Generation of Domains for the Equine Musculoskeletal Rehabilitation Outcome Score: Development by Expert Consensus


{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Delphi Step 1
2.2. Delphi Step 2
2.3. Delphi Step 3
2.4. Delphi Step 4
3. Results
3.1. Delphi Step 1
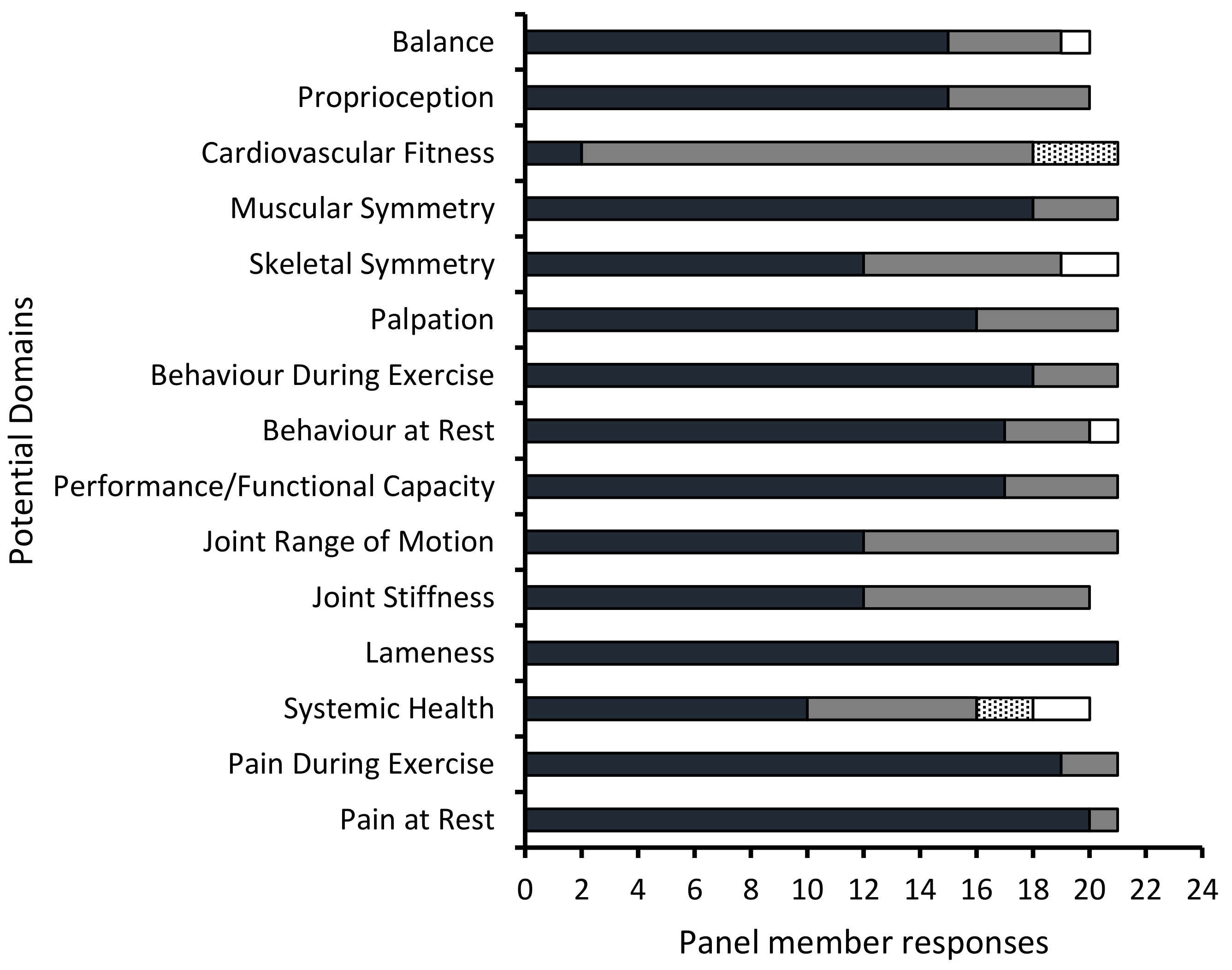
3.2. Delphi Step 2
3.3. Delphi Step 3
3.4. Delphi Step 4
4. Discussion
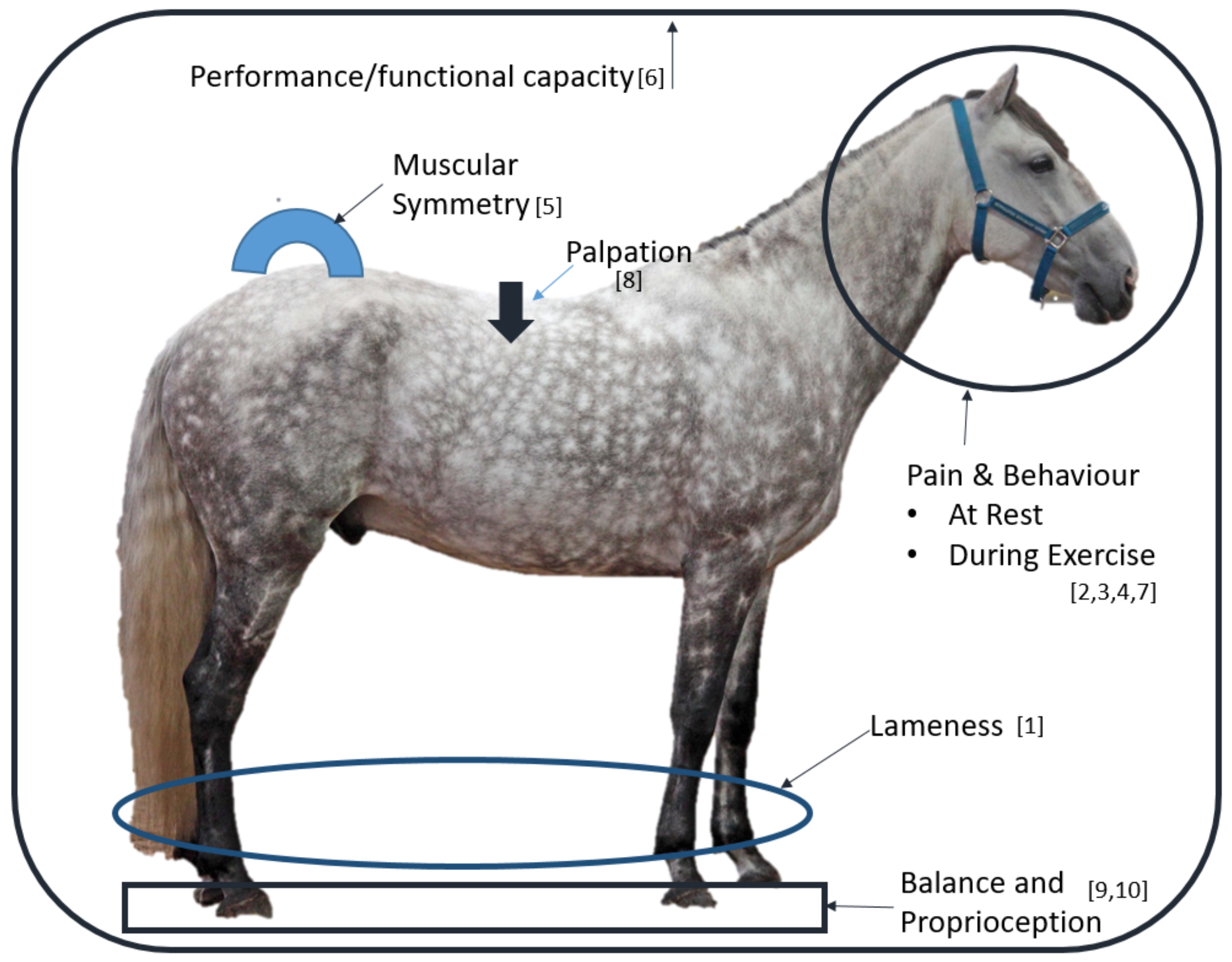
4.1. Lameness
4.2. Pain Assessment
4.3. Muscle Symmetry
4.4. Performance/Functional Capacity
4.5. Palpation
4.6. Balance and Proprioception
4.7. Limitations to the Study
4.8. TEMROS—Further Development
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kaneps, A.J. Practical rehabilitation and physical therapy for the general equine practitioner. Vet. Clin. N. Am. Equine Pract. 2016, 32, 167–180. [Google Scholar] [CrossRef] [PubMed]
- Tabor, G. Routine equine physiotherapy. Equine Vet. Educ. 2018. [Google Scholar] [CrossRef]
