO Severity Classification
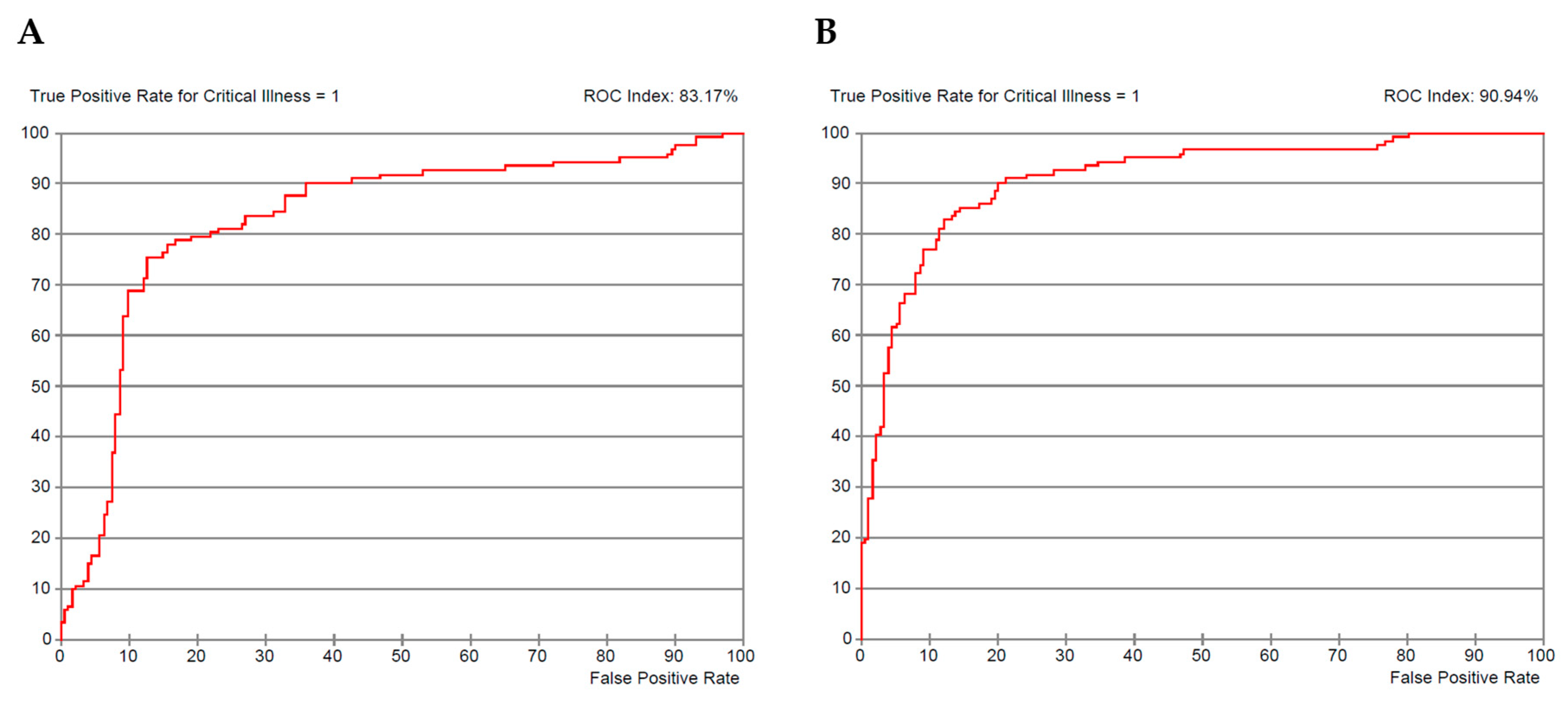
2.2. Bayesian Network Analysis and Score Modeling
3. Discussion
4. Materials and Methods
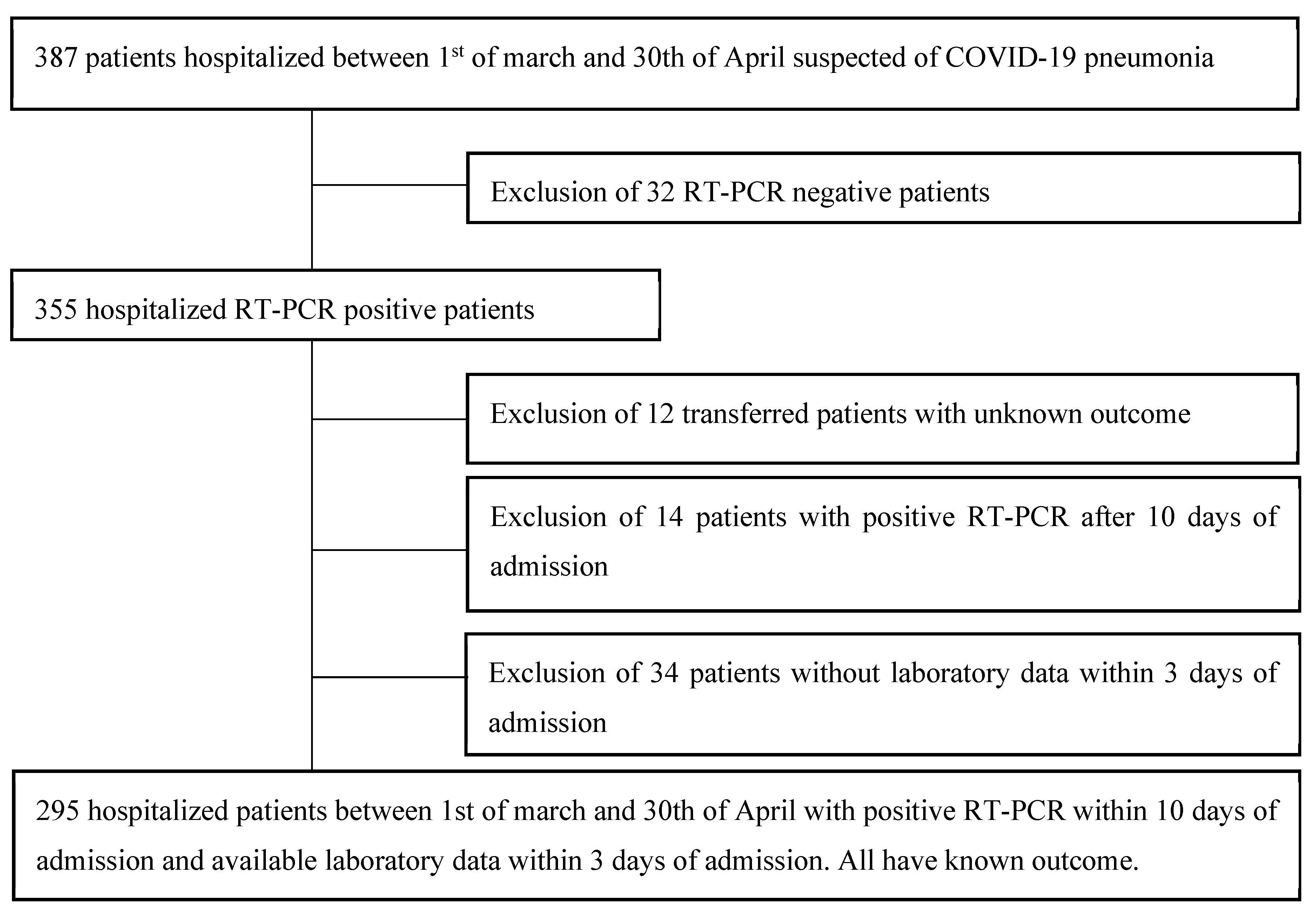
4.1. Study Population
4.2. Patients’ Management and Severity Classification
4.3. Data Collection
4.4. Conventional Statistical Analysis
4.5. Bayesian Network Analysis and Score Modeling
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Patients’ Characteristics According to Severity Classification following WHO-Guidelines
| Moderate (n = 125) | Severe (n = 69) | Critical (n = 101) | Total (n = 295) | p-Value | ||
| Demographic data | ||||||
| age | 72 (60; 83) | 75 (62; 86) | 72 (66; 82) | 73 (62; 83) | 0.377 | |
| female | 56a, b (44.8%) | 37b (53.6%) | 35a (34.7%) | 128 (43.4%) | 0.045 | |
| dead | 14a (11.2%) | 23b (33.3%) | 68c (67.3%) | 105 (35.6%) | 0.000 | |
| Critical Illness (dead or IMV) | 14a (11.2%) | 24b (34.8%) | 84c (83.2%) | 122 (41.4%) | 0.000 | |
| Institutionalized | 29 (23.8%) | 20 (29.4%) | 27 (26.7%) | 76 (26.1%) | 0.687 | |
| Symptoms | ||||||
| Fever | 76 (61.3%) | 48 (73.8%) | 72 (72.0%) | 196 (67.8%) | 0.116 | |
| Cough | 51a (41.5%) | 47b (72.3%) | 59b (59.0%) | 157 (54.5%) | 0.000 | |
| Dyspnea | 49a (40.2%) | 45b (71.4%) | 70b (70.7%) | 164 (57.7%) | 0.000 | |
| Thoracic pain | 12 (9.8%) | 2 (3.2%) | 4 (4.1%) | 18 (6.4%) | 0.114 | |
| Dysgeusia or Anosmia | 6 (5.0%) | 5 (7.9%) | 7 (7.2%) | 18 (6.4%) | 0.679 | |
| Myalgia | 17 (14.0%) | 13 (20.6%) | 22 (22.7%) | 52 (18.5%) | 0.234 | |
| Headache | 6 (5.0%) | 9 (14.3%) | 10 (10.3%) | 25 (8.9%) | 0.090 | |
| Nausea | 14 (11.5%) | 8 (12.9%) | 8 (8.2%) | 30 (10.7%) | 0.605 | |
| Vomiting | 15a (12.2%) | 5a, b (7.8%) | 2b (2.0%) | 22 (7.7%) | 0.017 | |
