Identification and Quantification of Transient Receptor Potential Vanilloid 1 (TRPV1) in Equine Articular Tissue

 , ,
, ,
Abstract
:Simple summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Animals and Sample Collection
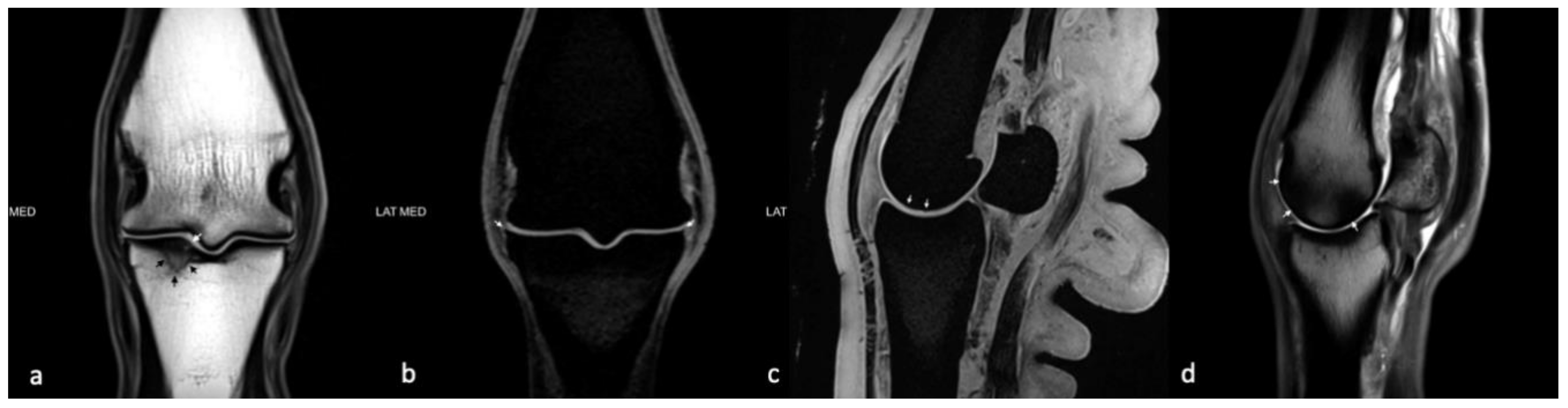
2.2. Magnetic Resonance Imaging
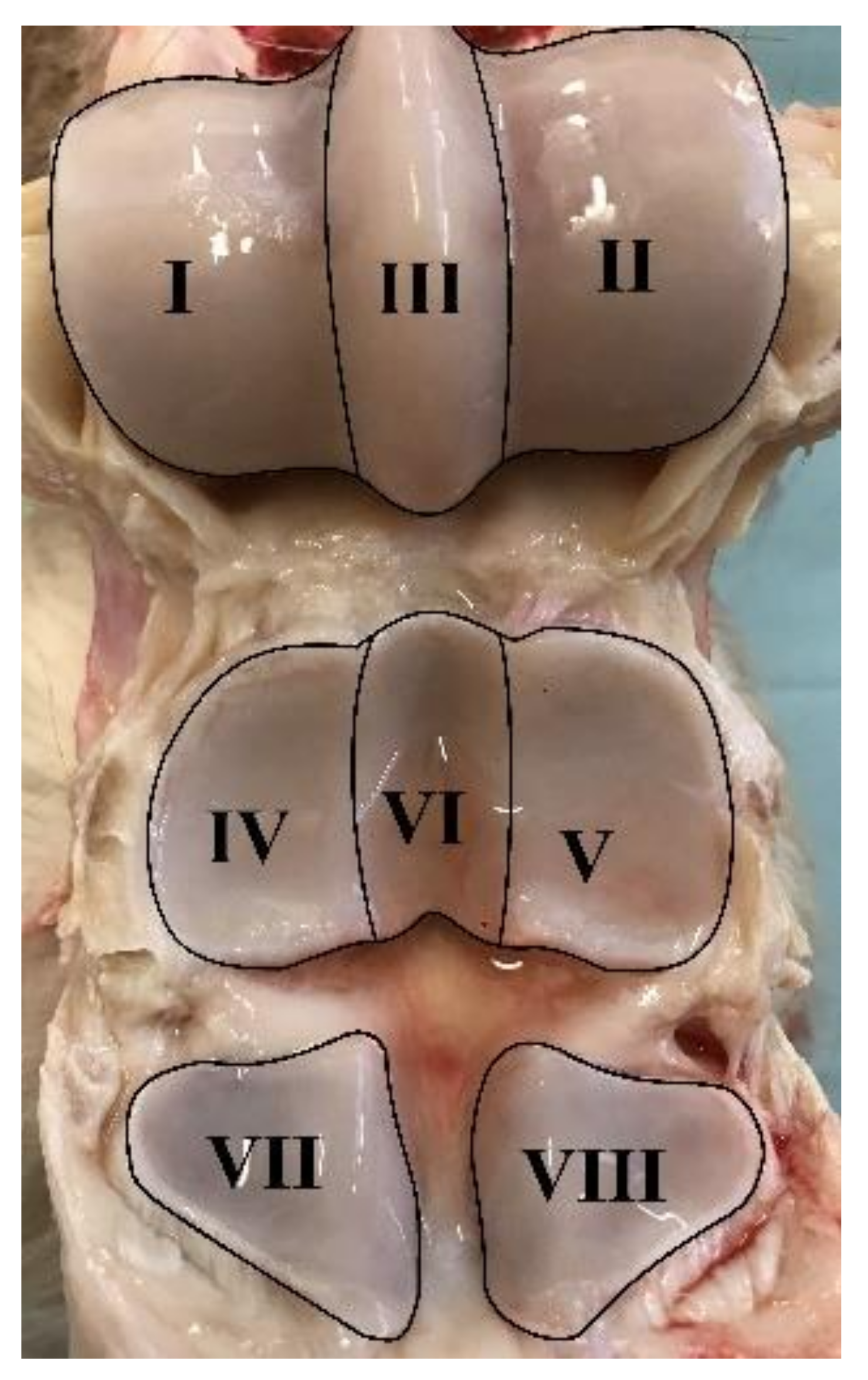
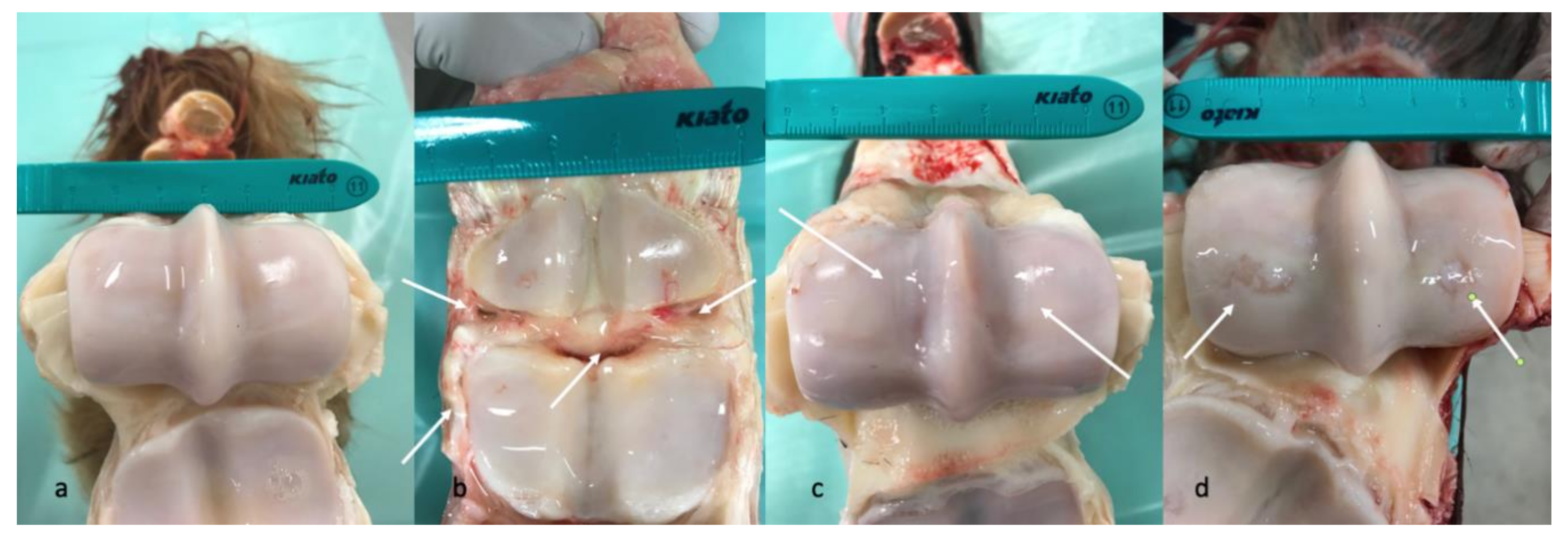
2.3. Macroscopic Evaluation
2.4. Synovial Fluid Analysis
2.5. ELISA
2.6. RNA Isolation and Quantitative Real-Time Reverse Transcriptase PCR Analysis
2.7. Statistics
3. Results
3.1. Division into Groups
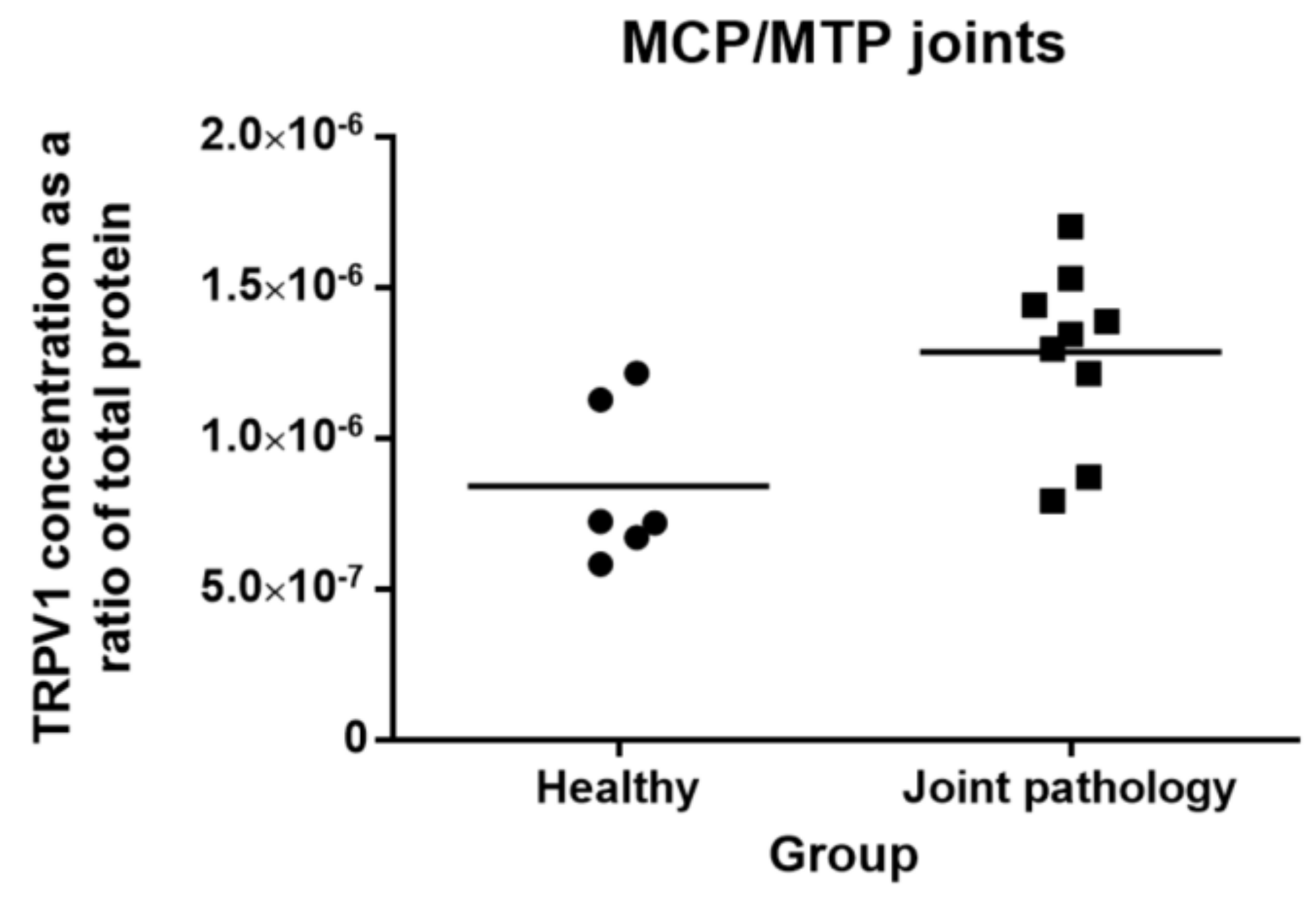
3.2. Levels of TRPV1 in Metacarpo-Phalangeal/Metatarso-Phalangeal (MCP/MTP) Joints
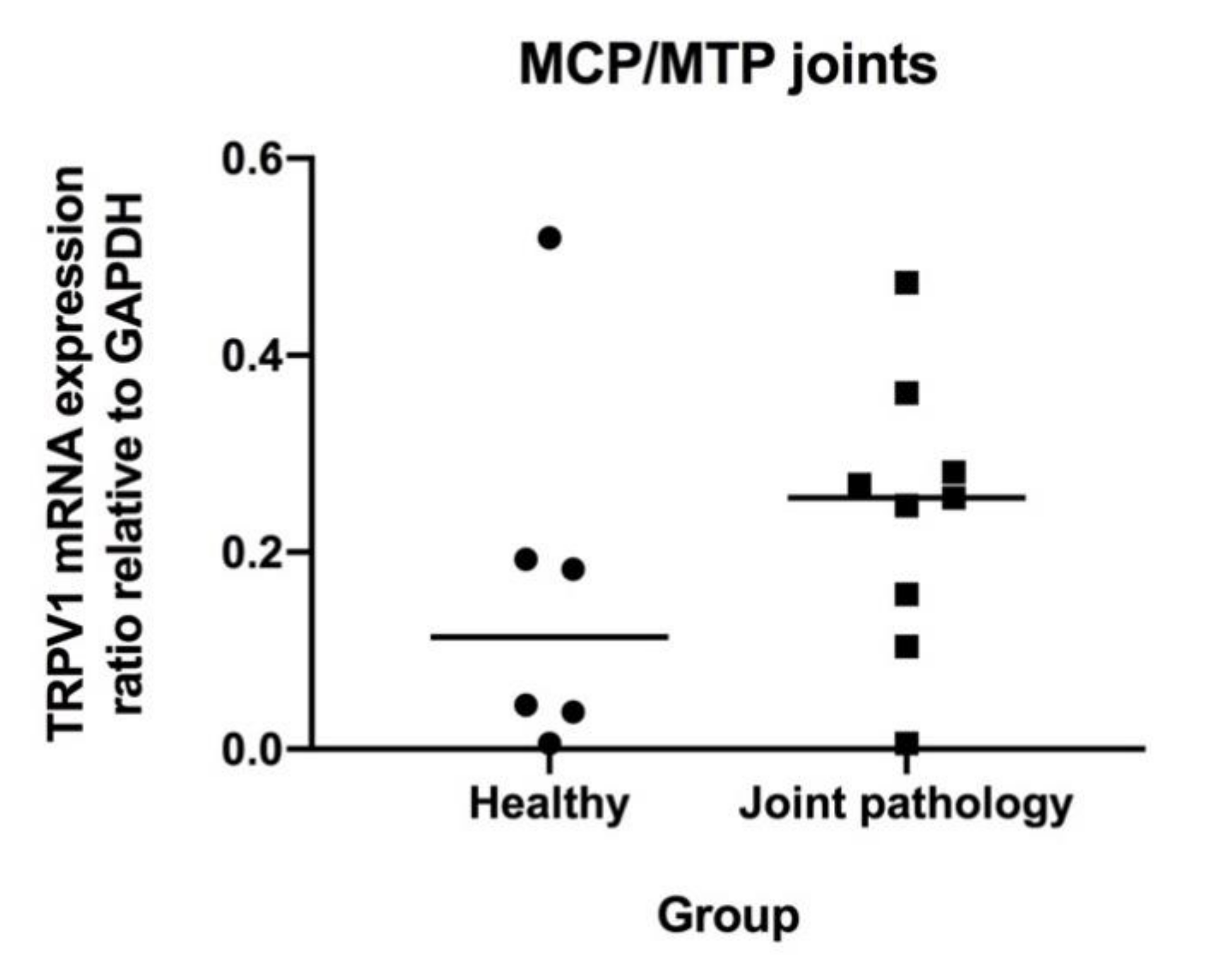
3.3. Levels of mRNA Coding for TRPV1, IL-6 and TNF-α in MCP/MTP Joints
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Joint Evaluation | Synovial Fluid Evaluation | ELISA | qPCR | |||||
|---|---|---|---|---|---|---|---|---|
| Horse no. | Macroscopic Evaluation (0–56) | WORMS Total (0-154) and Max Regional Score (0–19) | Protein (g/L) | TNCC (×109/L) | Differential Count (% Neutrophils of TNCC) | TRPV1 Concentration (ng/mL) Relative to Total Protein (ng/mL) | TRPV1 mRNA Expression Relative to GAPDH | Group |
| 1 | 0 | 6/2 * | 11 | 0.8 | 1.5 | 5.82 × 10−7 | 0.183 | A |
| 2 | 1 | 8/2 * | 10 | 0.3 | 2.3 | 7.25 × 10−7 | 0.038 | A |
| 3 | 4 | 3/1 * | 4 | 1.6 | 1.2 | 7.92 × 10−7 | 0.269 | B |
| 4 | 8 | 17/5 | 5 | 0.3 | 1.0 | 13.5 × 10−7 | 0.474 | B |
| 5 | 3 | 3/2 | 14 | 3.8 | 2.0 | 14.4 × 10−7 | 0.247 | C |
| 6 | 0 | 6/1 | 9 | 0.9 | 0.0 | 7.20 × 10−7 | 0.045 | A |
| 7 | 1 | 20/10 | 17 | 0.3 | 1.0 | 13.9 × 10−7 | 0.157 | B |
| 8 | 6 | 11/4 | 2 | 0.7 | 2.0 | 15.3 × 10−7 | 0.281 | B |
| 9 | 2 | 11/3 | 14 | 0.9 | 0.0 | 8.71 × 10−7 | 0.104 | B |
| 10 | 4 | 6/2 | 22 | 4.7 | 0.5 | 17.0 × 10−7 | 0.362 | B |
| 11 | 5 | 11/4 | 17 | 1.3 | 1.0 | 12.1 × 10−7 | 0.006 | B |
| 12 | 1 | 6/1 | 1 | 0.4 | 0.0 | 6.71 × 10−7 | 0.006 | A |
| 13 | 2 | 6/2 | 9 | 0.4 | 5.0 ** | 12.2 × 10−7 | 0.193 | A |
| 14 | 8 | 8/2 | 5 | 4.1 | 3.0 | 13.0 × 10−7 | 0.255 | B |
