
Reliability of a New Portable Dynamometer for Assessing Hip and Lower Limb Strength



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Protocol
2.3. Data Analysis
2.4. Statistical Analysis
3. Results
3.1. Intra-Session Reliability
3.2. Inter-Session Reliability
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Suchomel, T.J.; Nimphius, S.; Stone, M.H. The Importance of Muscular Strength in Athletic Performance. Sport. Med. 2016, 46, 1419–1449. [Google Scholar] [CrossRef]
- Timmins, R.G.; Bourne, M.N.; Shield, A.J.; Williams, M.D.; Lorenzen, C.; Opar, D.A. Short biceps femoris fascicles and eccentric knee flexor weakness increase the risk of hamstring injury in elite football (soccer): A prospective cohort study. Br. J. Sports Med. 2016, 50, 1524–1535. [Google Scholar] [CrossRef]
- Ryan, J.; Deburca, N.; Creesh, K.M. Risk factors for groin / hip injuries in field-based sports: A systematic review. Br. J. Sports Med. 2014, 48, 1–8. [Google Scholar] [CrossRef]
- Mosler, A.B.; Agricola, R.; Weir, A.; Hölmich, P.; Crossley, K.M. Which factors differentiate athletes with hip / groin pain from those without? A systematic review with. Br. J. Sports Med. 2015, 49, 810. [Google Scholar] [CrossRef]
- Opar, D.A.; Williams, M.D.; Shield, A.J. Hamstring strain injuries: Factors that Lead to injury and re-Injury. Sport. Med. 2012, 42, 209–226. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, T.; Tanaka, M.; Shida, M. Intrinsic Risk Factors of Lateral Ankle Sprain: A Systematic Review and Meta-analysis. Sports Health 2016, 8, 190–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopez, P.; Pinto, R.S.; Radaelli, R.; Rech, A.; Grazioli, R.; Izquierdo, M.; Cadore, E.L. Benefits of resistance training in physically frail elderly: A systematic review. Aging Clin. Exp. Res. 2018, 30, 889–899. [Google Scholar] [CrossRef] [PubMed]
- Cuthbert, S.C.; Goodheart, G.J. On the reliability and validity of manual muscle testing: A literature review. Chiropr. Osteopat. 2007, 15, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stark, T.; Walker, B.; Phillips, J.K.; Fejer, R.; Beck, R. Hand-held dynamometry correlation with the gold standard isokinetic dynamometry: A systematic review. PM R 2011, 3, 472–479. [Google Scholar] [CrossRef]
- Thorborg, K.; Bandholm, T.; Schick, M.; Jensen, J.; Hölmich, P. Hip strength assessment using handheld dynamometry is subject to intertester bias when testers are of different sex and strength. Scand. J. Med. Sci. Sport. 2013, 23, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Thorborg, K.; Bandholm, T.; Hölmich, P. Hip- and knee-strength assessments using a hand-held dynamometer with external belt-fixation are inter-tester reliable. Knee Surg. Sport. Traumatol. Arthrosc. 2013, 21, 550–555. [Google Scholar] [CrossRef] [PubMed]