- Haussler, K.K. The role of manual therapies in equine pain management. Vet. Clin. N. Am. Equine Pract. 2010, 26, 579–601. [Google Scholar] [CrossRef] [PubMed]
- Clayton, H.M. Core training and rehabilitation in horses. Vet. Clin. N. Am. Equine Pract. 2016, 32, 49–71. [Google Scholar] [CrossRef]
- Paulekas, R.; Haussler, K.K. Principles and practice of therapeutic exercise for horses. J. Equine Vet. Sci. 2009, 29, 870–893. [Google Scholar] [CrossRef]
- Tabor, G.; Williams, J. The use of outcome measures in equine rehabilitation. Vet. Nurs. 2018, 9, 497–500. [Google Scholar] [CrossRef] [Green Version]
- Coomer, R.P.; McKane, S.A.; Smith, N.; Vandeweerd, J.M.E. A controlled study evaluating a novel surgical treatment for kissing spines in standing sedated horses. Vet. Surg. 2012, 41, 890–897. [Google Scholar] [CrossRef]
- Stubbs, N.C.; Kaiser, L.J.; Hauptman, J.; Clayton, H.M. Dynamic mobilisation exercises increase cross sectional area of musculus multifidus. Equine Vet. J. 2011, 43, 22–529. [Google Scholar] [CrossRef]
- Schils, S.J.; Turner, T.A. Functional Electrical Stimulation for equine epaxial muscle spasms: Retrospective study of 241 clinical cases. Comp. Exerc. Physiol. 2014, 10, 89–97. [Google Scholar] [CrossRef]
- Haussler, K.K.; Hill, A.E.; Puttlitz, C.M.; McIlwraith, C.W. Effects of vertebral mobilization and manipulation on kinematics of the thoracolumbar region. Am. J. Vet. Res. 2007, 68, 508–516. [Google Scholar] [CrossRef]
- Sullivan, K.A.; Hill, A.E.; Haussler, K.K. The effects of chiropractic, massage and phenylbutazone on spinal mechanical nociceptive thresholds in horses without clinical signs. Equine Vet. J. 2008, 40, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Chartered Society of Physiotherapy. Outcome and Experience measures. Available online: https://www.csp.org.uk/professional-clinical/research-and-evaluation/outcome-and-experience-measures (accessed on 16 September 2019).
