Mindfulness, Interoception, and Olfaction: A Network Approach


 , and
, and
Abstract
:
1. Introduction
2. Material and Methods
2.1. Participants and Design
2.2. Measures
2.3. Data Analysis
3. Results
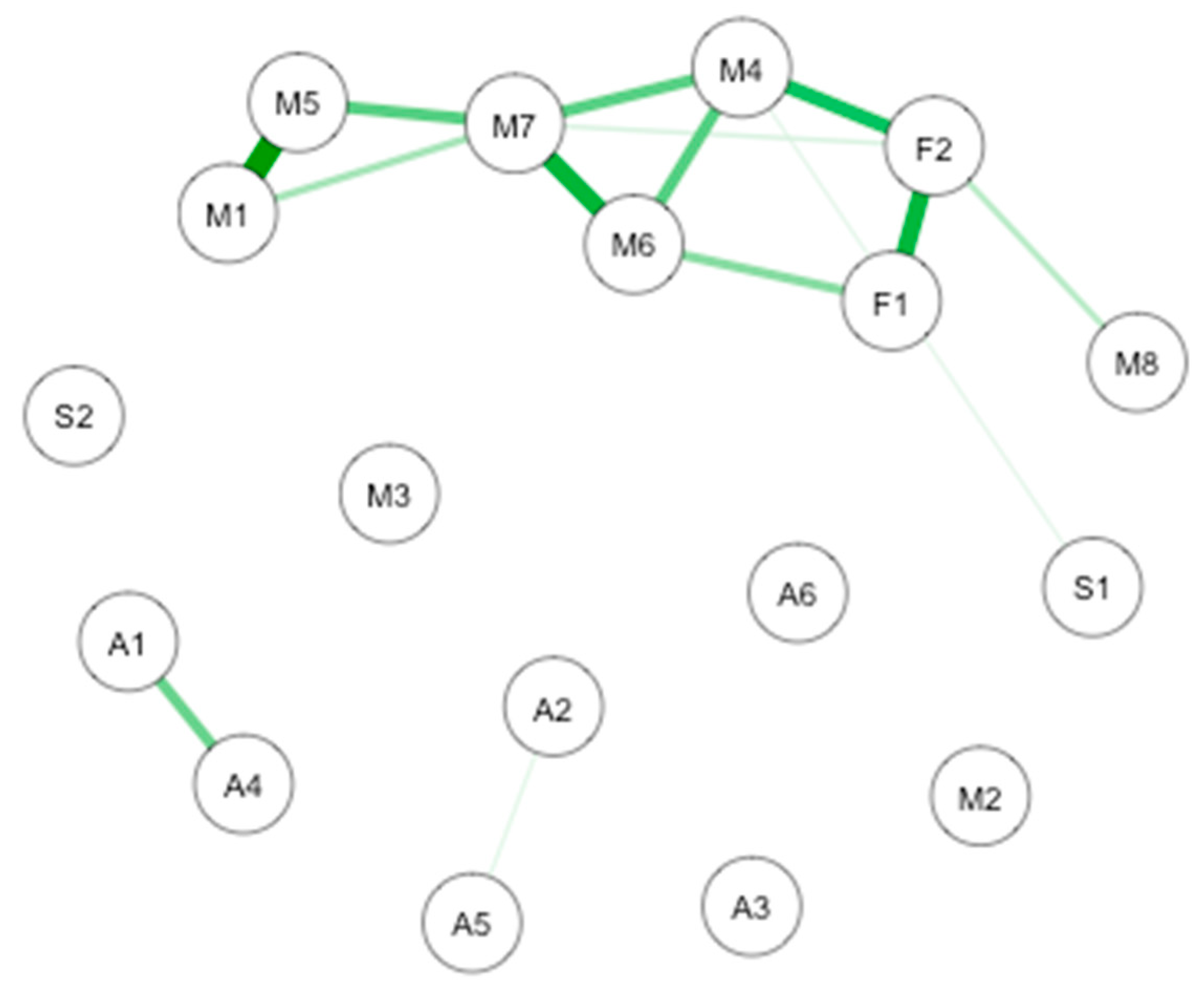
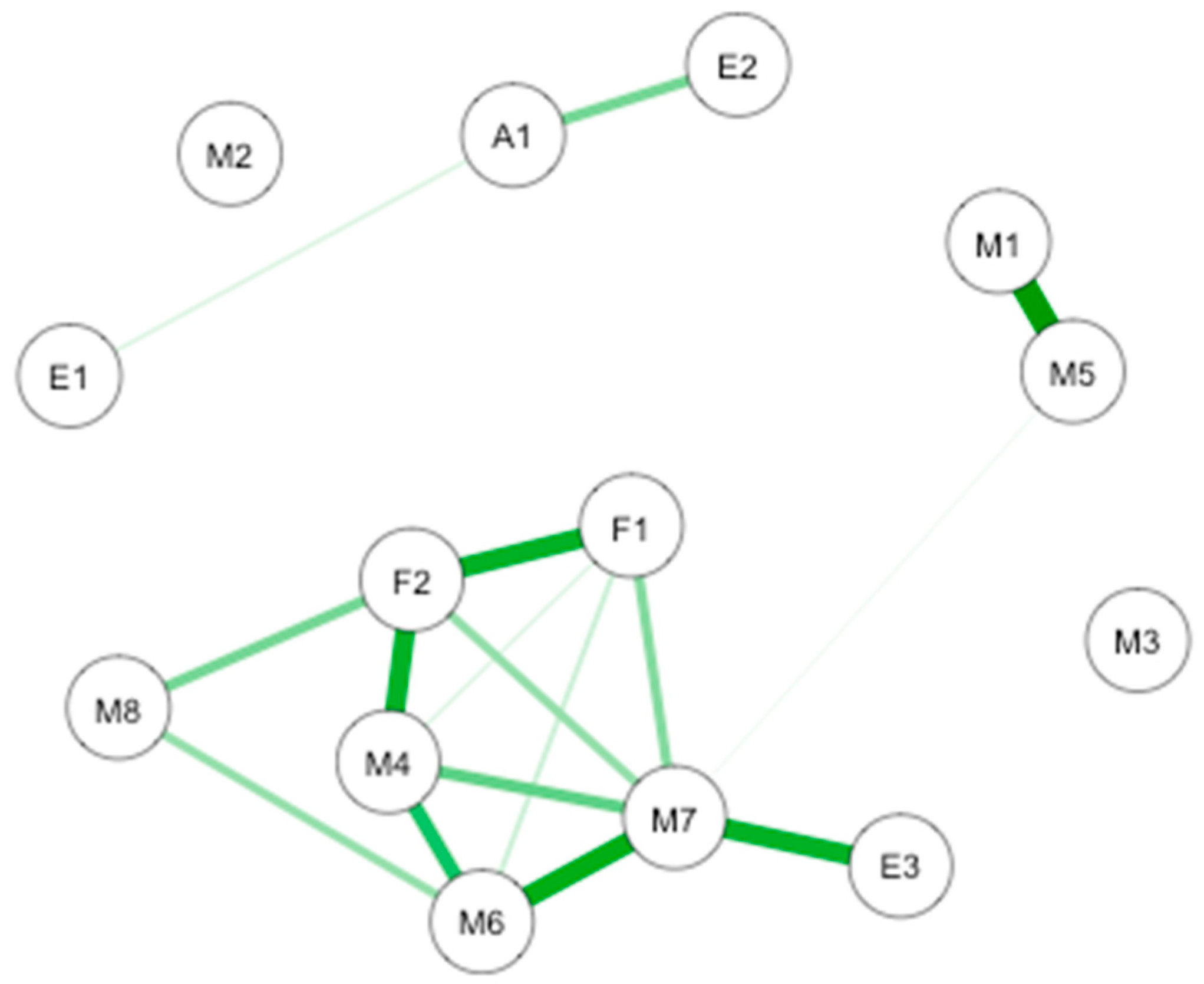
3.1. Causal Interaction Network between Interoception, Emotions, and Subjective Olfactory Acuity
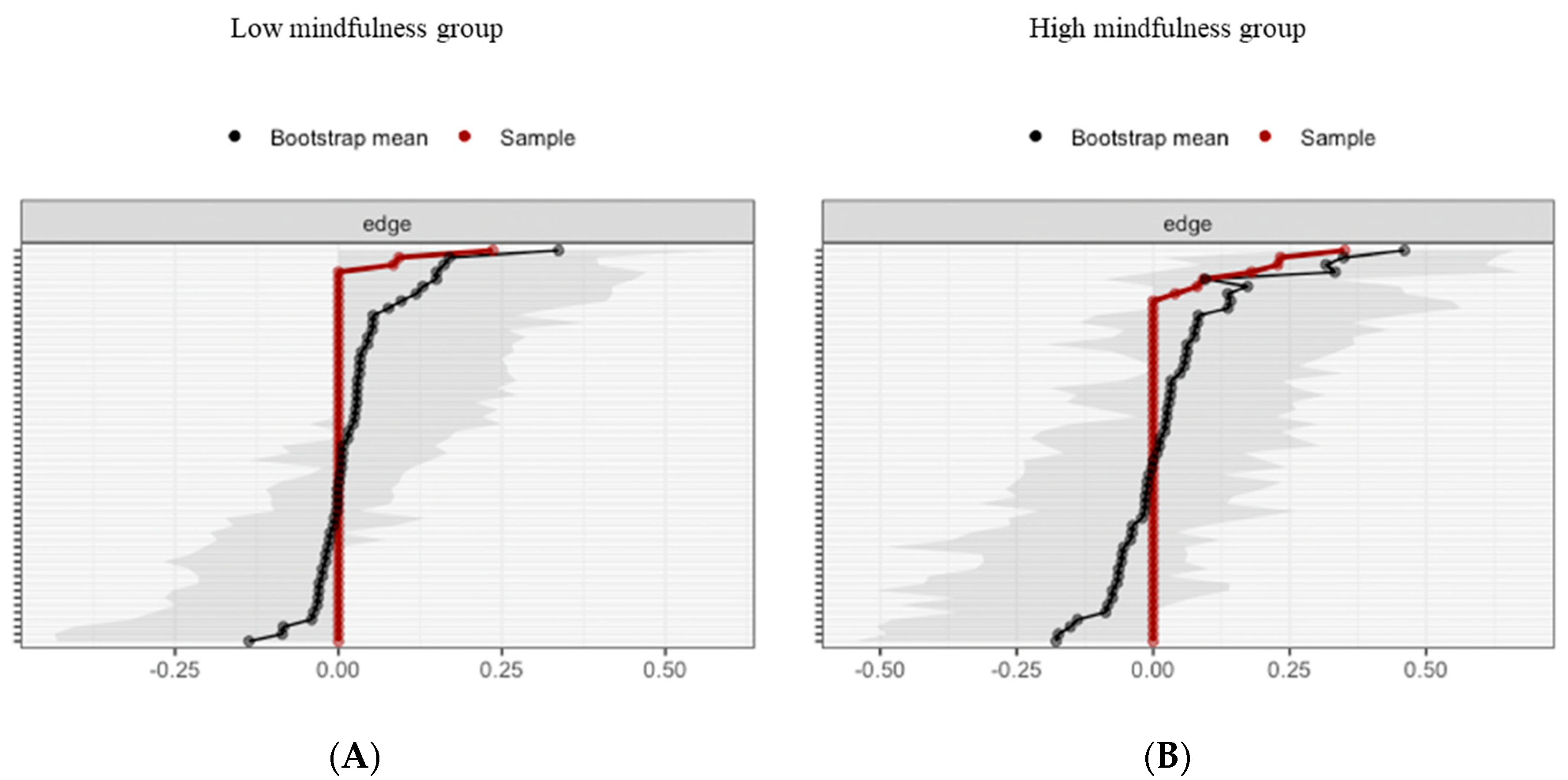
3.2. Impact of MD Clustering on Psychological Assessments
3.3. Impact of MD Clustering on Olfactory Sensitivity Assessments
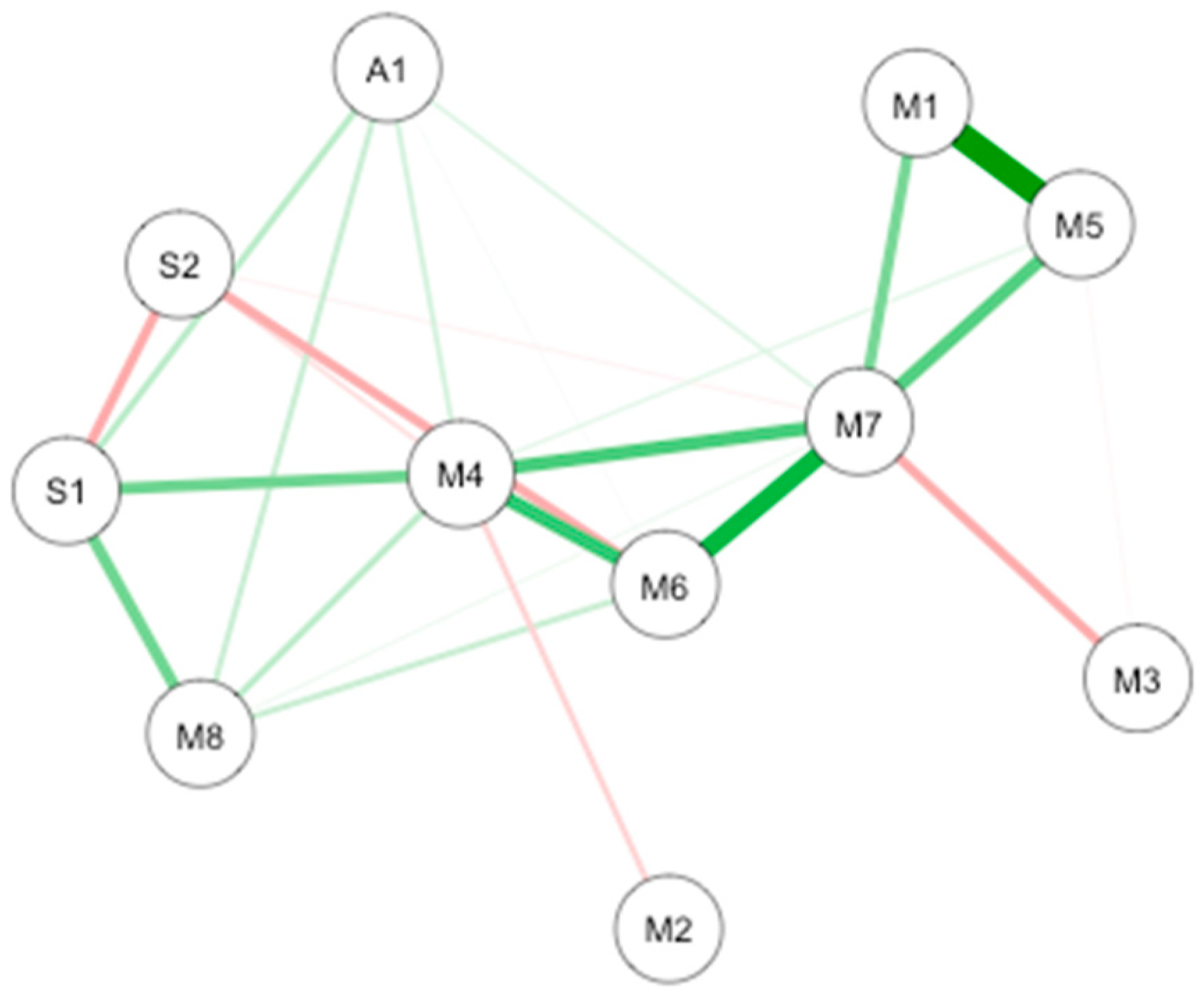
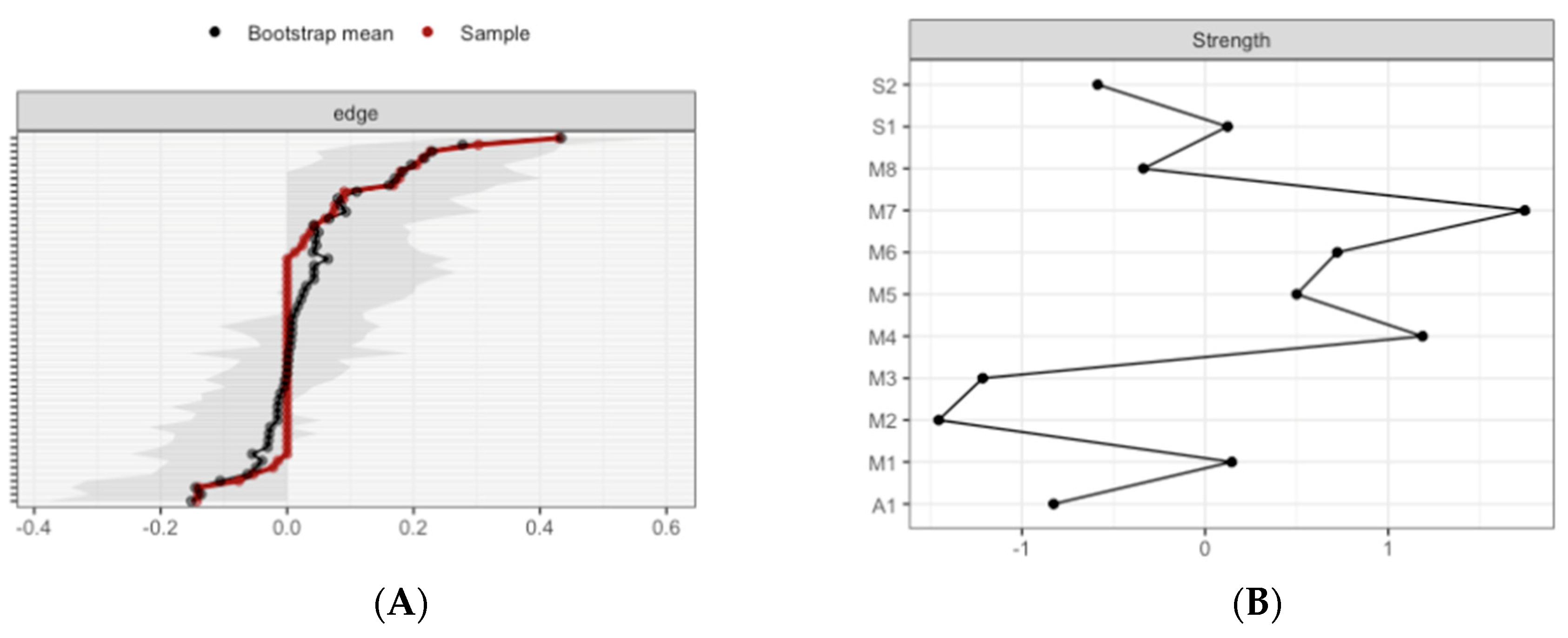
3.4. Causal Interaction Network Using Objective and Subjective Olfaction Data
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Craig, A.D. How do you feel? Interoception: The sense of the physiological condition of the body. Nat. Rev. Neurosci. 2002, 3, 655–666. [Google Scholar] [CrossRef] [PubMed]
- Mehling, W.E.; Gopisetty, V.; Daubenmier, J.; Price, C.J.; Hecht, F.M.; Stewart, A. Body awareness: Construct and self-report measures. PLoS ONE 2009, 4, e5614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehling, W.E.; Price, C.; Daubenmier, J.J.; Acree, M.; Bartmess, E.; Stewart, A. The Multidimensional Assessment of Interoceptive Awareness (MAIA). PLoS ONE 2012, 7, e48230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Treves, I.N.; Tello, L.Y.; Davidson, R.J.; Goldberg, S. The relationship between mindfulness and objective measures of body awareness: A meta-analysis. Sci. Rep. 2019, 9, 17386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baas, L.S.; Beery, T.A.; Allen, G.; Wizer, M.; Wagoner, L.E. An exploratory study of body awareness in persons with heart failure treated medically or with transplantation. J. Cardiovasc. Nurs. 2004, 19, 32–40. [Google Scholar] [CrossRef]
- Christensen, A.J.; Wiebe, J.S.; Edwards, D.L.; Michels, J.D.; Lawton, W. Body consciousness, illness-related impairment, and patient adherence in hemodialysis. J. Consult. Clin. Psychol. 1996, 64, 147–152. [Google Scholar] [CrossRef]
