
Electronic Cigarettes’ Toxicity: From Periodontal Disease to Oral Cancer


 ,
,
Abstract
:1. Introduction
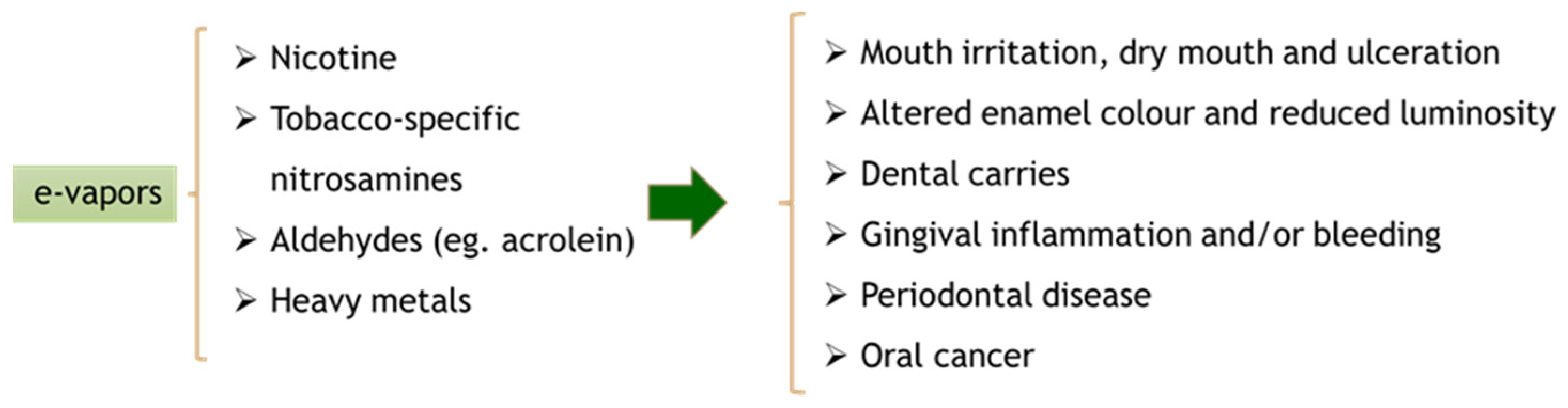
2. Effects of Electronic Cigarettes on the Oral Cavity
3. Potential Mechanisms Involved in Oral Cancer Development Associated with Electronic Cigarette Smoking
3.1. Oxidative Stress
3.2. Inflammatory Response
3.3. DNA Damage and Genotoxic Mechanism
3.4. Genetic and Epigenetic Alterations
4. Chemical Composition of e-Liquids and Vapors and the Implications in Oral Carcinogenesis
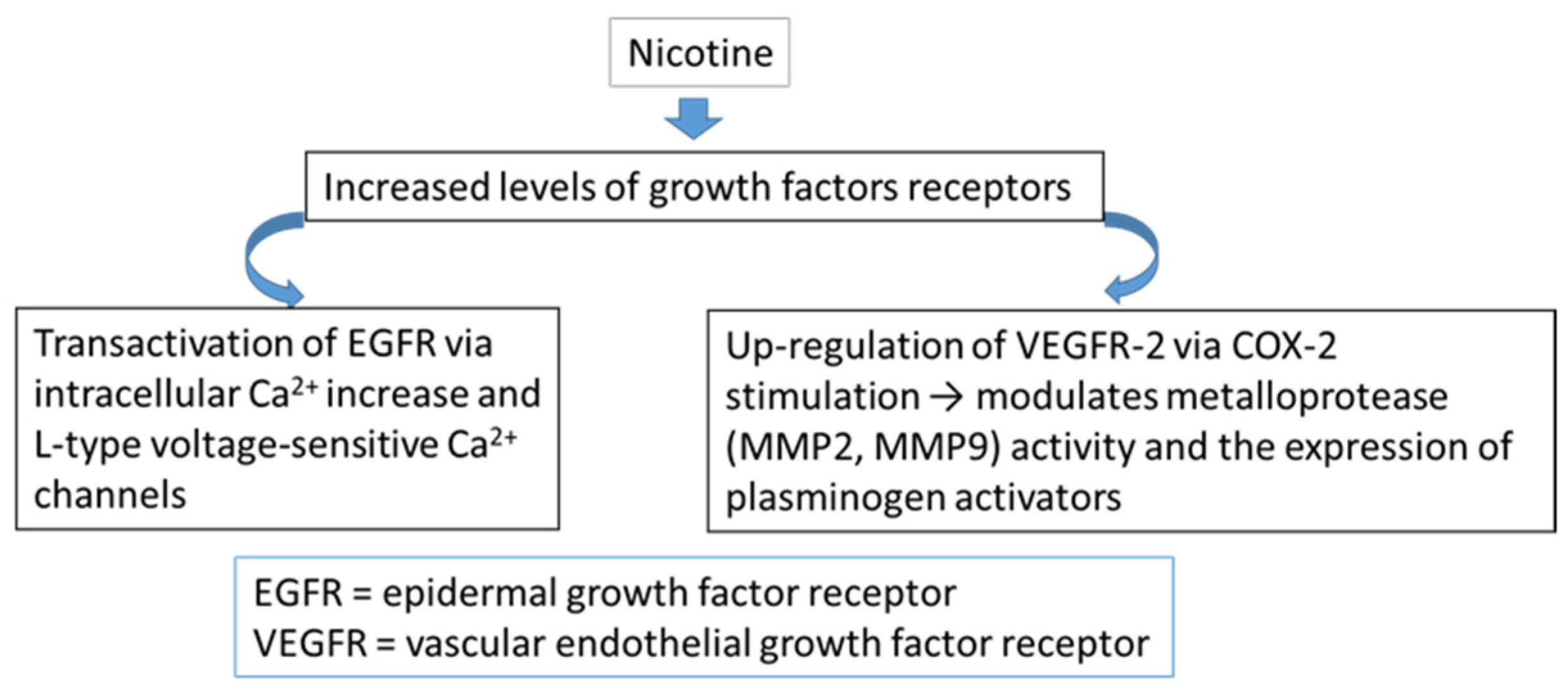
4.1. Nicotine
4.2. Propylene Glycol and Glycerol
4.3. Flavoring Agents
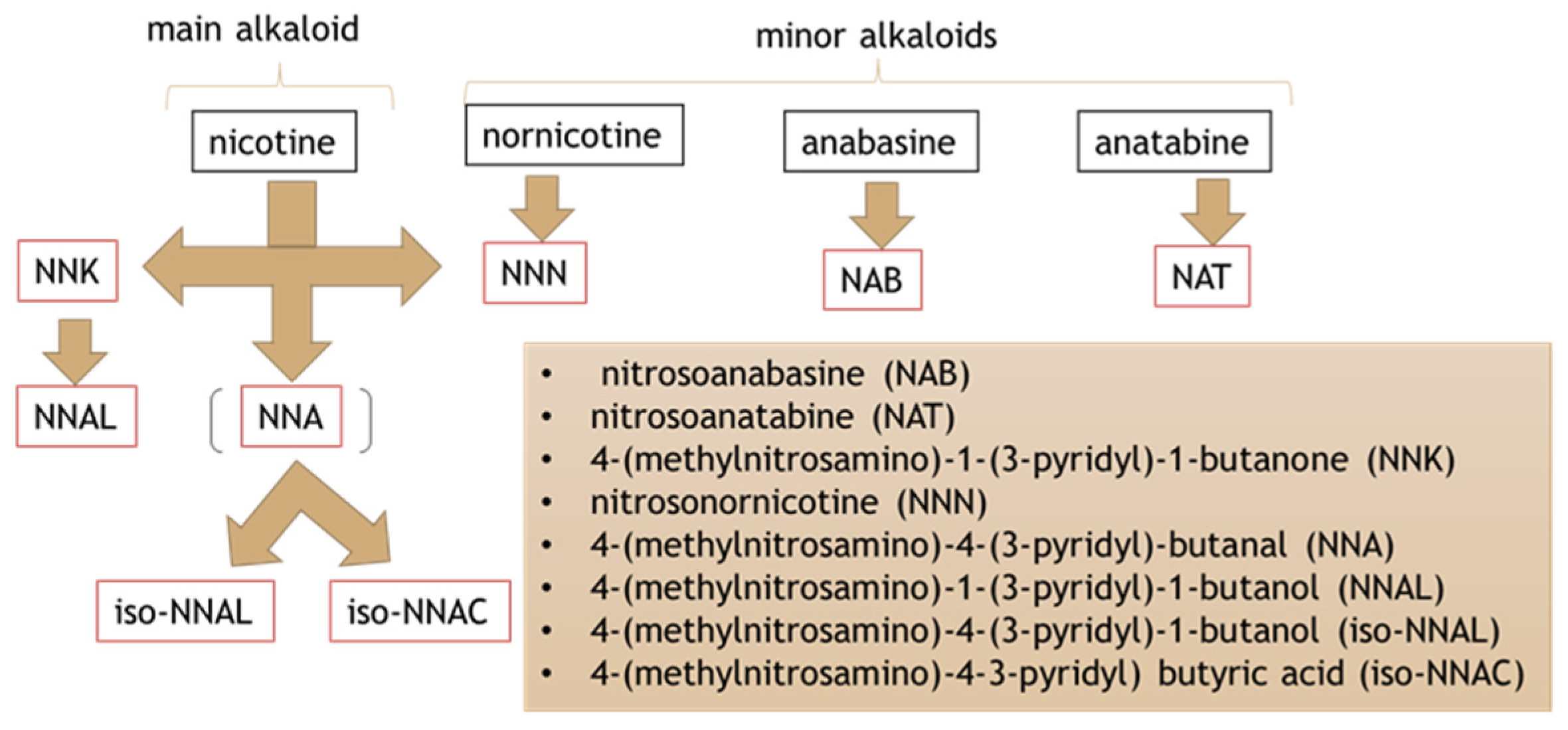
4.4. Tobacco-Specific Nitrosamines
4.5. Heavy Metals
5. Nicotine’s Influence on Chemotherapy Drug Resistance
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kumar, P.; Geisinger, M.; DeLong, H.R.; Lipman, R.D.; Araujo, M.W.B. Living under a cloud: Electronic cigarettes and the dental patient. J. Am. Dent. Assoc. 2020, 151, 155–158. [Google Scholar] [CrossRef] [Green Version]
- Sundar, I.K.; Javed, F.; Romanos, G.E.; Rahman, I. E-cigarettes and flavorings induce inflammatory and pro-senescence responses in oral epithelial cells and periodontal fibroblasts. Oncotarget 2016, 7, 77196–77204. [Google Scholar] [CrossRef] [Green Version]
- Kaur, G.; Pinkston, R.; Mclemore, B.; Dorsey, W.C.; Batra, S. Immunological and toxicological risk assessment of e-cigarettes. Eur. Respir. Rev. 2018, 27, 170119. [Google Scholar] [CrossRef]
- Holliday, R.; Chaffee, B.W.; Jakubovics, N.S.; Kist, R.; Preshaw, P.M. Electronic Cigarettes and Oral Health. J. Dent. Res. 2021, 100, 906–913. [Google Scholar] [CrossRef] [PubMed]
- Huilgol, P.; Bhatt, S.P.; Biligowda, N.; Wright, N.C.; Wells, J.M. Association of e-cigarette use with oral health: A population-based cross-sectional questionnaire study. J. Public Health 2019, 41, 354–361. [Google Scholar] [CrossRef]
- Rouabhia, M. Impact of Electronic Cigarettes on Oral Health: A Review. J. Can. Dent. Assoc. 2020, 86, k7. [Google Scholar] [PubMed]
- Wadia, R.; Booth, V.; Yap, H.F.; Moyes, D.L. A pilot study of the gingival response when smokers switch from smoking to vaping. Br. Dent. J. 2016, 221, 722–726. [Google Scholar] [CrossRef] [PubMed]
- Mokeem, S.A.; Alasqah, M.N.; Michelogiannakis, D.; Al-Kheraif, A.A.; Romanos, G.E.; Javed, F. Clinical and radiographic periodontal status and whole salivary cotinine, IL-1β and IL-6 levels in cigarette- and waterpipe-smokers and E-cig users. Environ. Toxicol. Pharmacol. 2018, 61, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Javed, F.; Abduljabbar, T.; Vohra, F.; Malmstrom, H.; Rahman, I.; Romanos, G.E. Comparison of Periodontal Parameters and Self-Perceived Oral Symptoms Among Cigarette Smokers, Individuals Vaping Electronic Cigarettes, and Never-Smokers. J. Periodontol. 2017, 88, 1059–1065. [Google Scholar] [CrossRef]
- Ralho, A.; Coelho, A.; Ribeiro, M.; Paula, A.; Amaro, I.; Sousa, J.; Marto, C.; Ferreira, M.; Carrilho, E. Effects of Electronic Cigarettes on Oral Cavity: A Systematic Review. J. Evid. Based Dent. Pract 2019, 19, 101318. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Allam, E.; Zhang, W.; Al-Shibani, N.; Sun, J.; Labban, N.; Song, F.; Windsor, L.J. Effects of cigarette smoke condensate on oral squamous cell carcinoma cells. Arch. Oral Biol. 2011, 56, 1154–1161. [Google Scholar] [CrossRef] [PubMed]
- Katarkar, A.; Patel, L.; Mukherjee, S.; Ray, J.G.; Haldar, P.K.; Chaudhuri, K. Association of oral tumor suppressor gene deleted in oral cancer-1 (DOC-1) in progression of oral precancer to cancer. Oral Sci. Int. 2015, 12, 15–21. [Google Scholar] [CrossRef] [Green Version]
