
The Comparison of Latero-Medial versus Dorso-Palmar/Plantar Drilling for Cartilage Removal in the Proximal Interphalangeal Joint

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Animals
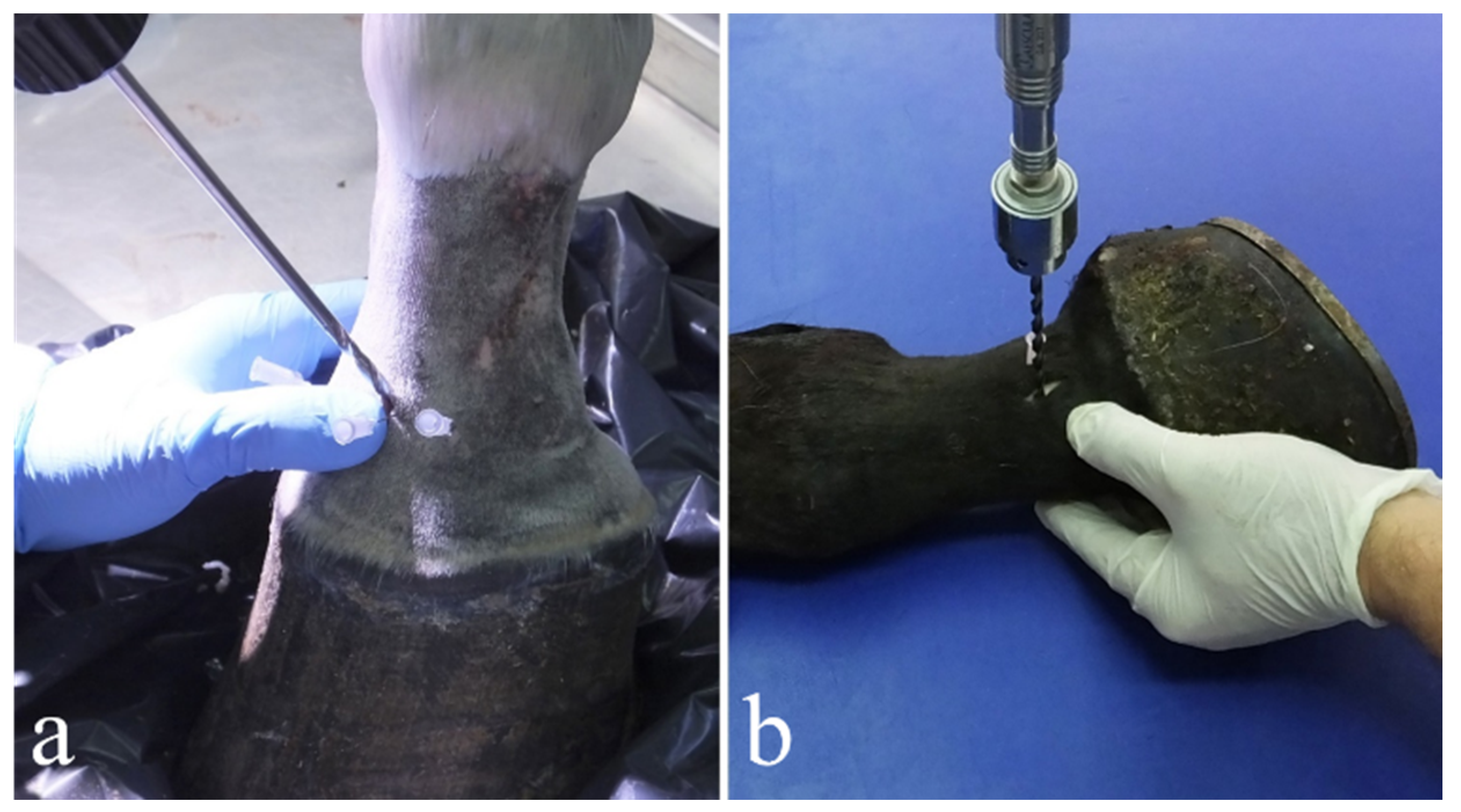
2.2. Dorsal Drilling Approach
2.3. Lateral Drilling Approach
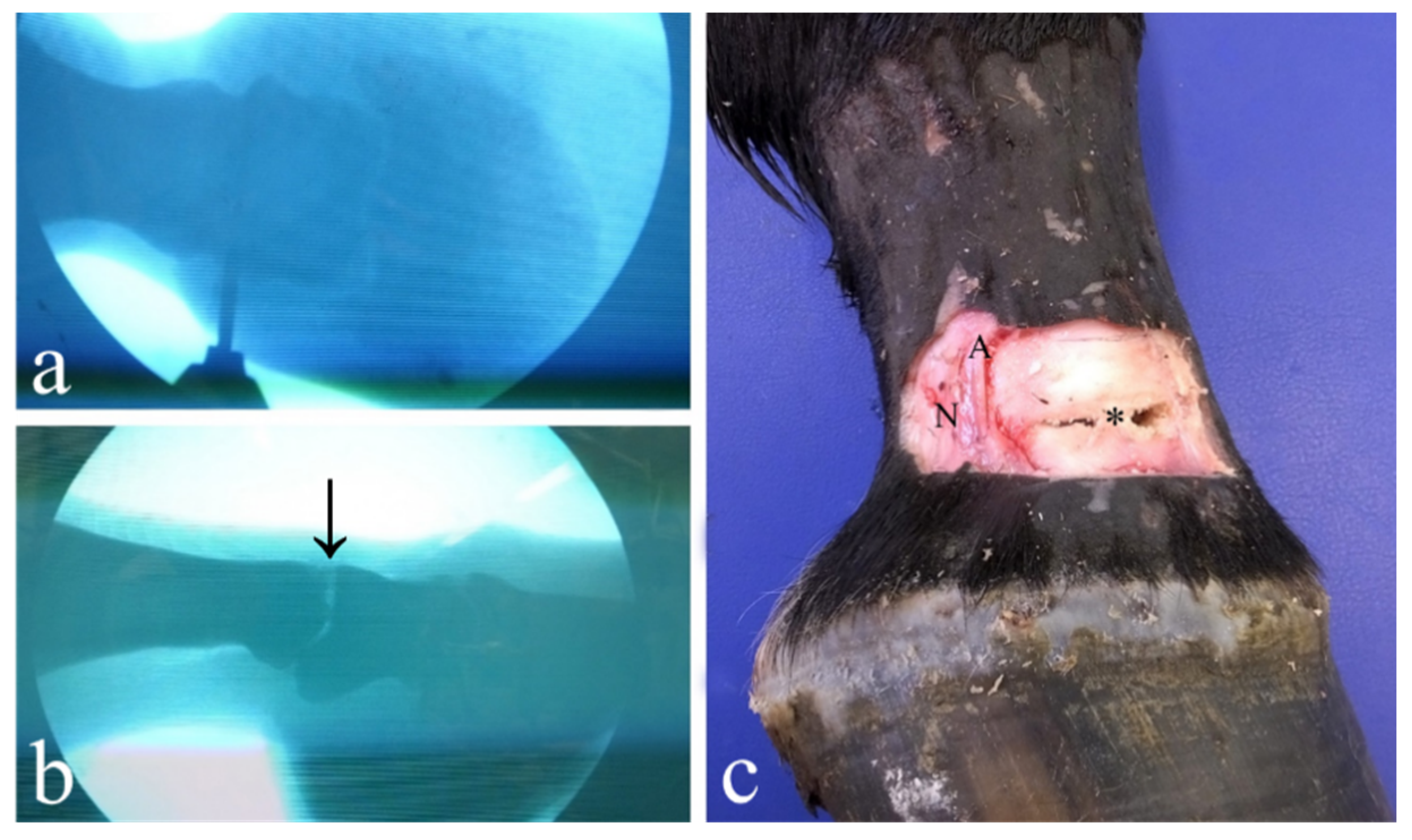
2.4. Lateral Drilling Approach under Digital Fluoroscopy
2.5. Measurements
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Knox, P.M.; Watkins, J.P. Proximal interphalangeal joint arthrodesis using a combination plate-screw technique in 53 horses (1994–2003). Equine Vet. J. 2006, 38, 538–542. [Google Scholar] [CrossRef] [PubMed]
- Jones, P.; Delco, M.; Beard, W.; Lillich, J.D.; Desormaux, A. A limited surgical approach for pastern arthrodesis in horses with severe osteoarthritis. Vet. Comp. Orthop. Traumatol. 2009, 22, 303–308. [Google Scholar] [PubMed]
- Lischer, C.J.; Auer, J.A. Arthrodesis techniques. In Equine Surgery, 5th ed.; W.B. Saunders Company: Philadelphia, PA, USA, 2019; pp. 1374–1398. [Google Scholar]
- Caston, S.; McClure, S.; Beug, J.; Kersh, K.; Reinertson, E.; Wang, C. Retrospective evaluation of facilitated pastern ankylosis using intra-articular ethanol injections: 34 cases (2006–2012). Equine Vet. J. 2013, 45, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Schaer, T.P.; Bramlage, L.R.; Embertson, R.M.; Hance, S. Proximal interphalangeal arthrodesis in 22 horses. Equine. Vet. J. 2001, 33, 360–365. [Google Scholar] [CrossRef] [PubMed]
- Zubrod, C.J.; Schneider, R.K. Arthrodesis techniques in horses. Vet. Clin. N. Am. Equine Pract. 2005, 21, 691–711. [Google Scholar] [CrossRef]
