1. Introduction
Life expectancy continues to increase, and complete edentulism is still a common health problem. Edentulous subjects routinely experience troubles with their mandibular complete dentures, including denture instability and loss of retention along with decreased chewing ability, which comprises their main complaints [
1]. These patients live a longer active life and have higher demands of their quality of life, which includes higher expectations from their dentures [
2,
3,
4].
The dental profession, in its efforts to meet edentulous patient’s expectations, must offer treatment modalities that accommodate appropriate and acceptable clinical standards. The combination therapy of an upper complete denture with a mandibular (lower) implant-supported overdenture (MISOD) is a well-documented successful treatment with proven patient satisfaction and chewing performance [
5,
6].
A debate remains concerning the number of implants to be installed in the edentulous mandible, intended to provide adequate retention and stability to the overdenture. The 2002 McGill Consensus statement put forth a new accepted standard of care for the complete mandibular edentulous patient [
3]. It involves a two-implant MISOD placed interforaminally with an optional immediate loading as the primary standard of care. In 2009, the York Consensus Statement [
4] observed that the two-implant MISOD is not the gold standard of implant therapy, but rather the minimum standard offered to edentulous patients considering masticatory performance, patient satisfaction, cost, clinical time, and patient choice [
7]. The 2015 EAO consensus conference also acknowledged that the oral health-related quality of life outcomes would improve by two or four implants MISOD [
8].
Situations where, for example, a severely compromised available oral mucosa remains in contact with the planned overdenture will dictate, among other considerations, the need for four implants rather than two [
9,
10,
11].
Kern et al.’s meta-analysis showed a preference in favor of four implants supporting MISOD over two implants with regards to long-term implant survival [
12]. That statistical finding even exceeded four implants supporting the mandibular fixed restoration. Therefore, using four implants to support an overdenture is common practice. The choice of the number of implants is affected by the following criteria: retention, patient satisfaction, implant survival, bone and tissue preservation, initial and long-term cost, complications, and aftercare [
10]. Post-insertion prosthetic maintenance requiring aftercare over time causes discomfort for the patients in addition to being costly. The two main categories of complications that may occur in implant therapy are biological and technical (mechanical). Biologic complications include implant failure, marginal bone loss, sore spots, and reduction in ridge volume. Technical complications collectively refer to mechanical damage to the implant and its components and superstructures, and they include implant fracture, wear or corrosion of the retention elements, fracture of the retentive elements or superstructure, abutment fracture, abutment screw loosening or fracture, attachment screw loosening or fracture, activation or changing of the clip, matrix activation (requiring change of rubber ring) or replacement (requiring change of ring housing), rebasing or relining of the overdenture, and repreparing overdenture due to fracture [
13,
14].
A systematic review on complications and aftercare along with patient satisfaction of MISODs revealed insignificant differences in radiographic and clinical parameters, patient satisfaction, and prosthetic complications when comparing between MISODs supported by two and four implants [
15]. A few studies had contradictory results regarding marginal bone loss and complications. Based on Roccuzo et al.’s review [
15], the third EAO Consensus Conference in 2012 also stated that there is no evidence for preferring four implants over two [
16]. Notably, however, all of the RCTs selected for review compared two non-splinted ball attachments with two or four splinted bar attachments. None of them compared between two and four non-splinted ball attachments [
17,
18,
19,
20,
21,
22,
23,
24,
25,
26,
27]. There is clinical logic for preferring an MISOD with four non-splinted implant attachments over splinted implant attachments. It requires less clinical time, and with the direct technique, as described in our former report, it is less expensive and entails fewer prosthetic elements [
28]. In addition, mandibular MISOD retained on separate implants shows a lower repair rate as well as easier oral hygiene protocol compared to splinted implant and their attachments [
29]. Furthermore, that same prosthesis requires less height in its construction, which makes its esthetical limits less challenging [
30,
31].
A more recent meta-analysis by Leao et al. found no compelling preference when comparing splinted and unsplinted implants between two or three implant cohorts in each reviewed article, assisting MISOD [
32]. Although the conclusion dealt with implant survival, marginal bone loss, and prosthetic aftercare, none of the studies reviewed compared the same attachment system between different numbers of unsplinted implants.
The purpose of this study was to compare the long-term aftercare of two-ball implant vs. four-ball implant attachment MISODs.