- Krause, D.A.; Schlagel, S.J.; Stember, B.M.; Zoetewey, J.E.; Hollman, J.H. Influence of Lever Arm and Stabilization on Measures of Hip Abduction and Adduction Torque Obtained by Hand-Held Dynamometry. Arch. Phys. Med. Rehabil. 2007, 88, 37–42. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, M.; Bourne, M.; Heerey, J.; Timmins, R.G.; Pizzari, T. A novel device to assess hip strength: Concurrent validity and normative values in male athletes. Phys. Ther. Sport 2019, 35, 63–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryan, S.; Kempton, T.; Pacecca, E.; Coutts, A.J. Measurement Properties of an Adductor Strength Assessment System in Professional Australian Footballers. Int. J. Sports Physiol. Perform. 2018, 14, 256–259. [Google Scholar] [CrossRef] [PubMed]
- Desmyttere, G.; Gaudet, S.; Begon, M. Test-retest reliability of a hip strength assessment system in varsity soccer players. Phys. Ther. Sport 2019, 37, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Markovic, G.; Šarabon, N.; Pausic, J.; Hadžić, V. Adductor muscles strength and strength asymmetry as risk factors for groin injuries among professional soccer players: A prospective study. Int. J. Environ. Res. Public Health 2020, 17, 4946. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: London, UK, 1988. [Google Scholar]
- Tourville, T.W.; Smith, H.C.; Shultz, S.J.; Vacek, P.M.; Slauterbeck, J.R.; Johnson, R.J.; Beynnon, B.D. Reliability of a New Stabilized Dynamometer System for the Evaluation of Hip Strength. Sports Health 2013, 5, 129–136. [Google Scholar] [CrossRef] [Green Version]
- Opar, D.A.; Piatkowski, T.; Williams, M.D.; Shield, A.J. A novel device using the nordic hamstring exercise to assess eccentric knee flexor strength: A reliability and retrospective injury study. J. Orthop. Sports Phys. Ther. 2013, 43, 636–640. [Google Scholar] [CrossRef] [Green Version]
- Lodge, C.; Tobin, D.; O’Rourke, B.; Thorborg, K. Reliability and Validity of a New Eccentric Hamstring Strength Measurement Device. Arch. Rehabil. Res. Clin. Transl. 2020, 2, 100034. [Google Scholar] [CrossRef] [PubMed]
- Green, B.; Bourne, M.N.; Pizzari, T. Isokinetic strength assessment offers limited predictive validity for detecting risk of future hamstring strain in sport: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 329–336. [Google Scholar] [CrossRef] [PubMed]
- van Dyk, N.; Witvrouw, E.; Bahr, R. Interseason variability in isokinetic strength and poor correlation with Nordic hamstring eccentric strength in football players. Scand. J. Med. Sci. Sport. 2018, 28, 1878–1887. [Google Scholar] [CrossRef] [Green Version]
- Van Dyk, N.; Behan, F.P.; Whiteley, R. Including the Nordic hamstring exercise in injury prevention programmes halves the rate of hamstring injuries: A systematic review and meta-analysis of 8459 athletes. Br. J. Sports Med. 2019, 53, 1362–1370. [Google Scholar] [CrossRef] [Green Version]
- Bourne, M.N.; Opar, D.A.; Williams, M.D.; Shield, A.J. Eccentric knee flexor strength and risk of hamstring injuries in rugby union. Am. J. Sports Med. 2015, 43, 2663–2670. [Google Scholar] [CrossRef]