- Eriksson, E.M.; Möller, I.E.; Söderberg, R.H.; Eriksson, H.T.; Kurlberg, G.K. Body awareness therapy: A new strategy for relief of symptoms in irritable bowel syndrome patients. World J. Gastroenterol. 2007, 13, 3206–3214. [Google Scholar] [CrossRef]
- Danielsson, L.; Rosberg, S. Opening toward life: Experiences of basic body awareness therapy in persons with major depression. Int. J. Qual. Stud. Health Well Being 2015, 10, 27069. [Google Scholar] [CrossRef]
- Gyllensten, A.L.; Hansson, L.; Ekdahl, C. Outcome of basic body awareness therapy. A randomized controlled study of patients in psychiatric outpatient care. Adv. Physiother. 2003, 5, 179–190. [Google Scholar] [CrossRef]
- Afrell, M.; Biguet, G.; Rudebeck, C.E. Living with a body in pain—between acceptance and denial. Scand. J. Caring Sci. 2007, 21, 291–296. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Wherever You Go, There You Are: Mindfulness Meditation in Everyday Life; Hyperion: New York, NY, USA, 1994. [Google Scholar]
- Lutz, A.; Jha, A.P.; Dunne, J.D.; Saron, C.D. Investigating the phenomenological matrix of mindfulness-related practices from a neurocognitive perspective. Am. Psychol. 2015, 70, 632–658. [Google Scholar] [CrossRef] [PubMed]
- Kilpatrick, L.A.; Suyenobu, B.Y.; Smith, S.R.; Bueller, J.A.; Goodman, T.; Creswell, J.D.; Tillisch, K.; Mayer, E.A.; Naliboff, B.D. Impact of Mindfulness-Based Stress Reduction training on intrinsic brain connectivity. NeuroImage 2011, 56, 290–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, K.W.; Ryan, R.M. The benefits of being present: Mindfulness and its role in psychological well-being. J. Personal. Soc. Psychol. 2003, 84, 822–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giluk, T.L. Mindfulness, Big Five personality, and affect: A meta-analysis. Personal. Individ. Differ. 2009, 47, 805–811. [Google Scholar] [CrossRef]
- Chamberlain, D.; Williams, A.; Stanley, D.; Mellor, P.; Cross, W.; Siegloff, L. Dispositional mindfulness and employment status as predictors of resilience in third year nursing students: A quantitative study. Nurs. Open 2016, 3, 212–221. [Google Scholar] [CrossRef] [Green Version]