2. Materials and Methods
All consecutive edentulous individuals with lack of stability and insufficient retention of their existing mandibular denture who presented to the Oral Rehabilitation Department, School of Dentistry, Tel-Aviv University, between 1990 and 2010 were eligible for study participation. The Ethics Committee of Tel Aviv University approved the current study protocol. This research did not receive any financial aid from any agencies in the public, commercial, or not-for-profit sectors. The inclusion criteria for this study were complete edentulism for at least 12 months prior to presentation and class III–IV resorption of the mandible according to the Cawood & Howell classification [
33].
Forty-six patients (21 females and 25 males, age range 23–80 years, mean age 65 ± 8 years, median 66 years) were included. They were all examined and surgically treated by well experienced oral and maxillofacial surgeons/periodontists and rehabilitated by specialist prosthodontists/prosthodontic residents. Th examination included panoramic and dental c.t. scans. The patients were treated by constructing new overdentures over two or four non-splinted implants with mounted ball attachments. Each attachment was composed of a metal insert screwed into the implant and a metal housing with an elastic liner that was incorporated into the denture. Twenty-five patients were treated by two implants (Group A) and 21 by four implants (Group B).
All implants were installed under local anesthesia into the anterior interforaminal mandible in a two-stage procedure. A total of 134 (50 Group A and 84 Group B) implants were inserted. Four implant manufacturers took part in this study: MIS (Implant Technologies, Bar Lev Industry, Israel) in 13 patients, Zimmer (Zimmer Dental) in 9 patients, 3I (Implant Innovations, Biomet) in 8 patients, and Replace Select (Nobel Biocare) in 16 patients. The implant lengths were 10, 11.5, or 13 mm, depending on the height of the available bone in the mandible. Standard postoperative treatment included chlorhexidine 0.2% mouth rinses, analgesics, and antibiotics. Second stage surgery was performed 3 months after implant placement. Postoperative panoramic and orthoradial periapical radiographs were taken prior to implant uncovering. After 4 weeks, standard prosthetic treatment consisting of a new MISOD retained by ball attachments was carried out. Incorporation of the attachment into the mandibular implant overdenture was by a direct (chair-side) technique. A balanced occlusion and monoplane acrylic teeth were used in all patients. The same laboratory fabricated all the overdentures.
The patients continued their visits to the clinic for up to 20 years after their first treatment appointment, and all surgical or prosthetic interventions were recorded. Prosthetic aftercare included yearly routine recall visits during which implants, attachments apparatuses, and prostheses were checked. Additional procedures for oral hygiene support and adjustment or repair of the MISODs were provided when required.
The data recorded from the patients’ files were as follows:
The number of visits for the relief of pressure sore spots.
The number of attachment liner replacements spots.
Whether the metal ball attachment needed replacement due to wear (yes/no).
Student’s t-test and the Mann–Whitney test for continuous data and Fisher’s exact test for categorical data were used for statistical analysis. All analyses were made with SAS version 9.2 software (SAS Institute Inc., Cary, NC, USA).
3. Results
Forty-six patients were enrolled on this retrospective study that extended up to 20 years. The mean follow-up period of the entire study population was 93 ± 57 months (range 9–242 months, median 95 months). No implants were lost, yielding a survival rate of 100%. Groups A and B were comparable for mean age (64.9 years in group A and 64.6 years in group B, p = 0.915), gender distribution (males/females 16/9 in group A and 9/12 in group B, p = 0.235), and mean length of follow-up (80.6 ± 56 months in group A and 108 ± 56 months in group B, p = 0.106).
