
Assessment of Mineralization, Oxidative Stress, and Inflammation Mechanisms in the Pulp of Primary Teeth

 , , , ,
, , , , 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Criteria for Diagnosis
2.3. Procedures for Samples Collection
2.4. Pulp Lysates Preparation and Determination Using Enzyme-Linked Immunosorbent Assay (ELISA) Analysis
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Farges, J.C.; Alliot-Licht, B.; Renard, E.; Ducret, M.; Gaudin, A.; Smith, A.J.; Cooper, P.R. Dental Pulp Defence and Repair Mechanisms in Dental Caries. Mediat. Inflamm. 2015, 2015, 230251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Šubarić, L.; Mitić, A.; Matvijenko, V.; Jovanović, R.; Živković, D.; Perić, D.; Vlahović, Z. Interleukin 1-beta analysis in chronically inflamed and healthy human dental pulp. Vojnosanit. Pregl. 2017, 74, 256–260. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; Bester, J.; Pretorius, E. The inflammatory effects of TNF-alpha and complement component 3 on coagulation. Sci. Rep. 2018, 8, 1812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, C.C.; Lin, W.N.; Cho, R.L.; Wang, C.Y.; Hsiao, L.D.; Yang, C.M. TNF-alpha-Induced cPLA2 Expression via NADPH Oxidase/Reactive Oxygen Species-Dependent NF-kappaB Cascade on Human Pulmonary Alveolar Epithelial Cells. Front. Pharmacol. 2016, 7, 447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Branicky, R.; Noe, A.; Hekimi, S. Superoxide dismutases: Dual roles in controlling ROS damage and regulating ROS signaling. J. Cell Biol. 2018, 217, 1915–1928. [Google Scholar] [CrossRef]
- Zanini, M.; Meyer, E.; Simon, S. Pulp Inflammation Diagnosis from Clinical to Inflammatory Mediators: A Systematic Review. J. Endod. 2017, 43, 1033–1051. [Google Scholar] [CrossRef]
- Ji, S.; Song, S.; Lee, J.; Kim, J.; Kim, J. Characterization of Odontoblasts in Supernumerary Tooth-derived Dental Pulp Stem Cells between Passages by Real-Time PCR. J. Korean Acad. Pediatr. Dent. 2021, 48, 291–301. [Google Scholar] [CrossRef]
- Abd-Elmeguid, A.; Abdeldayem, M.; Kline, L.W.; Moqbel, R.; Vliagoftis, H.; Yu, D.C. Osteocalcin expression in pulp inflammation. J. Endod. 2013, 39, 865–872. [Google Scholar] [CrossRef]
- Chisini, L.A.; Conde, M.C.; Alcazar, J.C.; Silva, A.F.; Nor, J.E.; Tarquinio, S.B.; Demarco, F.F. Immunohistochemical Expression of TGF-beta1 and Osteonectin in engineered and Ca(OH)2-repaired human pulp tissues. Braz. Oral Res. 2016, 30, e93. [Google Scholar] [CrossRef] [Green Version]
- Giuroiu, C.L.; Caruntu, I.D.; Lozneanu, L.; Melian, A.; Vataman, M.; Andrian, S. Dental Pulp: Correspondences and Contradictions between Clinical and Histological Diagnosis. BioMed Res. Int. 2015, 2015, 960321. [Google Scholar] [CrossRef]
- Ghaderi, F.; Jowkar, Z.; Tadayon, A. Caries Color, Extent, and Preoperative Pain as Predictors of Pulp Status in Primary Teeth. Clin. Cosmet. Investig. Dent. 2020, 12, 263–269. [Google Scholar] [CrossRef]
- Aishuwariya, T.; Ramesh, S. Evaluation Of Interleukin 6, Interleukin 8, TNF Alpha as Biomarkers For Pulpitis—In Vivo Study. Int. J. Dent. Oral Sci. 2021, 8, 1492–1497. [Google Scholar] [CrossRef]
- Tripodi, D.; Latrofa, M.; D’ercole, S. Microbiological aspects and inflammatory response of pulp tissue in traumatic dental lesions. Eur. J. Inflamm. 2007, 5, 1721–1727. [Google Scholar] [CrossRef] [Green Version]
- American Association of Endodontists. Glossary of Endodontic Terms; American Association of Endodontists: Chicago, IL, USA, 2020. [Google Scholar]
- WHO. Oral Health. Available online: https://www.who.int/news-room/fact-sheets/detail/oral-health (accessed on 10 December 2021).