- Verdonk, C.; Trousselard, M.; Canini, F.; Vialatte, F.; Ramdani, C. Toward a Refined Mindfulness Model Related to Consciousness and Based on Event-Related Potentials. Perspect. Psychol. Sci. A J. Assoc. Psychol. Sci. 2020, 15, 1095–1112. [Google Scholar] [CrossRef] [PubMed]
- Prakash, R.S.; Hussain, M.A.; Schirda, B. The role of emotion regulation and cognitive control in the association between mindfulness disposition and stress. Psychol. Aging 2015, 30, 160–171. [Google Scholar] [CrossRef] [Green Version]
- Leigh, J.; Bowen, S.; Marlatt, G.A. Spirituality, mindfulness and substance abuse. Addict. Behav. 2005, 30, 1335–1341. [Google Scholar] [CrossRef]
- Bornemann, B.; Herbert, B.M.; Mehling, W.E.; Singer, T. Differential changes in self-reported aspects of interoceptive awareness through 3 months of contemplative training. Front. Psychol. 2015, 5, 1504. [Google Scholar] [CrossRef] [Green Version]
- Carmody, J.; Baer, R.A. Relationships between mindfulness practice and levels of mindfulness, medical and psychological symptoms and well-being in a mindfulness-based stress reduction program. J. Behav. Med. 2008, 31, 23–33. [Google Scholar] [CrossRef]
- Farb, N.; Daubenmier, J.; Price, C.J.; Gard, T.; Kerr, C.; Dunn, B.D.; Klein, A.C.; Paulus, M.P.; Mehling, W.E. Interoception, contemplative practice, and health. Front. Psychol. 2015, 6, 763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanley, A.W.; Mehling, W.E.; Garland, E.L. Holding the body in mind: Interoceptive awareness, dispositional mindfulness and psychological well-being. J. Psychosom. Res. 2017, 99, 13–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalsa, S.S.; Rudrauf, D.; Damasio, A.R.; Davidson, R.J.; Lutz, A.; Tranel, D. Interoceptive awareness in experienced meditators. Psychophysiology 2008, 45, 671–677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalsa, S.S.; Rudrauf, D.; Hassanpour, M.S.; Davidson, R.J.; Tranel, D. The practice of meditation is not associated with improved interoceptive awareness of the heartbeat. Psychophysiology 2020, 57, e13479. [Google Scholar] [CrossRef]