| 15 | 0 | 3/1 | 8 | 0.7 | 2.0 | 12.8 × 10−7 | 0.520 | A |
References
- Ireland, J.L.; Wylie, C.E.; Collins, S.N.; Verheyen KL, P.; Newton, J.R. Preventive health care and owner-reported disease prevalence of horses and ponies in Great Britain. Res. Vet. Sci. 2013, 95, 418–424. [Google Scholar] [CrossRef]
- Nilsson, G. Lameness and pathologic changes in the distal joints and the phalanges of the standardbred horse. A correlative study. Acta Vet. Scnad. Suppl. 1973, 44, 83–96. [Google Scholar]
- McIlwraith, C.W. Current concepts in equine degenerative joint disease. J. Am. Vet. Med. Assoc. 1982, 180, 239–250. [Google Scholar] [PubMed]
- McIlwraith, C.W.; Van Sickle, D.C. Experimentally induced arthritis of the equine carpus: Histological and histochemical changes in the articular cartilage. Am. J. Vet. Res. 1981, 42, 209–217. [Google Scholar] [PubMed]
- Smith, S.B.; Clegg, P. Treatment of equine joint diseases Part 1: Pharmacological management of equine osteoarthritis (OA). Companion Anim. 2007, 12, 9–15. [Google Scholar] [CrossRef]
- McIlwraith, C.W.; Frisbie, D.D.; Kawcak, C.E. Evaluation of intramuscularly administered sodium pentosan polysulfate for treatment of experimentally induced osteoarthritis in horses. Am. J. Vet. Res. 2012, 73, 628–633. [Google Scholar] [CrossRef]
- Watson Levings, R.S.; Smith, A.D.; Broome, T.A.; Rice, B.L.; Gibbs, E.P.; Myara, D.A.; Viktoria Hyddmark, E.; Nasri, E.; Zarezadeh, A.; Levings, P.P.; et al. Self-Complementary Adeno-Associated Virus–Mediated Interleukin-1 Receptor Antagonist Gene Delivery for the Treatment of Osteoarthritis: Test of Efficacy in an Equine Model. Hum. Gen. Ther. Clin. Dev. 2018, 29, 101–112. [Google Scholar] [CrossRef]
- Broeckx, S.Y.; Martens, A.M.; Bertone, A.L.; Van Brantegem, L.; Duchateau, L.; Van Hecke, L.; Dumoulin, M.; Oosterlinck, M.; Chiers, K.; Hussein, H.; et al. The use of equine chondrogenic-induced mesenchymal stem cells as a treatment for osteoarthritis: A randomised, double-blinded, placebo-controlled proof-of-concept study. Equine Vet. J. 2019, 51, 787–794. [Google Scholar] [CrossRef]