- Schneider, J.E.; Carnine, B.L.; Guffy, M.M. Arthrodesis of the proximal interphalangeal joint in the horse: A surgical treatment of high ringbone. J. Am. Vet. Med. Assoc. 1978, 173, 1364–1369. [Google Scholar]
- Watkins, J.P. Arthrodesis of the Proximal Interphalangeal Joint. In Equine Fracture Repair, 2nd ed.; Nixon, A.J., Ed.; John Wiley and Sons, Inc.: Hoboken, NJ, USA, 2020; pp. 277–294. [Google Scholar]
- Genetzky, R.M.; Schneider, E.J.; Butler, H.C.; Guffy, M.M. Comparison of two surgical procedures for arthrodesis of the proximal interphalangeal joint in horses. J. Am. Vet. Med. Assoc. 1981, 179, 464–468. [Google Scholar]
- Caron, J.P.; Fretz, P.B.; Bailey, J.V.; Barber, S.M. Proximal interphalangeal joint arthrodesis in the horse: A retrospective study and modified screw technique. Vet. Surg. 1990, 19, 196–202. [Google Scholar] [CrossRef]
- Steenhaut, M.; Verschooten, F.; De Moor, A. Arthrodesis of the pastern joint in the horse. Equine Vet. J. 1985, 17, 35–40. [Google Scholar] [CrossRef]
- Zamos, D.T.; Honnas, C.M. Principles and applications of arthrodesis in horses. Compend. Contin. Educ. Pract. Vet. 1993, 15, 1533–1541. [Google Scholar]
- Zert, Z.; Krisova, S.; Zuffova, K. Pastern joint arthrodesis using two paraaxial and one axial crossed lag screws: A case report. Vet. Med. 2013, 58, 322–326. [Google Scholar] [CrossRef] [Green Version]
- Watt, B.C.; Edwards, R.B.; Markel, M.D.; McCabe, R.; Wilson, D.G. Arthrodesis of the equine proximal interphalangeal joint: A biomechanical comparison of three 4.5 mm and two 5.5 mm cortical screws. Vet. Surg. 2001, 20, 287–294. [Google Scholar] [CrossRef]
