1. Introduction
Regenerative endodontic procedures (REPs) have emerged as a treatment option for immature necrotic teeth with apical periodontitis to allow the reestablishment of a newly formed vital tissue and enable continued root development. There is no standard protocol of REPs; hence, the American Association of Endodontists (AAE) as well as the European Society of Endodontology (ESE) suggest Quality Clinical Guidelines for a regenerative procedure which was adapted in both of the case reports hereby described [
1,
2]. The clinical protocol of REPs differs mostly in terms of concentrations of sodium hypochlorite irrigant, intracanal medication, the method to induce the bleeding, and the use of biological matrices (
Table 1).
One of the goals of REP is root thickness and length augmentation to reinforce root canal walls [
3]. The appropriate management of infected canals can create a favorable environment for tissue regeneration since open-apex immature teeth favor the reestablishment of a rich blood supply and stem cells [
4]. Considerable advances in disinfection techniques that combine the balance between antimicrobial effect and biocompatibility with mesenchymal stem cells (MSCs) have been developed. Similarly, it has been demonstrated that intracanal bleeding evoked from the apical tissues brings substantial numbers of MSCs into the canal system during REPs in immature teeth [
5]. However, the characteristics and phenotype of this tissue in the presence of inflammation are still largely unknown [
6].
The apical papilla is the source of a particular type of MSC, namely, stem cells of the apical papilla (SCAPs), which plays an important role in physiologic root development and may also contribute to further root development during REPs [
4,
7,
8].
The development of a normal dentin–pulp complex implies not only the survival of SCAPs but also the presence of epithelial cells, derived from Hertwig’s epithelial root sheath (HERS) or its defragmentation as epithelial rests of Malassez (ERM), that allows their interaction with each other and recapitulates the early events of tooth development [
9].Moreover, HERS acts as a barrier between the dental follicle and dental papilla cells as well as a regulator for shape, size, and number of roots and dentin and cementum development [
10].
HERS and the apical papilla are two embryologic structures which coordinate all the radicular development through epithelial–mesenchymal interactions. During endodontic infection in immature teeth with an open apex, diagnosed with pulp necrosis and apical periodontitis, the microenvironment created in the apical area as well as the presence of a microbial biofilm may provoke the death of the undifferentiated cells from the apical papilla and HERS and consequently root development will be impaired [
11].
In the literature concerning this theme, there have been some clinical cases in which radiology confirmed remarkable progress in root development after apexogenesis/maturogenesis or REPs [
12,
13,
14,
15], or the formation of a root-tip further away from the corresponding root wall [
16]. Moreover, recent histologic findings from animal studies [
17,
18] and human clinical cases [
19] give information about the nature of the newly formed tissues after REPs.
The main goal of those two case reports is to show evidence of the apical papilla survival and development, in human teeth with apical periodontitis, after regenerative endodontic procedures, and with 5-years clinical and radiographic follow-up.
2. Case Report
2.1. Case 1
An 11-year-old girl was referred for REP of tooth 15. Her medical history was noncontributory. Sensibility tests (heat, cold, and electrical pulp testing) of the tooth 15 were negative, with evidence of coronal restoration leakage. Clinical examination showed that tooth 15 had edema and suppuration with sinus tract (chronic apical abscess), pain with vertical and lateral percussion, no mobility and the probing depth was within normal limits. Radiographically, the root canal was wide with a divergent open apical foramen (
Figure 1A). After assessing the possibility of restoring the tooth without intracanal post and explaining all therapeutic alternatives to the patient and guardians, informed consent was obtained, and REP was performed. Local anesthesia was achieved with 3% mepivacaine (Mepivastesin
®, 3M ESPE, Neuss, Germany). After isolation with a rubber dam, restorative material and carious lesions were removed and the access cavity was performed. After access, the wide-open canal was observed by dental microscope (Leica M320 F12, Leica Microsystems, Heerbrugg Switzerland) with 10x magnification depicting that some vital pulp tissue remained inside the root canal. The working length to this vital tissue was confirmed with paper points (size #80, Dentsply-Maillefer, Balaigues, Switzerland) by the presence of bleeding at 15 millimeters (mm). The canal was irrigated with 20 mL of 3% sodium hypochlorite (NaOCl; CanalPro
TM 3%, Coltène/Whaledent, Langenau, Germany) using a Navitip
TM needle (Ultradent Products Inc, South Jordan, UT) at 13 mm, followed by rinsing with 20 mL of a saline solution for 5 minutes (min). The canal was dried with paper points, and intracanal medication of 45% calcium hydroxide (Calcicur Voco, Cuxhaven, Germany) (CH) paste was placed into the canal. The access cavity was sealed with a sterilized cotton pellet and Cavit
TM (3M, Neuss, Germany) and intermediate restorative material (IRM
®, DentsplyDetrey GmgH, Konstanz, Germany). The patient was scheduled for a second visit after 4 weeks.