- Yao, Q.W.; Zhou, D.S.; Peng, H.J.; Ji, P.; Liu, D.S. Association of periodontal disease with oral cancer:a meta-analysis. Tumour. Biol. 2014, 35, 7073–7077. [Google Scholar] [CrossRef] [PubMed]
- Zeng, X.T.; Deng, A.P.; Li, C.; Xia, L.Y.; Niu, Y.M.; Leng, W.D. Periodontal disease and risk of head and neck cancer: A meta-analysis of observational studies. PLoS ONE 2013, 8, e79017. [Google Scholar] [CrossRef]
- Lu, M.; Xuan, S.; Wang, Z. Oral microbiota: A new view of body health. Food Sci. Hum. Wellness 2019, 8, 8–15. [Google Scholar] [CrossRef]
- Almeida-da-Silva, C.L.C.; Matshik Dakafay, H.; O’Brien, K.; Montierth, D.; Xiao, N.; Ojcius, D.M. Effects of electronic cigarette aerosol exposure on oral and systemic health. Biomed. J. 2021, 44, 252–259. [Google Scholar] [CrossRef]
- Radaic, A.; Kapila, Y.L. The oralome and its dysbiosis: New insights into oral microbiome-host interactions. Comput. Struct. Biotechnol. J. 2021, 19, 1335–1360. [Google Scholar] [CrossRef]
- Pushalkar, S.; Paul, B.; Li, Q.; Yang, J.; Vasconcelos, R.; Makwana, S.; González, J.M.; Shah, S.; Xie, C.; Janal, M.N.; et al. Electronic Cigarette Aerosol Modulates the Oral Microbiome and Increases Risk of Infection. iScience 2020, 23, 100884. [Google Scholar] [CrossRef] [Green Version]
- Ganesan, S.M.; Dabdoub, S.M.; Nagaraja, H.N.; Scott, M.L.; Pamulapati, S.; Berman, M.L.; Shields, P.G.; Wewers, M.E.; Kumar, P.S. Adverse effects of electronic cigarettes on the disease-naive oral microbiome. Sci. Adv. 2020, 6, eaaz0108. [Google Scholar] [CrossRef]
- Javed, F.; Warnakulasuriya, S. Is there a relationship between periodontal disease and oral cancer? A systematic review of currently available evidence. Crit. Rev. Oncol. Hematol. 2016, 97, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Sahingur, S.E.; Yeudall, W.A. Chemokine function in periodontal disease and oral cavity cancer. Front. Immunol. 2015, 6, 214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tommasi, S.; Caliri, A.W.; Caceres, A.; Moreno, D.E.; Li, M.; Chen, Y.; Siegmund, K.D.; Besaratinia, A. Deregulation of Biologically Significant Genes and Associated Molecular Pathways in the Oral Epithelium of Electronic Cigarette Users. Int. J. Mol. Sci. 2019, 20, 738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vairaktaris, E.; Yapijakis, C.; Serefoglou, Z.; Derka, S.; Vassiliou, S.; Nkenke, E.; Vylliotis, A.; Wiltfang, J.; Avgoustidis, D.; Critselis, E.; et al. The interleukin-8 (-251A/T) polymorphism is associated with increased risk for oral squamous cell carcinoma. Eur. J. Surg. Oncol. 2007, 33, 504–507. [Google Scholar] [CrossRef] [PubMed]
- Cordero, O.J.; Varela-Calviño, R. Oral hygiene might prevent cancer. Heliyon 2018, 4, e00879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merecz-Sadowska, A.; Sitarek, P.; Zielinska-Blizniewska, H.; Malinowska, K.; Zajdel, K.; Zakonnik, L.; Zajdel, R. A Summary of In Vitro and In Vivo Studies Evaluating the Impact of E-Cigarette Exposure on Living Organisms and the Environment. Int. J. Mol. Sci. 2020, 21, 652. [Google Scholar] [CrossRef] [Green Version]
- Lucas, J.H.; Muthumalage, T.; Wang, Q.; Friedman, M.R.; Friedman, A.E.; Rahman, I. E-Liquid Containing a Mixture of Coconut, Vanilla, and Cookie Flavors Causes Cellular Senescence and Dysregulated Repair in Pulmonary Fibroblasts: Implications on Premature Aging. Front. Physiol. 2020, 11, 924. [Google Scholar] [CrossRef]
