Estimating Health Impacts Due to the Reduction of Particulate Air Pollution from the Household Sector Expected under Various Scenarios


 , , ,
, , ,
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Emission Data for Scenarios
2.2. Air Pollution Modeling and Emission Data
2.3. Health and Population Data
- deaths caused by natural causes, older than 30;
- days of sickness absence, older than 18;
- bronchitis among children, aged 6–18; and
- chronic bronchitis among adults, older than 18.
2.4. Methodology of the Health Impact Assessment
- Premature death from natural causes—1.062; pollutant metric PM2.5;
- Bronchitis among children—1.080; pollutant metric PM10;
- Chronic bronchitis among adults—1.117; pollutant metric PM10; and
- Work absence—1.046; pollutant metric PM2.5.
3. Results
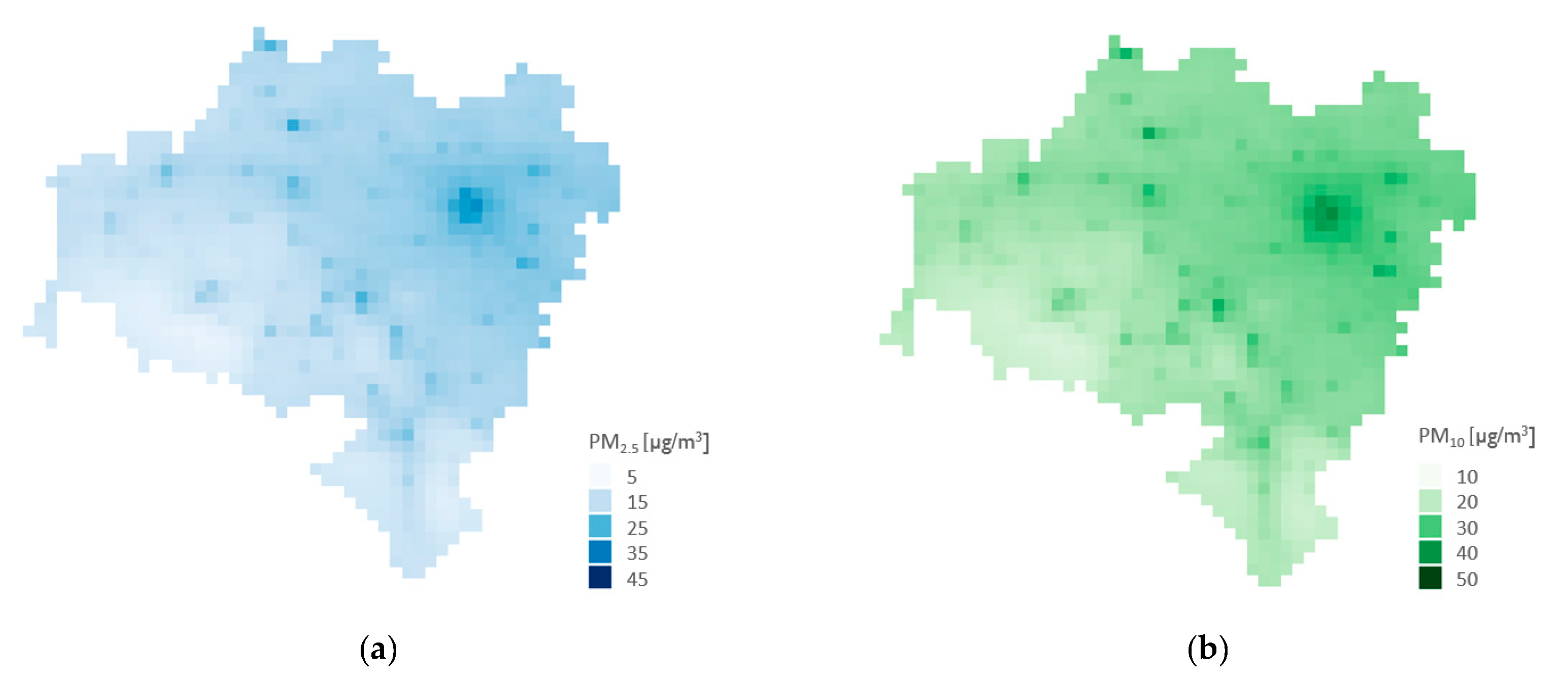
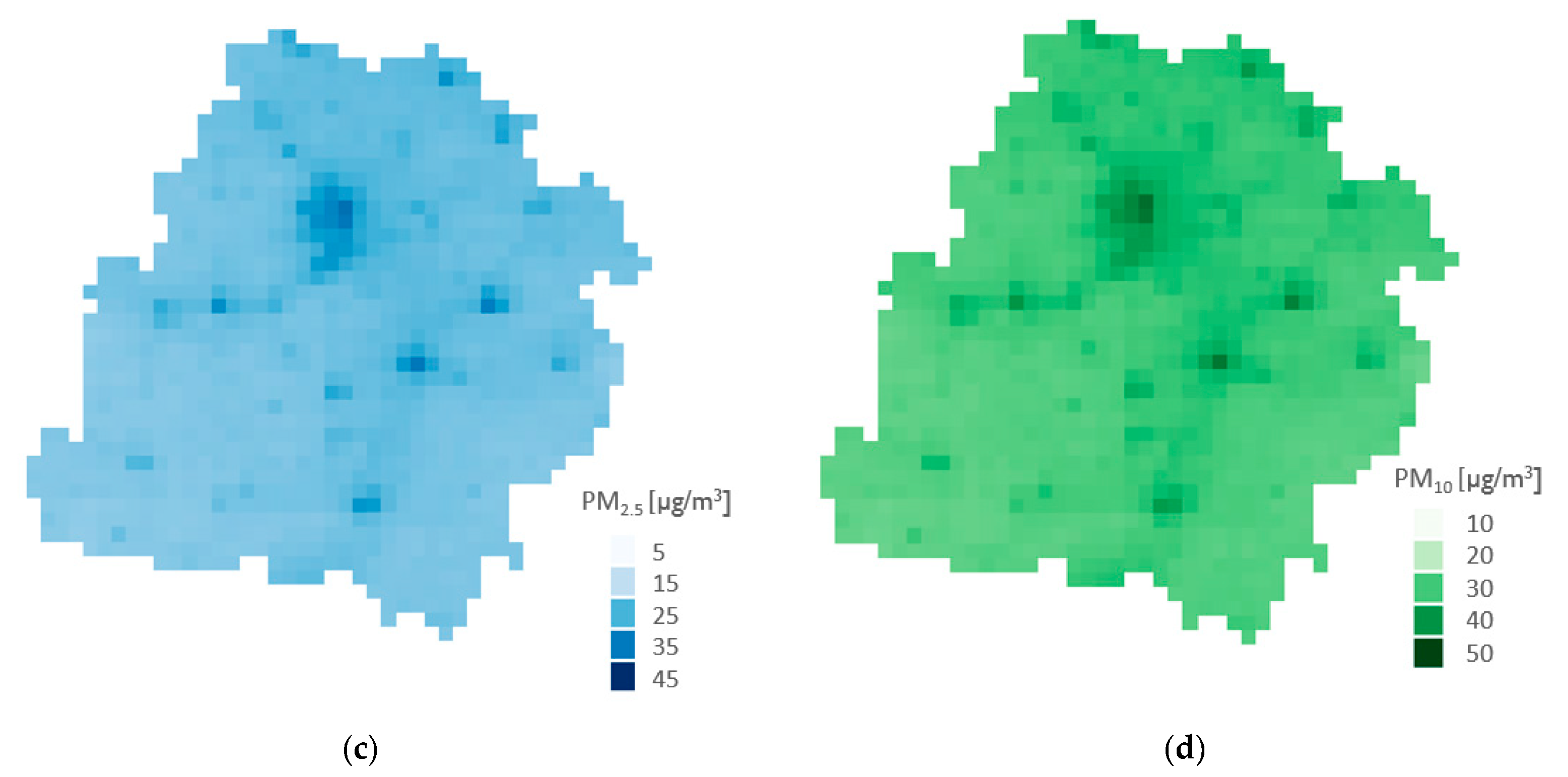
3.1. Reduction of Air Pollution
3.2. Reduction of Health Impacts
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Available online: https://www.who.int/health-topics/air-pollution#tab=tab_2 (accessed on 10 March 2020).