- Thorborg, K.; Petersen, J.; Magnusson, S.P.; Hölmich, P. Clinical assessment of hip strength using a hand-held dynamometer is reliable. Scand. J. Med. Sci. Sport. 2010, 20, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Charlton, P.C.; Mentiplay, B.F.; Grimaldi, A.; Pua, Y.H.; Clark, R.A. The reliability of a maximal isometric hip strength and simultaneous surface EMG screening protocol in elite, junior rugby league athletes. J. Sci. Med. Sport 2017, 20, 139–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, D.A.; Bond, E.Q.; Sisto, S.A.; Nadler, S.F. The intra- and interrater reliability of hip muscle strength assessments using a handheld versus a portable dynamometer anchoring station. Arch. Phys. Med. Rehabil. 2004, 85, 598–603. [Google Scholar] [CrossRef]
- Van Melick, N.; Van Cingel, R.E.H.; Brooijmans, F.; Neeter, C.; Van Tienen, T.; Hullegie, W.; Nijhuis-Van Der Sanden, M.W.G. Evidence-based clinical practice update: Practice guidelines for anterior cruciate ligament rehabilitation based on a systematic review and multidisciplinary consensus. Br. J. Sports Med. 2016, 50, 1506–1515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flagg, K.Y.; Karavatas, S.G.; Thompson Jr, S.; Bennett, C. Current criteria for return to play after anterior cruciate ligament reconstruction: An evidence-based literature review. Ann. Transl. Med. 2019, 7, S252. [Google Scholar] [CrossRef]
- O’Neill, S.; Barry, S.; Watson, P. Plantarflexor strength and endurance deficits associated with mid-portion Achilles tendinopathy: The role of soleus. Phys. Ther. Sport 2019, 37, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Delahunt, E.; Kennelly, C.; McEntee, B.L.; Coughlan, G.F.; Green, B.S. The thigh adductor squeeze test: 45° of hip flexion as the optimal test position for eliciting adductor muscle activity and maximum pressure values. Man. Ther. 2011, 16, 476–480. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Task | Body Position | Sensor & Lower Leg Contact |
|---|---|---|
| HIP FLX HIP ADD HIP ABD | seated position; hip in ~45° flexion and neutral in other planes (0° abduction/adduction; 0° external/internal rotation); knee locked in full extension; ankle in slight dorsiflexion and neutral in other planes; hands placed on the floor behind the device for support; non-elastic strap placed across the pelvis on the anterior side for stabilization | anterior (for FLX), medial (for ADD), or lateral (for ABD) side of the lower leg in contact with superior (for FLX), medial (for ADD), or lateral (for ABD) part of sensor brace; 5 cm proximal to the medial malleoli |
| HIP EXT | prone position; hip in neutral position in all planes (0° flexion/extension; 0° abduction/adduction; 0° external/internal rotation); knee locked in full extension and placed slightly above the surface (to further emphasize hip extension movement and to avoid any knee flexion during contraction); ankle in slight dorsiflexion and neutral in other planes; elbows placed on the padded mat on the floor behind the device for support; non-elastic strap placed across the pelvis on the posterior side for stabilization | posterior side of the lower leg in contact with superior part of sensor brace; 5 cm proximal to the medial malleoli |