- Read, E.K.; Chandler, D.; Wilson, D.G. Arthrodesis of the equine proximal interphalangeal joint: A mechanical comparison of 2 parallel 5.5 mm cortical screws and 3 parallel 5.5 mm cortical screws. Vet. Surg. 2005, 34, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Sod, G.A.; Riggs, L.M.; Mitchell, C.F.; Hubert, J.D.; George, S.; Martin, G.S. An in vitro biomechanical comparison of equine proximal interphalangeal joint arthrodesis techniques: An axial positioned dynamic compression plate and two abaxial transarticular cortical screws inserted in lag fashion versus three parallel transarticular cortical screws inserted in lag fashion. Vet. Surg. 2010, 39, 83–90. [Google Scholar] [PubMed]
- Watt, B.C.; Edwards, R.B., III; Markel, M.D.; McCabe, R.; Wilson, D.G. Arthrodesis of the equine proximal interphalangeal joint: A biomechanical comparison of two 7-hole 3.5 mm broad and two 5-hole 4.5 mm narrow dynamic compression plates. Vet. Surg. 2002, 31, 85–93. [Google Scholar] [CrossRef] [PubMed]
- James, F.M.; Richardson, D.W. Minimally invasive plate fixation of lower limb injury in horses: 32 cases (1999–2003). Equine Vet. J. 2006, 38, 246–251. [Google Scholar] [CrossRef]
- Galuppo, L.D.; Stover, S.M.; Willits, N.H. A biomechanical comparison of double-plate and Y-plate fixation for comminuted equine second phalangeal fractures. Vet. Surg. 2000, 29, 152–162. [Google Scholar] [CrossRef]
- Richardson, D.W. Less invasive techniques for equine fracture repair and arthrodesis. Vet. Clin. N. Am. Equine Pract. 2008, 24, 177–189. [Google Scholar] [CrossRef]
- Wolker, R.E.; Carmalt, J.L.; Wilson, D.G. Arthrodesis of the equine proximal interphalangeal joint: A biomechanical comparison of two parallel headless, tapered, variable pitched, titanium compression screws and two parallel 5.5 mm stainless steel cortical screws. Vet. Surg. 2009, 38, 861–886. [Google Scholar] [CrossRef]
