
Double-Outlet Right Ventricle in a Chianina Calf


{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials, Methods and Results
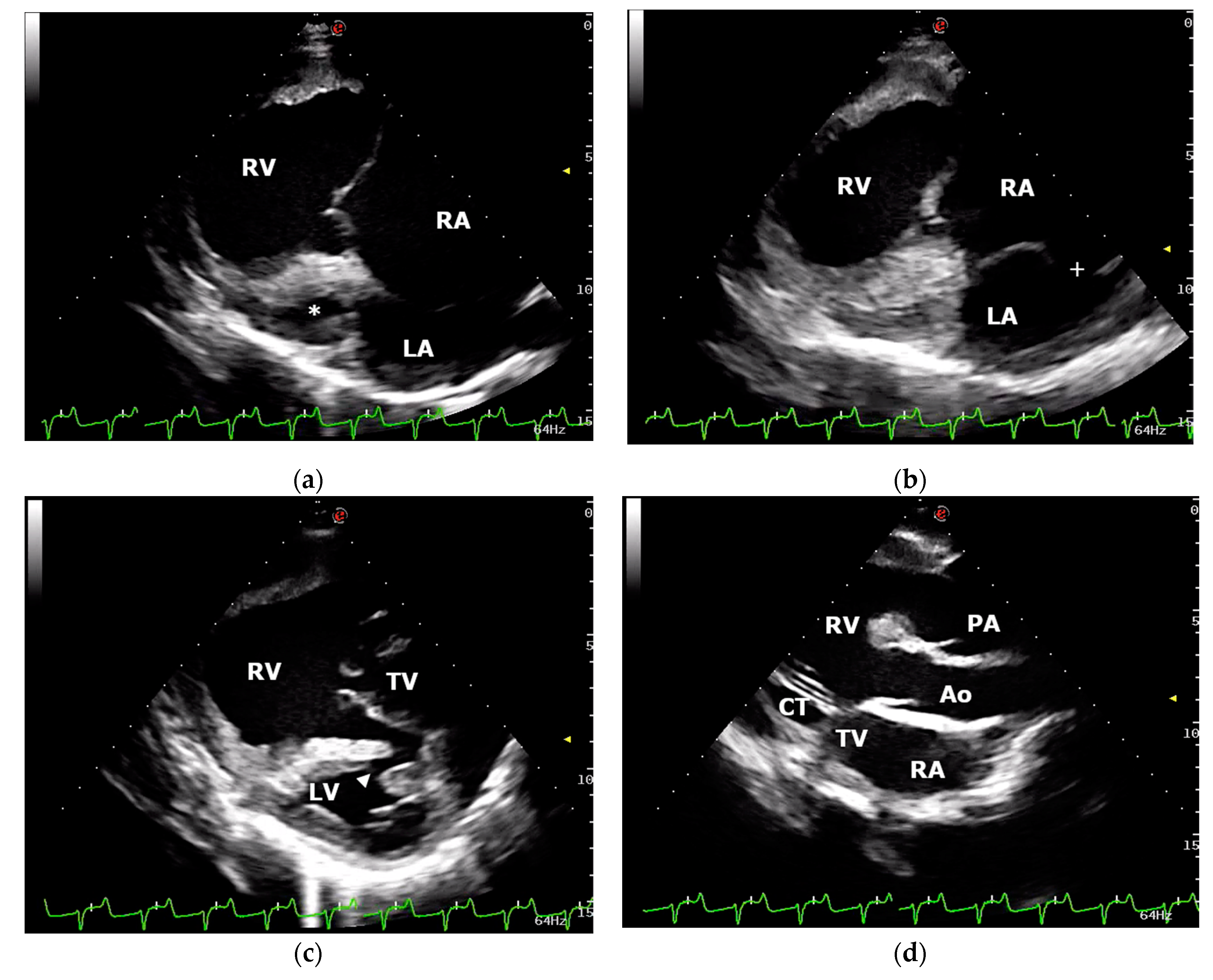
2.1. Case Description and Clinical Investigations
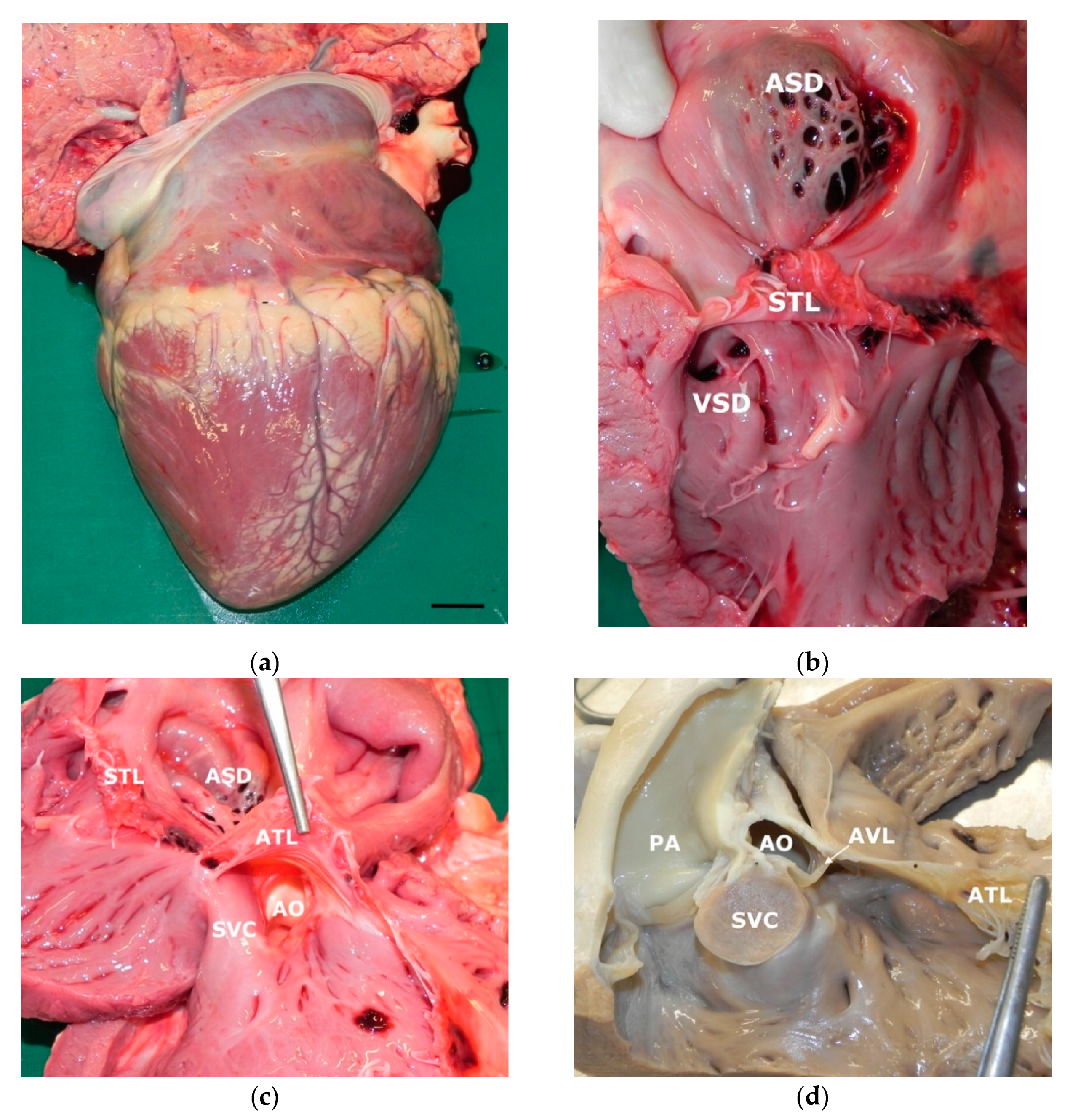
2.2. Gross Examination and Histopathology
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kemler, A.G.; Martin, J.E. Incidence of congenital cardiac defects in bovine fetuses. Am. J. Vet. Res. 1972, 33, 249–251. [Google Scholar]
- Buczinski, S.; Fecteau, G.; DiFruscia, R. Ventricular septal defects in cattle: A retrospective study of 25 cases. Can. Vet. J. 2006, 47, 246–252. [Google Scholar]
- Buczinski, S. Cardiovascular ultrasonography in cattle. Vet. Clin. N. Am. Food Anim. Pract. 2009, 25, 611–632. [Google Scholar] [CrossRef]
- Buczinski, S.; Rezakhani, A.; Boerboom, D. Heart disease in cattle: Diagnosis, therapeutic approaches and prognosis. Vet. J. 2010, 184, 258–263. [Google Scholar] [CrossRef]
- Murakami, T.; Hagio, M.; Hamana, K.; Moritomo, Y. Morphology of the Atrial Septal Defect in Cattle. J. Jpn. Vet. Med. Assoc. 1991, 44, 696–699. [Google Scholar] [CrossRef] [Green Version]
- Wilson, R.B.; Cave, J.S.; Horn, J.B.; Kasselberg, A.G. Double outlet right ventricle in a calf. Can. J. Comp. Med. 1985, 49, 115–116. [Google Scholar]
- Prosek, R.; Oyama, M.A.; Church, W.M.; Nagy, D.W.; Sisson, D.D. Double-outlet right ventricle in an Angus calf. J. Vet. Intern. Med. 2005, 19, 262–267. [Google Scholar] [CrossRef]
- Nourani, H.; Parchami, A.; Bonyadian, M. Double outlet right ventricle in a calf. Comp. Clin. Pathol. 2009, 18, 187–189. [Google Scholar] [CrossRef]
- Newhard, D.K.; Jung, S.W.; Winter, R.L.; Kuca, T.; Bayne, J.; Passler, T. Double-outlet right ventricle with an intact interventricular septum and concurrent hypoplastic left ventricle in a calf. J. Vet. Cardiol. 2017, 19, 205–210. [Google Scholar] [CrossRef]
- McManus, A.; Moloney, T.; Kelly, P.; Rowan, C.; Skelly, C.; McAloon, C.I. An unusual presentation of developmental anomalies of the cardiovascular system including tetralogy of fallot, double outlet right ventricle, patent foramen ovale and persistent right aortic arch in a Friesian calf. Vet. Res. 2020, 16, 224–230. [Google Scholar] [CrossRef]
