
Effects of the SGLT2 Inhibition on Cardiac Remodeling in Streptozotocin-Induced Diabetic Rats, a Model of Type 1 Diabetes Mellitus

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Groups
2.2. Echocardiographic Study
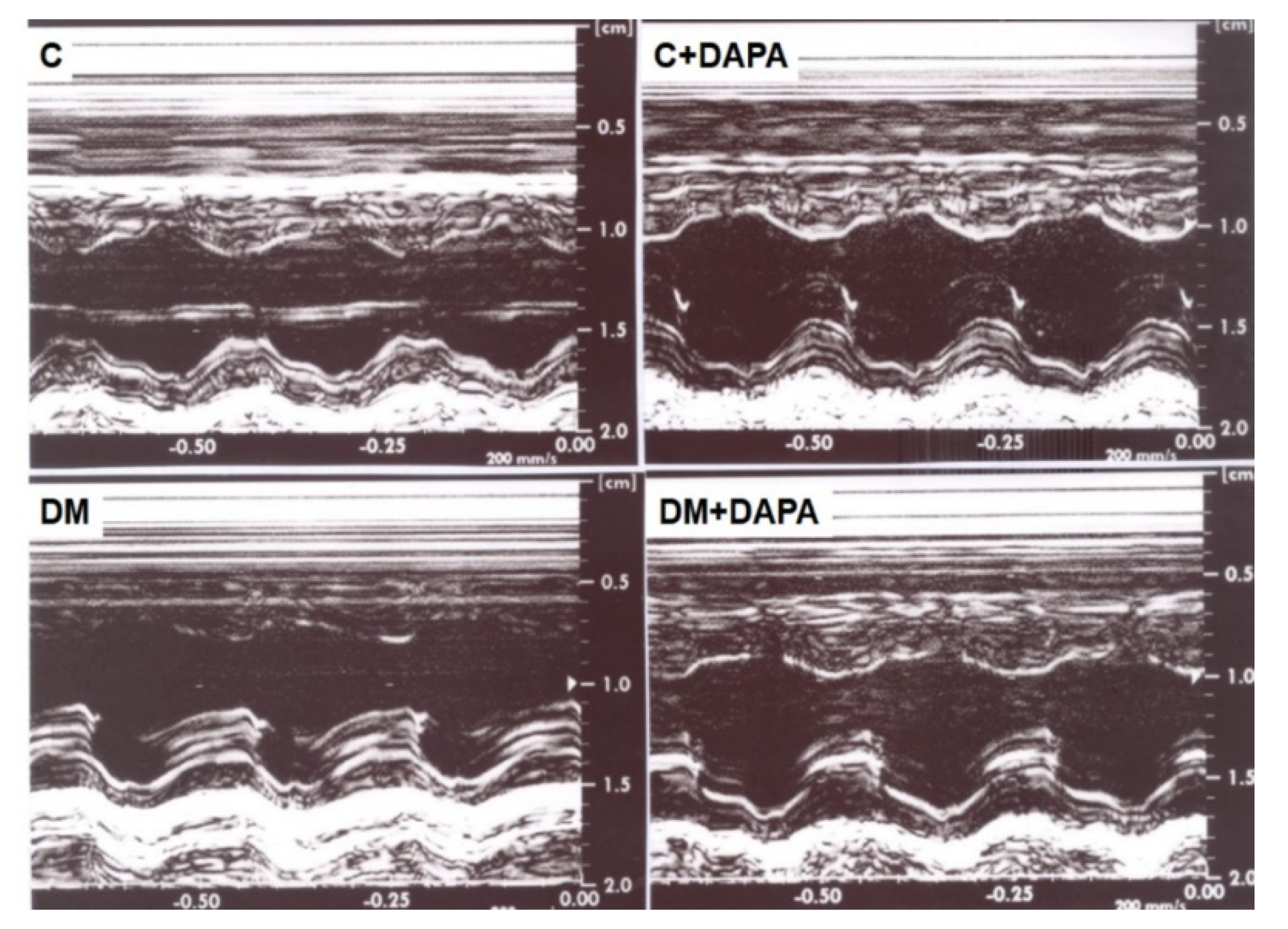
2.2.1. M-Mode
2.2.2. Tissue Doppler Imaging
2.3. Histological Analysis
2.4. Myocardial Hydroxyproline Concentration
2.5. Western Blotting
2.6. Myocardial Oxidative Stress
2.7. Advanced Glycation End Products
2.8. Statistical Analyzes
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| A-wave | late diastolic mitral flow velocity |
| AGE | advanced glycation end products |
| ANOVA | analysis of variance |
| AO | aorta diameter |
| C | control group |
| C + DAPA | control group treated with dapagloflozin |
| DAB | 3,3′-diaminobenzidine |
| DM | diabetes mellitus |
| DM + DAPA | diabetes mellitus group treated with dapagloflozin |
| E-wave | early diastolic mitral flow velocity |
| E/A | ratio |
| E/E’ | ratio |
| EDT | E-wave deceleration time |
| EDTA | ethylenediamine tetraacetic acid |
| EFS | endocardial fraction shortening |
| GSH-Px | glutathione peroxidase |
| HOP | hydroxyproline |
| H2O2 | Hydrogen peroxide |
| IVRT | isovolumetric relation time |
| LA | left atrium |
| LV | left ventricle |
| LVDD | left ventricle diastolic dimensions |
| LVPWT | left ventricle posterior wall thickness |
| LVM | left ventricle mass |
| LVSWT | left ventricle septal wall thickness |
| LVSD | left ventricle sistolic dimensions |
| NADH | nicotinamida adenina dinucleotídeo |
| PWSV | posterior wall shortening velocity |
| RWT | left ventricle relative wall thickness |
| SGLT2 | sodium-glucose co-transporter 2 |
| SOD | superoxide dismutase |
| TDI | tissue Doppler imaging |
| TDI-A’ | tissue Doppler imaging of mitral annular late velocity (lateral, septal and average) |
| TDI-E’ | tissue Doppler imaging of mitral annular early velocity (lateral, septal and average) |
| TDI-S’ | tissue Doppler imaging for systolic velocity of the mitral annulus (lateral, septal and average) |
| Tei index | myocardial performance index |
References
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; Boehme, A.K.; Buxton, A.E.; Carson, A.P.; Commodore-Mensah, Y.; et al. American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics-2022 Update: A report from the American Heart Association. Circulation 2022, 145, e153–e639. [Google Scholar]
- Maack, C.; Lehrke, M.; Backs, J.; Heinzel, F.R.; Hulot, J.-S.; Marx, N.; Paulus, W.J.; Rossignol, P.; Taegtmeyer, H.; Bauersachs, J.; et al. Heart failure and diabetes: Metabolic alterations and therapeutic interventions: A state-of-the-art review from the Translational Research Committee of the Heart Failure Association—European Society of Cardiology. Eur. Heart J. 2018, 39, 4243–4254. [Google Scholar]