- Dockery, D.W. Health effects of particulate air pollution. Anna. Epidemiol. 2009, 19, 257–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forouzanfar, M.H.; Afshin, A.; Alexander, L.T.; Anderson, H.R.; Bhutta, Z.A.; Biryukov, S.; Brauer, M.; Burnett, R.; Cercy, K.; Charlson, F.J.; et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef] [Green Version]
- Brook, R.D.; Rajagopalan, S.; Pope, C.A.; Brook, J.R.; Bhatnagar, A.; Diez-Roux, A.V.; Holguin, F.; Hong, Y.; Luepker, R.V.; Mittleman, M.A.; et al. Particulate Matter Air Pollution and Cardiovascular Disease. Circulation 2010, 121, 2331–2378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pope, C.A.; Burnett, R.T.; Turner, M.C.; Cohen, A.; Krewski, D.; Jerrett, M.; Gapstur, S.M.; Thun, M.J. Lung Cancer and Cardiovascular Disease Mortality Associated with Ambient Air Pollution and Cigarette Smoke: Shape of the Exposure–Response Relationships. Environ. Health Perspect. 2011, 119, 1616–1621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Dandona, L.; Dandona, R.; et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the Global Burden of Diseases Study 2015. Lancet 2017, 389, 1907–1918. [Google Scholar] [CrossRef] [Green Version]
- Lelieveld, J.; Klingmüller, K.; Pozzer, A.; Pöschl, U.; Fnais, M.; Daiber, A.; Münzel, T. Cardiovascular disease burden from ambient air pollution in Europe reassessed using novel hazard ratio functions. Eur. Heart J. 2019, 40, 1590–1596. [Google Scholar] [CrossRef] [Green Version]
- European Environment Agency. Air Quality in Europe—2019 Report; Publications Office of the European Union: Luxembourg, 2019. [Google Scholar]
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; AlMazroa, M.A.; Amann, M.; Anderson, H.R.; Andrews, K.G.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Health Risks of Air Pollution in Europe—HRAPIE Project Recommendations for Concentration–Response Functions for Cost–Benefit Analysis of Particulate Matter, Ozone and Nitrogen Dioxide; WHO Regional Office for Europe: Copenhagen, Denmark, 2013. [Google Scholar]
- Hurley, F.; Hunt, A.; Cowie, H.; Holland, M.; Miller, B.; Pye, S.; Watkiss, P. Methodology Paper for Service Contract for Carrying Out Cost-Benefit Analysis of Air Quality Related Issues, in Particular in the Clean Air for Europe (CAFE) Programme; AEA Technology Environment: Didcot, UK, 2005; Volume 2. [Google Scholar]
- Liu, J.; Kiesewetter, G.; Klimont, Z.; Cofala, J.; Heyes, C.; Schöpp, W.; Zhu, T.; Cao, G.; Sanabria, A.G.; Sander, R.; et al. Mitigation pathways of air pollution from residential emissions in the Beijing-Tianjin-Hebei region in China. Environ. Int. 2019, 125, 236–244. [Google Scholar] [CrossRef]
- Kheirbek, I.; Haney, J.; Douglas, S.; Ito, K.; Caputo, S.; Matte, T. The Public Health Benefits of Reducing Fine Particulate Matter through Conversion to Cleaner Heating Fuels in New York City. Environ. Sci. Technol. 2014, 48, 13573–13582. [Google Scholar] [CrossRef]
- Zhao, B.; Zheng, H.; Wang, S.-X.; Smith, K.R.; Lu, X.; Aunan, K.; Gu, Y.; Wang, Y.; Ding, D.; Xing, J.; et al. Change in household fuels dominates the decrease in PM2.5 exposure and premature mortality in China in 2005–2015. Proc. Natl. Acad. Sci. USA 2018, 115, 12401–12406. [Google Scholar] [CrossRef] [Green Version]