The tooth (15) was asymptomatic during the entire postoperative period, with no sinus tract or edema, and the temporary filling was intact. In the second session, local anesthesia was accomplished with 3% mepivacaine (Mepivastesin®, 3M ESPE, Neuss, Germany). Under the rubber dam, temporary material and cotton pellet were removed from the access cavity and the canal was rinsed with 20 mL of EDTA 17% (Coltène/Whaledent, Langenau, Germany) for 5 min, followed by irrigation with 5 mL of a sterile saline solution. The root canal space was dried with paper points and a microsurgical suction tip (Roeko Surgitip-endo, Coltène/Whaledent, Langenau, Germany). Subsequently, a manual sterilized k-file (size #25, Dentsply-Maillefer, Balaigues, Switzerland) was introduced until reaching the 15 mm working length and then deliberately pushed 2 mm past the working length to induce bleeding into the canal. After blood filled the canal up to 2 mm bellow cementoenamel junction (CEJ), an absorbable hemostatic gelatin matrix (Spongostan DentalTM, MS0005, Ethicon Inc, New Jersey, EUA) was placed over the blood clot. Finally, a 3 mm mineral trioxide aggregate barrier (ProRoot® MTA, Dentsply Tulsa Dental, Johnson City, TN, USA) was placed in the cervical third of the root canal with a