| Abdominal pain | 15 (12.3%) | 3 (4.7%) | 5 (5.1%) | 23 (8.1%) | 0.077 | |
| Confusion | 19 (15.4%) | 9 (13.8%) | 18 (18.0%) | 46 (16.0%) | 0.759 | |
| Fall | 22 (17.9%) | 5 (7.6%) | 12 (12.1%) | 39 (13.5%) | 0.125 | |
| Diarrhoea | 15 (12.3%) | 5 (7.8%) | 13 (13.0%) | 33 (11.5%) | 0.563 | |
| Chonic conditions | ||||||
| Mininum of one comorbidity | 111 (88.8%) | 60 (87.0%) | 95 (94.1%) | 266 (90.2%) | 0.248 | |
| History of heart infarction | 24 (19.4%) | 8 (11.8%) | 19 (18.8%) | 51 (17.4%) | 0.373 | |
| History of heart failure | 18 (14.4%) | 11 (15.9%) | 21 (20.8%) | 50 (16.9%) | 0.430 | |
| History of peripheric arterial disease | 12 (9.6%) | 6 (8.7%) | 11 (10.9%) | 29 (9.8%) | 0.889 | |
| History of stroke or transient ischemic attack | 10 (8.0%) | 10 (14.5%) | 18 (17.8%) | 38 (12.9%) | 0.082 | |
| History of cerebro-vascular disease | 43 (34.4%) | 25 (36.2%) | 43 (42.6%) | 111 (37.6%) | 0.435 | |
| Dementia | 18 (14.4%) | 13 (19.1%) | 21 (20.8%) | 52 (17.7%) | 0.429 | |
| COPD | 13 (10.4%) | 14 (20.9%) | 13 (12.9%) | 40 (13.7%) | 0.125 | |
| Asthma | 12 (9.6%) | 8 (11.9%) | 7 (6.9%) | 27 (9.2%) | 0.536 | |
| Chronic liver disease | 4a (3.2%) | 9b (13.4%) | 4a, b (4.0%) | 17 (5.8%) | 0.009 | |
| Diabetes (type I or II) | 41 (32.8%) | 19 (27.5%) | 33 (32.7%) | 93 (31.5%) | 0.717 | |
| Dyslipidemia | 42 (33.6%) | 29 (42.6%) | 47 (46.5%) | 118 (40.1%) | 0.127 | |
| Hypertension | 75 (60.0%) | 48 (70.6%) | 68 (67.3%) | 191 (65.0%) | 0.280 | |
| Past or active smoker | 25 (22.1%) | 11 (17.7%) | 26 (27.7%) | 62 (23.0%) | 0.339 | |
| Chronic kidney failure | 31 (24.8%) | 15 (21.7%) | 24 (23.8%) | 70 (23.7%) | 0.891 | |
| CHARLSON | 4 (2; 6) | 5 (3; 6) | 5 (3; 6) | 5.0 (2.0; 6.0) | 0.259 | |
