The Effects of Smoking Cigarettes on Immediate Dental Implant Stability—A Prospective Case Series Study

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Implants Features
2.3. Surgical Procedures
2.4. Post-Operative Care
2.5. Stability Measurement
2.6. Marginal Bone Loss Measurement
2.7. Statistical Analysis
3. Results
3.1. Characteristic of Patients
3.2. Aesthetic Area
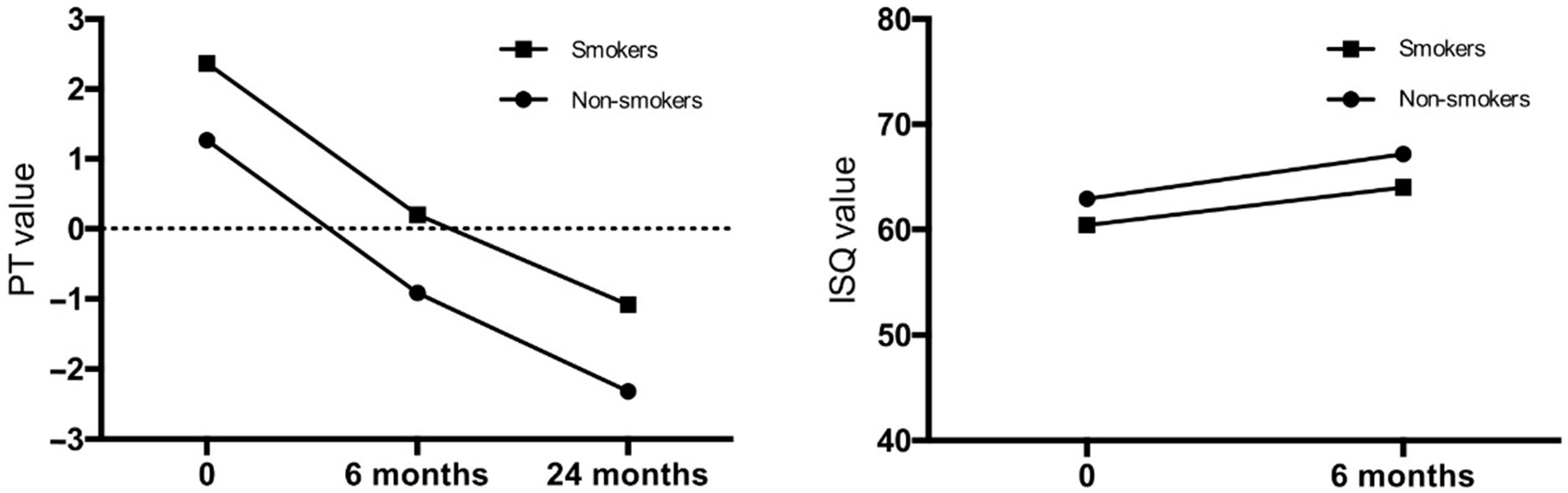
3.3. Posterior Area
3.4. Other Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alfadda, S.A. Current Evidence on Dental Implants Outcomes in Smokers and Nonsmokers: A Systematic Review and Meta-Analysis. J. Oral Implantol. 2018, 44, 390–399. [Google Scholar] [CrossRef] [PubMed]
- Naseri, R.; Yaghini, J.; Feizi, A. Levels of smoking and dental implants failure: A systematic review and meta-analysis. J. Clin. Periodontol. 2020, 47, 518–528. [Google Scholar] [CrossRef]
- Bezerra Ferreira, J.D.; Rodrigues, J.A.; Piattelli, A.; Iezzi, G.; Gehrke, S.A.; Shibli, J.A. The effect of cigarette smoking on early osseointegration of dental implants: A prospective controlled study. Clin. Oral Implants Res. 2016, 27, 1123–1128. [Google Scholar] [CrossRef] [PubMed]
- Lassig, A.A.D.; Bechtold, J.E.; Lindgren, B.R.; Pisansky, A.; Itabiyi, A.; Yueh, B.; Joseph, A.M. Tobacco exposure and wound healing in head and neck surgical wounds. Laryngoscope 2018, 128, 618–625. [Google Scholar] [CrossRef] [PubMed]
- Pimentel, S.P.; Fontes, M.; Ribeiro, F.V.; Corrêa, M.G.; Nishii, D.; Cirano, F.R.; Casati, M.Z.; Casarin, R.C.V. Smoking habit modulates peri-implant microbiome: A case-control study. J. Periodontal. Res. 2018, 53, 983–991. [Google Scholar] [CrossRef]
- Monje, A.; Ravidà, A.; Wang, H.L.; Helms, J.A.; Brunski, J.B. Relationship Between Primary/Mechanical and Secondary/Biological Implant Stability. Int. J. Oral Maxillofac. Implants 2019, 34, 7–23. [Google Scholar] [CrossRef]
- Chrcanovic, B.R.; Albrektsson, T.; Wennerberg, A. Reasons for failures of oral implants. J. Oral Rehabil. 2014, 41, 443–476. [Google Scholar] [CrossRef]
- Marcello-Machado, R.M.; Faot, F.; Schuster, A.J.; Bielemann, A.M.; Nascimento, G.G.; Del Bel Cury, A.A. Mapping of inflammatory biomarkers in the peri-implant crevicular fluid before and after the occlusal loading of narrow diameter implants. Clin. Oral Investig. 2020, 24, 1311–1320. [Google Scholar] [CrossRef]
- Mesa, F.; Muñoz, R.; Noguerol, B.; de Dios Luna, J.; Galindo, P.; O’Valle, F. Multivariate study of factors influencing primary dental implant stability. Clin. Oral Implants Res. 2008, 19, 196–200. [Google Scholar] [CrossRef]