- Sakai, R.R.; Goodrich, L.R.; Katzman, S.A.; Moorman, V.J.; Leise, B.S.; Kawcak, C.E.; Galuppo, L.D. Use of a locking compression plate for equine proximal interphalangeal joint arthrodesis: 29 cases (2008–2014). J. Am. Vet. Med. Assoc. 2018, 253, 1460–1466. [Google Scholar] [CrossRef]
- Vidović, A.; Jansen, D.; Schwan, S.; Goldstein, A.; Ludtka, C.; Brehm, W. Arthrodesis of the equine proximal interphalangeal joint: A biomechanical comparison of 2 different LCP systems. Tierärztl. Prax. Ausg. G. Großtiere/Nutztiere. 2020, 48, 25–34. [Google Scholar] [CrossRef]
- Heaton, K.; Farnsworth, K.D.; Souza, C.R.; Jones, A.R. A Standing Percutaneous Technique for Proximal Interphalangeal Joint Arthrodesis in Twelve Horses (2014–2017). Vet. Comp. Orthop. Traumatol. 2019, 32, 165–170. [Google Scholar] [PubMed]
- Bras, J.J.; Lillich, J.D.; Beard, W.L.; Anderson, D.E.; Armbrust, L.J.; Frink, E.; Lease, K. Effect of a collateral ligament sparing surgical approach on mechanical properties of equine proximal interphalangeal joint arthrodesis constructs. Vet. Surg. 2011, 40, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Von Salis, B. Arthrodesis of the pastern joint in horses. Tijdschr. Diergeneesk. 1973, 98, 1030–1031. [Google Scholar]
- Johnson, J.E. Ringbone: Treatment by ankylosis. Proc. Annu. Gen. Meet. Am. Assoc. Equine Pract. 1974, 20, 67–80. [Google Scholar]
- Penraat, J.; Allen, A.; Fretz, P.; Bailey, L.V. An evaluation of chemical arthrodesis of the proximal interphalangeal joint in the horse by using monoiodoacetate. Can. J. Vet. Res. 2000, 64, 212–221. [Google Scholar] [PubMed]