- Conibear, L.; Butt, E.W.; Knote, C.; Arnold, S.R.; Spracklen, D.V. Residential energy use emissions dominate health impacts from exposure to ambient particulate matter in India. Nat. Commun. 2019, 9, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holnicki, P.; Tainio, M.; Kałuszko, A.; Nahorski, Z. Burden of Mortality and Disease Attributable to Multiple Air Pollutants in Warsaw, Poland. Int. J. Environ. Res. Public Health 2017, 14, 1359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xia, T.; Nitschke, M.; Zhang, Y. Traffic-related air pollution and health co-benefits of alternative transport in Adelaide, South Australia. Environ. Int. 2015, 74, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Van Brusselen, D.; De Oñate, W.A.; Maiheu, B.; Vranckx, S.; Lefebvre, W.; Janssen, S.; Nawrot, T.S.; Nemery, B.; Avonts, D. Health Impact Assessment of a Predicted Air Quality Change by Moving Traffic from an Urban Ring Road into a Tunnel. The Case of Antwerp, Belgium. PLoS ONE 2016, 11, e0154052. [Google Scholar] [CrossRef] [Green Version]
- Requia, W.J.; Higgins, C.D.; Adams, M.D.; Mohamed, M.; Koutrakis, P. The health impacts of weekday traffic: A health risk assessment of PM2.5 emissions during congested periods. Environ. Int. 2018, 111, 164–176. [Google Scholar] [CrossRef]
- Martenies, S.E.; Akherati, A.; Jathar, S.; Magzamen, S. Health and environmental justice implications of retiring two coal-fired power plants in the southern Front Range region of Colorado. GeoHealth 2019, 3, 266–283. [Google Scholar] [CrossRef] [Green Version]
- Chio, C.-P.; Lo, W.-C.; Tsuang, B.-J.; Hu, C.-C.; Ku, K.-C.; Chen, Y.-J.; Lin, H.-H.; Chan, C.-C. Health impact assessment of PM2.5 from a planned coal-fired power plant in Taiwan. J. Formos. Med. Assoc. 2019, 118, 1494–1503. [Google Scholar] [CrossRef]
- Institute of Environmental Economics. Energy Efficiency in Poland 2015 Review. Single-Family Houses Mechanism to Support Modernisation; Institute of Environmental Economics: Kraków, Poland, 2016; pp. 13–14, 49. [Google Scholar]
- National Centre for Emissions Management (KOBIZE) at the Institute of Environmental Protection—National Research Institute. Poland‘s Informative Inventory Report 2019; KOBIZE: Warsaw, Poland, 2019. [Google Scholar]
- Hlawiczka, S.; Klis, C.; Cenowski, M. New approach to the impact assessment of dust emission from home heating processes on the air pollutant concentration of a single municipality. I. Emission sources inventory and emission modelling. Ochrona Środowiska i Zasobów Naturalnych 2011, 47, 22–46. [Google Scholar]
- Central Statistical Office. Available online: https://bdl.stat.gov.pl/BDL/dane/podgrup/temat/31/524 (accessed on 10 March 2020).
- Simpson, D.; Benedictow, A.; Berge, H.; Bergstrom, R.W.; Emberson, L.D.; Fagerli, H.; Flechard, C.R.; Hayman, G.D.; Gauss, M.; Jonson, J.E.; et al. The EMEP MSC-W chemical transport model–Technical description. Atmos. Chem. Phys. Discuss. 2012, 12, 7825–7865. [Google Scholar] [CrossRef] [Green Version]
- Vieno, M.; Dore, A.J.; Stevenson, D.S.; Doherty, R.; Heal, M.R.; Reis, S.; Hallsworth, S.; Tarrason, L.; Wind, P.; Fowler, D.; et al. Modelling surface ozone during the 2003 heat-wave in the UK. Atmos. Chem. Phys. Discuss. 2010, 10, 7963–7978. [Google Scholar] [CrossRef] [Green Version]
- Vieno, M.; Heal, M.R.; Hallsworth, S.; Famulari, D.; Doherty, R.M.; Dore, A.J.; Tang, Y.S.; Braban, C.F.; Leaver, D.; Sutton, M.A.; et al. The role of long-range transport and domestic emissions in determining atmospheric secondary inorganic particle concentrations across the UK. Atmos. Chem. Phys. Discuss. 2014, 14, 8435–8447. [Google Scholar] [CrossRef] [Green Version]