- Sanchez-Perez, A.; Villaescusa, M.; Caffesse, R. Tobacco as a Risk Factor for Survival of Dental Implants. J. Periodontol. 2007, 78, 351–359. [Google Scholar] [CrossRef]
- Sun, C.; Zhao, J.; Jianghao, C.; Hong, T. Effect of Heavy Smoking on Dental Implants Placed in Male Patients Posterior Mandibles: A Prospective Clinical Study. J. Oral Implantol. 2016, 42, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Zhu, B.; Duan, Y.; Wang, X.; Li, D. The Effect of Smoking Behavior on Alveolar Bone Marrow Mesenchymal Stem Cells of Clinical Implant Patient. Biomed. Res. Int. 2018, 2018, 7672695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badenes, J.; Pallarés, A. Influence of smoking upon dental implant osseointegration: A radiofrequency analysis of 194 implants. J. Oral Implantol. 2020. [Google Scholar] [CrossRef]
- Sayardoust, S.; Omar, O.; Thomsen, P. Gene expression in peri-implant crevicular fluid of smokers and nonsmokers. 1. The early phase of osseointegration. Clin. Implant Dent. Relat. Res. 2017, 19, 681–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wychowanski, P.; Starzynska, A.; Woliński, J.; Kosieradzki, M.; Fiedor, P. New Surgical Technique Using Xenograft as a Microinvasive Method to Avoid Extensive Bone Reconstruction in Patients with Compromised General Health: Promising Surgical Methodology and First Clinical Results. Transplant. Proc. 2020, 52, 2244–2247. [Google Scholar] [CrossRef] [PubMed]
- Aleksandrowicz, P.; Kusa-Podkańska, M.; Grabowska, K.; Kotuła, L.; Szkatuła-Łupina, A.; Wysokińska-Miszczuk, J. Extra-Sinus Zygomatic Implants to Avoid Chronic Sinusitis and Prosthetic Arch Malposition: 12 Years of Experience. J. Oral Implantol. 2019, 45, 73–78. [Google Scholar] [CrossRef]
- Wychowanski, P.; Woliński, J.; Morawiec, T.; Kownacki, P.; Starzynska, A.; Kosieradzki, M.; Fiedor, P. Preliminary Clinical Data and the Comparison of the Safety and Efficacy of Autogenous Bone Grafts Versus Xenograft Implantations in Vertical Bone Deficiencies Before Dental Implant Installation. Transplant. Proc. 2020, 52, 2248–2251. [Google Scholar] [CrossRef] [PubMed]
- Wychowański, P.; Woliński, J.; Kacprzak, M.; Tomkiewicz, W.; Bartłomiej, I.; Szubińska-Lelonkiewicz, D.; Wojtowicz, A.; Nevis, M. Immediate Palatal Molar Implants: A Simple, Safe, Minimally Invasive Technique. Int. J. Periodontics Restor. Dent. 2017, 37, e297–e301. [Google Scholar]
- Lekholm, U.; Zarb, G.A. Patient selection and preparation. In Tissueintegrated Prostheses: Osseointegration in Clinical Dentistry; Brånemark, P.-I., Zarb, G.A., Albrektsson, T., Eds.; Quintessence: Chicago, IL, USA, 1985; pp. 199–209. [Google Scholar]