- Melloni, M.; Sedeño, L.; Couto, B.; Reynoso, M.; Gelormini, C.; Favaloro, R.; Canales-Johnson, A.; Sigman, M.; Manes, F.; Ibanez, A. Preliminary evidence about the effects of meditation on interoceptive sensitivity and social cognition. Behav. Brain Funct. BBF 2013, 9, 47. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, L.; Kaszniak, A.W. Awareness of subtle emotional feelings: A comparison of long-term meditators and nonmeditators. Emotion 2006, 6, 392–405. [Google Scholar] [CrossRef] [Green Version]
- Otten, S.; Schötz, E.; Wittmann, M.; Kohls, N.; Schmidt, S.; Meissner, K. Psychophysiology of duration estimation in experienced mindfulness meditators and matched controls. Front. Psychol. 2015, 6, 1215. [Google Scholar] [CrossRef] [Green Version]
- Parkin, L.; Morgan, R.; Rosselli, A.; Howard, M.; Sheppard, A.; Evans, D.; Hawkins, A.; Martinelli, M.; Golden, A.M.; Dalgleish, T.; et al. Exploring the Relationship Between Mindfulness and Cardiac Perception. Mindfulness 2014, 5, 298–313. [Google Scholar] [CrossRef]
- Schwoebel, J.; Friedman, R.; Duda, N.; Coslett, H.B. Pain and the body schema: Evidence for peripheral effects on mental representations of movement. Brain 2001, 124 Pt 10, 2098–2104. [Google Scholar] [CrossRef] [Green Version]
- Schwoebel, J.; Coslett, H.B.; Bradt, J.; Friedman, R.; Dileo, C. Pain and the body schema: Effects of pain severity on mental representations of movement. Neurology 2002, 59, 775–777. [Google Scholar] [CrossRef]
- Bray, H.; Moseley, G.L. Disrupted working body schema of the trunk in people with back pain. Br. J. Sports Med. 2011, 45, 168–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valenzuela-Moguillansky, C.; Reyes-Reyes, A.; Gaete, M.I. Exteroceptive and Interoceptive Body-Self Awareness in Fibromyalgia Patients. Front. Hum. Neurosci. 2017, 11, 117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harshaw, C. Interoceptive dysfunction: Toward an integrated framework for understanding somatic and affective disturbance in depression. Psychol. Bull. 2015, 141, 311–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, K.; Garfinkel, S.N.; Critchley, H.D.; Seth, A.K. Multisensory integration across exteroceptive and interoceptive domains modulates self-experience in the rubber-hand illusion. Neuropsychologia 2013, 51, 2909–2917. [Google Scholar] [CrossRef] [Green Version]