- Munther, S. The effects of cigarette smoking and exercise on total salivary antioxidant activity. Saudi Dent. J. 2019, 31, 31–38. [Google Scholar] [CrossRef]
- Dalle-Donne, I.; Garavaglia, M.L.; Colombo, G.; Astori, E.; Lionetti, M.C.; La Porta, C.A.M.; Santucci, A.; Rossi, R.; Giustarini, D.; Milzani, A. Cigarette smoke and glutathione: Focus on in vitro cell models. Toxicol. In Vitro 2020, 65, 104818. [Google Scholar] [CrossRef]
- Lerner, C.A.; Sundar, I.K.; Watson, R.M.; Elder, A.; Jones, R.; Done, D.; Kurtzman, R.; Ossip, D.J.; Robinson, R.; McIntosh, S.; et al. Environmental health hazards of e-cigarettes and their components: Oxidants and copper in e-cigarette aerosols. Environ. Pollut. 2015, 198, 100–107. [Google Scholar] [CrossRef] [Green Version]
- Lerner, C.A.; Rutagarama, P.; Ahmad, T.; Sundar, I.K.; Elder, A.; Rahman, I. Electronic cigarette aerosols and copper nanoparticles induce mitochondrial stress and promote DNA fragmentation in lung fibroblasts. Biochem. Biophys. Res. Commun. 2016, 477, 620–625. [Google Scholar] [CrossRef] [Green Version]
- Isik Andrikopoulos, G.; Zagoriti, Z.; Topouzis, S.; Poulas, K. Oxidative stress induced by electronic nicotine delivery systems (ENDS): Focus on respiratory system. Curr. Opin. Toxicol. 2019, 13, 81–89. [Google Scholar] [CrossRef]
- Isik Andrikopoulos, G.; Farsalinos, K.; Poulas, K. Electronic Nicotine Delivery Systems (ENDS) and Their Relevance in Oral Health. Toxics 2019, 7, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faridoun, A. A Comparison of the Levels of Salivary Biomarkers between Conventional Smokers and Electronic Cigarette Users (A Pilot Study). Master’s Thesis, Biomedical Sciences-Dental School University of Maryland, Baltimore, MD, USA, 2019. [Google Scholar]
- Peng, H.Y.; Hsiao, J.R.; Chou, S.T.; Hsu, Y.M.; Wu, G.H.; Shieh, Y.S.; Shiah, S.G. MiR-944/CISH mediated inflammation via STAT3 is involved in oral cancer malignance by cigarette smoking. Neoplasia 2020, 22, 554–565. [Google Scholar] [CrossRef] [PubMed]
- Alanazi, H.; Park, H.J.; Chakir, J.; Semlali, A.; Rouabhia, M. Comparative study of the effects of cigarette smoke and electronic cigarettes on human gingival fibroblast proliferation, migration and apoptosis. Food Chem. Toxicol. 2018, 118, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Willershausen, I.; Wolf, T.; Weyer, V.; Sader, R.; Ghanaati, S.; Willershausen, B. Influence of E-smoking liquids on human periodontal ligament fibroblasts. Head Face Med. 2014, 10, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, V.; Rahimy, M.; Korrapati, A.; Xuan, Y.; Zou, A.E.; Krishnan, A.R.; Tsui, T.; Aguilera, J.A.; Advani, S.; Crotty Alexander, L.E.; et al. Electronic cigarettes induce DNA strand breaks and cell death independently of nicotine in cell lines. Oral Oncol. 2016, 52, 58–65. [Google Scholar] [CrossRef] [Green Version]
- Schwarzmeier, L.Â.T.; da Cruz, B.S.; Ferreira, C.C.P.; Carvalho, B.F.D.C.; Alves, M.G.O.; Lima Carta, C.F.; Scholz, J.R.; Almeida, J.D. E-cig might cause cell damage of oral mucosa. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 131, 435–443. [Google Scholar] [CrossRef]
- Argentin, G.; Cicchetti, R. Genotoxic and antiapoptotic effect of nicotine on human gingival fibroblasts. Toxicol. Sci. 2004, 79, 75–81. [Google Scholar] [CrossRef] [Green Version]
- Ginzkey, C.; Steussloff, G.; Koehler, C.; Burghartz, M.; Scherzed, A.; Hackenberg, S.; Hagen, R.; Kleinsasser, N.H. Nicotine derived genotoxic effects in human primary parotid gland cells as assessed in vitro by comet assay, cytokinesis-block micronucleus test and chromosome aberrations test. Toxicol. In Vitro 2014, 28, 838–846. [Google Scholar] [CrossRef]