coronal barrier (Buchanan Hand Barrierger #2; SybronEndo, Orange, CA, USA) over the blood clot. After placing a moist cotton pellet over the MTA, the access cavity was sealed with a temporary restoration material (CavitTM) and two weeks later replaced with a resin-based composite (SDRTM flow and Spectrum®, DentsplyDetrey GmgH, Konstanz, Germany).
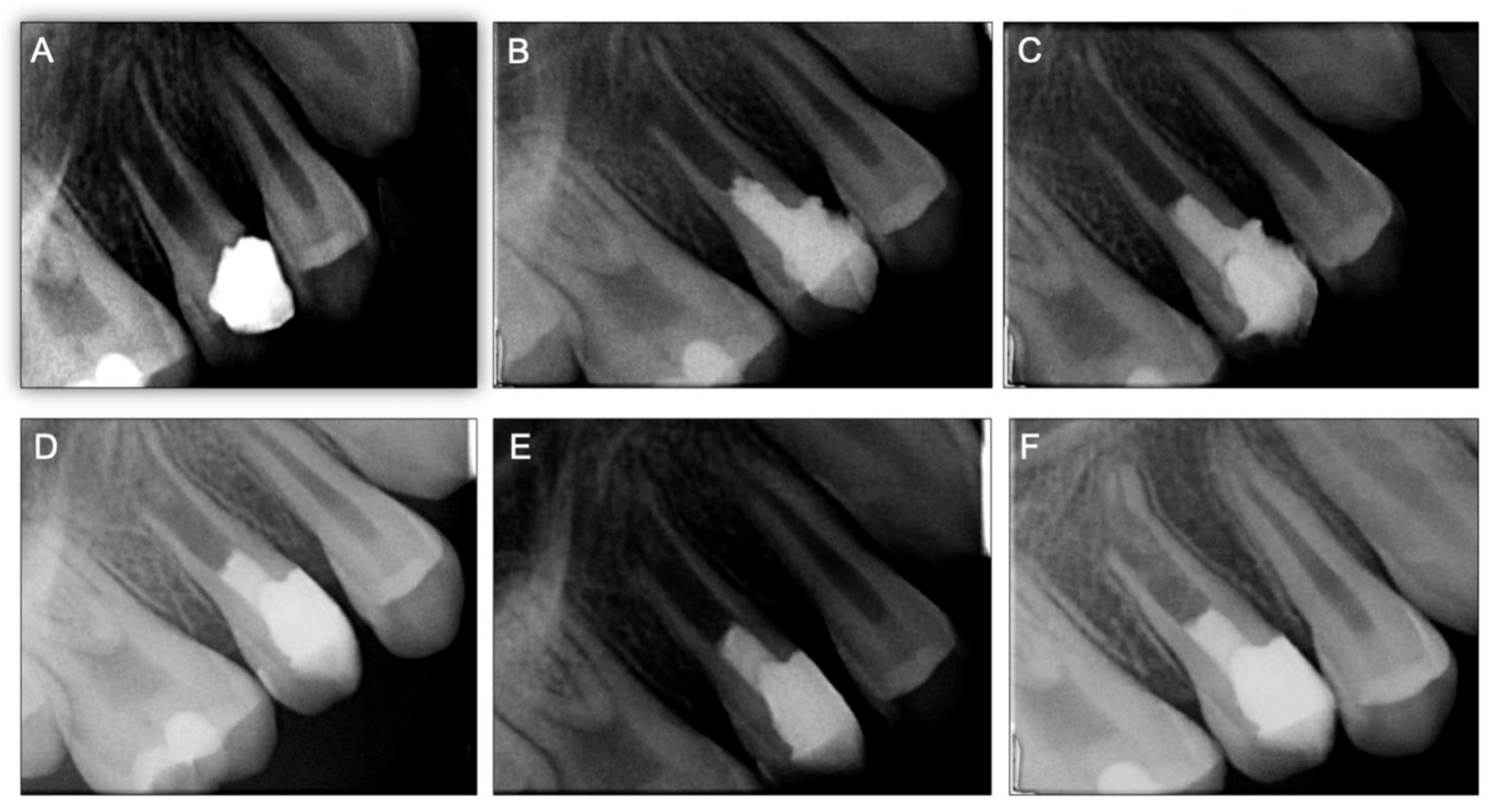
After REPs, the tooth (15) was asymptomatic without signs of coronal discoloration. Follow-up was successively performed at 3, 6, 12 months, 3 years, and 5 years (
Figure 1E,F and
Figure 2). The radiographic evaluation depicted a continuity of the periodontal ligament space (confirming the absence of an apical radiolucency) as well as an appreciable increase in the root length and thickness. With the progression in time of follow-up, the partial separation of the apical root portion observed at 3, 6, and 12 months decreased significantly compared to the 2- and 5-year follow-up X-rays. After 5 years, a fully developed root structure was observed at the periapical radiography, and on the cone-beam computed tomographic (CBCT) scan (
Supplementary materials: Video S1A, S1B), with an increase in length and thickness of the root walls as well as a decrease of the root canal lumen width.