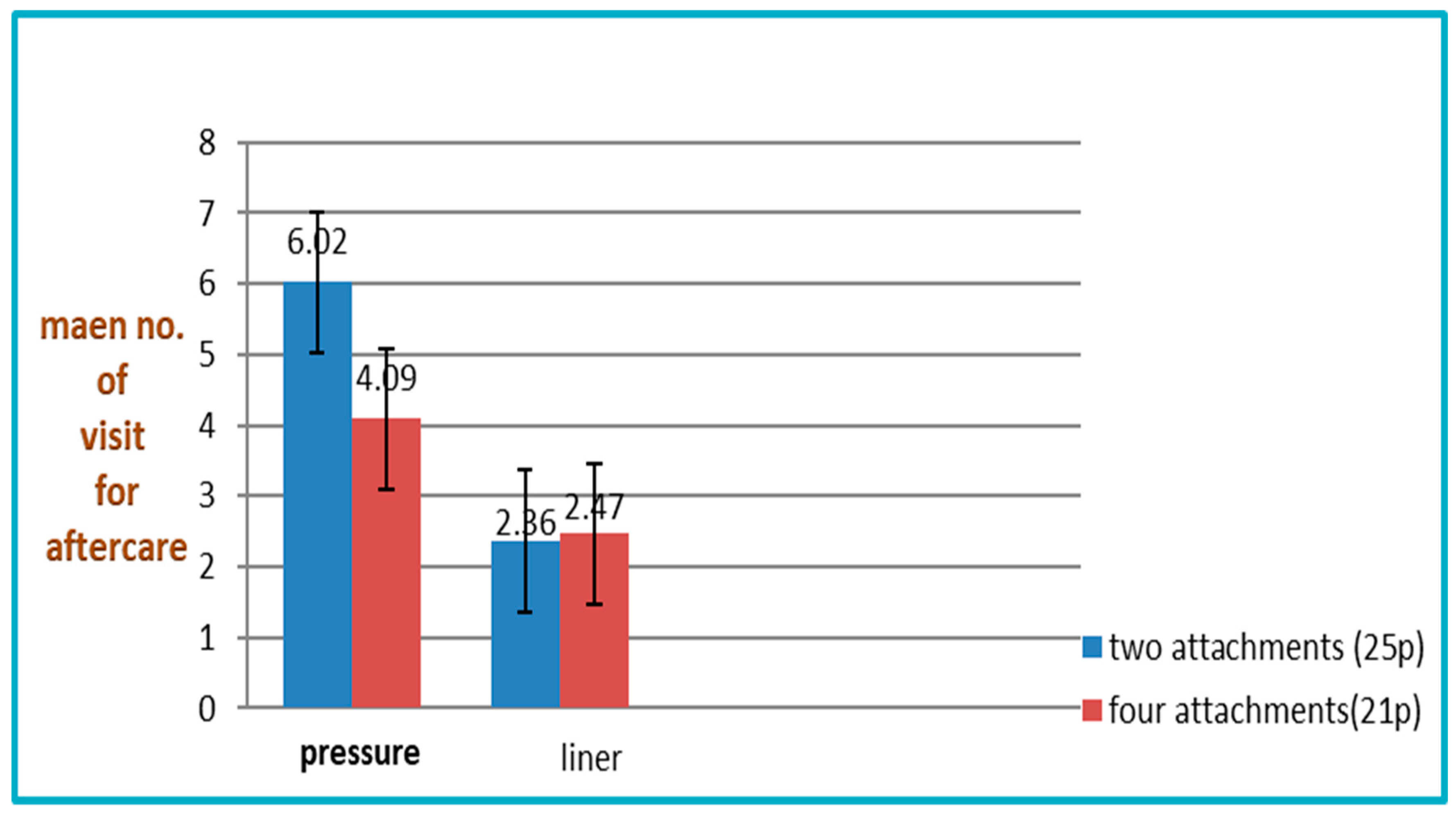
The mean number of visits due to the relief of pressure sore spots was significantly higher in Group A than in Group B (6.2 ± 2 in group A vs. 4.09 ± 1.54 in group B,
p < 0.0001) (
Table 1,
Figure 1). The other two recorded parameters were not significantly different: the number of attachment liner replacements due to loss of retention was 2.36 ± 1.84 in group A and 2.47 ± 1.63 in group B (
p = 0.814) (
Table 2,
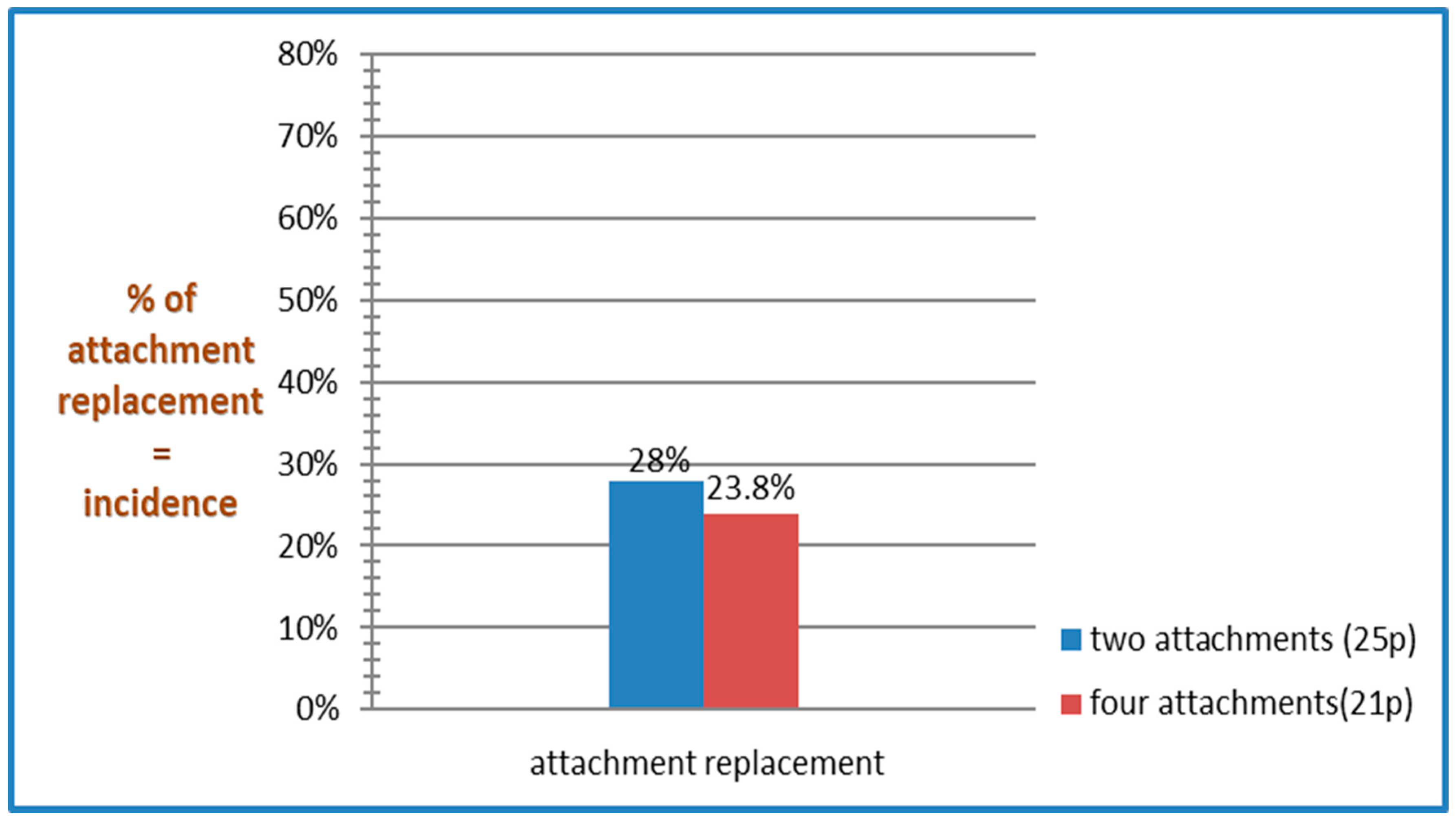
Figure 1). The number of patients for whom metal ball attachment was replaced due to wear was 7/25 (28%) in group A and 5/21 (23.8%) in group A,
p = 1.000 (
Table 3,
Figure 2).
The independent variables (group A vs. group B, respectively) including age (mean age in both groups—64 years, p = 0.915), gender (male/female—14/11 in group A vs. 9/12 in group B), implant length (mean 11.3 in group A vs. 11.6 in group B, p = 0.53), and implant manufacturer (p = 0.47) had no effect on prosthetic aftercare maintenance significantly following statistical analysis.
4. Discussion
Prosthetic aftercare of edentulous patients treated by either two- or four-implant MISODs is an important concern for their quality of life. The main findings of the present study were that two-implant MISODs required 50% more visits to relieve pressure sore spots (6.2 ± 2 visits) compared to four-implant MISOD (4.09 ±1.54 visits), which implies a significantly higher aftercare treatment capacity, with the two-implant MISODs. Conversely, the insignificant difference between the groups regarding mechanical wear of the attachments’ parts or loss of retention implies, as mentioned, no difference with the aftercare requirements in the long term.