- Herrero-Climent, M.; Santos-García, R.; Jaramillo-Santos, R.; Romero-Ruiz, M.M.; Fernández-Palacin, A.; Lázaro-Calvo, P.; Bullón, P.; Ríos-Santos, J.V. Assessment of Osstell ISQ’s reliability for implant stability measurement: A cross-sectional clinical study. Med. Oral Patol. Oral Cir. Bucal 2013, 18, e877–e882. [Google Scholar] [CrossRef]
- Sennerby, L.; Meredith, N. Implant stability measurements using resonance frequency analysis: Biological and biomechanical aspects and clinical implications. Periodontology 2000 2008, 47, 51–66. [Google Scholar] [CrossRef]
- Bornstein, M.M.; Hart, C.N.; Halbritter, S.A.; Morton, D.; Buser, D. Early Loading of Nonsubmerged Titanium Implants with a Chemically Modified Sand-Blasted and Acid-Etched Surface: 6-Month Results of a Prospective Case Series Study in the Posterior Mandible Focusing on Peri-Implant Crestal Bone Changes and Implant Stability Quotient (ISQ) Values. Clin. Implant Dent. Relat. Res. 2009, 11, 338–347. [Google Scholar] [PubMed]
- Kokovic, V.; Jung, R.; Feloutzis, A.; Todorovic, V.; Jurisic, M.; Hämmerle, C. Immediate vs. early loading of SLA implants in the posterior mandible: 5-year results of randomized controlled clinical trial. Clin. Oral Implants Res. 2014, 25, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Aparicio, C.; Lang, N.P.; Rangert, B. Validity and clinical significance of biomechanical testing of implant/bone interface. Clin. Oral Implants Res. 2006, 17 (Suppl. S2), 2–7. [Google Scholar] [CrossRef]
- Bohner, L.O.L.; Mukai, E.; Oderich, E.; Porporatti, A.L.; Pacheco-Pereira, C.; Tortamano, P.; De Luca Canto, G. Comparative analysis of imaging techniques for diagnostic accuracy of peri-implant bone defects: A meta-analysis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2017, 124, 432–440. [Google Scholar] [CrossRef] [PubMed]
- Naveau, A.; Shinmyouzu, K.; Moore, C.; Avivi-Arber, L.; Jokerst, J.; Koka, S. Etiology and Measurement of Peri-Implant Crestal Bone Loss (CBL). J. Clin. Med. 2019, 8, 166. [Google Scholar] [CrossRef] [Green Version]
- Manzano-Moreno, F.J.; Herrera-Briones, F.J.; Bassam, T.; Vallecillo-Capilla, M.F.; Reyes-Botella, C. Factors Affecting Dental Implant Stability Measured Using the Ostell Mentor Device: A Systematic Review. Implant Dent. 2015, 24, 565–577. [Google Scholar] [CrossRef]
- Albrektsson, T.; Zarb, G.A. Current interpretations of the osseointegrated response: Clinical significance. Int. J. Prosthodont. 1993, 6, 95–105. [Google Scholar]
- Szmukler-Moncler, S.; Salama, H.; Reingewirtz, Y.; Dubruille, J.H. Timing of loading and effect of micromotion on bone-dental implant interface: Review of experimental literature. J. Biomed. Mater. Res. 1998, 43, 192–203. [Google Scholar] [CrossRef]