- Moses, V.S.; Bertone, A.L. Nonsteroidal anti-inflammatory drugs. Vet. Clin. N. Am. Equine Pract. 2002, 18, 21–37. [Google Scholar] [CrossRef]
- Karcher, L.F.; Dill, S.G.; Anderson, W.I.; King, J.M. Right dorsal colitis. J. Vet. Int. Med. 1990, 4, 247–253. [Google Scholar] [CrossRef]
- Byron, C.R.; Benson, B.M.; Stewart, A.A.; Pondenis, H.C. Effects of methylprednisolone acetate and glucosamine on proteoglycan production by equine chondrocytes in vitro. Am. J. Vet. Res. 2008, 69, 1123–1128. [Google Scholar] [CrossRef] [PubMed]
- Fubini, S.L.; Todhunter, R.J.; Burton-Wurster, N.; Vernier-Singer, M.; Macleod, J.N. Corticosteroids alter the differentiated phenotype of articular chondrocytes. J. Orthop. Res. 2001, 19, 688–695. [Google Scholar] [CrossRef]
- Karsdal, M.A.; Michaelis, M.; Ladel, C.; Siebuhr, A.S.; Bihlet, A.R.; Andersen, J.R.; Guehring, H.; Christiansen, C.; Bay-Jensen, A.C.; Kraus, V.B. Disease-modifying treatments for osteoarthritis (DMOADs) of the knee and hip: Lessons learned from failures and opportunities for the future. Osteoarthr. Cartil. 2016, 24, 2013–2021. [Google Scholar] [CrossRef] [PubMed]
- Wong, G.Y.; Gavva, N.R. Therapeutic potential of vanilloid receptor TRPV1 agonists and antagonists as analgesics: Recent advances and setbacks. Brain Res. Rev. 2009, 60, 267–277. [Google Scholar] [CrossRef]
- Kelly, S. TRPV1 antagonists in the treatment of osteoarthritis pain. Int. J. Clin. Rheum. 2015, 10, 161–175. [Google Scholar] [CrossRef]
- Galindo, T.; Reyna, J.; Weyer, A. Evidence for Transient Receptor Potential (TRP) Channel Contribution to Arthritis Pain and Pathogenesis. Pharmaceuticals 2018, 11, 105. [Google Scholar] [CrossRef] [Green Version]
- Oh, U.; Hwang, S.W.; Kim, D. Capsaicin activates a nonselective cation channel in cultured neonatal rat dorsal root ganglion neurons. J. Neurosci. 1996, 16, 1659–1667. [Google Scholar] [CrossRef] [Green Version]
- Caterina, M.J.; Schumacher, M.A.; Tominaga, M.; Rosen, T.A.; Levine, J.D.; Julius, D. The capsaicin receptor: A heat-activated ion channel in the pain pathway. Nature 1997, 389, 816–824. [Google Scholar] [CrossRef]