2.2. Case 2
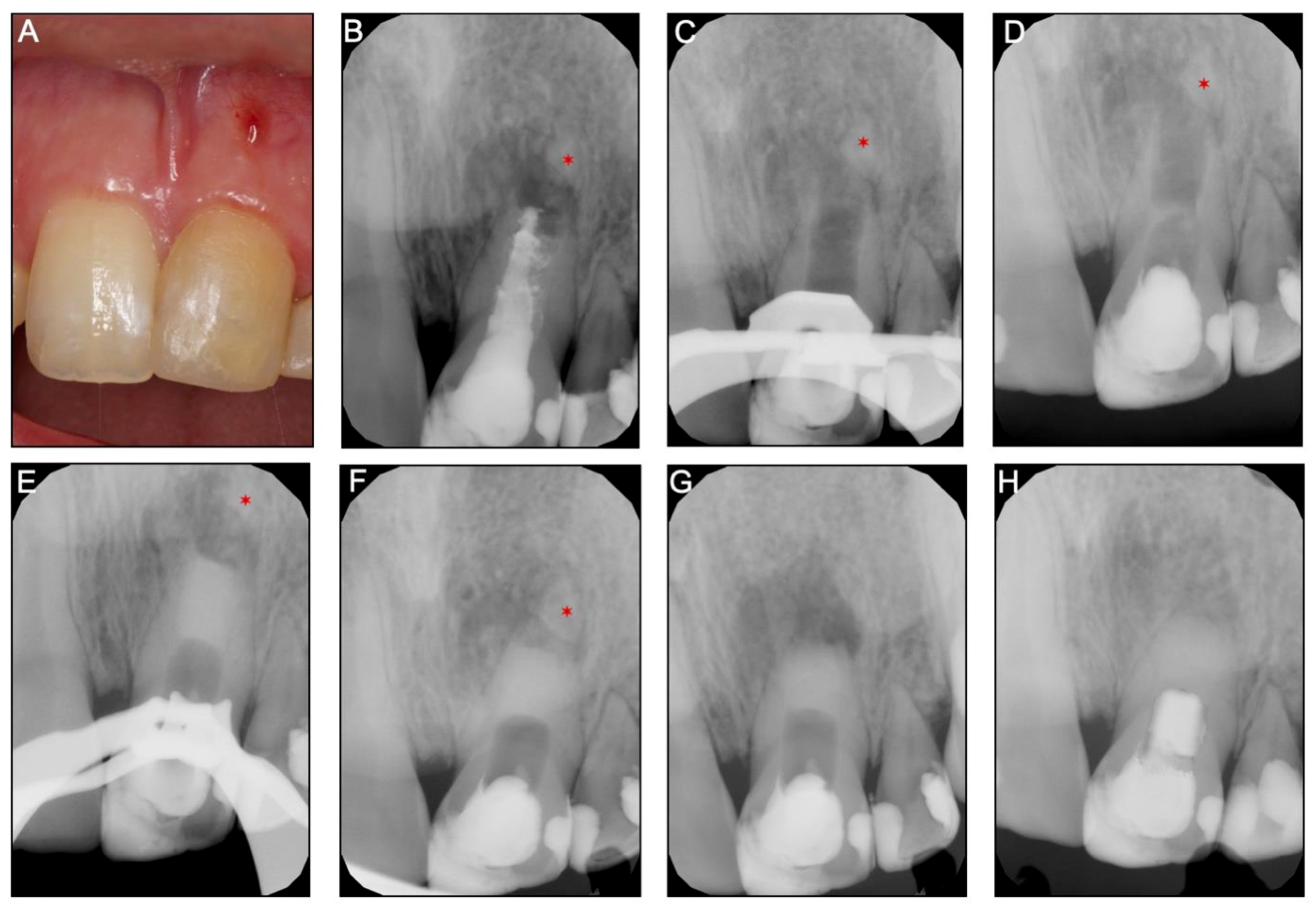
A 16-year-old girl was referred for the nonsurgical endodontic retreatment of the maxillary left central incisor (21) with pulp necrosis and chronic apical periodontitis with the presence of a long-standing sinus tract and a previous endodontic treatment failure. The periapical radiograph and CBTC revealed the maxillary left central incisor with pulp chamber and the canal underfilled with core material and a mineralized tissue beyond the tooth apical portion, separated from the root (
Figure 3A,B and
Supplementary Materials: Video S2). The agenesis of several teeth was confirmed (12, 22, 32, and 42) with the patient records. Previous dental trauma (non-specified on the parent’s records) on tooth 21 at age 7, followed by an attempt of REP by a generalist dentist, two years before the visit was referred by the child parents. However, the patient remained with edema, swelling, and a sinus tract associated with tooth 21. At the day of evaluation, tooth 21 had normal periodontal probing, and response to sensibility tests (thermal and electrical pulp testing) was negative. After an extended discussion with the children parents about the several treatment options, a nonsurgical root canal retreatment with an apical barrier with a biomaterial (Biodentine
TM, Septodont, Saint-Maur-des-Fossés Cedex, France) was elected.