- Baltayan, S.; Pi-Anfruns, J.; Aghaloo, T.; Moy, P.K. The Predictive Value of Resonance Frequency Analysis Measurements in the Surgical Placement and Loading of Endosseous Implants. J. Oral Maxillofac. Surg. 2016, 74, 1145–1152. [Google Scholar] [CrossRef] [Green Version]
- Rodrigo, D.; Aracil, L.; Martin, C.; Sanz, M. Diagnosis of implant stability and its impact on implant survival: A prospective case series study. Clin. Oral Implants Res. 2010, 21, 255–261. [Google Scholar] [CrossRef]
- Degidi, M.; Daprile, G.; Piattelli, A.; Iezzi, G. Development of a New Implant Primary Stability Parameter: Insertion Torque Revisited. Clin. Implant Dent. Relat. Res. 2013, 15, 637–644. [Google Scholar] [CrossRef] [PubMed]
- Clementini, M.; Rossetti, P.H.; Penarrocha, D.; Micarelli, C.; Bonachela, W.C.; Canullo, L. Systemic risk factors for peri-implant bone loss: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2014, 43, 323–334. [Google Scholar] [CrossRef] [PubMed]
- Moraschini, V.; Barboza, E.S. Effect of autologous platelet concentrates for alveolar socket preservation: A systematic review. Int. J. Oral Maxillofac. Surg. 2015, 44, 632–641. [Google Scholar] [CrossRef] [PubMed]
- Pagliani, L.; Sennerby, L.; Petersson, A.; Verrocchi, D.; Volpe, S.; Andersson, P. The relationship between resonance frequency analysis (RFA) and lateral displacement of dental implants: An in vitro study. J. Oral Rehabil. 2013, 40, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Cai, M.; Yang, J.; Aldhohrah, T.; Wang, Y. Immediate versus early or conventional loading dental implants with fixed prostheses: A systematic review and meta-analysis of randomized controlled clinical trials. J. Prosthet. Dent. 2019, 122, 516–536. [Google Scholar] [CrossRef] [Green Version]
- Do, T.A.; Le, H.S.; Shen, Y.W.; Huang, H.L.; Fuh, L.J. Risk Factors related to Late Failure of Dental Implant-A Systematic Review of Recent Studies. Int. J. Environ. Res. Public Health 2020, 17, 3931. [Google Scholar] [CrossRef]
- Khalaila, W.; Nasser, M.; Ormianer, Z. Evaluation of the relationship between Periotest values, marginal bone loss, and stability of single dental implants: A 3-year prospective study. J. Prosthet. Dent. 2020, 124, 183–188. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Aesthetic Area | Posterior Area | |||||||
|---|---|---|---|---|---|---|---|---|
| Smokers | Non-Smokers | Smokers | Non-Smokers | |||||
| n | % | n | % | n | % | n | % | |
| Overall number of patients | 47 | 42 | 65 | 58 | 20 | 100 | 32 | 100 |
| Female | 27 | 57.5 | 36 | 55.4 | 10 | 50 | 17 | 53 |
| Male | 20 | 42.5 | 29 | 44.6 | 10 | 50 | 15 | 47 |