- Koeppel, C.J.; Ruser, P.; Kitzler, H.; Hummel, T.; Croy, I. Interoceptive accuracy and its impact on neuronal responses to olfactory stimulation in the insular cortex. Hum. Brain Mapp. 2020, 41, 2898–2908. [Google Scholar] [CrossRef]
- Mazzola, L.; Royet, J.P.; Catenoix, H.; Montavont, A.; Isnard, J.; Mauguiere, F. Gustatory and olfactory responses to stimulation of the human insula. Ann. Neurol. 2017, 82, 360–370. [Google Scholar] [CrossRef]
- Krajnik, J.; Kollndorfer, K.; Notter, L.A.; Mueller, C.A.; Schopf, V. The impact of olfactory dysfunction on interoceptive awareness. Psychophysiology 2015, 52, 263–268. [Google Scholar] [CrossRef]
- Kremer, S.; Holthuysen, N.; Boesveldt, S. The influence of olfactory impairment in vital, independently living older persons on their eathing behaviour and food liking. Food Qual. Prefer. 2014, 38, 30–39. [Google Scholar] [CrossRef]
- Willander, J.; Larsson, M. Olfaction and emotion: The case of autobiographical memory. Mem. Cogn. 2007, 35, 1659–1663. [Google Scholar] [CrossRef] [Green Version]
- Sergeant, M.T.; Davies, M.O.; Dickins, T.E.; Griffiths, M.D. The self-reported importance of olfactions during human mate choice. Sex. Evol. Gend. 2005, 7, 199–213. [Google Scholar] [CrossRef] [Green Version]
- Weir, K. Scents and sensibility. Monit. Psychol. 2011, 42, 40. [Google Scholar]
- Stevenson, R.J. Olfactory perception, cognition, and dysfunction in humans. Wires Cogn. Sci. 2013, 4, 273–284. [Google Scholar] [CrossRef] [PubMed]
- Pacharra, M.; Schäper, M.; Kleinbeck, S.; Blaszkewicz, M.; Wolf, O.T.; van Thriel, C. Stress lowers the detection threshold for foul-smelling 2-mercaptoethanol. Stress 2016, 19, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Deems, D.A.; Doty, R.L.; Settle, R.G.; Moore-Gillon, V.; Shaman, P.; Mester, A.F.; Kimmelman, C.P.; Brightman, V.J.; Snow, J.B., Jr. Smell and taste disorders, a study of 750 patients from the University of Pennsylvania Smell and Taste Center. Arch. Otolaryngol. Head Neck Surg. 1991, 117, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Henry, C.; Dargél, A.A. What can we learn about mood disorders from olfactory processes? Bipolar Disord. 2018, 20, 562–563. [Google Scholar] [CrossRef] [PubMed]