- Javed, F.; Kellesarian, S.V.; Sundar, I.K.; Romanos, G.E.; Rahman, I. Recent updates on electronic cigarette aerosol and inhaled nicotine effects on periodontal and pulmonary tissues. Oral Dis. 2017, 23, 1052–1057. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.C.; Valerio, L.G., Jr. Investigating DNA adduct formation by flavor chemicals and tobacco byproducts in electronic nicotine delivery system (ENDS) using in silico approaches. Toxicol. Appl. Pharmacol. 2020, 398, 115026. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, M.; Kusama, K.; Sakashita, H. Molecular insights into the proliferation and progression mechanisms of the oral cancer: Strategies for the effective and personalized therapy. Jpn. Dent. Sci. Rev. 2012, 48, 23–41. [Google Scholar] [CrossRef] [Green Version]
- Vo, J.N.; Cieslik, M.; Zhang, Y.; Shukla, S.; Xiao, L.; Zhang, Y.; Wu, Y.M.; Dhanasekaran, S.M.; Engelke, C.G.; Cao, X.; et al. The Landscape of Circular RNA in Cancer. Cell 2019, 176, 869–881.e13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, W.; Shen, Y.; Wang, Y.; Wang, F.; Hong, X.; Chen, Y.; Lin, Y.; Yang, H. circPHIP promotes oral squamous cell carcinoma progression by sponging miR-142-5p and regulating PHIP and ACTN4 expression. Mol. Ther. Nucleic Acids 2020, 23, 185–199. [Google Scholar] [CrossRef]
- Singh, K.P.; Maremanda, K.P.; Li, D.; Rahman, I. Exosomal microRNAs are novel circulating biomarkers in cigarette, waterpipe smokers, E-cigarette users and dual smokers. BMC Med. Genom. 2020, 13, 128. [Google Scholar] [CrossRef]
- Solleti, S.K.; Bhattacharya, S.; Ahmad, A.; Wang, Q.; Mereness, J.; Rangasamy, T.; Mariani, T.J. MicroRNA expression profiling defines the impact of electronic cigarettes on human airway epithelial cells. Sci. Rep. 2017, 7, 1081. [Google Scholar] [CrossRef]
- Sewer, A.; Zanetti, F.; Iskandar, A.R.; Guedj, E.; Dulize, R.; Peric, D.; Bornand, D.; Mathis, C.; Martin, F.; Ivanov, N.V.; et al. A meta-analysis of microRNAs expressed in human aerodigestive epithelial cultures and their role as potential biomarkers of exposure response to nicotine-containing products. Toxicol. Rep. 2020, 7, 1282–1295. [Google Scholar] [CrossRef]
- Xie, Z.; Rahman, I.; Goniewicz, M.L.; Li, D. Perspectives on Epigenetics Alterations Associated with Smoking and Vaping. Function 2021, 2, zqab022. [Google Scholar] [CrossRef]
- Armendáriz-Castillo, I.; Guerrero, S.; Vera-Guapi, A.; Cevallos-Vilatuña, T.; García-Cárdenas, J.M.; Guevara-Ramírez, P.; López-Cortés, A.; Pérez-Villa, A.; Yumiceba, V.; Zambrano, A.K.; et al. Genotoxic and Carcinogenic Potential of Compounds Associated with Electronic Cigarettes: A Systematic Review. BioMed Res. Int. 2019, 2019, 1386710. [Google Scholar] [CrossRef] [Green Version]
- Sancilio, S.; Gallorini, M.; Cataldi, A.; Sancillo, L.; Rana, R.A.; di Giacomo, V. Modifications in Human Oral Fibroblast Ultrastructure, Collagen Production, and Lysosomal Compartment in Response to Electronic Cigarette Fluids. J. Periodontol. 2017, 88, 673–680. [Google Scholar] [CrossRef]
- Heeschen, C.; Jang, J.J.; Weis, M.; Pathak, A.; Kaji, S.; Hu, R.S.; Tsao, P.S.; Johnson, F.L.; Cooke, J.P. Nicotine stimulates angiogenesis and promotes tumor growth and atherosclerosis. Nat. Med. 2001, 7, 833–839. [Google Scholar] [CrossRef]
- Xin, M.; Deng, X. Nicotine inactivation of the proapoptotic function of Bax through phosphorylation. J. Biol. Chem. 2005, 280, 10781–10789. [Google Scholar] [CrossRef] [Green Version]