- Dillmann, W.H. Diabetic cardiomyopathy. Circ. Res. 2019, 124, 1160–1162. [Google Scholar]
- El Hayek, M.S.; Ernande, L.; Benitah, J.-P.; Gomez, A.-M.; Pereira, L. The role of hyperglycaemia in the development of diabetic cardiomyopathy. Arch. Cardiovasc. Dis. 2021, 114, 748–760. [Google Scholar]
- Pappachan, J.M.; Varughese, G.I.; Sriraman, R.; Arunagirinathan, G. Diabetic cardiomyopathy: Pathophysiology, diagnostic evaluation and management. World J. Diabetes 2013, 4, 177–189. [Google Scholar]
- Prasad, A.; Bekker, P.; Tsimikas, S. Advanced glycation end products and diabetic cardiovascular disease. Cardiol. Rev. 2012, 20, 177–183. [Google Scholar]
- Andreadou, I.; Efentakis, P.; Balafas, E.; Togliatto, G.; Davos, C.H.; Varela, A.; Dimitriou, C.A.; Nikolaou, P.E.; Maratou, E.; Lambadiari, V.; et al. Empagliflozin limits myocardial infarction in vivo and cell death in vitro: Role of STAT3, mitochondria, and redox aspects. Front. Physiol. 2017, 8, 1077. [Google Scholar]
- Zelniker, T.A.; Braunwald, E. Mechanisms of cardiorenal effects of sodium-glucose cotransporter 2 inhibitors: JACC State-of-the-art Review. J. Am. Coll. Cardiol. 2020, 75, 422–434. [Google Scholar]
- Anderson, S.L. Dapagliflozin efficacy and safety: A perspective review. Ther. Adv. Drug. Saf. 2014, 5, 242–254. [Google Scholar]
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johansen, O.E.; Woerle, H.J.; et al. EMPA-REG Outcome Investigators. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N. Engl. J. Med. 2015, 373, 2117–2128. [Google Scholar]
- Neal, B.; Perkovic, V.; Mahaffey, K.W.; de Zeeuw, D.; Fulcher, G.; Erondu, N.; Shaw, W.; Law, G.; Desai, M.; Matthews, D.R.; et al. CANVAS Program Collaborative Group. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N. Engl. J. Med. 2017, 377, 644–657. [Google Scholar]
- Lopaschuk, G.D.; Verma, S. Mechanisms of cardiovascular benefits of sodium glucose co-transporter 2 (SGLT2) inhibitors: A State-of-the-art Review. JACC Basic Transl. Sci. 2020, 5, 632–644. [Google Scholar]
- Anker, S.D.; Butler, J.; Filippatos, G.; Ferreira, J.P.; Bocchi, E.; Bohm, M.; Rocca, H.-P.B.; Choi, D.-J.; Chopra, V.; Chuquiure-Valenzuela, E.; et al. EMPEROR-Preserved Trial Investigators. Empagliflozin in heart failure with a preserved ejection fraction. N. Engl. J. Med. 2021, 385, 1451–1461. [Google Scholar]