- Raducanu, A.M. Pedodontie Indrumar Practic, 1st ed.; Bren: Bucharest, Romania, 2018. (In Romanian) [Google Scholar]
- Suwanchai, A.; Theerapiboon, U.; Chattipakorn, N.; Chattipakorn, S.C. NaV 1.8, but not NaV 1.9, is upregulated in the inflamed dental pulp tissue of human primary teeth. Int. Endod. J. 2012, 45, 372–378. [Google Scholar] [CrossRef]
- Gusman, H.; Santana, R.B.; Zehnder, M. Matrix metalloproteinase levels and gelatinolytic activity in clinically healthy and inflamed human dental pulps. Eur. J. Oral. Sci. 2002, 110, 353–357. [Google Scholar] [CrossRef]
- Sattari, M.; Haghighi, A.K.; Tamijani, H.D. The relationship of pulp polyp with the presence and concentration of immunoglobulin E, histamine, interleukin-4 and interleukin-12. Aust. Endod. J. 2009, 35, 164–168. [Google Scholar] [CrossRef]
- Evrosimovska, B.; Dimova, C.; Kovacevska, I.; Panov, S. Concentration of collagenases (MMP-1, -8, -13) in patients with chronically inflamed dental pulp tissue. Prilozi 2012, 33, 191–204. [Google Scholar]
- Serra, M.B.; Barroso, W.A.; da Silva, N.N.; Silva, S.D.N.; Borges, A.C.R.; Abreu, I.C.; Borges, M. From Inflammation to Current and Alternative Therapies Involved in Wound Healing. Int. J. Inflam. 2017, 2017, 3406215. [Google Scholar] [CrossRef] [Green Version]
- Pezelj-Ribaric, S.; Anic, I.; Brekalo, I.; Miletic, I.; Hasan, M.; Simunovic-Soskic, M. Detection of tumor necrosis factor alpha in normal and inflamed human dental pulps. Arch. Med. Res. 2002, 33, 482–484. [Google Scholar] [CrossRef]
- Elsalhy, M.; Azizieh, F.; Raghupathy, R. Cytokines as diagnostic markers of pulpal inflammation. Int. Endod. J. 2013, 46, 573–580. [Google Scholar] [CrossRef]