| Age at insertion (range) | 47 (27–63) | 50 (29–64) | 54 (29–71) | 48 (27–68) | ||||
| Total number of implants placed | 54 | 100 | 75 | 100 | 24 | 100 | 37 | 100 |
| Patients who received 1 implant | 40 | 85 | 55 | 85 | 16 | 80 | 27 | 84 |
| Patients who received 2 implants | 7 | 15 | 10 | 15 | 4 | 20 | 5 | 16 |
| 10 mm-long implants | - | - | - | - | 9 | 37.5 | 13 | 35 |
| 11.5 mm-long implants | 20 | 37 | 25 | 33.5 | 15 | 62.5 | 24 | 65 |
| 13.0 mm-long implants | 28 | 52 | 40 | 53.5 | - | - | - | - |
| 16.0 mm-long implants | 6 | 11 | 10 | 13 | - | - | - | - |
| Platform (3.3 mm) implant diameter | 12 | 22 | 14 | 18.5 | - | - | - | - |
| Platform (3.75 mm) implant diameter | 31 | 57.5 | 43 | 57.5 | 9 | 37.5 | 6 | 16 |
| Platform (4.2 mm) implant diameter | 11 | 20.5 | 18 | 24 | 15 | 62.5 | 31 | 84 |
| Bone class III | 26 | 48.15 | 39 | 52 | 11 | 45.83 | 17 | 45.95 |
| Bone class IV | 28 | 51.85 | 36 | 48 | 13 | 54.17 | 20 | 54.05 |
| Mean Insertion Torque Value (Ncm) | 16.3 | - | 17.5 | - | 16.8 | - | 17.9 | - |
| Standard deviation of Insertion Torque Value | 5.2 | - | 4.9 | - | 5.7 | - | 6.1 | - |
| Aesthetic Area | Posterior Area | |||||||
|---|---|---|---|---|---|---|---|---|
| Smokers | Non-Smokers | Smokers | Non-Smokers | |||||
| n | % | n | % | n | % | n | % | |
| Caries | 22 | 41 | 16 | 21 | 11 | 46 | 18 | 49 |
| Endodontic problem | 14 | 26 | 22 | 29.5 | 7 | 30 | 6 | 16 |
| Periodontitis | 5 | 9 | 7 | 9.5 | 2 | 8 | 6 | 16 |
| Fracture | 8 | 15 | 21 | 28 | 2 | 8 | 4 | 11 |
| Resorption | 5 | 9 | 9 | 12 | 2 | 8 | 3 | 8 |
| Smokers; n = 54 | Non-Smokers; n = 75 | ||||||||
| ISQ | |||||||||
| Time of measurement | Mean ± SD | Median | Range | CI 95% | Mean ± SD | Median | Range | CI 95% | pValue |
| 0 | 58.5 ± 5.05 | 58.00 | 52.00–71.00 | 57.48–59.55 | 60.0 ± 5.1 | 59.00 | 51.00–73.00 | 58.89–60.79 | 0.06 |
| 6 months | 65.52 ± 5.05 | 65.00 | 58.00–78.00 | 64.14–66.90 | 67.61 ± 5.11 | 67.00 | 58.00–81.00 | 66.44–68.79 | 0.02 |
| PT | |||||||||
| Time of measurement | Mean ± SD | Median | Range | CI 95% | Mean ± SD | Median | Range | CI 95% | pValue |
| 0 | 2.52 ± 0.11 | 2.00 | 0.00–4.00 | 2.29–2.74 | 2.27 ± 0.10 | 2.00 | 0.00–4.00 | 2.06–2.46 | 0.10 |
| 6 months | 0.34 ± 0.12 | 0.00 | −2.00–2.00 | 0.09–0.58 | 0.0 ± 0.09 | 0.00 | −2.00–2.00 | −0.18–0.18 | 0.02 |
| 24 months | −1.40 ± 0.12 | −1.00 | −3.00–0.00 | −1.64–(−1.16) | −1.44 ± 0.09 | −1.00 | −3.00–0.00 | −1.62–(−1.25) | 0.82 |
| Bone atrophy 18 months after loading [mm] | |||||||||
| Time of measurement | Mean ± SD | Mean ± SD | pValue | ||||||
| 18 months post-loading | 0.07 ± 0.01 | 0.07 ± 0.01 | 0.94 | ||||||