| HIP IR HIP ER | 4-point support on the dynamometer (on hands and knees); hip in 90° flexion and neutral in other planes (0° abduction/adduction; 0° external/internal rotation); knee in 90° flexion and neutral in transversal plane (0° internal/external rotation); ankle in slight dorsiflexion and neutral in other planes, no stabilization strap was used | lateral (for IR) or medial (for ER) side of the lower leg in contact with lateral (for IR) or medial (for ER) part of sensor brace; 5 cm proximal to the medial malleoli |
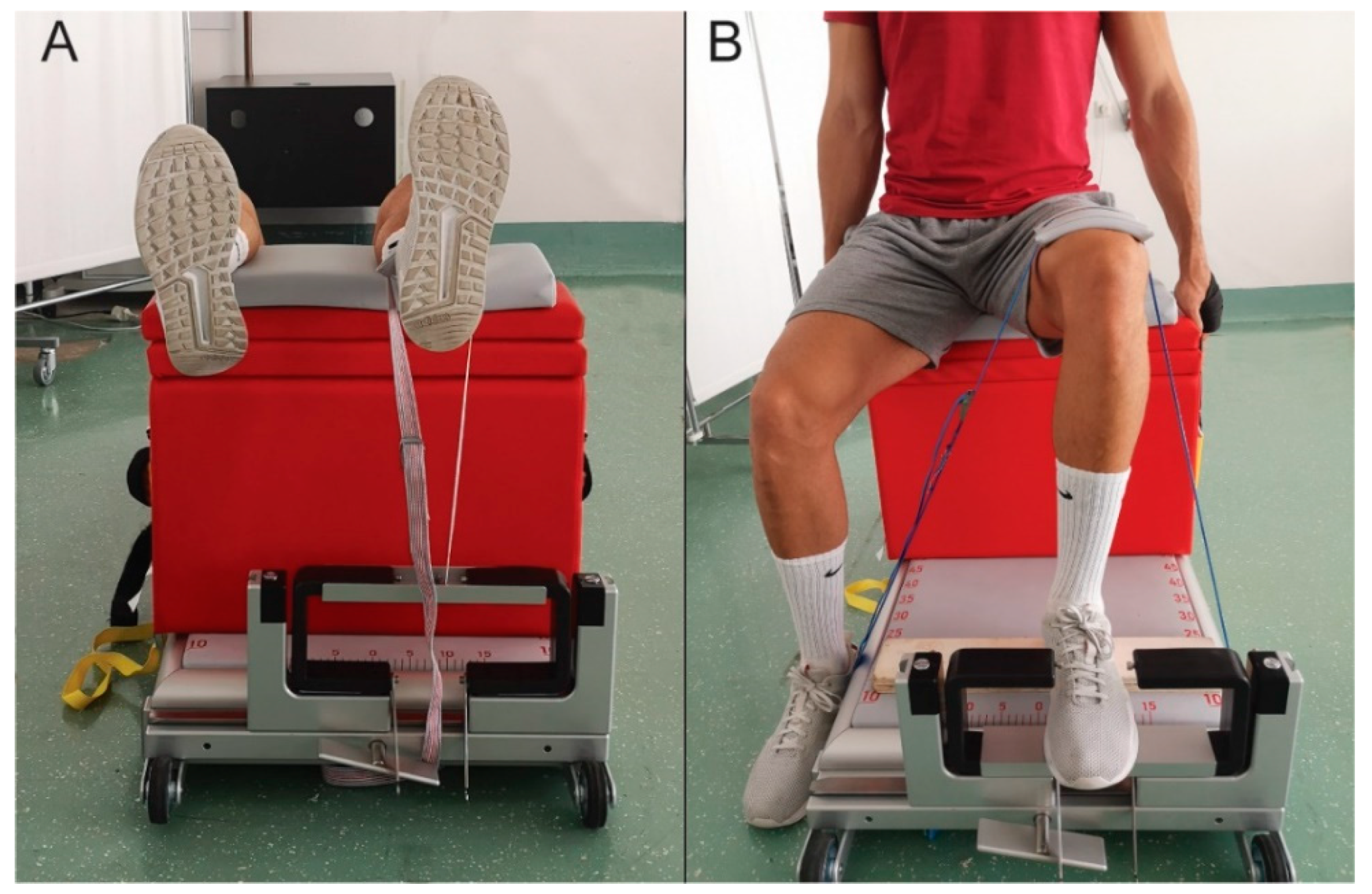
| KNEE EXT | supine position, hip in 90° flexion and neutral in other planes (0° abduction/adduction; 0° external/internal rotation); knee in 90° flexion and neutral in transverse plane (0° internal/external rotation); ankle in slight dorsiflexion and neutral in other planes; posterior side of lower leg was placed on the box, which was fixated on the dynamometer with non-elastic strap (yellow strap, shown in Figure 2D); posterior side of thigh in contact with the box; for stabilization, participant held the straps attached to the box (black strap, shown in Figure 2D) | the measurement was performed using non-elastic strap that connected participant’s lower leg on the anterior side (5 cm proximal to medial malleoli) with a rigid rod mounted on both sensor braces on the superior part (shown in Figure 3A) |
| ANKLE PFLX | seated position, hip in 90° flexion and neutral in other planes (0° abduction/adduction; 0° external/internal rotation); knee in 90° flexion and neutral in transverse plane (0° internal/external rotation); ankle in neutral position in all planes (0° plantar/dorsal flexion, 0° inversion/eversion); non-elastic strap that enabled isometric plantar flexion was placed across the thigh proximal to the knee; for stabilization, the participant held the straps attached to the box (black strap, shown in Figure 2E) | the measurement was performed using a rigid rod that was mounted on both sensor braces on the inferior part; metatarso-phalangeal joints were placed on the middle of the rigid rod (shown in Figure 3B) |
| NHE | kneeling position; lower leg placed on the padded mat distally to the patella (to allow free movement of the patella during the descend); participant slowly descended in 3–5 s (eccentric contraction of knee flexors) while maintaining straight knee-hip-shoulder line | posterior side of the lower leg in contact with superior part of sensor brace; 5 cm proximal to the medial malleoli |
| Task | Parameter | S1 Mean (SD) | S1 95% CI | S2 Mean (SD) | S2 95% CI | %CV | ICC2.k | Bias | ||
|---|---|---|---|---|---|---|---|---|---|---|
| F | sig | d | ||||||||
| HIP ADD | R AVG | 0.77 (0.2) | 0.69–0.85 | 0.76 (0.23) | 0.67–0.85 | 6.0 | 0.90 | 0.37 | 0.55 | 0.05 |
| L AVG | 0.77 (0.21) | 0.69–0.85 | 0.75 (0.21) | 0.66–0.84 | 5.4 | 0.92 | 0.25 | 0.62 | 0.10 | |
| B AVG | 2.09 (0.5) | 1.89–2.29 | 2.02 (0.49) | 1.82–2.22 | 3.6 | 0.94 | 0.59 | 0.45 | 0.14 | |
| R MAX | 0.83 (0.2) | 0.75–0.91 | 0.82 (0.25) | 0.72–0.92 | 6.0 | 0.90 | 0.04 | 0.85 | 0.04 | |