- Watts, A.E.; Fortier, L.A.; Nixon, A.J.; Ducharme, N.G. A technique for laser facilitated equine pastern arthrodesis using parallel screws inserted in lag fashion. Vet. Surg. 2010, 39, 244–253. [Google Scholar] [CrossRef]
- Wolker, R.R.; Wilson, D.G.; Allen, A.L.; Carmalt, J.L. Evaluation of ethyl alcohol for use in a minimally invasive technique for equine proximal interphalangeal joint arthrodesis. Vet. Surg. 2011, 40, 291–298. [Google Scholar] [CrossRef]
- Hague, B.A.; Guccione, A. Laser-facilitated arthrodesis of the distal tarsal joints. Clin. Tech. Equine Pract. 2002, 1, 32–35. [Google Scholar] [CrossRef]
- Lauge-Pedersen, H.; Knutson, K.; Rydholm, U. Percutaneous ankle arthrodesis in the rheumatoid patient without debridement of the joint. Foot 1998, 8, 226–229. [Google Scholar] [CrossRef]
- Lauge-Pedersen, H.; Aspenberg, P. Arthrodesis by percutaneous fixation: Patellofemoral arthrodesis in rabbits without debridement of the joint. Acta Orthop. Scand. 2002, 73, 186–189. [Google Scholar] [CrossRef] [Green Version]
- Oosterlinck, M.; Pille, F.; Gasthuys, F.; Saunders, J.H. Spontaneous bilateral ankylosis of the carpometacarpal joint in a Paint Horse. Equine Vet. Educ. 2009, 21, 452–454. [Google Scholar] [CrossRef]
- Peroni, J. ANK-ylosis: A molecular basis for progressive joint fusion. Equine Vet. Educ. 2009, 21, 455. [Google Scholar] [CrossRef]
- MacLellan, K.; Crawford, W.; MacDonald, D. Proximal interphalangeal joint arthrodesis in 34 horses using two parallel 5.5-mm cortical bone screws. Vet. Surg. 2001, 30, 454–459. [Google Scholar] [CrossRef] [PubMed]