- Meek, C.; Heckerman, D. Structure and Parameter Learning for Causal Independence and Causal Interaction Models. arXiv 2013, arXiv:1302.1561. [Google Scholar]
- Borsboom, D. A network theory of mental disorders. World Psychiatry 2017, 16, 5–13. [Google Scholar] [CrossRef] [Green Version]
- Walach, H.; Buchheld, N.; Buttenmüller, V.; Kleinknecht, N.; Schmidt, S. Measuring mindfulness-the Freiburg Mindfulness Inventory (FMI). Personal. Individ. Differ. 2006, 40, 1543–1555. [Google Scholar] [CrossRef]
- Trousselard, M.; Steiler, D.; Raphel, C.; Cian, C.; Duymedjian, R.; Claverie, D.; Canini, F. Validation of a french version of the Freiburg Mindfulness Inventory-short version: How mindfulness deals with the stress in a working middle-aged population. Biopsychosoc. Med. 2010, 4, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Diener, E.; Wirtz, D.; Tov, W.; Prieto, C.K.; Choi, D.; Oishi, S.; Biswas-Diener, R. New Well-being Measures: Short Scales to Assess Flourishing and Positive and Negative Feelings. Soc. Indic. Res. 2010, 97, 143–156. [Google Scholar] [CrossRef]
- Martin-Krumm, C.; Fenouillet, F.; Csillik, A.; Kern, L.; Besancon, M.; Heutte, J.; Paquet, Y.; Delas, Y.; Trousselard, M.; Lecorre, B.; et al. Changes in Emotions from Childhood to Young Adulthood. Child Indic. Res. 2017, 11, 541–561. [Google Scholar] [CrossRef]
- Kacha, S.; Guillemin, F.; Jankowski, R. Development and validity of the DyNaChron questionnaire for chronic nasal dysfunction. Eur. Arch. Oto Rhino Laryngol. 2012, 269, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Thomas-Danguin, T.; Rouby, C.; Sicard, G.; Vigouroux, M.; Farget, V.; Johanson, A.; Bengtzon, A.; Hall, G.; Ormel, W.; De Graaf, C.; et al. Development of the ETOC: A European test of olfactory capabilities. Rhinology 2003, 41, 142–151. [Google Scholar] [PubMed]