- Fortier, A.M.; Asselin, E.; Cadrin, M. Functional specificity of Akt isoforms in cancer progression. Biomol. Concepts 2011, 2, 1–11. [Google Scholar] [CrossRef]
- Chen, R.-J.; Ho, Y.-S.; Wu, C.-H.; Wang, Y.-J. Molecular Mechanisms of Nicotine-induced Bladder Cancer. J. Exp. Clin. Med. 2011, 3, 252–256. [Google Scholar] [CrossRef]
- Chernyavsky, A.I.; Shchepotin, I.B.; Grando, S.A. Mechanisms of growth-promoting and tumor-protecting effects of epithelial nicotinic acetylcholine receptors. Int. Immunopharmacol. 2015, 29, 36–44. [Google Scholar] [CrossRef]
- Gotti, C.; Clementi, F. Neuronal nicotinic receptors: From structure to pathology. Prog. Neurobiol. 2004, 74, 363–396. [Google Scholar] [CrossRef] [PubMed]
- Egleton, R.D.; Brown, K.C.; Dasgupta, P. Nicotinic acetylcholine receptors in cancer: Multiple roles in proliferation and inhibition of apoptosis. Trends Pharmacol. Sci. 2008, 29, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Afrashteh Nour, M.; Hajiasgharzadeh, K.; Kheradmand, F.; Asadzadeh, Z.; Bolandi, N.; Baradaran, B. Nicotinic acetylcholine receptors in chemotherapeutic drugs resistance: An emerging targeting candidate. Life Sci. 2021, 278, 119557. [Google Scholar] [CrossRef] [PubMed]
- Wisniewski, D.J.; Ma, T.; Schneider, A. Nicotine induces oral dysplastic keratinocyte migration via fatty acid synthase-dependent epidermal growth factor receptor activation. Exp. Cell Res. 2018, 370, 343–352. [Google Scholar] [CrossRef]
- Hsu, C.C.; Tsai, K.Y.; Su, Y.F.; Chien, C.Y.; Chen, Y.C.; Wu, Y.C.; Liu, S.Y.; Shieh, Y.S. α7-Nicotine acetylcholine receptor mediated nicotine induced cell survival and cisplatin resistance in oral cancer. Arch. Oral Biol. 2020, 111, 104653. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.C.; Chang, Y.C. Enhancement of cancer stem-like and epithelial-mesenchymal transdifferentiation property in oral epithelial cells with long-term nicotine exposure: Reversal by targeting SNAIL. Toxicol. Appl. Pharmacol. 2013, 266, 459–469. [Google Scholar] [CrossRef] [PubMed]
- Bitzer, Z.T.; Goel, R.; Reilly, S.M.; Foulds, J.; Muscat, J.; Elias, R.J.; Richie, J.P., Jr. Effects of Solvent and Temperature on Free Radical Formation in Electronic Cigarette Aerosols. Chem. Res. Toxicol. 2018, 31, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Kaur, G.; Muthumalage, T.; Rahman, I. Mechanisms of toxicity and biomarkers of flavoring and flavor enhancing chemicals in emerging tobacco and non-tobacco products. Toxicol. Lett. 2018, 288, 143–155. [Google Scholar] [CrossRef] [PubMed]
- Bitzer, Z.T.; Goel, R.; Reilly, S.M.; Elias, R.J.; Silakov, A.; Foulds, J.; Muscat, J.; Richie, J.P., Jr. Effect of flavoring chemicals on free radical formation in electronic cigarette aerosols. Free Radic. Biol. Med. 2018, 120, 72–79. [Google Scholar] [CrossRef]
- Hua, M.; Omaiye, E.E.; Luo, W.; McWhirter, K.J.; Pankow, J.F.; Talbot, P. Identification of Cytotoxic Flavor Chemicals in Top-Selling Electronic Cigarette Refill Fluids. Sci. Rep. 2019, 9, 2782. [Google Scholar] [CrossRef] [Green Version]
- Aldakheel, F.M.; Abuderman, A.A.; Alali, B.H.; Mateen, A.; Alduraywish, S.A.; Jamil, K.; Alqahtani, M.S.; Syed, R. Smoking and P53 polymorphism association with chromosomal aberration in lung cancer. J. King Saud Univ. Sci. 2021, 33, 101533. [Google Scholar] [CrossRef]
- Ishizaki, A.; Kataoka, H. A sensitive method for the determination of tobacco-specific nitrosamines in mainstream and sidestream smokes of combustion cigarettes and heated tobacco products by online in-tube solid-phase microextraction coupled with liquid chromatography-tandem mass spectrometry. Anal. Chim. Acta 2019, 1075, 98–105. [Google Scholar] [CrossRef]