- Kokkas, A.B.; Goulas, A.; Varsamidis, K.; Mirtsou, V.; Tziafas, D. Irreversible but not reversible pulpitis is associated with up-regulation of tumour necrosis factor-alpha gene expression in human pulp. Int. Endod. J. 2007, 40, 198–203. [Google Scholar] [CrossRef]
- Keller, J.F.; Carrouel, F.; Staquet, M.J.; Kufer, T.A.; Baudouin, C.; Msika, P.; Bleicher, F.; Farges, J.C. Expression of NOD2 is increased in inflamed human dental pulps and lipoteichoic acid-stimulated odontoblast-like cells. Innate Immun. 2011, 17, 29–34. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Ding, W.-S.; Zhao, J.; Liu, Z.-H.; Wang, J.-H. Detection of TNF-α in dental pulps of normal, acute and chronic pulpitis. J. Shandong Univ. (Health Sci.) 2005, 1, 25. [Google Scholar]
- Baumgardner, K.R.; Sulfaro, M.A. The anti-inflammatory effects of human recombinant copper-zinc superoxide dismutase on pulp inflammation. J. Endod. 2001, 27, 190–195. [Google Scholar] [CrossRef]
- Bodor, C.; Matolcsy, A.; Bernath, M. Elevated expression of Cu, Zn-SOD and Mn-SOD mRNA in inflamed dental pulp tissue. Int. Endod. J. 2007, 40, 128–132. [Google Scholar] [CrossRef]
- Davis, W.L.; Jacoby, B.H.; Craig, K.R.; Wagner, G.; Harrison, J.W. Copper-zinc superoxide dismutase activity in normal and inflamed human dental pulp tissue. J. Endod. 1991, 17, 316–318. [Google Scholar] [CrossRef]
- Ge, J.; Ji, J.; Wang, T. Superoxide dismutase and malonyl dialdehyde in human pulp tissue. Zhonghua Kou Qiang Yi Xue Za Zhi 1996, 31, 201–203. [Google Scholar]
- Tulunoglu, O.; Alacam, A.; Bastug, M.; Yavuzer, S. Superoxide dismutase activity in healthy and inflamed pulp tissues of permanent teeth in children. J. Clin. Pediatr. Dent. 1998, 22, 341–345. [Google Scholar]