A MISOD receives its support from the intraoral tissues and dental implants combined [
34]. It can be assumed that a mandibular overdenture retained on four implants has less tissue support and less contact with its bearing (non-implant-attached) area and the tissue underlying it and thus causes fewer pressure sore spots over time. These assumptions are verified by the findings of a prospective comparative study that examined the effect of two- vs. four-implant MISODs on mandibular posterior residual ridge reduction over a 10-year period [
27]. Moreover, the results of that study showed a significantly greater residual ridge resorption in the two-implant group due to the rotation of the MISOD around the two-implant axis, thus applying greater pressure on the soft tissues and the residual ridge posterior to that axis. In contrast, a four-implant MISOD is supported mainly by the implants and has limited ability to rotate.
In the present study, the two groups of patients needed a similar number of attachment liner replacements (2.36 for Group A and 2.47 for Group B,
p = 0.8,
Figure 1). Additionally, the rate of patients who needed metal ball replacement was similar (7/25 [28%] in group A and 5/21 [23.8%] in group B,
p = 1.000,
Figure 2). Meijer et al.’s prospective study compared two-bar with four-bar-retained MISODs and demonstrated a comparable need for treatment of loss of retention after 10 years of follow-up [
23,
35]. Their two-implant group needed 2.0 retention-improving appointments, and their four-implant group needed 2.35 appointments (
p = NS). The results of the present study fall well within this range. Furthermore, the mean number of visits intended to treat pressure spots was 0.93 (+/−1.17) with the four-implant group in comparison to 1.30 (+/−1.18) with the two-implant group. This may imply the superiority of using four implants MISOD with limited rotation, which leads to decreased patient’s discomfort. On the other hand, an 8-year follow-up RCT by Stoker et al. [
22] reported a significantly higher number of visits in two-ball attachment MISODs (6.7 ± 5.2) vs. four-bar retained MISODs (3.1 ± 3.2,
p = 0.018). The higher aftercare rate found in their study may have been, however, due to the inclusion of denture base adjustments and attachment reactivation. To date, the largest systematic review concerning prosthetic aftercare with MISODs summarized in one of its conclusions that implant number has no clear effect on the complication rate [
14]. That same review, however, took into account the technical aftercare procedures, not the pain-relieving supportive treatment.
The OHQoL of denture users may be affected by several factors, including the appearance of sore spots and loss of retention, which are reported in the present study. Although our patients had not filled in OHRQoL questionnaires, we can assume that a patient’s QoL is an outcome of those sequelae. The presence of pressure sore spots is not uncommon, as one clinical study by Bilhan et al. [
36] reported, with a 22% incidence of pressure sore spots during a single year use of MISOD (12/59 patients).
In this study, the 50% excess visits for sore spots in the two-implant MISODs compared with the four-implant MISODs would inevitably result in better OHRQoL scores for the latter group. On the other hand, the retentivity of the two-implant MISODs compared to the four-implant MISODs would likely lead to a comparable OHRQoL for both treatment options, especially in the long-term aftercare needs. Several studies have dealt with the OHQoL of patients treated by MISODs, and their findings are contradictory. Karbach et al. treated 30 patients with locator-retained mandibular overdentures [
31]. Those authors randomly assigned one-half of the patients to begin with two-implant MISODs and were then switched to four-implant MISODs, and the other half to begin with four MISODs and switched to two MISODs. They measured subjective OHRQoL by having the participants fill in questionnaires, and the results revealed higher (
p = 0.026) patient satisfaction when the four-implant MISODs were used. Similar findings of a better QoL in the four-bar-retained overdentures compared with two single-ball attachments were reported by Mumco et al. [
37]. They further reported that patient satisfaction was not related to the number of implants nor to the type of attachment system. In contrast, in their research, Meijer et al. reported on two groups, each with 30 patients treated with either two intramobile cylinder (IMZ) implants and four IMZ implants in the edentulous mandible [
23]. All of those patients were treated with bar-retained overdentures, and in both groups, satisfaction rates were quite identical. In a short-term prospective, randomized crossover clinical trial by Burns et al. [
27], 30 subjects received four interforaminal mandibular implants. Three different attachment types were delivered and/or fitted to the implants for each subject: four-implant bar, two-implant bar, and two-ball attachments. Each subject experienced all three attachment types for approximately 1 year. The two-ball attachment resulted in equivalent or more favorable treatment outcomes for most measured parameters compared with the two- and four-implant bar attachments. The four-implant bar treatment provided greater prosthesis retention than the other treatment types in that study, but after the experience with all three systems, most of the subjects chose the two-ball attachment as their favorable prosthesis at the conclusion of the investigation. A different preference was reported in another crossover study where patients wore both two-implant MISOD and four-implant MISOD and preferred the latter in an OHIP-14 questionnaire [
38]. As in this research, all implants were separate, but unlike this study, two implants were positioned posterior to the interforaminal area, and all received locator attachments.