- Konstantinou, E.; Fotopoulou, F.; Drosos, A.; Dimakopoulou, N.; Zagoriti, Z.; Niarchos, A.; Makrynioti, D.; Kouretas, D.; Farsalinos, K.; Lagoumintzis, G.; et al. Tobacco-specific nitrosamines: A literature review. Food Chem. Toxicol. 2018, 118, 198–203. [Google Scholar] [CrossRef]
- Yalcin, E.; de la Monte, S. Tobacco nitrosamines as culprits in disease: Mechanisms reviewed. J. Physiol. Biochem. 2016, 72, 107–120. [Google Scholar] [CrossRef]
- Improgo, M.R.; Tapper, A.R.; Gardner, P.D. Nicotinic acetylcholine receptor-mediated mechanisms in lung cancer. Biochem. Pharmacol. 2011, 82, 1015–1021. [Google Scholar] [CrossRef]
- Xu, L.; Deng, X. Tobacco-specific nitrosamine 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanone induces phosphorylation of mu- and m-calpain in association with increased secretion, cell migration, and invasion. J. Biol. Chem. 2004, 279, 53683–53690. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.J.; Shin, H.S. Determination of tobacco-specific nitrosamines in replacement liquids of electronic cigarettes by liquid chromatography-tandem mass spectrometry. J. Chromatogr. A 2013, 1291, 48–55. [Google Scholar] [CrossRef]
- Goniewicz, M.L.; Knysak, J.; Gawron, M.; Kosmider, L.; Sobczak, A.; Kurek, J.; Prokopowicz, A.; Jablonska-Czapla, M.; Rosik-Dulewska, C.; Havel, C.; et al. Levels of selected carcinogens and toxicants in vapour from electronic cigarettes. Tob. Control 2014, 23, 133–139. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.S.; Kim, K.H.; Lee, S.S.; Brown, R.J.C.; Jo, S.H. Analytical Method for Measurement of Tobacco-Specific Nitrosamines in E-Cigarette Liquid and Aerosol. Appl. Sci. 2018, 8, 2699. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Sánchez, J.M.; Ballbè, M.; Pérez-Ortuño, R.; Fu, M.; Sureda, X.; Pascual, J.A.; Peruga, A.; Fernández, E. Secondhand exposure to aerosol from electronic cigarettes: Pilot study of assessment of tobacco-specific nitrosamine (NNAL) in urine. Gac. Sanit. 2019, 33, 575–578. [Google Scholar] [CrossRef] [PubMed]
- Hess, C.A.; Olmedo, P.; Navas-Acien, A.; Goessler, W.; Cohen, J.E.; Rule, A.M. E-cigarettes as a source of toxic and potentially carcinogenic metals. Environ. Res. 2017, 152, 221–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Na, C.J.; Jo, S.H.; Kim, K.H.; Sohn, J.R.; Son, Y.S. The transfer characteristics of heavy metals in electronic cigarette liquid. Environ. Res. 2019, 174, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Costa, M. Metals and molecular carcinogenesis. Carcinogenesis 2020, 41, 1161–1172. [Google Scholar] [CrossRef]
- Kim, H.S.; Kim, Y.J.; Seo, Y.R. An Overview of Carcinogenic Heavy Metal: Molecular Toxicity Mechanism and Prevention. J. Cancer Prev. 2015, 20, 232–240. [Google Scholar] [CrossRef]
- Geiger, J.L.; Adelstein, D.J. Chemotherapy in the definitive management of oral cancers: Where do we stand today? Oral Oncol. 2020, 102, 104584. [Google Scholar] [CrossRef]
- Dasari, S.; Tchounwou, P.B. Cisplatin in cancer therapy: Molecular mechanisms of action. Eur. J. Pharmacol. 2014, 740, 364–378. [Google Scholar] [CrossRef] [Green Version]
- Ghosh, S. Cisplatin: The first metal based anticancer drug. Bioorg. Chem. 2019, 88, 102925. [Google Scholar] [CrossRef]
- Zhu, L.; Chen, L. Progress in research on paclitaxel and tumor immunotherapy. Cell Mol. Biol. Lett. 2019, 24, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farha, N.G.; Kasi, A. Docetaxel. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2021; Available online: https://www.ncbi.nlm.nih.gov/books/NBK537242/ (accessed on 15 September 2021).