- Varvara, G.; Traini, T.; Esposito, P.; Caputi, S.; Perinetti, G. Copper-zinc superoxide dismutase activity in healthy and inflamed human dental pulp. Int. Endod. J. 2005, 38, 195–199. [Google Scholar] [CrossRef]
- Piattelli, A.; Rubini, C.; Fioroni, M.; Tripodi, D.; Strocchi, R. Transforming growth factor-beta 1 (TGF-beta 1) expression in normal healthy pulps and in those with irreversible pulpitis. Int. Endod. J. 2004, 37, 114–119. [Google Scholar] [CrossRef]
- Jarad, M.; Kuczynski, E.A.; Morrison, J.; Viloria-Petit, A.M.; Coomber, B.L. Release of endothelial cell associated VEGFR2 during TGF-beta modulated angiogenesis in vitro. BMC Cell Biol. 2017, 18, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niwa, T.; Yamakoshi, Y.; Yamazaki, H.; Karakida, T.; Chiba, R.; Hu, J.C.; Nagano, T.; Yamamoto, R.; Simmer, J.P.; Margolis, H.C.; et al. The dynamics of TGF-beta in dental pulp, odontoblasts and dentin. Sci. Rep. 2018, 8, 4450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laurent, P.; Camps, J.; About, I. Biodentine(TM) induces TGF-beta1 release from human pulp cells and early dental pulp mineralization. Int. Endod. J. 2012, 45, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.C.; Chang, H.H.; Lin, P.S.; Huang, Y.A.; Chan, C.P.; Tsai, Y.L.; Lee, S.Y.; Jeng, P.Y.; Kuo, H.Y.; Yeung, S.Y.; et al. Effects of TGF-beta1 on plasminogen activation in human dental pulp cells: Role of ALK5/Smad2, TAK1 and MEK/ERK signalling. J. Tissue Eng. Regen. Med. 2018, 12, 854–863. [Google Scholar] [CrossRef]
- Manolagas, S.C. Osteocalcin promotes bone mineralization but is not a hormone. PLoS Genet. 2020, 16, e1008714. [Google Scholar] [CrossRef]