- Testoni, S.; Boni, P.; Gentile, A. Congenital pseudomyotonia in Chianina cattle. Vet. Rec. 2008, 163, 252. [Google Scholar] [CrossRef]
- Sacchetto, R.; Testoni, S.; Gentile, A.; Damiani, E.; Rossi, M.; Liguori, R.; Drögemüller, C.; Mascarello, F. A defective SERCA1 protein is responsible for congenital pseudomyotonia in Chianina cattle. Am. J. Pathol. 2009, 174, 565–573. [Google Scholar] [CrossRef] [Green Version]
- Murgiano, L.; Testoni, S.; Drögemüller, C.; Bolcato, M.; Gentile, A. Frequency of bovine congenital pseudomyotonia carriers in selected Italian Chianina sires. Vet. J. 2013, 195, 238–240. [Google Scholar] [CrossRef]
- Bianchini, E.; Testoni, S.; Gentile, A.; Calì, T.; Ottolini, D.; Villa, A.; Brini, M.; Betto, R.; Mascarello, F.; Nissen, P.; et al. Inhibition of ubiquitin proteasome system rescues the defective sarco(endo)plasmic reticulum Ca2+-ATPase (SERCA1) protein causing Chianina cattle pseudomyotonia. J. Biol. Chem. 2014, 289, 33073–33082. [Google Scholar] [CrossRef] [Green Version]
- Molteni, L.; Dardano, S.; Parma, P.; Polli, M.; De Giovanni, A.M.; Sironi, G.; Longeri, M. Ichthyosis in Chianina cattle. Vet. Rec. 2006, 158, 412–414. [Google Scholar] [CrossRef]
- Ho, S.Y.; Rigby, M.L.; Anderson, R.H. Echocardiography in Congenital Heart Disease Made Simple, 1st ed.; Imperial College Press: London, UK, 2005; pp. 67–75. [Google Scholar]
- Digilio, M.C.; Casey, B.; Toscano, A.; Calabro, R.; Pacileo, G.; Marasini, M.; Banaudi, E.; Giannotti, A.; Dallapiccola, B.; Marino, B. Complete transposition of the great arteries. Patterns of congenital heart disease in familial precurrence. Circulation 2001, 104, 2809–2814. [Google Scholar] [CrossRef] [Green Version]
- Schrope, D.P. Prevalence of congenital heart disease in 76,301 mixed-breed dogs and 57,025 mixed-breed cats. J. Vet. Cardiol. 2015, 17, 192–202. [Google Scholar] [CrossRef]