| Chronic medications | ||||||
| Immunosuppresive treatment | 6 (4.9%) | 6 (8.7%) | 9 (8.9%) | 21 (7.2%) | 0.433 | |
| Oral antidiabetics | 26 (20.8%) | 9 (13.0%) | 23 (22.8%) | 58 (19.7%) | 0.268 | |
| Insuline | 17 (13.6%) | 6 (8.7%) | 15 (14.9%) | 38 (12.9%) | 0.476 | |
| Antiplatelet therapy | 39 (31.2%) | 19 (27.5%) | 43 (42.6%) | 101 (34.2%) | 0.082 | |
| Anticoagulation therapy | 26 (20.8%) | 17 (24.6%) | 20 (19.8%) | 63 (21.4%) | 0.737 | |
| ACE inhibitor | 16a (12.8%) | 15a, b (21.7%) | 28b (27.7%) | 59 (20.0%) | 0.019 | |
| Sartan | 17 (13.6%) | 6 (9.0%) | 12 (11.9%) | 35 (11.9%) | 0.639 | |
| Admission vitals | ||||||
| Temperature (℃) | 37.2a (36.4; 38) | 37.5a, b (36.7; 38.2) | 37.8 b (36.8; 38.3) | 37.5 (36.6; 38.2) | 0.044 | |
| Heart rate (/min) | 90 (78; 102) | 87.5 (75; 102) | 91 (80; 100) | 90 (78; 101) | 0.751 | |
| Systolic blood pressure (mmHg) | 136.5 (120; 150) | 135.5 (117; 154) | 130.5 (118; 152) | 133 (120; 150) | 0.740 | |
| Diastolic blood pressure (mmHg) | 76 (70; 87) | 75 (66; 86) | 73 (65; 85) | 75 (67; 86) | 0.263 | |
| Need of oxygen at admission | 0a (0%) | 31b (44.9%) | 31b (30.7%) | 62 (21%) | 0.000 | |
| Pulse oxymetry | 95a (93; 97) | 89b (88; 94) | 91b (85.5; 94) | 93 (90; 96) | 0.000 | |
| Arterial blood gas analysis | ||||||
| pH | 7.48 (7.44; 7.50) | 7.47 (7.41; 7.53) | 7.47 (7.43; 7.50) | 7.47 (7.43; 7.50) | 0.844 | |
| paCO2 (mmHg) | 33 (30; 37) | 35 (31; 43) | 34 (29; 37) | 34 (30; 38) | 0.120 | |
| paO2 (mmHg) | 67 a (60; 74) | 64 a, b (54; 72) | 61b (54; 70) | 64 (56; 73) | 0.030 | |
| Bicarbonate (mmol/ L) | 25.5a, b (22.8; 27.2) | 26.3a (23.5; 30.1) | 24.0b (21.3; 27.1) | 25.3 (22.5; 27.2) | 0.014 | |