| Vestibular bone plate thickness 18 months after loading [mm] | |||||||||
| Site of measurement | Mean ± SD | Mean ± SD | pValue | ||||||
| Shoulder | 2.06 ± 0.41 | 1.98 ± 0.39 | 0.43 | ||||||
| Middle | 2.37 ± 0.48 | 2.28 ± 0.43 | 0.23 | ||||||
| Apex | 2.91 ± 0.58 | 2.83 ± 0.58 | 0.36 | ||||||
| Smokers; n = 24 | Non-Smokers; n =37 | ||||||||
| ISQ | |||||||||
| Time of measurement | Mean ± SD | Median | Range | CI 95% | Mean ± SD | Median | Range | CI 95% | pValue |
| 0 | 60.4 ± 0.4 | 60.60 | 55.70–64.30 | 59.49–61.37 | 62.9 ± 0.6 | 62.50 | 55.50–69.30 | 61.60–64.12 | 0.0047 |
| 6 months | 64.0 ± 0.5 | 63.55 | 60.40–70.10 | 63.00–65.05 | 67.2 ± 0.6 | 66.70 | 60.20–75.60 | 65.88–68.58 | 0.0002 |
| PT | |||||||||
| Time of measurement | Mean ± SD | Median | Range | CI 95% | Mean ± SD | Median | Range | CI 95% | pValue |
| 0 | 2.37 ± 0.2 | 2.50 | 0.00–4.00 | 1.89–2.85 | 1.27 ± 0.3 | 2.00 | −2.00–4.00 | 0.67–1.87 | 0.0179 |
| 6 months | 0.20 ± 0.18 | 0.00 | −2.00–2.00 | −0.16–0.58 | −0.91 ± 0.2 | −1.00 | −3.00–1.00 | −1.34–(−0.50) | 0.0003 |
| 24 months | −1.08 ± 0.18 | −1.00 | −3.00–0.00 | −1.47–(−0.69) | −2.32 ± 0.2 | −2.00 | −4.00–(−1.00) | −2.65–(−1.99) | <0.0001 |
| Bone atrophy 18 months after loading [mm] | |||||||||
| Time of measurement | Mean ± SD | Mean ± SD | pValue | ||||||
| 18 months post-loading | 0.08 ± 0.02 | 0.06 ± 0.01 | 0.49 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wychowański, P.; Starzyńska, A.; Jereczek-Fossa, B.A.; Iwanicka-Grzegorek, E.; Kosewski, P.; Adamska, P.; Woliński, J. The Effects of Smoking Cigarettes on Immediate Dental Implant Stability—A Prospective Case Series Study. Appl. Sci. 2021, 11, 27. https://doi.org/10.3390/app11010027
Wychowański P, Starzyńska A, Jereczek-Fossa BA, Iwanicka-Grzegorek E, Kosewski P, Adamska P, Woliński J. The Effects of Smoking Cigarettes on Immediate Dental Implant Stability—A Prospective Case Series Study. Applied Sciences. 2021; 11(1):27. https://doi.org/10.3390/app11010027
Chicago/Turabian StyleWychowański, Piotr, Anna Starzyńska, Barbara Alicja Jereczek-Fossa, Ewa Iwanicka-Grzegorek, Przemysław Kosewski, Paulina Adamska, and Jarosław Woliński. 2021. "The Effects of Smoking Cigarettes on Immediate Dental Implant Stability—A Prospective Case Series Study" Applied Sciences 11, no. 1: 27. https://doi.org/10.3390/app11010027
APA StyleWychowański, P., Starzyńska, A., Jereczek-Fossa, B. A., Iwanicka-Grzegorek, E., Kosewski, P., Adamska, P., & Woliński, J. (2021). The Effects of Smoking Cigarettes on Immediate Dental Implant Stability—A Prospective Case Series Study. Applied Sciences, 11(1), 27. https://doi.org/10.3390/app11010027