| L MAX | 0.84 (0.25) | 0.74–0.94 | 0.8 (0.22) | 0.71–0.89 | 7.0 | 0.90 | 1.59 | 0.22 | 0.17 | |
| B MAX | 2.17 (0.51) | 1.97–2.37 | 2.11 (0.5) | 1.91–2.31 | 3.5 | 0.94 | 0.41 | 0.53 | 0.12 | |
| HIP ABD | R AVG | 0.74 (0.14) | 0.68–0.8 | 0.7 (0.16) | 0.64–0.76 | 7.1 | 0.84 | 2.08 | 0.16 | 0.27 |
| L AVG | 0.69 (0.12) | 0.64–0.74 | 0.68 (0.14) | 0.62–0.74 | 7.8 | 0.77 | 0.12 | 0.73 | 0.08 | |
| B AVG | 2.04 (0.38) | 1.89–2.19 | 1.99 (0.39) | 1.83–2.15 | 7.8 | 0.87 | 0.12 | 0.73 | 0.13 | |
| R MAX | 0.78 (0.15) | 0.72–0.84 | 0.74 (0.18) | 0.67–0.81 | 6.00 | 0.81 | 0.93 | 0.35 | 0.24 | |
| L MAX | 0.74 (0.13) | 0.69–0.79 | 0.73 (0.15) | 0.67–0.79 | 8.5 | 0.76 | 1.47 | 0.24 | 0.07 | |
| B MAX | 2.12 (0.4) | 1.96–2.28 | 2.05 (0.4) | 1.89–2.21 | 8.6 | 0.86 | 0.10 | 0.76 | 0.18 | |
| HIP IR | R AVG | 0.7 (0.15) | 0.64–0.76 | 0.73 (0.17) | 0.66–0.8 | 17.4 | 0.61 | 1.00 | 0.33 | 0.19 |
| L AVG | 0.67 (0.19) | 0.59–0.75 | 0.74 (0.17) | 0.67–0.81 | 9.3 | 0.82 | 8.53 | 0.01 | 0.39 | |
| B AVG | 2.2 (0.53) | 1.99–2.41 | 2.15 (0.49) | 1.95–2.35 | 6.6 | 0.86 | 0.44 | 0.52 | 0.10 | |
| R MAX | 0.75 (0.17) | 0.68–0.82 | 0.78 (0.17) | 0.71–0.85 | 18.7 | 0.54 | 0.84 | 0.37 | 0.18 | |
| L MAX | 0.74 (0.19) | 0.66–0.82 | 0.8 (0.19) | 0.72–0.88 | 9.4 | 0.79 | 3.77 | 0.06 | 0.32 | |
| B MAX | 2.32 (0.51) | 2.12–2.52 | 2.25 (0.5) | 2.05–2.45 | 5.0 | 0.88 | 1.04 | 0.32 | 0.14 | |
| HIP ER | R AVG | 0.76 (0.16) | 0.69–0.83 | 0.73 (0.14) | 0.67–0.79 | 9.9 | 0.67 | 1.01 | 0.33 | 0.20 |
| L AVG | 0.74 (0.18) | 0.67–0.81 | 0.7 (0.13) | 0.65–0.75 | 6.2 | 0.86 | 2.66 | 0.12 | 0.25 | |
| B AVG | 1.81 (0.32) | 1.68–1.94 | 1.74 (0.34) | 1.6–1.88 | 2.1 | 0.95 | 5.31 | 0.03 | 0.21 | |
| R MAX | 0.83 (0.19) | 0.75–0.91 | 0.79 (0.17) | 0.72–0.86 | 11.1 | 0.67 | 1.46 | 0.24 | 0.22 | |
| L MAX | 0.8 (0.21) | 0.72–0.88 | 0.76 (0.14) | 0.7–0.82 | 8.4 | 0.81 | 1.87 | 0.18 | 0.22 | |
| B MAX | 1.88 (0.34) | 1.74–2.02 | 1.82 (0.34) | 1.68–1.96 | 2.2 | 0.94 | 5.50 | 0.03 | 0.18 | |
| HIP EXT | R AVG | 2.71 (0.48) | 2.51–2.91 | 2.65 (0.5) | 2.45–2.85 | 6.4 | 0.69 | 0.03 | 0.88 | 0.12 |
| L AVG | 2.63 (0.55) | 2.4–2.86 | 2.55 (0.49) | 2.35–2.75 | 5.9 | 0.75 | 0.28 | 0.60 | 0.15 | |
| R MAX | 2.87 (0.4) | 2.7–3.04 | 2.83 (0.56) | 2.61–3.05 | 6.4 | 0.71 | 0.06 | 0.82 | 0.08 | |
| L MAX | 2.77 (0.53) | 2.55–2.99 | 2.69 (0.48) | 2.5–2.88 | 3.9 | 0.81 | 0.34 | 0.57 | 0.16 | |
| HIP FLX | R AVG | 1.94 (0.41) | 1.78–2.1 | 2.04 (0.45) | 1.86–2.22 | 7.5 | 0.69 | 2.01 | 0.17 | 0.23 |
| L AVG | 1.89 (0.35) | 1.75–2.03 | 2.04 (0.45) | 1.86–2.22 | 8.2 | 0.60 | 4.43 | 0.05 | 0.37 | |
| R MAX | 2.03 (0.42) | 1.86–2.2 | 2.14 (0.46) | 1.96–2.32 | 7.3 | 0.68 | 2.19 | 0.15 | 0.25 | |
| L MAX | 1.97 (0.36) | 1.83–2.11 | 2.16 (0.46) | 1.98–2.34 | 8.0 | 0.63 | 7.56 | 0.01 | 0.46 | |
| KNEE EXT | R AVG | 6.59 (1.81) | 5.87–7.31 | 6.06 (1.69) | 5.38–6.74 | 10.0 | 0.67 | 3.65 | 0.07 | 0.30 |
| L AVG | 6.24 (1.72) | 5.55–6.93 | 6.25 (1.91) | 5.49–7.01 | 6.4 | 0.83 | 0.00 | 0.97 | 0.01 | |
| R MAX | 6.91 (1.92) | 6.14–7.68 | 6.47 (1.77) | 5.76–7.18 | 9.7 | 0.70 | 2.40 | 0.14 | 0.24 | |