- Boers, M.; Kirwan, J.R.; Wells, G.; Beaton, D.; Gossec, L.; d’Agostino, M.A.; Conaghan, P.G.; Bingham, C.O.; Brooks, P., III; Landewé, R.; et al. Developing core outcome measurement sets for clinical trials: OMERACT filter 2.0. J. Clin. Epidemiol. 2014, 67, 745–753. [Google Scholar] [CrossRef] [Green Version]
- Chiarotto, A.; Terwee, C.B.; Deyo, R.A.; Boers, M.; Lin, C.W.C.; Buchbinder, R.; Corbin, T.P.; Costa, L.O.; Foster, N.E.; Grotle, M.; et al. A core outcome set for clinical trials on non-specific low back pain: Study protocol for the development of a core domain set. Trials 2014, 15, 511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacklin, B.D.; Minshall, G.J.; Wright, I.M. A new technique for subtotal (cranial wedge) ostectomy in the treatment of impinging/overriding spinous processes: Description of technique and outcome of 25 cases. Equine Vet. J. 2014, 46, 339–344. [Google Scholar] [CrossRef]
- Walmsley, J.P.; Pettersson, H.; Winberg, F.; McEvoy, F. Impingement of the dorsal spinous processes in two hundred and fifteen horses: Case selection, surgical technique and results. Equine Vet. J. 2014, 34, 23–28. [Google Scholar] [CrossRef]
- Nagy, A.; Quiney, L.; Dyson, S. Long-term outcome of 84 horses with sacroiliac joint region pain with (n= 69) or without (n= 15) other orthopaedic problems. Equine Vet. Educ. 2019. [CrossRef]
- Chiarotto, A.; Deyo, R.A.; Terwee, C.B.; Boers, M.; Buchbinder, R.; Corbin, T.P.; Costa, L.O.; Foster, N.E.; Grotle, M.; Koes, B.W.; et al. Core outcome domains for clinical trials in non-specific low back pain. Eur. Spine J. 2015, 24, 1127–1142. [Google Scholar] [CrossRef]
- Kyte, D.G.; Calvert, M.; Van der Wees, P.J.; Ten Hove, R.; Tolan, S.; Hill, J.C. An introduction to patient-reported outcome measures (PROMs) in physiotherapy. Physiotherapy 2015, 101, 119–125. [Google Scholar] [CrossRef] [Green Version]
- Visentini, P.J.; Khan, K.M.; Cook, J.L.; Kiss, Z.S.; Harcourt, P.R.; Wark, J.D. and Victorian Institute of Sport Tendon Study Group. The VISA score: An index of severity of symptoms in patients with jumper’s knee (patellar tendinosis). J. Sci. Med. Sport. 1998, 1, 22–28. [Google Scholar] [CrossRef]
- Robinson, J.M.; Cook, J.L.; Purdam, C.; Visentini, P.J.; Ross, J.; Maffulli, N.; Taunton, J.E.; Khan, K.M. The VISA-A questionnaire: A valid and reliable index of the clinical severity of Achilles tendinopathy. Br. J. Sports Med. 2001, 35, 335–341. [Google Scholar] [CrossRef]
- Thorborg, K.; Hölmich, P.; Christensen, R.; Petersen, J.; Roos, E.M. The Copenhagen Hip and Groin Outcome Score (HAGOS): Development and validation according to the COSMIN checklist. Br. J. Sports Med. 2011, 45, 478–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hielm-Björkman, A.K.; Kuusela, E.; Liman, A.; Markkola, A.; Saarto, E.; Huttunen, P.; Leppäluoto, J.; Tulamo, R.M.; Raekallio, M. Evaluation of methods for assessment of pain associated with chronic osteoarthritis in dogs. J. Am. Vet. Med. Assoc. 2003, 222, 1552–1558. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.C.; Boston, R.C.; Coyne, J.C.; Farrar, J.T. Development and psychometric testing of an instrument designed to measure chronic pain in dogs with osteoarthritis. Am. J. Vet. Res. 2007, 68, 631–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boström, A.F.; Hyytiäinen, H.K.; Koho, P.; Cizinauskas, S.; Hielm-Björkman, A.K. Development of the Finnish neurological function testing battery for dogs and its intra-and inter-rater reliability. Acta Vet. Scand. 2018, 60, 56. [Google Scholar] [CrossRef]