- Epskamp, S.; Borsboom, D.; Fried, E.I. Estimating psychological networks and their accuracy: A tutorial paper. Behav. Res. Methods 2018, 50, 195–212. [Google Scholar] [CrossRef] [Green Version]
- Mehling, W.E.; Acree, M.; Stewart, A.; Silas, J.; Jones, A. The Multidimensional Assessment of Interoceptive Awareness, Version 2 (MAIA-2). PLoS ONE 2018, 13, e0208034. [Google Scholar] [CrossRef] [Green Version]
- Guendelman, S.; Medeiros, S.; Rampes, H. Mindfulness and Emotion Regulation: Insights from Neurobiological, Psychological, and Clinical Studies. Front. Psychol. 2017, 8, 220. [Google Scholar] [CrossRef]
- Price, C.J.; Hooven, C. Interoceptive Awareness Skills for Emotion Regulation: Theory and Approach of Mindful Awareness in Body-Oriented Therapy (MABT). Front. Psychol. 2018, 9, 798. [Google Scholar] [CrossRef] [Green Version]
- Boucher, O.; Citherlet, D.; Ghaziri, J.; Hébert-Seropian, B.; Von Siebenthal, Z.; Nguyen, D. Insula: Neuropsychology of the fifth lobe of the brain. Rev. Neuropsychol. 2017, 9, 154–161. [Google Scholar] [CrossRef]
- Jang, J.H.; Kim, J.-H.; Yun, J.-Y.; Choi, S.-H.; An, S.C.; Kang, D.-H. Differences in Functional Connectivity of the Insula Between Brain Wave Vibration in Meditators and Non-meditators. Mindfulness 2018, 9, 1857–1866. [Google Scholar] [CrossRef] [Green Version]
- Shinder, M.E.; Newlands, S.D. Sensory convergence in the parieto-insular vestibular cortex. J. Neurophysiol. 2014, 111, 2445–2464. [Google Scholar] [CrossRef] [Green Version]
- Soudry, Y.; Lemogne, C.; Malinvaud, D.; Consoli, S.M.; Bonfils, P. Olfactory system and emotion: Common substrates. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2011, 128, 18–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toet, A.; Eijsman, S.; Liu, Y.; Donker, S.; Kaneko, D.; Brouwer, A.-M.; van Erp, J.B.F. The Relation between Valence and Arousal in Subjective Odor Experience. Chem. Percept. 2020, 13, 141–151. [Google Scholar] [CrossRef]
- Leveton, L.; Shea, C.; Slack, K.J.; Keeton, K.E.; Palinkas, L.A. Antarctica Meta-Analysis: Psychosocial Factors Related to Long Duration Isolation and Confinement. Available online: https://ntrs.nasa.gov/citations/20090007551 (accessed on 15 October 2020).