- Dechant, J.E.; Baxter, G.M.; Southwood, L.L.; Crawford, W.H.; Jackman, B.R.; Stashak, T.S.; Trotter, G.W.; Hendrickson, D.A. Use of a three-drill-tract technique for arthrodesis of the distal tarsal joints in horses with distal tarsal osteoarthritis: 54 cases (1990–1999). J. Am. Vet. Med. Assoc. 2003, 223, 1800–1805. [Google Scholar] [CrossRef]
- Lang, H.M.; Panizzi, L.; Allen, A.L.; Woodbury, M.R.; Barber, S.M. Comparison of three drilling techniques for carpometacarpal joint arthrodesis in horses. Vet. Surg. 2009, 38, 990–997. [Google Scholar] [CrossRef]
- Seo, J.P.; Yamaga, T.; Tsuzuki, N.; Yamada, K.; Haneda, S.; Furuoka, H.; Tabata, Y.; Sasaki, N. Minimally invasive proximal interphalangeal joint arthrodesis using a locking compression plate and tissue engineering in horses: A pilot study. Can. Vet. J. 2014, 55, 1050–1056. [Google Scholar]
- Kuemmerle, J.M.; Berchtold, S. Area of cartilage accessible to curettage for subsequent arthrodesis of the equine proximal interphalangeal joint. Vet. Comp. Orthop. Traumatol. 2013, 26, 489–492. [Google Scholar]
- Bignozzi, L.; Spadari, A.; Pigato, M. Pastern joint arthrodesis: A varying technique in comparison to the classique one in the horse. Atti Della Società Italiana di Scienze Veterinarie 1993, 48, 2345–2349. [Google Scholar]
- Van Hecke, L.L.; Oosterlinck, M.; Pille, F.J.; Martens, A.M. Minimally invasive surgical pastern arthrodesis: An ex vivo study comparing three different drilling techniques for cartilage destruction. J. Equine Vet. Sci. 2014, 34, 1003–1008. [Google Scholar] [CrossRef]
- Siegler, S.; Block, J.; Schneck, C. The mechanical characteristics of the collateral ligaments of the human ankle joint. Foot Ankle 1988, 8, 234–242. [Google Scholar] [CrossRef] [PubMed]