| Lactates (mmol/L) | 1.2 (0.8; 1.6) | 1.4 (0.9; 2.2) | 1.4 (1.0; 2.0) | 1.3 (0.9; 1.9) | 0.136 | |
| Laboratory work-up | C-reactive protein mg/L | 61.7a (23.8; 105.8) | 90.7b (45.5; 142.3) | 92.8b (53.4; 153.1) | 81.3 (39.4; 132.8) | 0.001 |
| Hemoglobin g/dL | 13.5 (11.9; 14.9) | 13.6 (12.7; 14.7) | 13.5 (12,0; 15,0) | 13,6 (12,2; 14,8) | 0,843 | |
| Platelets × 1000/mm3 | 222 (160; 290) | 203 (147; 263) | 191 (154; 251) | 204 (154; 268) | 0.110 | |
| White blood cell count × 1000/mm3 | 7.2 (4.7; 10.5) | 7.0 (5.8; 9.9) | 6.8 (5.4; 8.3) | 7.0 (5.2; 9.4) | 0.281 | |
| Neutrophiles × 1000/ mm3 | 5.7 (3.4; 8.1) | 5.2 (4.3; 8.4) | 5.5 (3.9; 6.9) | 5.5 (3.7; 7.5) | 0.554 | |
| Lymphocytes × 1000/mm3 | 0.9a (0.7; 1.2) | 0.8a, b (0.5; 1.2) | 0.7b (0.5; 1.1) | 0.8 (0.6; 1.2) | 0.033 | |
| Neutrophiles/lymphocytes | 6.3 (3.2; 10.3) | 7.2 (3.7; 14.3) | 6.6 (3.8; 11.1) | 6.8 (3.6; 11.7) | 0.275 | |
| Urea mg/dL | 40 (27; 58) | 41 (26; 78) | 47 (34; 75) | 43 (29; 67) | 0.110 | |
| Creatinine mg/dL | 1.0 (0.8; 1.4) | 1.0 (0.8; 1.6) | 1.1 (0.9; 1.6) | 1.1 (0.9; 1.5) | 0.259 | |
| Urea/creat | 38 (29; 53) | 37 (29; 52) | 42 (32; 52) | 39 (30; 52) | 0.159 | |
| Acute kidney failure in 72 h of admission | 34a (27.2%) | 25a, b (36.8%) | 56b (55.4%) | 115 (39.1%) | 0.000 | |
| Sodium mmol/L | 137 (135; 140) | 138 (134; 140) | 138 (134; 140) | 138 (134; 140) | 0.591 | |
| Potassium mmol/L | 4.1 (3.7; 4.4) | 4.0 (3.6; 4.4) | 4.0 (3.7; 4.5) | 4.0 (3.7; 4.4) | 0.721 | |
| Chloride mmol/L | 97a,b (94; 100) | 96a (93; 99) | 98b (94; 101) | 97 (94; 100) | 0.034 | |
| Bicarbonate mmol/L | 25 (22; 27) | 25 (23; 27) | 24 (22; 27) | 25 (22; 27) | 0.206 | |
| Lactate dehydrogenases UI/L | 317a (255; 395) | 341a,b (284; 410) | 421b (287; 548) | 342 (270; 447) | 0.000 | |