- Tidholm, A.; Ljungvall, I.; Michal, J.; Haĝgström, J.; Höglund, K. Congenital heart defects in cats: A retrospective study of 162 cats (1996–2013). J. Vet. Cardiol. 2015, 17, 215–219. [Google Scholar] [CrossRef]
- Gopal, T.; Leipold, H.W.; Dennis, S.M. Congenital cardiac defects in calves. Am. J. Vet. Res. 1986, 47, 1120–1121. [Google Scholar]
- Chaffin, M.K.; Miller, M.W.; Morris, E.L. Double outlet right ventricle and other associated congenital cardiac anomalies in an American miniature horse foal. Equine Vet. J. 1992, 24, 402–406. [Google Scholar] [CrossRef]
- Stieger-Vanegas, S.M.; Scollan, K.F.; Meadows, L.; Sisson, D.; Schlipf, J.; Riebold, T.; Löhr, C.V. Cardiac-gated computed tomography angiography in three alpacas with complex congenital heart disease. J. Vet. Cardiol. 2016, 18, 88–98. [Google Scholar] [CrossRef]
- Obler, D.; Juraszek, A.L.; Smoot, L.B.; Natowicz, M.R. Double outlet right ventricle: Aetiologies and associations. J. Med. Genet. 2008, 45, 481–497. [Google Scholar] [CrossRef] [Green Version]
- Cetta, F.; Boston, U.S.; Dearani, J.A.; Hagler, D.J. Double outlet right ventricle: Opinions regarding management. Curr. Treat. Options Cardiovasc. Med. 2005, 7, 385–390. [Google Scholar] [CrossRef]
- Walters, H.; Mavroudis, C.; Tchervenkov, C.; Jacobs, J.; LacourGayet, F.; Jacobs, M. Congenital heart surgery nomenclature and database project: Double outlet right ventricle. Ann. Thorac. Surg. 2000, 69, 249–263. [Google Scholar] [CrossRef]
- Mahle, W.T.; Martinez, R.; Silverman, N.; Cohen, M.S.; Anderson, R.H. Anatomy, echocardiography, and surgical approach to double outlet right ventricle. Cardiol. Young 2008, 18, 39–51. [Google Scholar] [CrossRef]
- van der Linde-Sipman, J.S. Hypoplasia of the left ventricle in four ruminants. Vet. Pathol. 1978, 15, 474–480. [Google Scholar] [CrossRef]
- Fennell, L.; Church, S.; Tyrell, D.; Forbes, G.; Charles, J.; McCowan, C.; Savage, C. Double-outlet right ventricle in a 10-month-old Friesian filly. Aust. Vet. J. 2009, 87, 204–209. [Google Scholar] [CrossRef]
- Abduch, M.C.; Tonini, P.L.; de Oliveira, D.; Barbusci, L.; de Oliveira, S.M.; de Freitas, R.R.; Aiello, V.D. Double-outlet right ventricle associated with discordant atrioventricular connection and dextrocardia in a cat. J. Small Anim. Pract. 2003, 44, 374–377. [Google Scholar] [CrossRef]