At the first appointment, anesthesia was performed with 3% mepivacaine (Mepivastesin
®, 3M ESPE, Neuss, Germany) and under the rubber dam, an access cavity was made with a diamond bur (size #12, Dentsply Sirona, Ballaigues, Switzerland) and refined with an Endo-Z drill (Dentsply Maillefer, Ballaigues, Switzerland). After accessing the pulp chamber, a previous root filling was removed under magnification. Then, a long-neck (LN) bur (size #10, Dentsply Sirona, Ballaigues Switzerland) and an ultrasonic tip (size #3, Start-X
TM, Dentsply Sirona, Ballaigues Switzerland) were used to remove the hard material from the canal walls, which was similar to a hydraulic silicate cement (
Figure 3C). The same tip was used for ultrasonic agitation of the irrigant. After minimal manual instrumentation with a K-file (size #50, Dentsply-Maillefer, Balaigues, Switzerland) of the canal walls, the disinfection procedure was achieved with copious irrigation of 3% sodium hypochlorite (NaOCl; CanalPro
TM, Coltène/Whaledent, Langenau, Germany). Intracanal medication (45% CH, Calcicur) was placed in the coronal portion of the canal (
Figure 3C) and the access cavity closed with a temporary restorative material (Cavit
TM).
Three weeks later, the tooth (21) was asymptomatic, and no edema or sinus tract were observed. In the second session, local anesthesia was performed with 2% lidocaine with 1:100,000 epinephrine (XylesteinTM 2%, 3M ESPE, Neuss, Germany), a rubber dam placed, and the provisional material was removed.
The intracanal medication was removed with continuous irrigation of 3% sodium hypochlorite (NaOCl; CanalProTM, Coltène/Whaledent, Langenau, Germany) and saline solution. The canal was dried with paper points and a bioceramic material (BiodentineTM) was prepared in accordance with the manufacturer’s instructions. It was smoothly carried into the canal and compacted apically with a hand barrierger (size #2, Buchanan Hand Plugger) to form an apical barrier of 5 mm in thickness. The excess of material from the walls was removed with paper points, a moist cotton pellet was added, and the access cavity was temporarily closed (CavitTM). Intraoperative and postoperative radiographs were taken to confirm the apical barrier position.