- Haussler, K.K.; Erb, H.N. Pressure algometry for the detection of induced back pain in horses: A preliminary study. Equine Vet. J. 2006, 38, 76–81. [Google Scholar] [CrossRef] [PubMed]
- De Heus, P.; Van Oossanen, G.; Van Dierendonck, M.C.; Back, W. A pressure algometer is a useful tool to objectively monitor the effect of diagnostic palpation by a physiotherapist in warmblood horses. J. Equine Vet. Sci. 2010, 30, 310–321. [Google Scholar] [CrossRef]
- Varcoe-Cocks, K.; Sagar, K.N.; Jeffcott, L.B.; McGowan, C.M. Pressure algometry to quantify muscle pain in racehorses with suspected sacroiliac dysfunction. Equine Vet. J. 2006, 38, 558–562. [Google Scholar] [CrossRef]
- Merrifield-Jones, M.; Tabor, G.; Williams, J. Inter and Intra-Rater Reliability of Soft Tissue Palpation in the Equine Thoracic Epaxial Region. J. Equine Vet. Sci. 2019. [Google Scholar] [CrossRef]
- Tabor, G.; Elliott, A.; Mann, N.; Williams, J. Equine Posture Analysis: Development of a Simple Tool to Record Equine Thoracolumbar Posture. J. Equine Vet. Sci. 2019, 73, 81–83. [Google Scholar] [CrossRef]
- Greve, L.; Dyson, S. A longitudinal study of back dimension changes over 1 year in sports horses. Vet. J. 2015, 203, 65–73. [Google Scholar] [CrossRef]
- Liljebrink, Y.; Bergh, A. Goniometry: Is it a reliable tool to monitor passive joint range of motion in horses? Equine Vet. J. 2010, 42, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Adair, H.; Marcellin-Little, D.; Levine, D. Validity and repeatability of goniometry in normal horses. Vet. Comp. Orthop. Traumatol. 2016, 29, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Gleerup, K.B.; Lindegaard, C. Recognition and quantification of pain in horses: A tutorial review. Equine Vet. Educ. 2016, 28, 47–57. [Google Scholar] [CrossRef]
- Klassen, A.F.; Cano, S.J.; Schwitzer, J.A.; Scott, A.M.; Pusic, A.L. FACE-Q scales for health-related quality of life, early life impact, satisfaction with outcomes, and decision to have treatment: Development and validation. Plast. Reconstr. Surg. 2015, 135, 375–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tabor, G.; Williams, J. Objective Measurement in Equine Physiotherapy. Comp. Exerc. Physiol. 2018, in press. [Google Scholar] [CrossRef]
- Hsu, C.C.; Sandford, B.A. The Delphi technique: Making sense of consensus. Pract. Assess. Res. Eval. 2007, 12, 10. [Google Scholar]
- Murray, I.R.; Geeslin, A.G.; Goudie, E.B.; Petrigliano, F.A.; LaPrade, R.F. Minimum information for studies evaluating biologics in orthopaedics (MIBO): Platelet-rich plasma and mesenchymal stem cells. J. Bone Joint Surg. Am. 2017, 99, 809–819. [Google Scholar] [CrossRef]
- Lawshe, C.H. A quantitative approach to content validity. Pers. Psychol. 1974, 28, 563–575. [Google Scholar] [CrossRef]
- Ayre, C.; Scally, A.J. Critical values for Lawshe’s content validity ratio: Revisiting the original methods of calculation. Meas Eval Couns Dev. 2014, 47, 79–86. [Google Scholar] [CrossRef] [Green Version]
- Starke, S.D.; Oosterlinck, M. Reliability of equine visual lameness classification as a function of expertise, lameness severity and rater confidence. Vet. Rec. 2018. [Google Scholar] [CrossRef]
- Keegan, K.G.; Dent, E.V.; Wilson, D.A.; Janicek, J.; Kramer, J.; Lacarrubba, A.; Walsh, D.M.; Cassells, M.W.; Esther, T.M.; Schiltz, P.; et al. Repeatability of subjective evaluation of lameness in horses. Equine Vet. J. 2010, 42, 92–97. [Google Scholar] [CrossRef] [PubMed]