- Aneiros, E.; Cao, L.; Papakosta, M.; Stevens, E.B.; Phillips, S.; Grimm, C. The biophysical and molecular basis of TRPV1 proton gating. EMBO J. 2011, 30, 994–1002. [Google Scholar] [CrossRef]
- Baez-Nieto, D.; Alvarez, O.; Brauchi, S.; Gonzalez, C.; Latorre, R. Voltage-Dependence in Thermo-Voltage Sensitive Channel TRPV1. A Delocalized Voltage Sensor? Biophys. J. 2013, 104, 456. [Google Scholar] [CrossRef] [Green Version]
- Ioi, H.; Kido, M.A.; Zhang, J.Q.; Yamaza, T.; Nakata, S.; Nakasima, A.; Tanaka, T. Capsaicin receptor expression in the rat temporomandibular joint. Cell Tissue Res. 2006, 325, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Engler, A.; Aeschlimann, A.; Simmen, B.R.; Michel, B.A.; Gay, R.E.; Gay, S.; Sprott, H. Expression of transient receptor potential vanilloid 1 (TRPV1) in synovial fibroblasts from patients with osteoarthritis and rheumatoid arthritis. Biochem. Biophys. Res. Commun. 2007, 359, 884–888. [Google Scholar] [CrossRef] [PubMed]
- Gavenis, K.; Schumacher, C.; Schneider, U.; Eisfeld, J.; Mollenhauer, J.; Schmidt-Rohlfing, B. Expression of ion channels of the TRP family in articular chondrocytes from osteoarthritic patients: Changes between native and in vitro propagated chondrocytes. Mol. Cell. Biochem. 2008, 321, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Rossi, F.; Siniscalco, D.; Luongo, L.; De Petrocellis, L.; Bellini, G.; Petrosino, S.; Torella, M.; Santoro, C.; Nobili, B.; Perrotta, S.; et al. The endovanilloid/endocannabinoid system in human osteoclasts: Possible involvement in bone formation and resorption. Bone 2009, 44, 476–484. [Google Scholar] [CrossRef] [PubMed]
- Pan, L.; Song, K.; Hu, F.; Sun, W.; Lee, I. Nitric oxide induces apoptosis associated with TRPV1 channel-mediated Ca2+ entry via S-nitrosylation in osteoblasts. Eur. J. Pharmacol. 2013, 715, 280–285. [Google Scholar] [CrossRef]
- Kelly, S.; Chapman, R.J.; Woodhams, S.; Sagar, D.R.; Turner, J.; Burston, J.J.; Bullock, C.; Paton, K.; Huang, J.; Wong, A.; et al. Increased function of pronociceptive TRPV1 at the level of the joint in a rat model of osteoarthritis pain. Ann. Rheum. Dis. 2015, 74, 252–259. [Google Scholar] [CrossRef]