After 2 weeks, the patient developed spontaneous pain, swelling, and a sinus tract. At this time, the surgical endodontic treatment was proposed and explained to the patient and parents. After informed consent was obtained, the surgical procedure was performed by the same Endodontist who performed earlier the apical barrier. Anesthesia was achieved with 2% lidocaine with 1:80,000 epinephrine (Xylestesin
TM, 3M ESPE, Neuss, Germany), and an Ochsenbein Luebke flap was raised. Following flap retraction, the lesion was accessible and the granulation tissue was carefully removed by curettage. Approximately 2 mm of the root-end was resected with a surgical bur in an air impact high-speed handpiece. After root-end resection (~2 mm), the previous Biodentine barrier was inspected under magnification—nor voids nor chromogenic pigmentation or discoloration detected—as well as mechanically tested with a probe to evaluate its resistance and the lack of voids showing a well condensed barrier and for these reasons no retrograde root-end filling was done. The flap was repositioned and sutured (
Figure 3G). One week later, the patient returned with no signs or symptoms, and a resin-based composite (SDR
TM flow and Spectrum
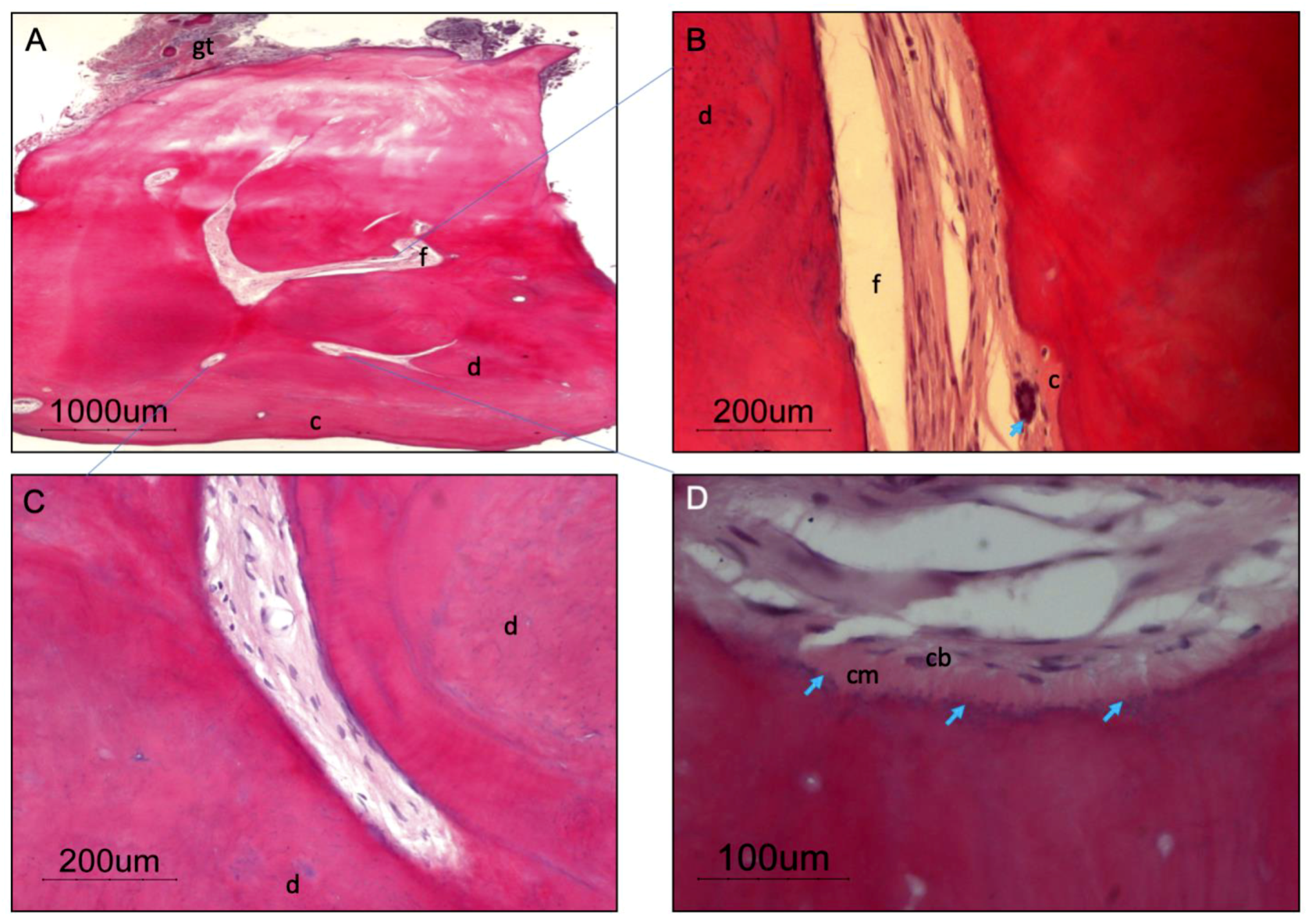
®) was placed into the root canal structure above the apical barrier all the way to the incisal edge. The resected apical root portion was processed for histologic evaluation. Histopathological assessment of the apical root fragment removed during the surgical root canal treatment was performed (
Figure 4). Staining with hematoxylin and eosin (H&E) depicts the presence of a root tip, with pulp tissue at the main foramen as well as small foramina, surrounded by dentin and cement. The presence of a giant multinucleated cell in the pulp tissue near the major foramen shall be emphasized. Granulation tissue was observed in and around the excised root tip.
A 5-year follow-up after endodontic surgery as well as clinical and radiographic (
Figure 3H) examination revealed almost complete apical healing and healthy soft tissues.