- Moser, S.C.; van der Eerden, B.C.J. Osteocalcin-A Versatile Bone-Derived Hormone. Front. Endocrinol. 2018, 9, 794. [Google Scholar] [CrossRef] [Green Version]
- Hirata, M.; Yamaza, T.; Mei, Y.F.; Akamine, A. Expression of osteocalcin and Jun D in the early period during reactionary dentin formation after tooth preparation in rat molars. Cell Tissue Res. 2005, 319, 455–465. [Google Scholar] [CrossRef]
- Ho, M.H.; Yao, C.J.; Liao, M.H.; Lin, P.I.; Liu, S.H.; Chen, R.M. Chitosan nanofiber scaffold improves bone healing via stimulating trabecular bone production due to upregulation of the Runx2/osteocalcin/alkaline phosphatase signaling pathway. Int. J. Nanomed. 2015, 10, 5941–5954. [Google Scholar] [CrossRef] [Green Version]
- Vetra, A.; Smane, L.; Pilmane, M.; Vilka, L. Osteopontin, osteocalcin, and osteoprotegerin expression in human tissue affected by cleft lip and palate. SHS Web Conf. 2016, 30, 00008. [Google Scholar] [CrossRef] [Green Version]
- Ballini, A.; Tete, S.; Scattarella, A.; Cantore, S.; Mastrangelo, F.; Papa, F.; Nardi, G.M.; Perillo, L.; Crincoli, V.; Gherlone, E.; et al. The role of anti-cyclic citrullinated peptide antibody in periodontal disease. Int. J. Immunopathol. Pharmacol. 2010, 23, 677–681. [Google Scholar] [CrossRef]
- Cooper, P.R.; Chicca, I.J.; Holder, M.J.; Milward, M.R. Inflammation and Regeneration in the Dentin-pulp Complex: Net Gain or Net Loss? J. Endod. 2017, 43, S87–S94. [Google Scholar] [CrossRef]
- Mullen, A.C.; Wrana, J.L. TGF-beta Family Signaling in Embryonic and Somatic Stem-Cell Renewal and Differentiation. Cold Spring Harb. Perspect. Biol. 2017, 9, a022186. [Google Scholar] [CrossRef]