| L MAX | 6.59 (1.79) | 5.87–7.31 | 6.58 (1.97) | 5.79–7.37 | 5.6 | 0.84 | 0.00 | 0.98 | 0.01 | |
| ANKLE PFLX | R AVG | 4.86 (0.6) | 4.61–5.11 | 4.83 (0.62) | 4.57–5.1 | 6.7 | 0.54 | 0.04 | 0.85 | 0.04 |
| L AVG | 4.61 (0.5) | 4.4–4.82 | 4.75 (0.85) | 4.39–5.11 | 6.3 | 0.43 | 0.66 | 0.43 | 0.20 | |
| R MAX | 5.19 (0.59) | 4.94–5.44 | 5.18 (0.75) | 4.86–5.49 | 5.8 | 0.68 | 0.01 | 0.91 | 0.02 | |
| L MAX | 4.85 (0.54) | 4.62–5.08 | 4.94 (0.91) | 4.55–5.32 | 6.4 | 0.44 | 0.24 | 0.63 | 0.12 | |
| NHE | R AVG | 1.97 (0.44) | 1.79–2.15 | 1.98 (0.38) | 1.83–2.13 | 2.5 | 0.91 | 0.17 | 0.68 | 0.02 |
| L AVG | 1.92 (0.42) | 1.75–2.09 | 1.94 (0.39) | 1.78–2.1 | 3.0 | 0.90 | 0.45 | 0.51 | 0.05 | |
| B AVG | 3.88 (0.84) | 3.54–4.22 | 3.92 (0.76) | 3.62–4.22 | 2.6 | 0.91 | 0.34 | 0.56 | 0.05 | |
| R MAX | 2.06 (0.45) | 1.88–2.24 | 2.07 (0.36) | 1.93–2.21 | 3.0 | 0.90 | 0.14 | 0.72 | 0.02 | |
| L MAX | 1.98 (0.43) | 1.81–2.15 | 2.03 (0.36) | 1.89–2.17 | 4.7 | 0.83 | 1.04 | 0.32 | 0.13 | |
| B MAX | 4.03 (0.84) | 3.69–4.37 | 4.09 (0.7) | 3.81–4.37 | 3.6 | 0.87 | 0.71 | 0.41 | 0.08 | |
| Parameter | S1 Mean (SD) | S1 95% CI | S2 Mean (SD) | S2 95% CI | % CV | ICC2.k | Bias | ||
|---|---|---|---|---|---|---|---|---|---|
| F | sig | d | |||||||
| ADD:ABD UNI R | 105.74 (24.58) | 95.91–115.57 | 110.29 (30) | 98.03–122.55 | 19.3 | 0.55 | 0.17 | 0.68 | 0.17 |
| ADD:ABD UNI L | 112.13 (24.5) | 102.33–121.93 | 114.39 (27.85) | 103.01–125.77 | 12.6 | 0.65 | 0.06 | 0.81 | 0.09 |
| ADD:ABD BI R | 102.03 (17.51) | 93.32–110.4 | 101.83 (15.74) | 94.09–108.94 | 9.4 | 0.71 | 0.00 | 0.95 | 0.01 |
| ADD:ABD BI L | 103.19 (19.66) | 92.89–111.99 | 102.63 (15.86) | 94.77–109.79 | 11.9 | 0.66 | 0.01 | 0.94 | 0.03 |
| IR:ER UNI R | 97.08 (24.47) | 86.85–107.31 | 102.4 (25.74) | 92.1–112.7 | 22.5 | 0.39 | 1.08 | 0.31 | 0.21 |
| IR:ER UNI L | 95.14 (28.38) | 83.79–106.49 | 108.36 (25.86) | 98.01–118.71 | 11.3 | 0.78 | 9.95 | 0.00 | 0.49 |
| IR:ER BI R | 125.85 (32.20) | 109.87–138.97 | 128.15 (27.68) | 114.67–141.09 | 9.9 | 0.76 | 0.18 | 0.68 | 0.08 |
| IR:ER BI L | 122.04 (26.94) | 109.79–133.06 | 123.44 (26.37) | 111.78–135.91 | 8.1 | 0.83 | 0.11 | 0.74 | 0.05 |
| FLX:EXT UNI R | 74.8 (15.67) | 68.25–81.35 | 78.53 (17.71) | 71.44–85.62 | 7.5 | 0.8 | 0.95 | 0.34 | 0.22 |
| FLX:EXT UNI L | 74.89 (14.43) | 68.86–80.92 | 81.1 (16.17) | 74.63–87.57 | 8.1 | 0.75 | 4.68 | 0.04 | 0.40 |
| Task | Parameter | S1 Mean (SD) | S1 95% CI | S3 Mean (SD) | S3 95% CI | % CV | ICC2.k | Bias | ||
|---|---|---|---|---|---|---|---|---|---|---|
| F | sig | d | ||||||||
| HIP ADD | R AVG | 0.77 (0.2) | 0.69–0.85 | 0.77 (0.18) | 0.7–0.84 | 8.8 | 0.8 | 0 | 0.96 | 0.00 |
| L AVG | 0.77 (0.21) | 0.69–0.85 | 0.8 (0.21) | 0.72–0.88 | 14.7 | 0.7 | 0.72 | 0.41 | 0.14 | |
| B AVG | 2.09 (0.5) | 1.89–2.29 | 2.09 (0.47) | 1.9–2.28 | 2.3 | 0.96 | 0.01 | 0.94 | 0.00 | |
| R MAX | 0.83 (0.2) | 0.75–0.91 | 0.85 (0.18) | 0.78–0.92 | 9.1 | 0.78 | 0.29 | 0.59 | 0.11 | |
| L MAX | 0.84 (0.25) | 0.74–0.94 | 0.87 (0.21) | 0.79–0.95 | 14.8 | 0.74 | 0.5 | 0.49 | 0.13 | |
| B MAX | 2.17 (0.51) | 1.97–2.37 | 2.18 (0.46) | 2–2.36 | 1.9 | 0.97 | 0.02 | 0.88 | 0.02 | |