- Fernihough, J.; Gentry, C.; Bevan, S.; Winter, J. Regulation of calcitonin gene-related peptide and TRPV1 in a rat model of osteoarthritis. Neurosci. Lett. 2005, 388, 75–80. [Google Scholar] [CrossRef]
- Barton, N.J.; McQueen, D.S.; Thomson, D.; Gauldie, S.D.; Wilson, A.W.; Salter, D.M.; Chessell, I.P. Attenuation of experimental arthritis in TRPV1R knockout mice. Exp. Mol. Pathol. 2006, 81, 166–170. [Google Scholar] [CrossRef]
- Szabó, Á.; Helyes, Z.; Sandor, K.; Bite, A.; Pinter, E.; Nemeth, J.; Bánvölgyi, A.; Bölcskei, K.; Elekes, K.; Szolcsányi, J. Role of transient receptor potential vanilloid 1 receptors in adjuvant-induced chronic arthritis: In vivo study using gene-deficient mice. J. Pharmacol. Exp. Ther. 2005, 314, 111–119. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, M.; Bjurholm, A.; Srinivasan, G.R.; Lundeberg, T.; Theodorsson, E.; Schultzberg, M.; Kreicbergs, A. Capsaicin effects on substance P and CGRP in rat adjuvant arthritis. Regul. Pept. 1995, 55, 85–102. [Google Scholar] [CrossRef]
- Iadarola, M.J.; Sapio, M.R.; Raithel, S.J.; Mannes, A.J.; Brown, D.C. Long-term pain relief in canine osteoarthritis by a single intra-articular injection of resiniferatoxin, a potent TRPV1 agonist. Pain 2018, 159, 2105–2114. [Google Scholar] [CrossRef] [PubMed]
- Cathcart, C.J.; Johnston, S.A.; Reynolds, L.R.; Al-Nadaf, S.; Budsberg, S.C. Efficacy of ABT-116, an antagonist of transient receptor potential vanilloid type 1, in providing analgesia for dogs with chemically induced synovitis. Am. J. Vet. Res. 2012, 73, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Round, P.; Priestley, A.; Robinson, J. An investigation of the safety and pharmacokinetics of the novel TRPV1 antagonist XEN-D0501 in healthy subjects. Br. J. Clin. Pharmacol. 2011, 72, 921–931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Cunha, A.F.; Stokes, A.M.; Chirgwin, S.; Pettifer, G.; Moore, R.M. Quantitative expression of the TRPV-1 gene in central and peripheral nervous tissue in horses. Int. J. Appl. Res. Vet. Med. 2008, 6, 15–23. [Google Scholar]