- McCracken, M.J.; Kramer, J.; Keegan, K.G.; Lopes, M.; Wilson, D.A.; Reed, S.K.; LaCarrubba, A.; Rasch, M. Comparison of an inertial sensor system of lameness quantification with subjective lameness evaluation. Equine Vet. J. 2012, 44, 652–656. [Google Scholar] [CrossRef] [PubMed]
- Keegan, K.G.; Wilson, D.A.; Wilson, D.J.; Smith, B.; Gaughan, E.M.; Pleasant, R.S.; Lillich, J.D.; Kramer, J.; Howard, R.D.; Bacon-Miller, C.; et al. Evaluation of mild lameness in horses trotting on a treadmill by clinicians and interns or residents and correlation of their assessments with kinematic gait analysis. Am. J. Vet. Res. 1998, 59, 1370–1377. [Google Scholar] [PubMed]
- Hewetson, M.; Christley, R.M.; Hunt, I.D.; Voute, L.C. Investigations of the reliability of observational gait analysis for the assessment of lameness in horses. Vet. Rec. 2006, 158, 852–858. [Google Scholar] [CrossRef] [PubMed]
- Fuller, C.J.; Bladon, B.M.; Driver, A.J.; Barr, A.R. The intra-and inter-assessor reliability of measurement of functional outcome by lameness scoring in horses. Vet. J. 2006, 171, 281286. [Google Scholar] [CrossRef] [PubMed]
- Dyson, S. Can lameness be graded reliably? Equine Vet. J. 2011, 43, 379–382. [Google Scholar] [CrossRef] [PubMed]
- Dyson, S.; Berger, J.M.; Ellis, A.D.; Mullard, J. Behavioral observations and comparisons of nonlame horses and lame horses before and after resolution of lameness by diagnostic analgesia. J. Vet. Behav. 2018, 26, 64–70. [Google Scholar] [CrossRef]
- Bragança, F.S.; Rhodin, M.; van Weeren, P.R. On the brink of daily clinical application of objective gait analysis: What evidence do we have so far from studies using an induced lameness model? Vet. J. 2018, 234, 11–23. [Google Scholar] [CrossRef] [Green Version]
- Dalla Costa, E.; Minero, M.; Lebelt, D.; Stucke, D.; Canali, E.; Leach, M.C. Development of the Horse Grimace Scale (HGS) as a pain assessment tool in horses undergoing routine castration. PLoS ONE 2014, 9, e92281. [Google Scholar] [CrossRef] [Green Version]
- Gleerup, K.B.; Forkman, B.; Lindegaard, C.; Andersen, P.H. An equine pain face. Vet. Anaesth. Analg. 2015, 42, 103–114. [Google Scholar] [CrossRef] [Green Version]
- Bussieres, G.; Jacques, C.; Lainay, O.; Beauchamp, G.; Leblond, A.; Cadoré, J.L.; Desmaizières, L.M.; Cuvelliez, S.G.; Troncy, E. Development of a composite orthopaedic pain scale in horses. Res. Vet. Sci. 2008, 85, 294–306. [Google Scholar] [CrossRef] [PubMed]
- Langford, D.J.; Bailey, A.L.; Chanda, M.L.; Clarke, S.E.; Drummond, T.E.; Echols, S.; Glick, S.; Ingrao, J.; Klassen-Ross, T.; LaCroix-Fralish, M.L.; et al. Coding of facial expressions of pain in the laboratory mouse. Nat. Methods. 2010, 7, 447. [Google Scholar] [CrossRef] [PubMed]
- Sotocina, S.G.; Sorge, R.E.; Zaloum, A.; Tuttle, A.H.; Martin, L.J.; Wieskopf, J.S.; Mapplebeck, J.C.; Wei, P.; Zhan, S.; Zhang, S.; et al. The Rat Grimace Scale: A partially automated method for quantifying pain in the laboratory rat via facial expressions. Mol. Pain. 2011, 7, 1744–8069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mullard, J.; Berger, J.M.; Ellis, A.D.; Dyson, S. Development of an ethogram to describe facial expressions in ridden horses (FEReq). J. Vet. Behav. 2017, 18, 7–12. [Google Scholar] [CrossRef]
- Dyson, S.; Berger, J.; Ellis, A.D.; Mullard, J. Development of an ethogram for a pain scoring system in ridden horses and its application to determine the presence of musculoskeletal pain. J. Vet. Behav. 2018, 23, 47–57. [Google Scholar] [CrossRef]