| HIP ABD | R AVG | 0.74 (0.14) | 0.68–0.8 | 0.74 (0.15) | 0.68–0.8 | 13.6 | 0.66 | 0 | 0.97 | 0.00 |
| L AVG | 0.69 (0.12) | 0.64–0.74 | 0.73 (0.15) | 0.67–0.79 | 10.1 | 0.68 | 2.2 | 0.15 | 0.29 | |
| B AVG | 2.04 (0.38) | 1.89–2.19 | 2.03 (0.4) | 1.87–2.19 | 2.7 | 0.94 | 0.06 | 0.81 | 0.03 | |
| R MAX | 0.78 (0.15) | 0.72–0.84 | 0.78 (0.15) | 0.72–0.84 | 13.8 | 0.61 | 0.05 | 0.83 | 0.00 | |
| L MAX | 0.74 (0.13) | 0.69–0.79 | 0.78 (0.16) | 0.72–0.84 | 9.4 | 0.73 | 2.08 | 0.16 | 0.27 | |
| B MAX | 2.12 (0.4) | 1.96–2.28 | 2.1 (0.41) | 1.94–2.26 | 2.7 | 0.94 | 0.27 | 0.61 | 0.05 | |
| HIP IR | R AVG | 0.7 (0.15) | 0.64–0.76 | 0.75 (0.18) | 0.68–0.82 | 8.6 | 0.82 | 1.92 | 0.18 | 0.30 |
| L AVG | 0.67 (0.19) | 0.59–0.75 | 0.74 (0.2) | 0.66–0.82 | 17.2 | 0.66 | 3.64 | 0.07 | 0.36 | |
| B AVG | 2.2 (0.53) | 1.99–2.41 | 2.1 (0.49) | 1.9–2.3 | 6.7 | 0.86 | 2.25 | 0.15 | 0.20 | |
| R MAX | 0.75 (0.17) | 0.68–0.82 | 0.81 (0.19) | 0.73–0.89 | 10.0 | 0.79 | 2.38 | 0.14 | 0.33 | |
| L MAX | 0.74 (0.19) | 0.66–0.82 | 0.81 (0.22) | 0.72–0.9 | 12.8 | 0.71 | 2.81 | 0.11 | 0.34 | |
| B MAX | 2.32 (0.51) | 2.12–2.52 | 2.19 (0.48) | 2–2.38 | 5.5 | 0.87 | 3.88 | 0.06 | 0.26 | |
| HIP ER | R AVG | 0.76 (0.16) | 0.69–0.83 | 0.78 (0.16) | 0.72–0.84 | 12.0 | 0.63 | 0.2 | 0.66 | 0.13 |
| L AVG | 0.74 (0.18) | 0.67–0.81 | 0.83 (0.19) | 0.75–0.91 | 13.0 | 0.68 | 7.56 | 0.01 | 0.49 | |
| B AVG | 1.81 (0.32) | 1.68–1.94 | 1.8 (0.35) | 1.66–1.94 | 2.4 | 0.94 | 0.07 | 0.8 | 0.03 | |
| R MAX | 0.83 (0.19) | 0.75–0.91 | 0.83 (0.18) | 0.76–0.9 | 10.0 | 0.72 | 0.06 | 0.81 | 0.00 | |
| L MAX | 0.8 (0.21) | 0.72–0.88 | 0.91 (0.23) | 0.82–1 | 12.6 | 0.76 | 8.44 | 0.01 | 0.50 | |
| B MAX | 1.88 (0.34) | 1.74–2.02 | 1.87 (0.36) | 1.73–2.01 | 2.2 | 0.95 | 0.27 | 0.61 | 0.03 | |
| HIP EXT | R AVG | 2.71 (0.48) | 2.51–2.91 | 2.63 (0.49) | 2.43–2.83 | 8.5 | 0.78 | 0.12 | 0.73 | 0.16 |
| L AVG | 2.63 (0.55) | 2.4–2.86 | 2.5 (0.52) | 2.29–2.71 | 4.5 | 0.86 | 1.07 | 0.31 | 0.24 | |
| R MAX | 2.87 (0.4) | 2.7–3.04 | 2.81 (0.51) | 2.61–3.01 | 6.7 | 0.77 | 0.05 | 0.83 | 0.13 | |
| L MAX | 2.77 (0.53) | 2.55–2.99 | 2.7 (0.53) | 2.49–2.91 | 5.2 | 0.85 | 0.09 | 0.77 | 0.13 | |
| HIP FLX | R AVG | 1.94 (0.41) | 1.78–2.1 | 2.13 (0.41) | 1.97–2.29 | 7.7 | 0.81 | 10.1 | 0 | 0.46 |
| L AVG | 1.89 (0.35) | 1.75–2.03 | 2.18 (0.41) | 2.02–2.34 | 14.7 | 0.58 | 15.3 | 0 | 0.76 | |
| R MAX | 2.03 (0.42) | 1.86–2.2 | 2.22 (0.43) | 2.05–2.39 | 7.4 | 0.81 | 9.12 | 0.01 | 0.45 | |
| L MAX | 1.97 (0.36) | 1.83–2.11 | 2.25 (0.43) | 2.08–2.42 | 14.6 | 0.58 | 12.3 | 0 | 0.71 | |
| KNEE EXT | R AVG | 6.59 (1.81) | 5.87–7.31 | 6.44 (2.02) | 5.63–7.25 | 6.5 | 0.9 | 0.4 | 0.53 | 0.08 |
| L AVG | 6.24 (1.72) | 5.55–6.93 | 6.25 (2.33) | 5.32–7.18 | 7.8 | 0.9 | 0 | 0.95 | 0.00 | |
| R MAX | 6.91 (1.92) | 6.14–7.68 | 6.86 (2.16) | 6–7.72 | 6.2 | 0.9 | 0.04 | 0.84 | 0.02 | |
| L MAX | 6.59 (1.79) | 5.87–7.31 | 6.55 (2.33) | 5.62–7.48 | 5.4 | 0.92 | 0.03 | 0.86 | 0.02 | |
| ANKLE PFLX | R AVG | 4.86 (0.6) | 4.61–5.11 | 5.24 (0.88) | 4.87–5.62 | 7.2 | 0.57 | 5.51 | 0.03 | 0.51 |