| Creatinine phosphokinases UI/L | 102a (53; 242) | 111a,b (50; 330) | 187b (90; 490) | 142 (62; 344) | 0.003 | |
| Total bilirubin mg/dL | 0.5 (0.4; 0.9) | 0.5 (0.4; 0.7) | 0.5 (0.4; 0.7) | 0.5 (0.4; 0.8) | 0.443 | |
| Direct bilirubin mg/dL | 0.3 (0.2; 0.4) | 0.2 (0.2; 0.4) | 0.3 (0.2; 0.4) | 0.3 (0.2; 0.4) | 0.587 | |
| Aspartate aminotransferase (AST) UI/L | 37a (26; 52) | 37a,b (25; 63) | 46b (31; 72) | 40 (27; 62) | 0.009 | |
| Alanine aminotransferases (ALT) UI/L | 27 (19; 40) | 26 (16; 43) | 26 (18; 45) | 26 (18; 42) | 0.873 | |
| Gamma-glutamyl-transferases (gGT) UI/L | 50 (32; 102) | 59 (26; 99) | 43 (29; 74) | 48 (30; 92) | 0.364 | |
| Alkaline phosphatases UI/L | 82a (58; 108) | 79a (61; 105) | 69b (52; 84) | 77 (58; 97) | 0.003 | |
| INR | 1.2 (1.1; 1.3) | 1.1 (1.1; 1.2) | 1.2 (1.1; 1.3) | 1.2 (1.1; 1.3) | 0.314 | |
| Prothrombin time (seconds) | 79 (68; 86) | 81 (72; 91) | 77 (68; 88) | 79 (68; 88) | 0.324 | |
| Partial thromboplastin time (seconds) | 32 (30; 35) | 32 (30; 36) | 33 (30; 36) | 33 (30; 35) | 0.314 | |
| Albumin (mg/dL) | 35.1a (32.0; 38.4) | 33.4a,b (30.8; 37.3) | 33.4b (30.4; 36.2) | 34.3 (31.4; 37.6) | 0.029 | |
| a, b, c: each letter denotes a subset of WHO Severity Classification categories whose column proportions do not differ significantly from each other at the 0.05 level after Bonferroni’s correction. | ||||||
Appendix B. Graphical Representations of Statistically Significant Values of the Table of Frequencies



References
- CDC. Interim Clinical Guidance for Management of Patients with Confirmed Coronavirus Disease (COVID-19). Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-guidance-management-patients.html (accessed on 28 August 2020).