- Bramlage, L.R. Arthrodesis of the Metacarpo/Metatarsophalangeal Joint. In Equine Fracture Repair, 2nd ed.; Nixon, A.J., Ed.; John Wiley and Sons, Inc.: Hoboken, NJ, USA, 2020; Volume 28, pp. 425–435. [Google Scholar]
- Lescun, T.B. Minimally invasive pastern arthrodesis in the horse. In Proceedings of the 2008 Annual Meeting of the American College of Veterinary Surgeons, San Diego, CA, USA, 23–25 October 2008; pp. 50–53. [Google Scholar]
- Martin, G.S.; McIlwraith, C.W.; Turner, A.S.; Nixon, A.J.; Stashak, T.S. Long-term results and complications of proximal interphalangeal arthrodesis in horses. J. Am. Vet. Med. Assoc. 1984, 184, 1136–1140. [Google Scholar] [PubMed]
- McIlwraith, C.W.; Turner, A.S. Equine Surgery, Advanced Techniques; Lea and Febiger: Philadelphia, PA, USA, 1987; pp. 179–184. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drilling Approach | Forelimb | |||||||
|---|---|---|---|---|---|---|---|---|
| Proximal Articular Surface (Distal P1) | Distal Articular Surface (Proximal P2) | % of Total PIPJ Erosion | p Value | |||||
| Total Area | Eroded Area | % of Removed Cartilage | Total Area | Eroded Area | % of Removed Cartilage | |||
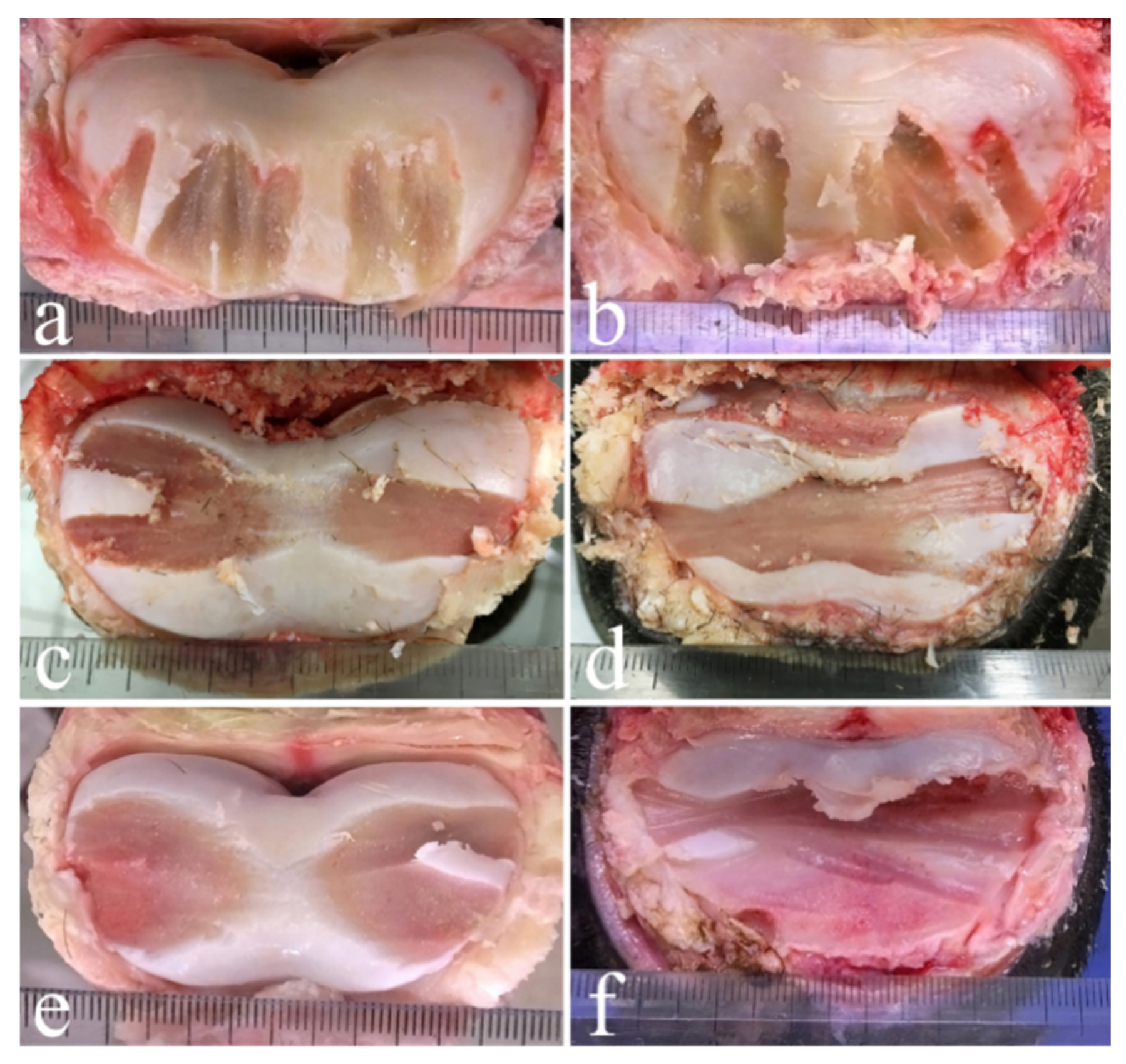
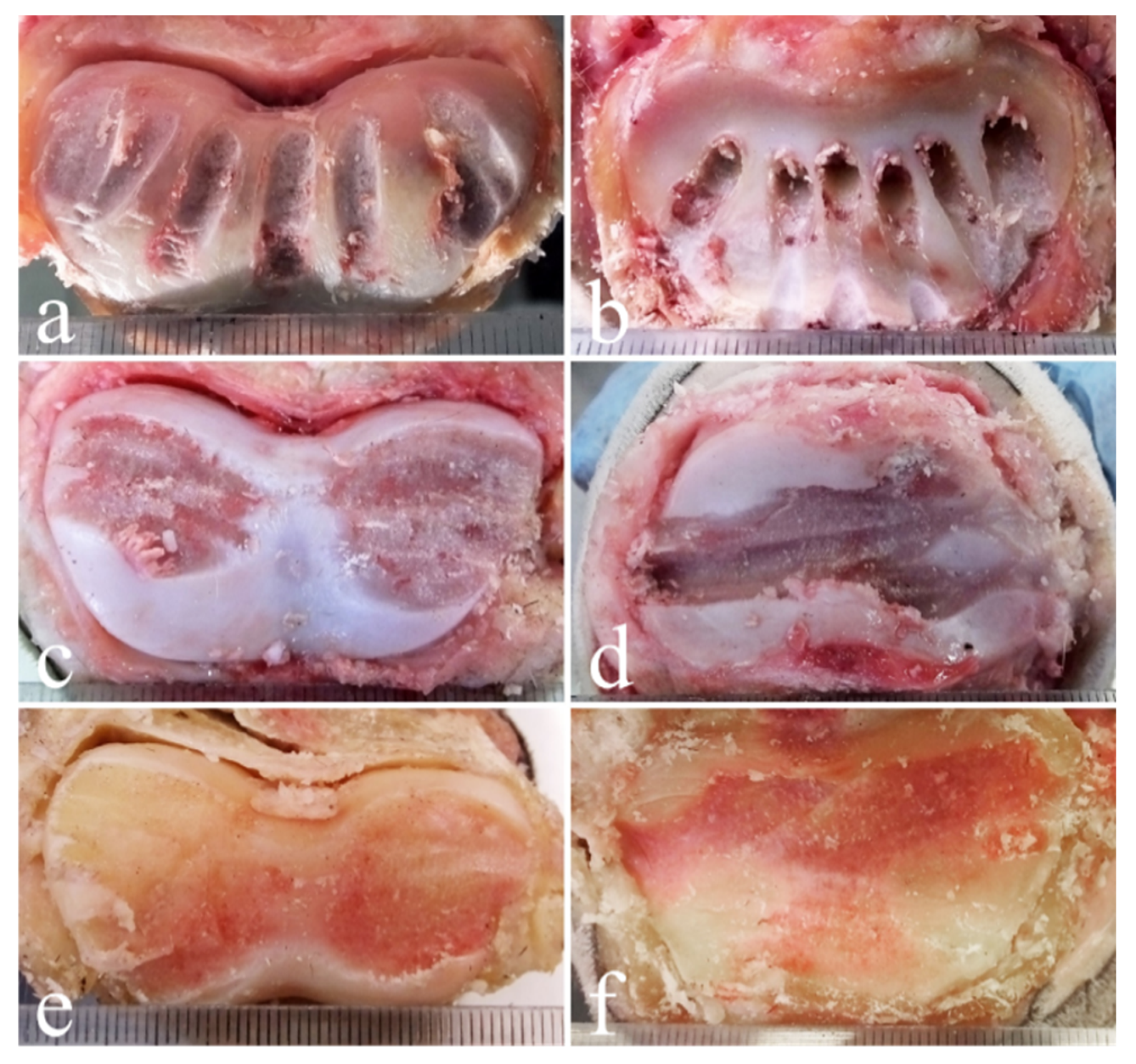
| Dorsal | 12 ± 3 | 4 ± 1 | 30 ± 10 | 14 ± 2 | 4 ± 1 | 25 ± 8 | 27 ± 8 | 0.00712 |
| Lateral without digital fluoroscopy | 12 ± 2 | 4 ± 2 | 33 ± 11 | 13 ± 2 | 5 ± 2 | 34 ± 13 | 34 ± 12 | |
| Lateral under digital fluoroscopy | 14 ± 4 | 6 ± 2 | 43 ± 16 | 14 ± 3 | 6 ± 2 | 48 ± 20 | 45 ± 12 | |
| Drilling Approach | Hindlimb | |||||||
|---|---|---|---|---|---|---|---|---|
| Proximal Articular Surface (Distal P1) | Distal Articular Surface (Proximal P2) | % of Total PIPJ Erosion | p Value | |||||