5. Conclusions
Within the limitations (retrospective, one center, single attachment system examined) of this study, it may be concluded that the four-ball attachment MISODs proved themselves more advantageous than two-ball attachments MISODs resulting in fewer pressure sore spots throughout the long-term aftercare period. However, the number of implants assisting MISOD has no effect on mechanical wear.
Author Contributions
Conceptualization: J.N., O.R., and E.Z.; Data collection: O.R., E.Z., H.H., J.N., G.M. and S.H.-N.; Formal analysis: O.R., H.H., G.M. and A.G.; Methodology: O.R., J.N., G.M. and S.M.; Writing—original draft: O.R., E.Z., H.H. and S.H.-N.; Writing—review and editing: O.R., E.Z., H.H., A.G., S.M., J.N. and G.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of the Tel Aviv University.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Van Waas, M.A. The influence of clinical variables on patients’ satisfaction with complete dentures. J. Prosthet. Dent. 1990, 63, 307–310. [Google Scholar] [CrossRef]
- Locker, D. Patient-based assessment of the outcomes of implant therapy: A review of the literature. Int. J. Prosthodont. 1998, 11, 453–461. [Google Scholar]
- Feine, J.S.; Carlsson, G.E.; Awad, M.A.; Chehade, A.; Duncan, W.J.; Gizani, S.; Head, T.; Lund, J.P.; MacEntee, M.; Mericske-Stern, R.; et al. The McGill consensus statement on overdentures. Mandibular two-implant overdentures as first choice standard of care for edentulous patients. Int. J. Oral Maxillofac. Implant. 2002, 17, 601–602. [Google Scholar]
- Thomason, J.M.; Feine, J.; Exley, C.; Moynihan, P.; Müller, F.; Naert, I. Mandibular two implant-supported overdentures as the first choice standard of care for edentulous patients—The York Consensus Statement. Br. Dent. J. 2009, 207, 185–186. [Google Scholar] [CrossRef]
- Engquist, B.; Bergendal, T.; Kallus, T.; Linden, U. A retrospective multicenter evaluation of osseointegrated implants supporting overdentures. Int. J. Oral Maxillofac. Implant. 1988, 3, 129–134. [Google Scholar]
- Rentsch-Kollar, A.; Huber, S.; Mericske-Stern, R. Mandibular implant overdentures followed for over 10 years: Patient compliance and prosthetic maintenance. Int. J. Prosthodont. 2010, 23, 91–98. [Google Scholar] [CrossRef]
- Thomason, J.M.; Kelly, S.A.M.; Bendkowski, A.; Ellis, J.S. Two implant retained overdentures—A review of the literature supporting the McGill and York consensus statements. J. Dent. 2012, 40, 22–34. [Google Scholar] [CrossRef]
- Beikler, T.; Flemmig, T.F. EAO consensus conference: Economic evaluation of implant- supported prostheses. Clin. Oral Implants Res. 2015, 26 (Suppl. 11), 57–63. [Google Scholar] [CrossRef]
- Payne, G.T.; Zarb, G. Prosthodontic Treatment for Edentulous Patients: Complete Dentures and Implant-Supported Prostheses; Elsevier: St. Louis, MO, USA, 2012; p. 334. [Google Scholar]
- Stellingsma, K.; Raghoeber, G.M.; Visser, A.; Vissink, A.; Meijer, H. The extremely Resorbed mandible, 10-year results of a randomized controlled trial on Treatment strategies. Clin. Oral Implants Res. 2014, 25, 926–932. [Google Scholar] [CrossRef]
- Krennmair, G.; Suto, D.; Seemann, R.; Piehslinger, E. Removable four implant-supported mandibular overdentures rigidly retained with telescopic crowns or milled bars: A 3- year prospective study. Clin. Oral. Implants Res. 2012, 23, 481–488. [Google Scholar] [CrossRef]