- Liu, Q.; Zhou, R.-L.; Zhao, X.; Chen, X.-P.; Chen, S.-G. Acclimation during space flight: Effects on human emotion. Mil. Med. Res. 2016, 3, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MD Cluster on All Participants (n = 76) | MD Cluster on ETOC Subsample (n = 31) | ||||
|---|---|---|---|---|---|
| Sociodemographic Data | High MD | Low MD | High MD | Low MD | p-Value * |
| N | 32 | 44 | 18 | 13 | |
| Age | 27 ± 5.59 | 30 ± 10.27 | 25 ± 4.91 | 30 ± 10.15 | 0.56 |
| Woman/man | 4/28 | 8/36 | 2/16 | 0/13 | 0.38 |
| Submariners | 17 | 11 | 8 | 6 | |
| Marines | 8 | 4 | 8 | 3 | |
| Overwinterers | 7 | 29 | 2 | 4 | |
| Variables | High MD | Low MD | p-Value * |
|---|---|---|---|
| SPANE Positive | 4.22 ± 0.47 | 3.94 ± 0.54 | 0.01 |
| SPANE negative | 2.43 ± 0.64 | 2.13 ± 0.54 | 0.02 |
| MAIA not distracting | 2.64 ± 0.76 | 2.96 ± 0.75 | 0.06 |
| MAIA attention regulation | 3.37 ± 0.68 | 2.51 ± 0.76 | 0.000 |
| MAIA self-regulation | 3.22 ± 0.79 | 2.48 ± 0.84 | 0.000 |
| MAIA body listening | 2.66 ± 1.18 | 1.93 ± 0.88 | 0.006 |
| MAIA trusting | 4.38 ± 0.59 | 3.55 ± 1.04 | 0.000 |
| Subjective olfactory acuity | 7.69 ± 1.97 | 6.27 ± 2.40 | 0.008 |
| Subjective taste acuity | 8.06 ± 1.79 | 7.70 ± 2.21 | 0.02 |
| Subjective hearing acuity | 8.97 ± 1.12 | 7.59 ± 2.17 | 0.005 |
| Subjective acuity of balance | 8.19 ± 1.45 | 7.11 ± 2.32 | 0.02 |
| Subjective visual acuity | 9.28 ± 0.92 | 8.59 ± 1.77 | 0.08 |
| Variables | High MD | Low MD | p-Value * |
|---|---|---|---|
| ETOC identification | 12.6 ± 1.50 | 11.3 ± 2.06 | 0.106 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lefranc, B.; Martin-Krumm, C.; Aufauvre-Poupon, C.; Berthail, B.; Trousselard, M. Mindfulness, Interoception, and Olfaction: A Network Approach. Brain Sci. 2020, 10, 921. https://doi.org/10.3390/brainsci10120921
Lefranc B, Martin-Krumm C, Aufauvre-Poupon C, Berthail B, Trousselard M. Mindfulness, Interoception, and Olfaction: A Network Approach. Brain Sciences. 2020; 10(12):921. https://doi.org/10.3390/brainsci10120921
Chicago/Turabian StyleLefranc, Barbara, Charles Martin-Krumm, Charlotte Aufauvre-Poupon, Benoit Berthail, and Marion Trousselard. 2020. "Mindfulness, Interoception, and Olfaction: A Network Approach" Brain Sciences 10, no. 12: 921. https://doi.org/10.3390/brainsci10120921
APA StyleLefranc, B., Martin-Krumm, C., Aufauvre-Poupon, C., Berthail, B., & Trousselard, M. (2020). Mindfulness, Interoception, and Olfaction: A Network Approach. Brain Sciences, 10(12), 921. https://doi.org/10.3390/brainsci10120921