- Thirumaran, R.; Prendergast, G.C.; Gilman, P.B. Cytotoxic Chemotherapy in Clinical Treatment of Cancer. In Cancer Immunotherapy: Immune Suppression and Tumor Growth; Prendergast, G.C., Jaffee, E.M., Eds.; Academic Press: San Diego, CA, USA, 2011; pp. 101–116. [Google Scholar]
- Zhang, N.; Yin, Y.; Xu, S.J.; Chen, W.S. 5-Fluorouracil: Mechanisms of resistance and reversal strategies. Molecules 2008, 13, 1551–1569. [Google Scholar] [CrossRef] [Green Version]
- Bedoui, Y.; Guillot, X.; Sélambarom, J.; Guiraud, P.; Giry, C.; Jaffar-Bandjee, M.C.; Ralandison, S.; Gasque, P. Methotrexate an Old Drug with New Tricks. Int. J. Mol. Sci. 2019, 20, 5023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petros, W.P.; Younis, I.R.; Ford, J.N.; Weed, S.A. Effects of tobacco smoking and nicotine on cancer treatment. Pharmacotherapy 2012, 32, 920–931. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; Huang, H.; Pan, C.; Zhang, B.; Liu, X.; Zhang, L. Nicotine inhibits apoptosis induced by cisplatin in human oral cancer cells. Int. J. Oral Maxillofac. Surg. 2007, 36, 739–744. [Google Scholar] [CrossRef] [PubMed]
- Cucina, A.; Dinicola, S.; Coluccia, P.; Proietti, S.; D’Anselmi, F.; Pasqualato, A.; Bizzarri, M. Nicotine stimulates proliferation and inhibits apoptosis in colon cancer cell lines through activation of survival pathways. J. Surg. Res. 2012, 178, 233–241. [Google Scholar] [CrossRef]
- Mohan, S.P.; Bhaskaran, M.K.; George, A.L.; Thirutheri, A.; Somasundaran, M.; Pavithran, A. Immunotherapy in Oral Cancer. J. Pharm. Bioallied Sci. 2019, 11 (Suppl. 2), S107–S111. [Google Scholar] [CrossRef] [PubMed]
- Piao, W.H.; Campagnolo, D.; Dayao, C.; Lukas, R.J.; Wu, J.; Shi, F.D. Nicotine and inflammatory neurological disorders. Acta Pharmacol. Sin. 2009, 30, 715–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalra, R.; Singh, S.P.; Pena-Philippides, J.C.; Langley, R.J.; Razani-Boroujerdi, S.; Sopori, M.L. Immunosuppressive and anti-inflammatory effects of nicotine administered by patch in an animal model. Clin. Diagn. Lab. Immunol. 2004, 11, 563–568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mo, J.; Hu, X.; Gu, L.; Chen, B.; Khadaroo, P.A.; Shen, Z.; Dong, L.; Lv, Y.; Chitumba, M.N.; Liu, J. Smokers or non-smokers: Who benefits more from immune checkpoint inhibitors in treatment of malignancies? An up-to-date meta-analysis. World J. Surg. Oncol. 2020, 18, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norum, J.; Nieder, C. Tobacco smoking and cessation and PD-L1 inhibitors in non-small cell lung cancer (NSCLC): A review of the literature. ESMO Open 2018, 3, e000406. [Google Scholar] [CrossRef] [Green Version]
- Zaleskis, G.; Pasukoniene, V.; Characiejus, D.; Urbonas, V. Do the benefits of being a smoker hint at the existence of PD-1/PD-L1 sensitizers for patients on single-agent immunotherapy? J. Immunother. Cancer 2021, 9, e003191. [Google Scholar] [CrossRef]
- Dai, L.; Jin, B.; Liu, T.; Chen, J.; Li, G.; Dang, J. The effect of smoking status on efficacy of immune checkpoint inhibitors in metastatic non-small cell lung cancer: A systematic review and meta-analysis. EClinicalMedicine 2021, 38, 100990. [Google Scholar] [CrossRef]
- Zanetti, F.; Titz, B.; Sewer, A.; Lo Sasso, G.; Scotti, E.; Schlage, W.K.; Mathis, C.; Leroy, P.; Majeed, S.; Torres, L.O.; et al. Comparative systems toxicology analysis of cigarette smoke and aerosol from a candidate modified risk tobacco product in organotypic human gingival epithelial cultures: A 3-day repeated exposure study. Food Chem. Toxicol. 2017, 101, 15–35. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Flavors | Chemical Compounds Found in Flavoring Agents | Toxic Potential |