- Vieno, M.; Heal, M.R.; Williams, M.L.; Carnell, E.J.; Nemitz, E.; Stedman, J.R.; Reis, S. The sensitivities of emissions reductions for the mitigation of UK PM2.5. Atmos. Chem. Phys 2016, 16, 265–276. [Google Scholar] [CrossRef] [Green Version]
- Werner, M.; Kryza, M.; Wind, P. High resolution application of the EMEP MSC-W model over Eastern Europe—Analysis of the EMEP4PL results. Atmos. Res. 2018, 212, 6–22. [Google Scholar] [CrossRef]
- Skamarock, W.C.; Klemp, J.B. A time-split nonhydrostatic atmospheric model for weather research and forecasting applications. J. Comput. Phys. 2008, 227, 3465–3485. [Google Scholar] [CrossRef]
- Kuenen, J.J.P.; Visschedijk, A.J.H.; Jozwicka, M.; Denier van der Gon, H.A.C. TNO-MACC_II emission inventory: A multi-year (2003–2009) consistent high-resolution European emission inventory for air quality modelling. Atmos. Chem. Phys. Discuss. 2014, 14, 10963–10976. [Google Scholar] [CrossRef] [Green Version]
- Instytut Ochrony Środowiska—Państwowy Instytut Badawczy; Krajowy Ośrodek Bilansowania i Zarządzania Emisjami (KOBiZE). Krajowy Bilans Emisji SO2, NOx, CO, NH3, NM-LZO, Pyłów, Metali Ciężkich i TZO za Lata 2015–2017 w Układzie Klasyfikacji SNAP; Raport Syntetyczny; Krajowy Ośrodek Bilansowania i Zarządzania Emisjami (KOBiZE): Warszawa, Poland, 2019. [Google Scholar]
- Kiesewetter, G.; Amann, M. Urban PM2.5 Levels under the EU Clean Air Policy Package TSAP Report #12, Figure 2.16; DG-Environment of the European Commission: Brussels, Belgium, 2014. [Google Scholar]
- Badyda, A.J.; Dąbrowiecki, P.; Czechowski, P.O.; Majewski, G.; Doboszyńska, A. Traffic-related air pollution and respiratory tract efficiency. Adv. Exp. Med. Biol. 2015, 834, 31–38. [Google Scholar] [CrossRef]
- Rogula-Kozłowska, W.; Kostrzon, M.; Rogula-Kopiec, P.; Badyda, A.J. Particulate Matter in the Air of the Underground Chamber Complex of the Wieliczka Salt Mine Health Resort. Adv. Exp. Med. Biol. 2017, 955, 9–18. [Google Scholar] [CrossRef]
- Kobus, D.; Iwanek, J.; Skotak, K. Ocena Jakości Powietrza w Strefach w Polsce za Rok 2019; Główny Inspektorat Ochrony Środowiska: Warszawa, Poland, 2020.
- Liu, C.; Chen, R.; Sera, F.; Vicedo-Cabrera, A.M.; Guo, Y.; Tong, S.; Coelho, M.S.Z.S.; Saldiva, P.H.N.; Lavigne, E.; Matus, P.; et al. Ambient Particulate Air Pollution and Daily Mortality in 652 Cities. N. Engl. J. Med. 2019, 381, 705–715. [Google Scholar] [CrossRef]
- Adamkiewicz, Ł.; Badyda, A.J.; Gayer, A.; Mucha, D. Disability-adjusted life years in the assessment of health effects of traffic-related air pollution. Adv. Exp. Med. Biol 2015, 834, 15–20. [Google Scholar] [CrossRef]
- Di, Q.; Wang, Y.; Zanobetti, A.; Wang, Y.; Koutrakis, P.; Choirat, C.; Dominici, F.; Schwartz, J.D. Air Pollution and Mortality in the Medicare Population. N. Engl. J. Med. 2017, 376, 2513–2522. [Google Scholar] [CrossRef]
- Pope, C.A.; Coleman, N.; Pond, Z.A.; Burnett, R.T. Fine particulate air pollution and human mortality: 25+ years of cohort studies. Environ. Res. 2020, 183, 108924. [Google Scholar] [CrossRef] [PubMed]
- Heal, M.R.; Heaviside, C.; Doherty, R.M.; Vieno, M.; Stevenson, D.; Vardoulakis, S. Health burdens of surface ozone in the UK for a range of future scenarios. Environ. Int. 2013, 61, 36–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carnell, E.J.; Vieno, M.; Vardoulakis, S.; Beck, R.C.; Heaviside, C.; Tomlinson, S.J.; Dragosits, U.; Heal, M.R.; Reis, S. Modelling public health improvements as a result of air pollution control policies in the UK over four decades—1970 to 2010. Environ. Res. Lett. 2019, 14, 074001. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Pollutant | Unit | Hard Coal | Other Fuels | ||||