| Total Area | Eroded Area | % of Removed Cartilage | Total Area | Eroded Area | % of Removed Cartilage | |||
| Dorsal | 11 ± 3 | 3 ± 7 | 28 ± 8 | 12 ± 2 | 3 ± 1 | 29 ± 5 | 28 ± 6 | 0.00962 |
| Lateral without digital fluoroscopy | 13 ± 3 | 5 ± 1 | 38 ± 10 | 13 ± 2 | 6 ± 2 | 45 ± 9 | 41 ± 9 | |
| Lateral under digital fluoroscopy | 13 ± 3 | 8 ± 2 | 61 ± 9 | 12 ± 3 | 8 ± 3 | 61 ± 24 | 64 ± 11 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spadari, A.; Forni, G.; Del Magno, S.; Tagliavia, C.; Canova, M.; Grandis, A.; Rinnovati, R. The Comparison of Latero-Medial versus Dorso-Palmar/Plantar Drilling for Cartilage Removal in the Proximal Interphalangeal Joint. Animals 2021, 11, 1838. https://doi.org/10.3390/ani11061838
Spadari A, Forni G, Del Magno S, Tagliavia C, Canova M, Grandis A, Rinnovati R. The Comparison of Latero-Medial versus Dorso-Palmar/Plantar Drilling for Cartilage Removal in the Proximal Interphalangeal Joint. Animals. 2021; 11(6):1838. https://doi.org/10.3390/ani11061838
Chicago/Turabian StyleSpadari, Alessandro, Giulia Forni, Sara Del Magno, Claudio Tagliavia, Marco Canova, Annamaria Grandis, and Riccardo Rinnovati. 2021. "The Comparison of Latero-Medial versus Dorso-Palmar/Plantar Drilling for Cartilage Removal in the Proximal Interphalangeal Joint" Animals 11, no. 6: 1838. https://doi.org/10.3390/ani11061838
APA StyleSpadari, A., Forni, G., Del Magno, S., Tagliavia, C., Canova, M., Grandis, A., & Rinnovati, R. (2021). The Comparison of Latero-Medial versus Dorso-Palmar/Plantar Drilling for Cartilage Removal in the Proximal Interphalangeal Joint. Animals, 11(6), 1838. https://doi.org/10.3390/ani11061838