- Keeling, L.J.; Jonare, L.; Lanneborn, L. Investigating horse–human interactions: The effect of a nervous human. Vet. J. 2009, 181, 70–71. [Google Scholar] [CrossRef]
- Barstow, A.; Dyson, S. Clinical features and diagnosis of sacroiliac joint region pain in 296 horses: 2004–2014. Equine Vet. Educ. 2015, 27, 637–647. [Google Scholar] [CrossRef]
- Zimmerman, M.; Dyson, S.; Murray, R. Close, impinging and overriding spinous processes in the thoracolumbar spine: The relationship between radiological and scintigraphic findings and clinical signs. Equine Vet. J. 2012, 44, 178–184. [Google Scholar] [CrossRef]
- De Oliveira, K.; Soutello, R.V.; da Fonseca, R.; Costa, C.; Paulo, R.D.L.; Fachiolli, D.F.; Clayton, H.M. Gymnastic training and dynamic mobilization exercises improve stride quality and increase epaxial muscle size in therapy horses. J. Equine Vet. Sci. 2015, 35, 888–893. [Google Scholar] [CrossRef] [Green Version]
- Abe, T.; Kearns, C.F.; Rogers, B. Reliability of ultrasound-measured muscle thickness of the longissimus dorsi muscle in thoroughbreds. Comp. Exerc. Physiol. 2012, 8, 189–194. [Google Scholar] [CrossRef]
- Walker, V.A.; Tranquille, C.A.; Dyson, S.J.; Spear, J.; Murray, R.C. Association of a subjective muscle score with increased angles of flexion during sitting trot in dressage horses. J. Equine Vet. Sci. 2016, 40, 6–15. [Google Scholar] [CrossRef]
- Sloet, M.V.; Barneveld, A. Comparison of the workload of Dutch warmblood horses ridden normally and on a treadmill. Vet. Rec. 1995, 137, 136–139. [Google Scholar]
- Couroucé, A. Field exercise testing for assessing fitness in French Standardbred trotters. Vet. J. 1999, 157, 112–122. [Google Scholar] [CrossRef] [PubMed]
- Munk, R.; Møller, S.; Lindner, A. Effects of training with different interval exercises on horses used for show jumping. Comp. Exerc. Physiol. 2013, 9, 33–41. [Google Scholar] [CrossRef]
- Munsters, C.C.; van Iwaarden, A.; van Weeren, R.; van Oldruitenborgh-Oosterbaan, M.M.S. Exercise testing in Warmblood sport horses under field conditions. Vet. J. 2014, 202, 11–19. [Google Scholar] [CrossRef]
- Gomez-Piqueras, P.; Gonzalez-Rubio, J.; De Baranda, P.S.; Najera, A. Use of functional performance tests in sports: Evaluation proposal for football players in the rehabilitation phase. Turk. J. Ph. Med. Rehab. 2018, 64, 2587–2823. [Google Scholar] [CrossRef]
- Larsen, J.B.; Farup, J.; Lind, M.; Dalgas, U. Muscle strength and functional performance is markedly impaired at the recommended time point for sport return after anterior cruciate ligament reconstruction in recreational athletes. Hum. Mov. Sci. 2015, 39, 73–87. [Google Scholar] [CrossRef]
- Clayton, H.M.; Kaiser, L.J.; Lavagnino, M.; Stubbs, N.C. Dynamic mobilisations in cervical flexion: Effects on intervertebral angulations. Equine Vet. J. 2010, 42, 688–694. [Google Scholar] [CrossRef]
- Goff, L. Physiotherapy assessment for animals. In Animal Physiotherapy, 2nd ed.; McGowan, C.M., Goff, L., Eds.; Wiley-Blackwell: West Sussex, UK, 2016; pp. 171–196. [Google Scholar]
- Haussler, K.K.; Erb, H.N. Mechanical nociceptive thresholds in the axial skeleton of horses. Equine Vet. J. 2006, 38, 70–75. [Google Scholar] [CrossRef]
- Menke, E.S.; Blom, G.; van Loon, J.P.; Back, W. Pressure algometry in Icelandic horses: Interexaminer and intraexaminer reliability. J. Equine Vet. Sci. 2016, 36, 26–31. [Google Scholar] [CrossRef]