3. Discussion
The literature documenting follow-up of REPs teeth beyond 18 months is limited, and its long-term effects and full impact in a young patient remain unknown [
20]. In this case report, we show the follow up of two cases at 5 years and their respective radiographic and clinical success. Despite the loss of pulp vitality with the development of a chronic abscess in both presented clinical cases, a successful outcome with the resolution of the symptoms and tooth survival was achieved. As reported on a meta-analysis by Kahler et al. [
20], corroborated by Tong et al. [
21] and He et al. [
22], the periapical healing and tooth survival after REPs are excellent (above 90%), showing also that periapical pathology resolution after REPs was comparable with treatment with an apical barrier or apexification.
In case 1, the progressive and continuous apical root formation can be seen through the follow-up X-rays. This phenomenon might be explained by Hertwig’s sheath survival, retaining its ability to perform its role on root development and organization (when the inflammatory process was eliminated), and associated to SCAP survival (source of odontoblasts and thereafter can develop root dentin).
Trauma, infection, or iatrogenic factors can be responsible for apical papilla and HERS dislodgement from the main root walls [
18]. However, if these two structures stay largely uncompromised, they might continue their development independently of periapical pathology resolution [
15]. Case report 2 shows that after the first endodontic treatment (by the previous dentist), the apical fragment of the root was dislodged but continued its development separated from the main root even without the resolution of the apical periodontitis.
To the best of our knowledge, Sonoyama et al. [
7] were the first to demonstrate that the apical papilla was a reservoir for mesenchymal stem cells (SCAPs) fundamental for root development of immature teeth. It appears that SCAP has the inherent aptitude to survive and thrive in the hypoxic environment due to its niche normally being poorly vascularized, its nutrition relying on passive diffusion from the surrounding tissues [
17,
19,
23]. Indeed, periradicular granuloma is a highly vascularized granulomatous tissue and is likely to provide even a greater vascular bed than in normal and non-pathological states. From the same research, investigators affirmed that HERS cells are essential for controlling stem cell differentiation in a complement to cementum formation through a process of epithelial–mesenchymal transition in which cells undergo a developmental switch from a polarized epithelial phenotype to a greatly motile mesenchymal phenotype [
4]. In addition, it was described that
in vitro HERS can promote differentiation of periodontal ligaments stem cells into cementum forming cells [
24].
It has been described that the physiologic continuous root development of revascularized immature permanent necrotic teeth depends on whether the HERS survives or not in apical periodontitis as well as in abscess cases [
25]. Subsequently, unaffected HERS regulate the continuous root development due to apical cementum deposition after revascularization procedures. However, a normal dentin–pulp complex development requires not only the survival of HERS and ERM but also SCAP.
Previously, our research group [
18] showed that 79% of necrotic immature teeth with periapical lesions had histological resolution with an increase in root thickness and length (74%). Complete apical closure was observed in 42% and partial closure in 32%. These findings suggest that SCAPS and HERS cells remain vital in continuity or close to the main root after infection. The present work supports these data with the clinical observation that even in larger periapical lesions, SCAP, HERS, and ERM are more resilient than expected, surviving to clinical adverse conditions and continue their development, as shown by the root tip growth in the clinical case 1. In the follow-up plain radiographs as well as the CBCT scan, a substantial increase in root thickness and length can be appreciated with a root tip development in which, in the beginning, one side is partially detached from the main root. These radiographic findings are supported by our results that note the almost constant presence of an associated, sometimes totally or partially detached, periapical radiopacity, surrounded by a well-defined periodontal ligament space, suggestive of a newly developed root tip. To our knowledge, only a few reports [
26,
27] about the histology of the newly formed root have been conducted in detail. Gibson et al. [
26] reported the presence of disturbed dentinogenesis and the formation beginning stages of pulp stone formation after a traumatic avulsion of an immature permanent incisor, while studies conducted by Yang et al. [
27] revealed that the detached root fragments had a normal histological root structure, although no previous studies showed the survival of the apical papilla and HERS cells (or ERM). In spite of the absence of signs and symptoms, the provided clinical evidence of pulp regeneration and the radiographic and CBCT findings were consistent with continued root formation, and the tooth remained unresponsive to pulp sensitivity tests. This was probably because of the distance between the crown and the pulp tissue, which was most likely confined to the apical portion of the tooth.