|---|---|---|
| Mint | Menthol | Cytotoxic, oxidative, inflammatory, loss of epithelial barrier function |
| Buttery | Diacetyl | Oxidative, inflammatory, lung toxicity |
| Chocolate | Pyrazine derivatives | Cytotoxic |
| Cherry | Benzaldehyde derivatives | Oxidative, irritant, protein carbonylation of extracellular matrix, DNA damage |
| Cinnamon | Cinnamaldehyde | Cytotoxic, oxidative, loss of epithelial barrier function |
| Vanilla | Vanillin | Oxidative, cytotoxic, inflammatory, irritant |
| Caramel | Maltol | Oxidative, inflammatory, loss of epithelial barrier function |
| Compound | Mean Concentration (μg/L) ± SD |
|---|---|
| NNN | 4.06 ± 9.34 |
| NNK | 1.71 ± 1.69 |
| NAT | 6.36 ± 12.52 |
| NAB | 0.90 ± 1.72 |
| Total TSNAs | 12.99 ± 18.23 |
| Active Compound | Mechanism of Action | Reference |
|---|---|---|
| Cisplatin | Induces apoptosis in cancer cells by crosslinking with the purine bases on the DNA, causing DNA damage | [83,84] |
| Carboplatin | Similar mechanism with cisplatin, but with lower reactivity and slower DNA binding kinetics | [83] |
| Paclitaxel | Binds to β-subunit of the tubulin protein of the microtubules, promotes the assembly of tubulin into microtubules and prevents the dissociation of microtubules, blocking cell cycle progression, preventing mitosis, and inhibiting cancer cells growth | [85] |
| Docetaxel | Similar mechanism to paclitaxel–binds to β-tubulin, and it inhibits the proper assembly of microtubules into the mitotic spindle, arresting the cell cycling during G2/M | [86] |
| 5-flurouracil | Pyrimidine antagonist-antimetabolite with a similar structure to naturally occurring compounds that are required for the viability and division of a cell; it inhibits the replication or the repair of DNA | [87,88] |
| Hydroxyurea | Inhibits ribonucleotide reductase and blocks the formation of nucleotides needed for DNA synthesis and repair | [87] |
| Methotrexate | Folate antagonist; it inhibits dihydrofolate reductase, affecting the de novo synthesis of purines used in DNA replication | [87,89] |
| Capecitabine | Similar mechanism with 5-fluorouracil | [87] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jităreanu, A.; Agoroaei, L.; Aungurencei, O.D.; Goriuc, A.; Diaconu Popa, D.; Savin, C.; Caba, I.-C.; Tătărușanu, S.; Profire, B.; Mârțu, I. Electronic Cigarettes’ Toxicity: From Periodontal Disease to Oral Cancer. Appl. Sci. 2021, 11, 9742. https://doi.org/10.3390/app11209742
Jităreanu A, Agoroaei L, Aungurencei OD, Goriuc A, Diaconu Popa D, Savin C, Caba I-C, Tătărușanu S, Profire B, Mârțu I. Electronic Cigarettes’ Toxicity: From Periodontal Disease to Oral Cancer. Applied Sciences. 2021; 11(20):9742. https://doi.org/10.3390/app11209742
Chicago/Turabian StyleJităreanu, Alexandra, Luminița Agoroaei, Ovidiu Dumitru Aungurencei, Ancuța Goriuc, Diana Diaconu Popa, Carmen Savin, Ioana-Cezara Caba, Simona Tătărușanu, Bianca Profire, and Ioana Mârțu. 2021. "Electronic Cigarettes’ Toxicity: From Periodontal Disease to Oral Cancer" Applied Sciences 11, no. 20: 9742. https://doi.org/10.3390/app11209742
APA StyleJităreanu, A., Agoroaei, L., Aungurencei, O. D., Goriuc, A., Diaconu Popa, D., Savin, C., Caba, I. -C., Tătărușanu, S., Profire, B., & Mârțu, I. (2021). Electronic Cigarettes’ Toxicity: From Periodontal Disease to Oral Cancer. Applied Sciences, 11(20), 9742. https://doi.org/10.3390/app11209742