- Yaksh, T.L. The Pain State Arising From the Laminitic Horse: Insights Into Future Analgesic Therapies. J. Equine Vet. Sci. 2010, 30, 79–82. [Google Scholar] [CrossRef]
- Brama, P.A.J.; TeKoppele, J.M.; Beekman, B.; Van Weeren, P.R.; Barneveld, A. Matrix metalloproteinase activity in equine synovial fluid: Influence of age, osteoarthritis, and osteochondrosis. Ann. Rheum. Dis. 1998, 57, 697–699. [Google Scholar] [CrossRef]
- McIlwraith, C.W. Synovial fluid analysis in the diagnosis of equine joint disease. Equine Pract. 1980, 2, 44–48. [Google Scholar]
- Trotter, G.W.; McIlwraith, C.W. Clinical features and diagnosis of equine joint disease. In Joint Disease in the Horse; McIlwraith, C.W., Trotter, G.W., Eds.; WB Saunders: Philadelphia, PA, USA, 1996; pp. 120–145. [Google Scholar]
- Bertone, A.L. Infectious Arthritis. In Joint Disease in the Horse; McIlwraith, C.W., Trotter, G.W., Eds.; WB Saunders: Philadelphia, PA, USA, 1996; pp. 397–409. [Google Scholar]
- Smith, A.D.; Morton, A.J.; Winter, M.D.; Colahan, P.T.; Ghivizzani, S.; Brown, M.P.; Hernandez, J.A.; Nickerson, D.M. Magnetic Resonance Imaging Scoring of an Experimental Model of Post-Traumatic Osteoarthritis in the Equine Carpus. Vet. Radiol. Ultrasound 2016, 57, 502–514. [Google Scholar] [CrossRef] [Green Version]
- McIlwraith, C.W.; Frisbie, D.D.; Kawcak, C.E.; Fuller, C.J.; Hurtig, M.; Cruz, A. The OARSI histopathology initiative—Recommendations for histological assessments of osteoarthritis in the horse. Osteoarthr. Cartil. 2010, 18, S93–S105. [Google Scholar] [CrossRef] [Green Version]
- Haneda, S.; Nagaoka, K.; Nambo, Y.; Kikuchi, M.; Nakano, Y.; Matsui, M.; Miyake, Y.; Macleod, J.N.; Imakawa, K. Interleukin-1 receptor antagonist expression in the equine endometrium during the peri-implantation period. Domest. Anim. Endocrinol. 2009, 36, 209–218. [Google Scholar] [CrossRef]
- Iqbal, J.; Bird, J.L.; Hollander, A.P.; Bayliss, M.T. Effect of matrix depleting agents on the expression of chondrocyte metabolism by equine chondrocytes. Res. Vet. Sci. 2004, 77, 249–256. [Google Scholar] [CrossRef] [PubMed]
- GraphPad Prism, Version 8; GraphPad Software: La Joalla, CA, USA, 2018.