Concerning the late-stage drawbacks from the REPs, such as undesirable discoloration, pulp canal obliteration, atypical root morphology development, and loss of vitality after apical closure, the available literature is sparse. From the Tong et al. meta-analysis [
21], tooth discoloration after REPs treatment was reported in 50% of studies, when minocycline as intracanal medication (known to cause tooth discoloration) as well as grey MTA (bismuth oxide content in MTA has also been associated with coronal discoloration) were used [
28]. In both clinical cases, the clinicians decided to use calcium hydroxide as intracanal medication, since calcium hydroxide has a lower risk of later discoloration in comparation to the antibiotic paste [
29]. Several studies showed that MTA presents even greater color change after contact with blood [
28,
30,
31]. However, it should be kept in mind that during REPs, MTA is placed over the blood clot on the cervical third of the root, just below the CEJ, increasing the potential for discoloration. In the first case report, where REP was performed, even though there is no discoloration at the 5-year follow-up, a higher risk of discoloration is still possible to occur in a longer-term follow-up.
The literature also points out that the risk of intracanal calcification after REPs was higher in cases medicated with calcium hydroxide (76.9%) compared with teeth medicated with antibiotic pastes (46.2%) [
32] Altai et al. [
33] in a comprehensive review highlighted that all the studies that used MTA directly on blood clot or on other scaffolds showed intracanal calcification. Correspondingly, other case reports have shown the formation of hard tissue bridges under MTA, and scattered calcification inside the canal, when some portion of the MTA was pushed into the canal. However, our data from case report 1, after five years of follow-up, where calcium hydroxide was used as intracanal medication, show that the root canal is still discernible at the X-ray, which allows being confident that revascularization-associated intracanal calcification did not occur.
The ESE position statement about revitalization procedures advises the use of 1.5–3% sodium hypochlorite [
1]. The choice of 3% sodium hypochlorite concentration reflects the need for adequate disinfection and at the same time the preservation of the apical tissues, allowing the further development of the root depicting the success of the clinical procedure in case report 1.
In clinical case 2, an apexification procedure with an apical barrier of Biodentine was the treatment of choice due to the presence of wide root canal and open apex (blunderbuss) [
34]. It should be emphasized that in the most recent ESE guidelines, irrigation with EDTA is advised when an apical barrier is placed. Despite this, EDTA irrigation was not performed when performing case report 2 as the irrigation of EDTA did not seem like it would impact the outcome of treatment. However, it is known that Biodentine has significant potential to stimulate TGF-b1 release from the root dentin with similar effects to the irrigation with EDTA [
35]. These high levels of TGF-b1 were explained by alkaline property (high pH levels of Biodentine) on solubilize of dentin matrix. We should stress that even after the apical barrier placement, there were no signs of periapical healing—pain, swelling, as well as a fistula were present after 2 weeks of the apical barrier. The persistence of apical infection might be explained by the presence of an extraradicular biofilm—as shown by the histologic slides after the apical surgery—which was not removed by the intrarradicular disinfection procedures [
19]. As reported by Siqueira et al. [
36], biofilms that adhered to the apical root surface (extraradicular biofilms) have been a possible cause of post-treatment apical periodontitis.
Furthermore, our findings provide evidence that in clinical case 2, the mineralized structures observed radiographically had histologic features of a root tip—composed by cellular cementum, periodontal ligament, dentin, predentin with an intact odontoblastic layer, and, in some cases, the presence of apical foramen were also seen. Thus, according to our findings, it is reasonable to suggest that even when partially or completely detached from the main root, the apical papilla associated with HERS preserves their potential of continuing root development [
18]. These findings confirm the results observed in a study by Yang et al. [
27] that the separation of the soft tissues from mineralized tissues and their development as an independent root tip was associated with HERS injure and its following detachment caused by the apexification procedure.

 ,
, 









{kind=link}
{kind=link}
{kind=link}
{kind=link}