- Cappare, P.; Tete, G.; Sberna, M.T.; Panina-Bordignon, P. The Emerging Role of Stem Cells in Regenerative Dentistry. Curr. Gene Ther. 2020, 20, 259–268. [Google Scholar] [CrossRef]
- Tete, G.; D’Orto, B.; Nagni, M.; Agostinacchio, M.; Polizzi, E.; Agliardi, E. Role of induced pluripotent stem cells (IPSCS) in bone tissue regeneration in dentistry: A narrative review. J. Biol. Regul. Homeost. Agents 2020, 34, 1–10. [Google Scholar]
- Ledesma-Martinez, E.; Mendoza-Nunez, V.M.; Santiago-Osorio, E. Mesenchymal Stem Cells Derived from Dental Pulp: A Review. Stem. Cells Int. 2016, 2016, 4709572. [Google Scholar] [CrossRef] [Green Version]
- Harichane, Y.; Hirata, A.; Dimitrova-Nakov, S.; Granja, I.; Goldberg, A.; Kellermann, O.; Poliard, A. Pulpal progenitors and dentin repair. Adv. Dent. Res. 2011, 23, 307–312. [Google Scholar] [CrossRef]
- Brizuela, C.; Meza, G.; Mercade, M.; Inostroza, C.; Chaparro, A.; Bravo, I.; Briceno, C.; Hernandez, M.; Giner, L.; Ramirez, V. Inflammatory biomarkers in dentinal fluid as an approach to molecular diagnostics in pulpitis. Int. Endod. J. 2020, 53, 1181–1191. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Biomarker | Clinically Healthy Pulp Samples | Acute Inflamed Pulp Samples | Chronically Inflamed Pulp Samples | p Value |
|---|---|---|---|---|
| TNF-α (pg/mg prot.) (median (IQR)) | 5.6 (3.55–9) | 55 (52–61) | 49 (41–59) | <0.001 * |
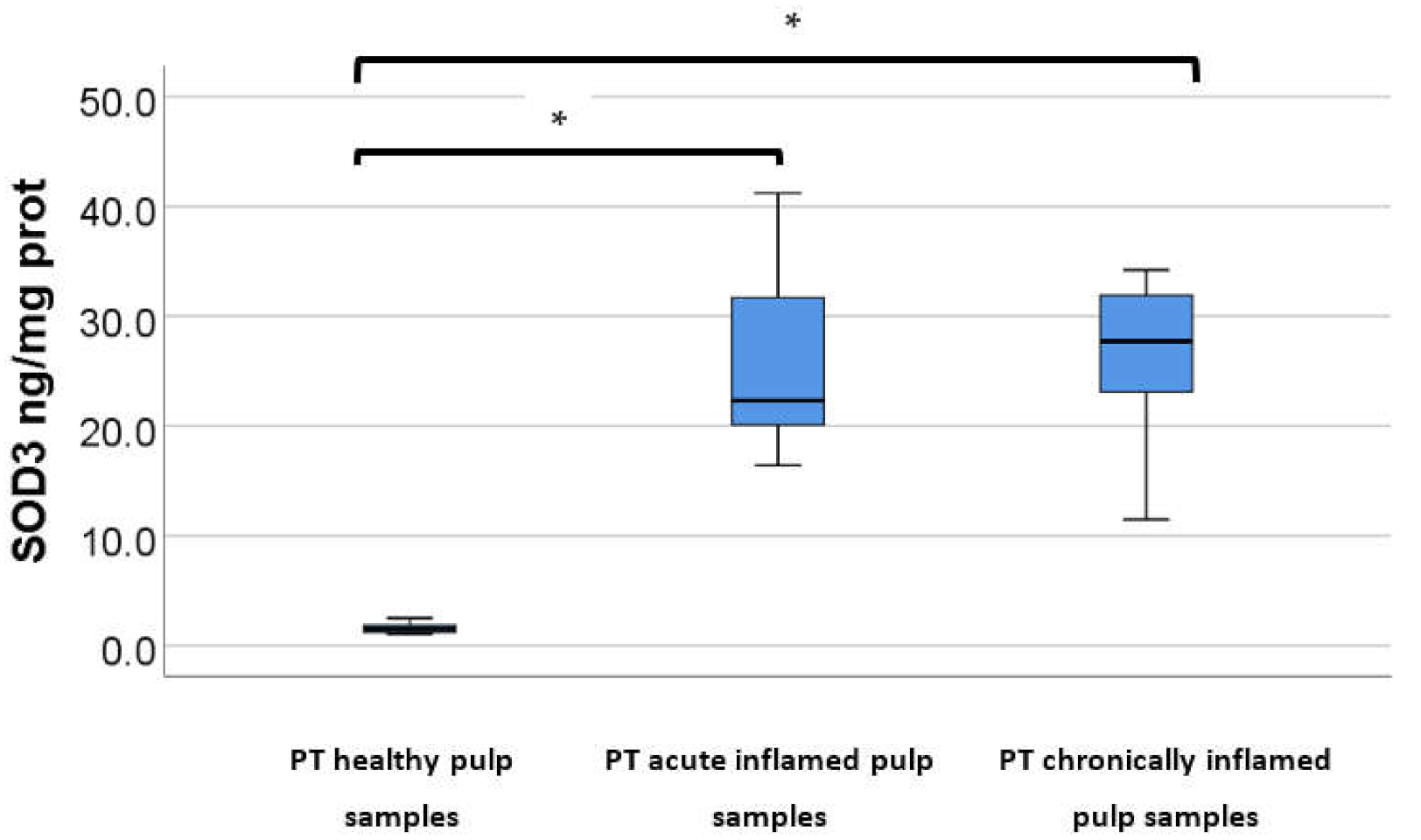
| SOD-3 (ng/mg prot.) (mean ± SD) | 1.56 ± 0.44 | 27.45 ± 8.31 | 26.78 ± 7.16 | <0.001 ** |
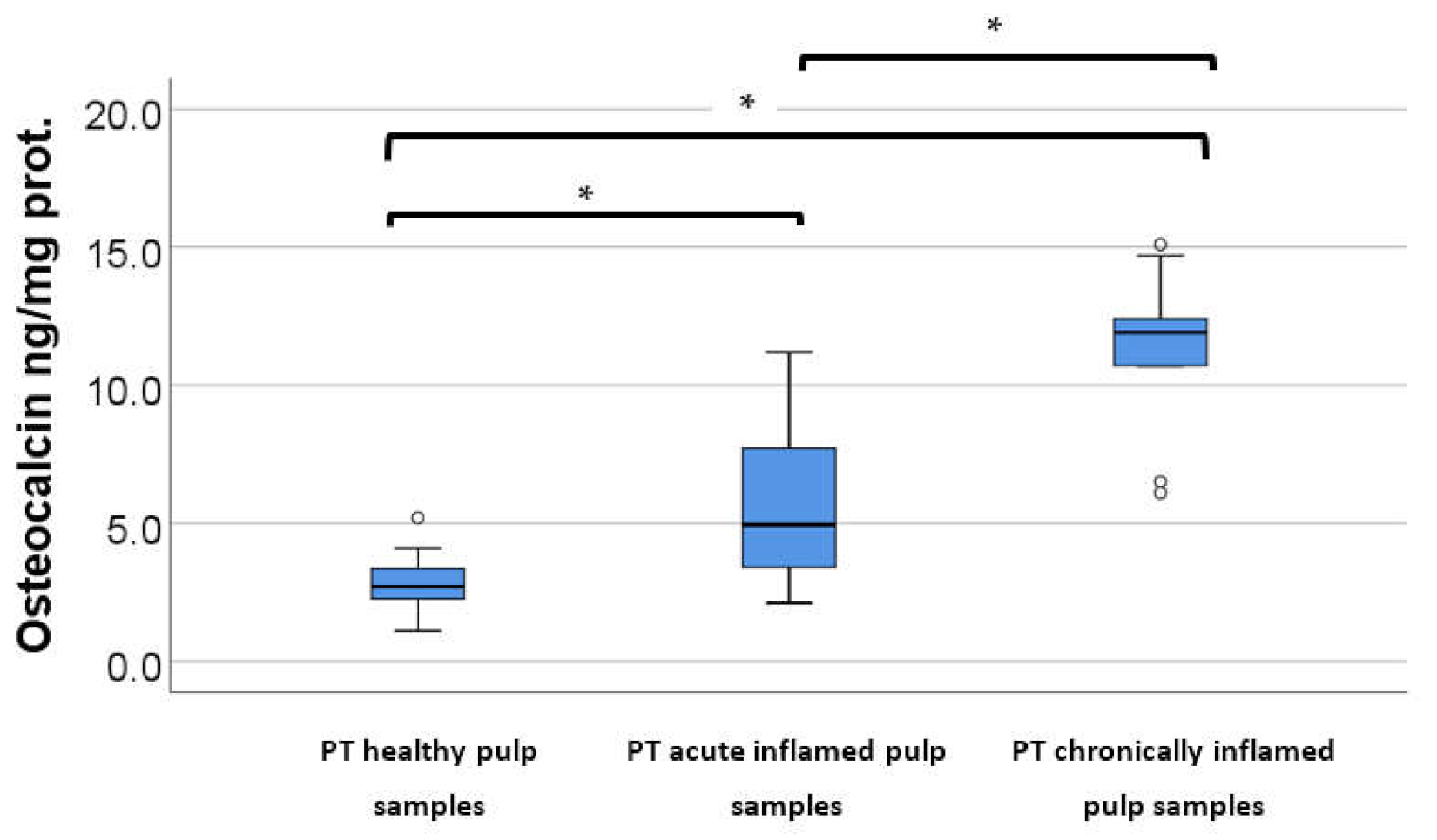
| Osteocalcin (ng/mg prot.) (mean ± SD) | 2.51 ± 1 | 5.87 ± 3 | 11.23 ± 3.13 | <0.001 ** |
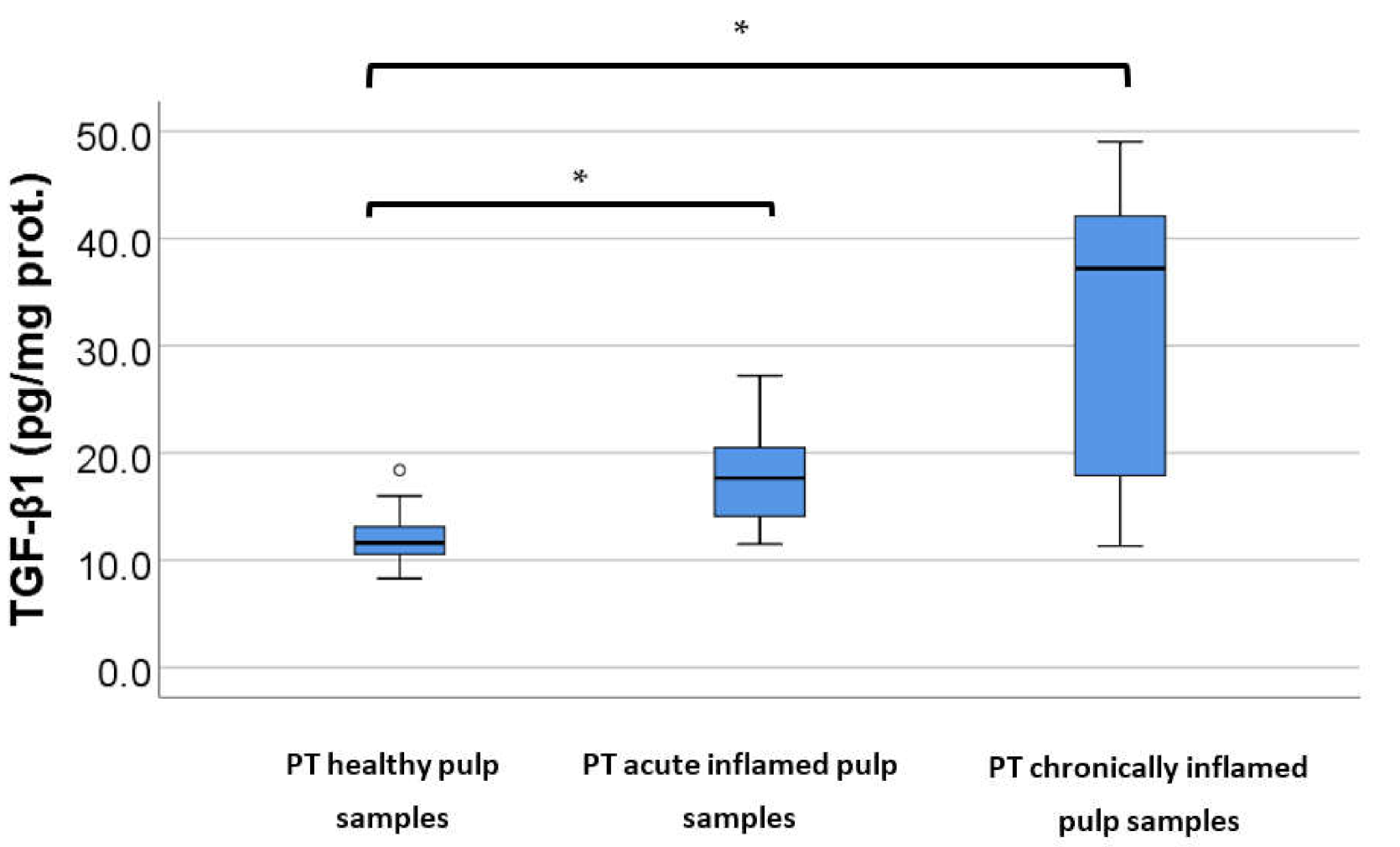
| TGF-β1 (pg/mg prot.) (mean ± SD) | 13.24 ± 1.48 | 18.07 ± 4.5 | 31.06 ± 15.3 | <0.001 ** |