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez-Morales, A.J.; Cardona-Ospina, J.A.; Gutiérrez-Ocampo, E.; Villamizar-Peña, R.; Holguin-Rivera, Y.; Escalera-Antezana, J.P.; Alvarado-Arnez, L.E.; Bonilla-Aldana, D.K.; Franco-Paredes, C.; Henao-Martinez, A.F.; et al. Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis. Travel Med. Infect. Dis. 2020, 34, 101623. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Zheng, Y.; Gou, X.; Pu, K.; Chen, Z.; Guo, Q.; Ji, R.; Wang, H.; Wang, Y.; Zhou, Y. Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: A systematic review and meta-analysis. Int. J. Infect. Dis. 2020, 94, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Liang, W.; Liang, H.; Ou, L.; Chen, B.; Chen, A.; Li, C.; Li, Y.; Guan, W.; Sang, L.; Lu, J.; et al. Development and Validation of a Clinical Risk Score to Predict the Occurrence of Critical Illness in Hospitalized Patients With COVID-19. JAMA Intern. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Ji, D.; Zhang, D.; Xu, J.; Chen, Z.; Yang, T.; Zhao, P.; Chen, G.; Cheng, G.; Wang, Y.; Bi, J.; et al. Prediction for Progression Risk in Patients with COVID-19 Pneumonia: The CALL Score. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Z.; Chen, A.; Hou, W.; Graham, J.M.; Li, H.; Richman, P.S.; Thode, H.C.; Singer, A.J.; Duong, T.Q. Prediction model and risk scores of ICU admission and mortality in COVID-19. PLoS ONE 2020, 15, e0236618. [Google Scholar] [CrossRef] [PubMed]
- Satici, C.; Demirkol, M.A.; Altunok, E.S.; Gursoy, B.; Alkan, M.; Kamat, S.; Demirok, B.; Surmeli, C.D.; Calik, M.; Cavus, Z.; et al. Performance of pneumonia severity index and CURB-65 in predicting 30-day mortality in patients with COVID-19. Int. J. Infect. Dis. 2020, 98, 84–89. [Google Scholar] [CrossRef] [PubMed]
- WHO. Clinical Management of Covid-19—Interim Guidance. Available online: https://www.who.int/publications/i/item/clinical-management-of-covid-19 (accessed on 29 June 2020).
- Conrady, S.; Jouffe, L. Bayesian Networks and BayesiaLab: A Practical Introduction for Researchers. In Bayesian Networks and BayesiaLab: A Practical Introduction for Researchers; Ed.; Bayesia: Franklin, TN, USA, 2015; Available online: https://library.bayesia.com/articles/#!bayesialab-knowledge-hub/2-bayesian-networks-theory (accessed on 4 October 2020).
- Wang, Y.; Lu, X.; Li, Y.; Chen, H.; Chen, T.; Su, N.; Huang, F.; Zhou, J.; Zhang, B.; Yan, F.; et al. Clinical Course and Outcomes of 344 Intensive Care Patients with COVID-19. Am. J. Respir. Crit. Care Med. 2020, 201, 1430–1434. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Shang, Y.; Liu, T.; Wei, Y.; Li, J.; Shao, L.; Liu, M.; Zhang, Y.; Zhao, Z.; Xu, H.; Peng, Z.; et al. Scoring systems for predicting mortality for severe patients with COVID-19. EClinicalMedicine 2020, 24, 100426. [Google Scholar] [CrossRef] [PubMed]
- Miesbach, W.; Makris, M. COVID-19: Coagulopathy, Risk of Thrombosis, and the Rationale for Anticoagulation. Clin. Appl. Thromb. Hemost. 2020, 26, 1076029620938149. [Google Scholar] [CrossRef] [PubMed]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikpouraghdam, M.; Farahani, A.J.; Alishiri, G.; Heydari, S.; Ebrahimnia, M.; Samadinia, H.; Sepandi, M.; Jafari, N.J.; Izadi, M.; Qazvini, A.; et al. Epidemiological characteristics of coronavirus disease 2019 (COVID-19) patients in IRAN: A single center study. J. Clin. Virol. 2020, 127, 104378. [Google Scholar] [CrossRef] [PubMed]