- Calzetta, L.; Rogliani, P.; Pistocchini, E.; Mattei, M.; Cito, G.; Alfonsi, P.; Page, C.; Matera, M.G. Effect of lipopolysaccharide on the responsiveness of equine bronchial tissue. Pulmon. Pharmacol. 2018, 49, 88–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warnock, J.J.; Baltzer, W.I.; Duesterdieck-Zellmer, K.; Ott, J. Minimally invasive synovium harvest for potential use in meniscal tissue engineering. Res. Vet. Sci. 2012, 93, 1472–1480. [Google Scholar] [CrossRef]
- Olive, J.; D’anjou, M.A.; Alexander, K.; Laverty, S.; Theoret, C. Comparison of Magnetic Resonance Imaging, Computed Tomography, and Radiography for Assessment of Noncartilaginous Changes in Equine Metacarpophalangeal Osteoarthritis. Vet. Radiol. Ultrasound. 2010, 51, 267–279. [Google Scholar] [CrossRef]
- Olive, J.; D’anjou, M.A.; Girard, C.; Laverty, S.; Theoret, C.L. Imaging and histological features of central subchondral osteophytes in racehorses with metacarpophalangeal joint osteoarthritis. Equine Vet. J. 2009, 41, 859–864. [Google Scholar] [CrossRef]
- Dyson, S.; Nagy, A.; Murray, R. Clinical and diagnostic imaging findings in horses with subchondral bone trauma of the sagittal groove of the proximal phalanx. Vet. Radiol. Ultrasound 2011, 52, 596–604. [Google Scholar] [CrossRef]
- D’anjou, M.A.; Moreau, M.; Troncy, E.; Martel-Pelletier, J.; Abram, F.; Raynauld, J.P.; Pelletier, J.P. Osteophytosis, Subchondral Bone Sclerosis, Joint Effusion and Soft Tissue Thickening in Canine Experimental Stifle Osteoarthritis: Comparison Between 1.5 T Magnetic Resonance Imaging and Computed Radiography. Vet. Surg. 2008, 37, 166–177. [Google Scholar] [CrossRef]
- Gonzalez, L.M.; Schramme, M.C.; Robertson, I.D.; Thrall, D.E.; Redding, R.W. MRI Features of Metacarpo(tarso)phalangeal Region Lameness in 40 Horses. Vet. Radiol. Ultrasound 2010, 51, 404–414. [Google Scholar] [CrossRef]
- King, J.N.; Zubrod, C.J.; Schneider, R.K.; Sampson, S.N.; Roberts, G. MRI Findings in Horses With Lameness Localized to the Metacarpo(tarso)phalangeal Region and Without a Radiographic Diagnosis. Vet. Radiol. Ultrasound 2013, 54, 36–47. [Google Scholar] [CrossRef]
- Powell, S.E. Low-field standing magnetic resonance imaging findings of the metacarpo/metatarsophalangeal joint of racing Thoroughbreds with lameness localised to the region: A retrospective study of 131 horses. Equine Vet. J. 2012, 44, 169–177. [Google Scholar] [CrossRef]
- Zubrod, C.J.; Schneider, R.K.; Tucker, R.L.; Gavin, P.R.; Ragle, C.A.; Farnsworth, K.D. Use of magnetic resonance imaging for identifying subchondral bone damage in horses: 11 cases (1999–2003). J. Am. Vet. Med. Assoc. 2004, 224, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Peterfy, C.G.; Guermazi, A.; Zaim, S.; Tirman PF, J.; Miaux, Y.; White, D.; Kothari, M.; Lu, Y.; Fye, K.; Zhao, S.; et al. Whole-Organ Magnetic Resonance Imaging Score (WORMS) of the knee in osteoarthritis. Osteoarthr. Cartil. 2004, 12, 177–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bautista, D.M. Spicy science: David Julius and the discovery of temperature- sensitive TRP channels. Temperature 2015, 2, 135–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]





| No Joint Pathology (Group A) | Osteoarthritis (Group B) | Arthritis (Group C) |
|---|---|---|
| - Minimum 1 year of age [36] and - No known history of lameness of the limb in question and - Normal synovial fluid analysis (clear yellow, viscous, protein < 20 g/L, TNCC < 1 × 109/L, <10% neutrophils) (adapted from [37]) and - No changes on MRI compatible with chronic arthrosis, i.e., WORMS <10 points and - Osteoarthritic changes graded <4 points during macroscopic evaluation of the joint | - A history of continuous or non-continuous lameness >3 months of the limb in question and/or - Positive MCP/MTP joint block or nerve blocks affecting this joint during the diagnostic work-up and/or - Synovial fluid can have increased TNCC but it should mainly be mononuclear cells, i.e., not compatible with acute arthritis (92) and/or - Changes on MRI compatible with osteoarthritis, i.e., WORMS graded 10 points or above and/or - Osteoarthritic changes graded four points or above during macroscopic evaluation of the joint | - Symptoms (acute lameness, effusion) of 1–7 days’ duration and - Synovial fluid compatible with acute synovitis (TNCC > 1 × 109/L and/or protein >25 g/L) and/or >85% neutrophils in cases with septic arthritis [38,39] and - No changes on MRI compatible with Osteoarthritis, i.e., WORMS <10 points and - Osteoarthritic changes graded <4 points during macroscopic evaluation of the joint |