- Jeraj, K.; Ogburn, P.N.; Jessen, C.A.; Miller, J.D.; Schenk, M.P. Double outlet right ventricle in a cat. J. Am. Vet. Med. Assoc. 1978, 173, 1356–1360. [Google Scholar]
- Northway, R.B. Use of an aortic homograft for surgical correction of a double-outlet right ventricle in a kitten. Vet. Med. Small Anim. Clin. 1979, 74, 191–192. [Google Scholar]
- Reef, V.B.; McGuirk, S.M. Diseases of the cardiovascular system. In Large Animal Internal Medicine, 5th ed.; Smith, B.P., Ed.; Elsevier Mosby: St. Louis, MO, USA, 2015; pp. 427–460. [Google Scholar]
- Sandusky, G.E.; Smith, C.W. Congenital cardiac anomalies in calves. Vet. Rec. 1981, 108, 163–165. [Google Scholar] [CrossRef]
- Mitchell, K.J.; Schwarzwald, C.C. Echocardiography for the Assessment of Congenital Heart Defects in Calves. Vet. Clin. N. Am. Food Anim. Pract. 2016, 32, 37–54. [Google Scholar] [CrossRef]
- Suzuki, K.; Uchida, E.; Schober, K.E.; Niehaus, A.; Rings, M.D.; Lakritz, J. Cardiac troponin I in calves with congenital heart disease. J. Vet. Intern. Med. 2012, 26, 1056–1060. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caivano, D.; Marchesi, M.C.; Boni, P.; Venanzi, N.; Angeli, G.; Porciello, F.; Lepri, E. Double-Outlet Right Ventricle in a Chianina Calf. Animals 2021, 11, 318. https://doi.org/10.3390/ani11020318
Caivano D, Marchesi MC, Boni P, Venanzi N, Angeli G, Porciello F, Lepri E. Double-Outlet Right Ventricle in a Chianina Calf. Animals. 2021; 11(2):318. https://doi.org/10.3390/ani11020318
Chicago/Turabian StyleCaivano, Domenico, Maria Chiara Marchesi, Piero Boni, Noemi Venanzi, Giovanni Angeli, Francesco Porciello, and Elvio Lepri. 2021. "Double-Outlet Right Ventricle in a Chianina Calf" Animals 11, no. 2: 318. https://doi.org/10.3390/ani11020318
APA StyleCaivano, D., Marchesi, M. C., Boni, P., Venanzi, N., Angeli, G., Porciello, F., & Lepri, E. (2021). Double-Outlet Right Ventricle in a Chianina Calf. Animals, 11(2), 318. https://doi.org/10.3390/ani11020318