- Kern, J.S.; Kern, T.; Wolfart, S.; Heussen, N. A systematic review and meta-analysis of removable and fixed implant-supported prostheses in edentulous jaws: Post-loading implant loss. Clin. Oral Implants Res. 2016, 27, 174–195. [Google Scholar] [CrossRef]
- Goodacre, C.J.; Bernal, G.; Rungcharassaeng, K.; Kan, J.Y. Clinical complications with implants and implant prostheses. J. Prosthet. Dent. 2003, 90, 121–132. [Google Scholar] [CrossRef]
- Assaf, A.; Daas, M.; Boittin, A.; Eid, N.; Postaire, M. Prosthetic maintenance of different mandibular implant overdentures: A systematic review. J. Prosthet. Dent. 2017, 118, 144–152. [Google Scholar] [CrossRef]
- Roccuzzo, M.; Bonino, F.; Gaudioso, L.; Zwahlen, M.; Meijer, H.J.A. What is the optimal number of implants for removable reconstructions? A systematic review on implant-supported overdentures. Clin. Oral Implants Res. 2012, 23, 229–237. [Google Scholar] [CrossRef]
- Gotfredsen, K.; Wiskott, A. Working Group Consensus report—Reconstructions on implants. The Third EAO Consensus Conference. Clin. Oral Implants Res. 2012, 23, 238–241. [Google Scholar] [CrossRef]
- Wismeijer, D.; Van Waas, M.A.; Vermeeren, J.I.; Mulder, J.; Kalk, W. Patient satisfaction with implant-supported mandibular overdentures. A comparison of three treatment strategies with ITI-dental implants. Int. J. Oral. Maxillofac. Surg. 1997, 26, 263–267. [Google Scholar] [CrossRef]
- Batenburg, R.H.; Meijer, H.J.; Raghoebar, G.M.; Vissink, A. Treatment concept for mandibular overdentures supported by endosseous implants: A literature review. Int. J. Oral Maxillofac. Implants 1998, 13, 539–545. [Google Scholar]
- Wismeijer, D.; van Waas, M.A.; Mulder, J.; Vermeeren, J.I.; Kalk, W. Clinical and radiological results of patients treated with three treatment modalities for overdentures on implants of the ITI Dental Implant System. A randomized controlled clinical trial. Clin. Oral Implants Res. 1999, 10, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Timmerman, R.; Stoker, G.T.; Wismeijer, D.; Oosterveld, P.; Vermeeren, J.I.J.F.; van Waas, M.A.J. An Eight-year Follow-up to a Randomized Clinical Trial of Participant Satisfaction with Three Types of Mandibular Implant-retained Overdentures. J. Dent. Res. 2004, 83, 630–633. [Google Scholar] [CrossRef]
- Visser, A.; Raghoebar, G.M.; Meijer, H.J.A.; Batenburg, R.H.K.; Vissink, A. Mandibular overdentures supported by two or four endosseous implants: A 5-year prospective study. Clin. Oral Implants Res. 2005, 16, 19–25. [Google Scholar] [CrossRef]
- Stoker, G.T.; Wismeijer, D.; van Waas, M.A.J. An eight-year follow-up to a randomized clinical trial of aftercare and cost-analysis with three types of mandibular implant-retained overdentures. J. Dent. Res. 2007, 86, 276–280. [Google Scholar] [CrossRef] [PubMed]
- Meijer, H.J.A.; Raghoebar, G.M.; Batenburg, R.H.K.; Visser, A.; Vissink, A. Mandibular overdentures supported by two or four endosseous implants: A 10-year clinical trial. Clin. Oral Implants Res. 2009, 20, 722–728. [Google Scholar] [CrossRef] [PubMed]
- Walton, J.N.; Glick, N.; Macentee, M.I. A randomized clinical trial comparing patient satisfaction and prosthetic outcomes with mandibular overdentures retained by one or two implants. Int. J. Prosthodont. 2009, 22, 331–339. [Google Scholar]