| TR (ms) | TE (ms) | TI (ms) | Slice Thickness (mm) | FA (°) | FOV (mm) | Echo Train length | Bandwidth (Hz/Px) | Matrix | NEX | Scan Time (min) | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Axial_fse_blade _fatsat | 5000 | 26 | - | 2.5 | 145 | 160 | 9 | 318 | 384 × 384 | 2 | 06:02 |
| Coronal_fse_T1W | 700 | 16 | - | 2.5 | 150 | 160 | 3 | 260 | 224 × 320 | 2 | 02:09 |
| Coronal_fse_T2W _fatsat | 5000 | 61 | - | 2.5 | 150 | 160 | 11 | 220 | 224 × 320 | 2 | 06:42 |
| Coronal_STIR | 4900 | 32 | 220 | 2.5 | 150 | 160 | 10 | 252 | 224 × 320 | 2 | 02:53 |
| Sagittal_fse_PDW | 5000 | 19 | - | 2.5 | 150 | 160 | 8 | 407 | 307 × 384 | 1 | 06:32 |
| Sagittal_fse_T2W | 5300 | 55 | - | 2.5 | 150 | 160 | 8 | 328 | 307 × 384 | 1 | 06:34 |
| T1W_Vibe_ISO _3D | 11.6 | 05:39 | - | 0.6 | 10 | 160 | - | 190 | 256 × 256 | 1 | 03:45 |
| Total Scan Time: | 33:06 |
| Parameter Assessed | 0 | 1 | 2 | 3 | 4 |
|---|---|---|---|---|---|
| High-signal bone lesions (PD-FS and T2-STIR), size | None | <25% of region | 25–50% of region | >50% of region | - |
| High-signal bone lesions (PD-FS and T2-STIR), intensity | None | Mild | Moderate | Marked | - |
| Low-signal bone lesions (PD- and T2-weighted images) | <10% of region | 10–25% of region | 26–50% of region | >50% of region | - |
| Osteophyte formation, size of largest osteophyte in the region | None | <1 mm | 1–2 mm | >2 mm | - |
| Cartilage signal abnormality (SPGR-FS and PD-FS) | No abnormalities | Single lesion <5 mm | Single lesion 5–10 mm or multiple lesions < 5 mm | Single lesion > 10 mm or multiple lesions 5–10 mm | - |
| Subchondral bone irregularity | Smooth and regular chondro-osseus junction | Mild subchondral plate irregularity | Marked subchondral plate irregularity with intact trabecular bone | Bone irregularity extending to the trabecular bone with preservation of some trabecular pattern | Cyst-like formation |
| Type of Pathology Assessed | 0 | 1 | 2 | 3 |
|---|---|---|---|---|
| Wear lines | None | 1 or 2 partial-thickness wear lines | 3–5 partial thickness or 1–2 full-thickness wearlines | >5 partial thickness or >2 full-thickness wear lines |
| Erosions | None | Partial-thickness erosion, <5 mm in diameter | Partial thickness erosion, >5 mm in diameter | Full thickness erosion |
| Primer Name | Forward Primer 5’–3’ | Reverse Primer 5’–3’ | Reference/Accession Number |
|---|---|---|---|
| TRPV1 | TTG AGG ACG GGA AGA ATG AC | GAT GAG CAT GTT GAT CAG GA | Berg, LC/XM_014727972.2 |
| IL-6 | ATG GCA GAA AAA GAC GGA TG | GGG TCA GGG GTG GTT ACT TC | Haneda et al. [42] |
| TNFα | GAG GGA AGA GCA GTT ACC GAA TG | GGC TAC AGG CTT GTC ACT TGG | Berg, LC/NM_001081819.2 |
| GAPDH | GGG TGG AGC CAA AAG GGT CAT CAT | AGC TTT CTC CAG GCG GCA GGT CAG | Iqbal et al. [43] |
| No Joint Pathology (A) | Chronic Arthrosis (B) | Acute Arthritis (C) | |
|---|---|---|---|
| Number of Horses | 6 | 8 | 1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
vom Braucke, A.F.G.; Lysemose Frederiksen, N.; Berg, L.C.; Aarsvold, S.; Müller, F.C.; Ploug Boesen, M.; Lindegaard, C. Identification and Quantification of Transient Receptor Potential Vanilloid 1 (TRPV1) in Equine Articular Tissue. Animals 2020, 10, 506. https://doi.org/10.3390/ani10030506
vom Braucke AFG, Lysemose Frederiksen N, Berg LC, Aarsvold S, Müller FC, Ploug Boesen M, Lindegaard C. Identification and Quantification of Transient Receptor Potential Vanilloid 1 (TRPV1) in Equine Articular Tissue. Animals. 2020; 10(3):506. https://doi.org/10.3390/ani10030506
Chicago/Turabian Stylevom Braucke, Anne Frank Gallagher, Nanna Lysemose Frederiksen, Lise Charlotte Berg, Stacie Aarsvold, Felix Christoph Müller, Mikael Ploug Boesen, and Casper Lindegaard. 2020. "Identification and Quantification of Transient Receptor Potential Vanilloid 1 (TRPV1) in Equine Articular Tissue" Animals 10, no. 3: 506. https://doi.org/10.3390/ani10030506
APA Stylevom Braucke, A. F. G., Lysemose Frederiksen, N., Berg, L. C., Aarsvold, S., Müller, F. C., Ploug Boesen, M., & Lindegaard, C. (2020). Identification and Quantification of Transient Receptor Potential Vanilloid 1 (TRPV1) in Equine Articular Tissue. Animals, 10(3), 506. https://doi.org/10.3390/ani10030506