|---|---|---|---|---|---|---|---|
| Manual Boilers, Low Quality | Manual Boilers, High Quality | Automatic Boilers | Stove | ||||
| Gas | Oil | ||||||
| PM10 | g/GJ | 460 | 130 | 70 | 450 | 0.5 | 3 |
| PM2.5 | g/GJ | 448 | 121 | 61 | 448 | 0.5 | 2.7 |
| Region | Before 1944 | 1945–1988 | 1989–2002 | 2003–2011 and under Construction |
|---|---|---|---|---|
| Lower Silesia [%] | 60.6 | 14.2 | 6.3 | 12.2 |
| Lodzkie province [%] | 11.1 | 64.7 | 10.6 | 8.1 |
| Region | Before 1944 | 1945–1988 | 1989–2002 | 2003–2011 and under Construction |
|---|---|---|---|---|
| Energy [kWh/m2 annual] | 350 | 260 | 180 | 120 |
| Region | Scenario 1 | Scenario 2 | Scenario 3 |
|---|---|---|---|
| Lower Silesia [%] | 94.87 | 85.84 | 63.04 |
| Lodzkie province [%] | 94.87 | 85.84 | 71.33 |
| PM2.5 [µg/m3] | PM10 [µg/m3] | |||||||
|---|---|---|---|---|---|---|---|---|
| Region | Base. | Scenario 1 | Scenario 2 | Scenario 3 | Base. | Scenario 1 | Scenario 2 | Scenario 3 |
| Lower Silesia | 18.5 | −6.58 | −4.57 | −2.82 | 33.5 | −10.2 | −7.82 | −5.01 |
| Lodzkie province | 28.4 | −9.01 | −7.62 | −5.98 | 42.5 | −12.8 | −10.6 | −9.12 |
| Lower Silesia | Lodzkie Province | |||||
|---|---|---|---|---|---|---|
| Health Impact | Scenario 1 | Scenario 2 | Scenario 3 | Scenario 1 | Scenario 2 | Scenario 3 |
| Premature death [cases] | 1122 | 776 | 476 | 1438 | 1 211 | 945 |
| [% reduction] | 34.3% | 23.7% | 14.6% | 29.9% | 25.2% | 19.7% |
| [per 100k a.] | 38.7 | 26.7 | 16.4 | 57.5 | 48.5 | 37.8 |
| Bronchitis amongst children [new cases] | 9602 | 7303 | 4628 | 9880 | 8067 | 6932 |
| [% reduction] | 27.7% | 21.1% | 13.4% | 26.8% | 21.9% | 18.8% |
| [per 100k a.] | 331 | 252 | 160 | 395 | 323 | 277 |
| Chronic bronchitis amongst adults [new cases] | 1516 | 1148 | 724 | 1502 | 1221 | 1047 |
| [% reduction] | 26.6% | 20.1% | 12.7% | 25.3% | 20.6% | 17.7% |
| [per 100k a.] | 52.3 | 39.6 | 25.0 | 60.1 | 48.9 | 41.9 |
| Work absence [days] | 481161 | 333083 | 204775 | 688981 | 581101 | 454101 |
| [% reduction] | 34.7% | 24.0% | 14.7% | 30.4% | 25.6% | 20.0% |
| [per 100k a.] | 16 592 | 11 486 | 7 061 | 27 559 | 23 244 | 18 164 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adamkiewicz, Ł.; Kryza, M.; Mucha, D.; Werner, M.; Gayer, A.; Drzeniecka-Osiadacz, A.; Sawiński, T. Estimating Health Impacts Due to the Reduction of Particulate Air Pollution from the Household Sector Expected under Various Scenarios. Appl. Sci. 2021, 11, 272. https://doi.org/10.3390/app11010272
Adamkiewicz Ł, Kryza M, Mucha D, Werner M, Gayer A, Drzeniecka-Osiadacz A, Sawiński T. Estimating Health Impacts Due to the Reduction of Particulate Air Pollution from the Household Sector Expected under Various Scenarios. Applied Sciences. 2021; 11(1):272. https://doi.org/10.3390/app11010272
Chicago/Turabian StyleAdamkiewicz, Łukasz, Maciej Kryza, Dominika Mucha, Małgorzata Werner, Anna Gayer, Anetta Drzeniecka-Osiadacz, and Tymoteusz Sawiński. 2021. "Estimating Health Impacts Due to the Reduction of Particulate Air Pollution from the Household Sector Expected under Various Scenarios" Applied Sciences 11, no. 1: 272. https://doi.org/10.3390/app11010272
APA StyleAdamkiewicz, Ł., Kryza, M., Mucha, D., Werner, M., Gayer, A., Drzeniecka-Osiadacz, A., & Sawiński, T. (2021). Estimating Health Impacts Due to the Reduction of Particulate Air Pollution from the Household Sector Expected under Various Scenarios. Applied Sciences, 11(1), 272. https://doi.org/10.3390/app11010272