| L AVG | 4.61 (0.5) | 4.4–4.82 | 4.87 (0.76) | 4.55–5.19 | 5.4 | 0.44 | 2.82 | 0.11 | 0.41 | |
| R MAX | 5.19 (0.59) | 4.94–5.44 | 5.51 (0.79) | 5.18–5.84 | 7.2 | 0.68 | 5.84 | 0.02 | 0.46 | |
| L MAX | 4.85 (0.54) | 4.62–5.08 | 5.15 (0.79) | 4.81–5.48 | 5.6 | 0.44 | 3.29 | 0.08 | 0.44 | |
| NHE | R AVG | 1.97 (0.44) | 1.79–2.15 | 2.06 (0.33) | 1.93–2.19 | 5.6 | 0.88 | 3.6 | 0.07 | 0.23 |
| L AVG | 1.92 (0.42) | 1.75–2.09 | 2.03 (0.33) | 1.9–2.16 | 5.5 | 0.88 | 6.14 | 0.02 | 0.29 | |
| B AVG | 3.88 (0.84) | 3.54–4.22 | 4.1 (0.65) | 3.84–4.36 | 5.4 | 0.88 | 5.15 | 0.03 | 0.29 | |
| R MAX | 2.06 (0.45) | 1.88–2.24 | 2.13 (0.33) | 2–2.26 | 6.1 | 0.85 | 1.47 | 0.24 | 0.18 | |
| L MAX | 1.98 (0.43) | 1.81–2.15 | 2.1 (0.33) | 1.97–2.23 | 5.8 | 0.87 | 5.51 | 0.03 | 0.31 | |
| B MAX | 4.03 (0.84) | 3.69–4.37 | 4.22 (0.65) | 3.96–4.48 | 5.9 | 0.86 | 3.34 | 0.08 | 0.25 | |
| Parameter | S1 Mean (SD) | S1 95% CI | S3 Mean (SD) | S3 95% CI | % CV | ICC2.k | Bias | ||
|---|---|---|---|---|---|---|---|---|---|
| F | sig | d | |||||||
| ADD:ABD UNI R | 105.74 (24.58) | 95.91–115.57 | 105.8 (25.25) | 95.7–115.9 | 12.4 | 0.68 | 0 | 0.99 | 0.00 |
| ADD:ABD UNI L | 112.13 (24.5) | 102.33–121.93 | 112.72 (34.35) | 98.98–126.46 | 25.6 | 0.30 | 0.01 | 0.94 | 0.02 |
| ADD:ABD BI R | 102.03 (17.51) | 93.32–110.4 | 102.55 (17.35) | 93.96–110.89 | 3.2 | 0.92 | 0.07 | 0.79 | 0.03 |
| ADD:ABD BI L | 103.19 (19.66) | 92.89–111.99 | 103.72 (13.43) | 97.03–109.81 | 4.4 | 0.89 | 0.06 | 0.81 | 0.03 |
| IR:ER UNI R | 97.08 (24.47) | 86.85–107.31 | 97.62 (26.62) | 86.97–108.27 | 11.9 | 0.78 | 0.06 | 0.81 | 0.02 |
| IR:ER UNI L | 95.14 (28.38) | 83.79–106.49 | 91.94 (26.26) | 81.43–102.45 | 12.0 | 0.73 | 0.38 | 0.54 | 0.12 |
| IR:ER BI R | 125.85 (32.2) | 109.87–138.97 | 121.94 (28.93) | 108.21–135.89 | 16.2 | 0.58 | 0.33 | 0.57 | 0.13 |
| IR:ER BI L | 122.04 (26.94) | 109.79–133.06 | 114.37 (23.85) | 103.02–125.12 | 12.5 | 0.67 | 2.25 | 0.15 | 0.30 |
| FLX:EXT UNI R | 74.8 (15.67) | 68.25–81.35 | 82.38 (16.34) | 75.84–88.92 | 18.1 | 0.55 | 4.02 | 0.06 | 0.47 |
| FLX:EXT UNI L | 74.89 (14.43) | 68.86–80.92 | 88.92 (13.96) | 83.33–94.51 | 12.6 | 0.53 | 19.18 | 0.00 | 0.99 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marušič, J.; Marković, G.; Šarabon, N. Reliability of a New Portable Dynamometer for Assessing Hip and Lower Limb Strength. Appl. Sci. 2021, 11, 3391. https://doi.org/10.3390/app11083391
Marušič J, Marković G, Šarabon N. Reliability of a New Portable Dynamometer for Assessing Hip and Lower Limb Strength. Applied Sciences. 2021; 11(8):3391. https://doi.org/10.3390/app11083391
Chicago/Turabian StyleMarušič, Jan, Goran Marković, and Nejc Šarabon. 2021. "Reliability of a New Portable Dynamometer for Assessing Hip and Lower Limb Strength" Applied Sciences 11, no. 8: 3391. https://doi.org/10.3390/app11083391
APA StyleMarušič, J., Marković, G., & Šarabon, N. (2021). Reliability of a New Portable Dynamometer for Assessing Hip and Lower Limb Strength. Applied Sciences, 11(8), 3391. https://doi.org/10.3390/app11083391