- Kronstrom, M.; Davis, B.; Loney, R.; Gerrow, J.; Hollender, L. A prospective randomized study on the immediate loading of mandibular overdentures supported by one or two implants: A 12-month follow-up report. Int. J. Oral Maxillofac. Implants 2009, 25, 181–188. [Google Scholar]
- Stoker, G.; van Waas, R.; Wismeijer, D. Long-term outcomes of three types of implant-supported mandibular overdentures in smokers. Clin. Oral Implants Res. 2012, 23, 925–929. [Google Scholar] [CrossRef]
- Burns, D.R.; Unger, J.W.; Coffey, J.P.; Waldrop, T.C.; Elswick, R.K.; Ronald, K. evaluation of prosthodontic modalities for mandibular implant overdenture treatment. J. Prosthet. Dent. 2011, 106, 12–22. [Google Scholar] [CrossRef]
- Nissan, J.; Oz-Ari, B.; Gross, O.; Ghelfan, O.; Chaushu, G. Long-term prosthetic aftercare of direct vs. indirect attachment incorporation techniques to mandibular implant-supported overdenture. Clin. Oral Implants Res. 2011, 22, 627–630. [Google Scholar] [CrossRef]
- Kleis, W.K.; Kammerer, P.W.; Hartmann, S.; Al-Nawas, B.; Wagner, W. A comparison of three different attachment systems for mandibular two implant overdentures: One-year report. Clin. Implant Dent. Relat. Res. 2010, 12, 209–218. [Google Scholar] [CrossRef]
- Eitner, S.; Schlegel, A.; Emeka, N.; Holst, S.; Will, J.; Hamel, J. Comparing bar and double—Crown attachments in implant-retained prosthetic reconstruction: A follow-up investigation. Clin. Oral Implants Res. 2008, 19, 530–537. [Google Scholar] [CrossRef]
- Karbach, J.; Hartmann, S.; Jahn-Eimermacher, A.; Wagner, W. Oral Health-Related Quality of Life in edentulous. Patients with Two- vs Four-Locator-Retained Mandibular Overdentures: A Prospective, Randomized, Crossover Study. Int. J. Oral Maxillofac. Implant. 2015, 30, 1143–1148. [Google Scholar] [CrossRef] [Green Version]
- Leão, R.S.; Moraes, S.L.D.; Vasconcelos, B.C.E.; Lemos, C.A.A.; Pellizzer, E.P. Splinted and unsplinted overdenture attachment systems: A systematic review and meta-analysis. J. Oral Rehabil. 2018, 45, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Cawood, J.I.; Howell, R.A. A classification of the edentulous jaws. Int. J. Oral Maxillofac. Surg. 1988, 17, 232–236. [Google Scholar] [CrossRef]
- Simon, H.; Yanase, T. Terminology for Implant Prostheses. Int. J. Oral Maxillofac. Implants 2003, 18, 539–543. [Google Scholar] [CrossRef] [PubMed]
- De Jong, M.H.M.; Wright, P.S.; Meijer, H.J.A.; Tymstra, N. Posterior mandibular residual ridge resorption in patients with overdentures supported by two or four endosseous implants in a 10-year prospective comparative study. Int. J. Oral Maxillofac. Implant. 2010, 25, 1168–1174. [Google Scholar]
- Bilhan, H.; Geckili, O.; Mumcu, E.; Bilmenoglu, C. Maintenance Requirements Associated with Mandibular Implant Overdentures: Clinical Results After First Year of Service. J. Oral Implantolog. 2011, 37, 697–704. [Google Scholar] [CrossRef]
- Mumcu, E.; Bilhan, H.; Geckili, O. The effect of attachment type and implant number on satisfaction and quality of life of mandibular implant-retained overdenture wearers. Gerodontology 2012, 29, e618–e623. [Google Scholar] [CrossRef]
- Le, G. A Quality-of-Life Comparison between 2-Implants and 4-Implants Retained Mandibular Overdenture: A Pilot Randomized Controlled Crossover Trial. Master’s Thesis, The University of Texas Health Science Center School of Dentistry, Houston, TX, USA, 2015. [Google Scholar]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).



 ,
, 



{kind=link}
{kind=link}