- Kaye, R.; Chang, C.W.D.; Kazahaya, K.; Brereton, J.; Denneny, I.J.C. COVID-19 Anosmia Reporting Tool: Initial Findings. Otolaryngol. Head Neck Surg. 2020, 163, 132–134. [Google Scholar] [CrossRef] [PubMed]
- Meng, X.; Deng, Y.; Dai, Z.; Meng, Z. COVID-19 and anosmia: A review based on up-to-date knowledge. Am. J. Otolaryngol. 2020, 41, 102581. [Google Scholar] [CrossRef] [PubMed]
- Chilimuri, S.; Sun, H.; Alemam, A.; Manthri, N.; Shehi, E.; Tejada, J.; Yugay, A.; Nayudu, S.K. Predictors of Mortality in Adults Admitted with COVID-19: Retrospective Cohort Study from New York City. West. J. Emerg. Med. 2020, 21, 779–784. [Google Scholar] [CrossRef] [PubMed]
- Turner, A.J.; A Hiscox, J.; Hooper, N.M. ACE2: From vasopeptidase to SARS virus receptor. Trends Pharmacol. Sci. 2004, 25, 291–294. [Google Scholar] [CrossRef] [PubMed]
- Rubenfeld, G.D.; Caldwell, E.; Slutsky, A.A.; Antonelli, M.; Anzueto, A.; Beale, R.; Bertsen, A.; Brochard, L.; Brower, R.; Camporota, L.; et al. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef]
- Mehta, R.L.; A Kellum, J.; Shah, S.V.; A Molitoris, B.; Ronco, C.; Warnock, D.G.; Levin, A. Acute Kidney Injury Network: Report of an initiative to improve outcomes in acute kidney injury. Crit. Care 2007, 11, R31. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| K-Fold (10), Structural Priors, Target: Critical Illness | ||
|---|---|---|
| Value | 0 | 1 |
| Gini Index | 29.66% | 42.53% |
| Relative Gini Index | 72.30% | 72.14% |
| Lift Index | 1.41 | 1.65 |
| Relative Lift Index | 92.45% | 88.18% |
| ROC Index | 86.39% | 86.31% |
| Calibration Index | 57.16% | 58.90% |
| Binary Log-Loss | 0.46 | 0.46 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Terwangne, C.; Laouni, J.; Jouffe, L.; Lechien, J.R.; Bouillon, V.; Place, S.; Capulzini, L.; Machayekhi, S.; Ceccarelli, A.; Saussez, S.; et al. Predictive Accuracy of COVID-19 World Health Organization (WHO) Severity Classification and Comparison with a Bayesian-Method-Based Severity Score (EPI-SCORE). Pathogens 2020, 9, 880. https://doi.org/10.3390/pathogens9110880
de Terwangne C, Laouni J, Jouffe L, Lechien JR, Bouillon V, Place S, Capulzini L, Machayekhi S, Ceccarelli A, Saussez S, et al. Predictive Accuracy of COVID-19 World Health Organization (WHO) Severity Classification and Comparison with a Bayesian-Method-Based Severity Score (EPI-SCORE). Pathogens. 2020; 9(11):880. https://doi.org/10.3390/pathogens9110880
Chicago/Turabian Stylede Terwangne, Christophe, Jabber Laouni, Lionel Jouffe, Jerome R. Lechien, Vincent Bouillon, Sammy Place, Lucio Capulzini, Shahram Machayekhi, Antonia Ceccarelli, Sven Saussez, and et al. 2020. "Predictive Accuracy of COVID-19 World Health Organization (WHO) Severity Classification and Comparison with a Bayesian-Method-Based Severity Score (EPI-SCORE)" Pathogens 9, no. 11: 880. https://doi.org/10.3390/pathogens9110880
APA Stylede Terwangne, C., Laouni, J., Jouffe, L., Lechien, J. R., Bouillon, V., Place, S., Capulzini, L., Machayekhi, S., Ceccarelli, A., Saussez, S., Sorgente, A., & on behalf of EPIBASE TEAM. (2020). Predictive Accuracy of COVID-19 World Health Organization (WHO) Severity Classification and Comparison with a Bayesian-Method-Based Severity Score (EPI-SCORE). Pathogens, 9(11), 880. https://doi.org/10.3390/pathogens9110880