| Comparison/Variable | Healthy vs. Acute | Healthy vs. Chronic | Acute vs. Chronic |
|---|---|---|---|
| TNF-α * | <0.001 | 0.001 | 1.000 |
| SOD-3 ** | <0.001 | <0.001 | 1.000 |
| Osteocalcin ** | 0.006 | <0.001 | 0.002 |
| TGF-β1 ** | 0.001 | 0.014 | 0.082 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kritikou, K.; Imre, M.; Tanase, M.; Vinereanu, A.; Ripszky Totan, A.; Spinu, T.-C.; Miricescu, D.; Stanescu-Spinu, I.-I.; Bordea, M.; Greabu, M. Assessment of Mineralization, Oxidative Stress, and Inflammation Mechanisms in the Pulp of Primary Teeth. Appl. Sci. 2022, 12, 1554. https://doi.org/10.3390/app12031554
Kritikou K, Imre M, Tanase M, Vinereanu A, Ripszky Totan A, Spinu T-C, Miricescu D, Stanescu-Spinu I-I, Bordea M, Greabu M. Assessment of Mineralization, Oxidative Stress, and Inflammation Mechanisms in the Pulp of Primary Teeth. Applied Sciences. 2022; 12(3):1554. https://doi.org/10.3390/app12031554
Chicago/Turabian StyleKritikou, Konstantina, Marina Imre, Mihaela Tanase, Arina Vinereanu, Alexandra Ripszky Totan, Tudor-Claudiu Spinu, Daniela Miricescu, Iulia-Ioana Stanescu-Spinu, Marilena Bordea, and Maria Greabu. 2022. "Assessment of Mineralization, Oxidative Stress, and Inflammation Mechanisms in the Pulp of Primary Teeth" Applied Sciences 12, no. 3: 1554. https://doi.org/10.3390/app12031554
APA StyleKritikou, K., Imre, M., Tanase, M., Vinereanu, A., Ripszky Totan, A., Spinu, T. -C., Miricescu, D., Stanescu-Spinu, I. -I., Bordea, M., & Greabu, M. (2022). Assessment of Mineralization, Oxidative Stress, and Inflammation Mechanisms in the Pulp of Primary Teeth. Applied Sciences, 12(3), 1554. https://doi.org/10.3390/app12031554