- Coghill, R.C. Individual differences in the subjective experience of pain: New insights into mechanisms and models. Headache. 2010, 50, 1531–1535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stasiak, K.L.; Maul, D.O.N.; French, E.; Hellyer, P.W.; Vandewoude, S. Species-specific assessment of pain in laboratory animals. J. Am. Assoc. Lab. Anim. Sci. 2003, 42, 13–20. [Google Scholar]
- Clayton, H.M.; Bialski, D.E.; Lanovaz, J.L.; Mullineaux, D.R. Assessment of the reliability of a technique to measure postural sway in horses. Am. J. Vet. Res. 2003, 64, 1354–1359. [Google Scholar] [CrossRef] [PubMed]
- Bialski, D.; Lanovaz, J.L.; Bohart, G.V.; Mullineaux, D.R.; Clayton, H.M. Effect of detomidine on postural sway in horses. Equine Comp. Exerc. Physiol. 2004, 1, 45–50. [Google Scholar] [CrossRef] [Green Version]
- Clayton, H.M.; Nauwelaerts, S. Effect of blindfolding on centre of pressure variables in healthy horses during quiet standing. Vet. J. 2014, 199, 365–369. [Google Scholar] [CrossRef]
- King, M.R.; Haussler, K.K.; Kawcak, C.E.; McIlwraith, C.W.; Reiser, R.F., II. Effect of underwater treadmill exercise on postural sway in horses with experimentally induced carpal joint osteoarthritis. Am. J. Vet. Res. 2013, 74, 971–982. [Google Scholar] [CrossRef]
- Stubbs, N.C.; Clayton, H.M. Activate Your Horse’s Core: Unmounted Exercises for Dynamic Mobility, Strength, & Balance; Sport Horse Publications: Mason, MI, USA, 2008. [Google Scholar]
- Clough, W.T.; Canapp, S.O., Jr. Assessing Clinical Relevance of Weight Distribution as Measured on a Stance Analyzer through Comparison with Lameness Determined on a Pressure Sensitive Walkway and Clinical Diagnosis. Vet. Comp. Orthop. Traumatol. 2018, 31, A3622. [Google Scholar] [CrossRef]
- Basch, E.; Spertus, J.; Dudley, R.A.; Wu, A.; Chuahan, C.; Cohen, P.; Smith, M.L.; Black, N.; Crawford, A.; Christensen, K.; et al. Methods for developing patient-reported outcome-based performance measures (PRO-PMs). Value Health. 2015, 18, 493–504. [Google Scholar] [CrossRef] [Green Version]
- Soroko, M.; Henklewski, R.; Filipowski, H.; Jodkowska, E. The effectiveness of thermographic analysis in equine orthopedics. J. Equine Vet. Sci. 2013, 33, 760–762. [Google Scholar] [CrossRef]
- Soroko, M.; Howell, K. Infrared thermography: Current applications in equine medicine. J. Equine Vet. Sci. 2018, 60, 90–96. [Google Scholar] [CrossRef]


© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tabor, G.; Nankervis, K.; Fernandes, J.; Williams, J. Generation of Domains for the Equine Musculoskeletal Rehabilitation Outcome Score: Development by Expert Consensus. Animals 2020, 10, 203. https://doi.org/10.3390/ani10020203
Tabor G, Nankervis K, Fernandes J, Williams J. Generation of Domains for the Equine Musculoskeletal Rehabilitation Outcome Score: Development by Expert Consensus. Animals. 2020; 10(2):203. https://doi.org/10.3390/ani10020203
Chicago/Turabian StyleTabor, Gillian, Kathryn Nankervis, John Fernandes, and Jane Williams. 2020. "Generation of Domains for the Equine Musculoskeletal Rehabilitation Outcome Score: Development by Expert Consensus" Animals 10, no. 2: 203. https://doi.org/10.3390/ani10020203
APA StyleTabor, G., Nankervis, K., Fernandes, J., & Williams, J. (2020). Generation of Domains for the Equine Musculoskeletal Rehabilitation Outcome Score: Development by Expert Consensus. Animals, 10(2), 203. https://doi.org/10.3390/ani10020203