- Baba, Y.; Ishibashi, R.; Takasaki, A.; Ito, C.; Watanabe, A.; Tokita, M.; Meguro, M.; Harama, T.; Hirayama, K.; Yamamoto, T.; et al. Effects of sodium glucose co-transporter 2 inhibitors in type 1 diabetes mellitus on body composition and glucose variabilities: Single-arm, exploratory trial. Diabetes Ther. 2021, 12, 1415–1427. [Google Scholar]
- Dandona, P.; Phillip, M.; Gillard, P.; Edelman, S.; Jendle, J.; Xu, J.; Scheerer, M.F.; Thoren, F.; Iqbal, N.; Repetto, E.; et al. Effect of dapagliflozin as an adjunct to insulin over 52 weeks in individuals with type 1 diabetes: Post-hoc renal analysis of the depict randomised controlled trials. Lancet Diabetes Endocrinol. 2020, 8, 845–854. [Google Scholar]
- Ishibashi, R.; Baba, Y.; Kakinuma, K.; Takasaki, A.; Hiraga, C.; Harama, T.; Yamamoto, T.; Nakamura, S.; Koshizaka, M.; Maezawa, Y.; et al. Assessing patient satisfaction following sodium glucose co-transporter 2 inhibitor treatment for type 1 diabetes mellitus: A prospective study in Japan. Diabetes Ther. 2021, 12, 453–460. [Google Scholar]
- Huang, Y.; Jiang, Z.; Wei, Y. Efficacy and safety of the SGLT2 inhibitor dapagliflozin in type 1 diabetes: A meta-analysis of randomized controlled trials. Exp. Ther. Med. 2021, 21, 382. [Google Scholar]
- Rao, L.; Ren, C.; Luo, S.; Huang, C.; Li, X. Sodium-glucose cotransporter 2 inhibitors as an add-on therapy to insulin for type 1 diabetes mellitus: Meta-analysis of randomized controlled trials. Acta Diabetol. 2021, 58, 869–880. [Google Scholar]
- Hughes, M.S.; Bailey, R.; Calhoun, P.; Shah, V.N.; Lyons, S.K.; DeSalvo, D.J. Off-label use of sodium glucose co-transporter inhibitors among adults in type 1 diabetes exchange registry. Diabetes Obes. Metab. 2022, 24, 171–173. [Google Scholar]
- Jankauskas, S.S.; Kansakar, U.; Varzideh, F.; Wilson, S.; Mone, P.; Lombardi, A.; Gambardella, J.; Santulli, G. Heart failure in diabetes. Metabolism 2021, 125, 154910. [Google Scholar]
- Rosa, C.M.; Gimenes, R.; Campos, D.H.; Guirado, G.N.; Gimenes, C.; Fernandes, A.A.H.; Cicogna, A.C.; Queiroz, R.M.; Falcão-Pires, I.; Miranda-Silva, D.; et al. Apocynin influence on oxidative stress and cardiac remodeling of spontaneously hypertensive rats with diabetes mellitus. Cardiovasc. Diabetol. 2016, 15, 126. [Google Scholar]
- Gimenes, C.; Gimenes, R.; Rosa, C.M.; Xavier, N.P.; Campos, D.H.S.; Fernandes, A.A.H.; Cezar, M.D.M.; Guirado, G.N.; Cicogna, A.C.; Takamoto, A.H.R.; et al. Low intensity physical exercise attenuates cardiac remodeling and myocardial oxidative stress and dysfunction in diabetic rats. J. Diabetes Res. 2015, 2015, 457848. [Google Scholar]
- Guimaraes, J.F.; Muzio, B.P.; Rosa, C.M.; Nascimento, A.F.; Sugizaki, M.M.; Fernandes, A.A.H.; Cicogna, A.C.; Padovani, C.R.; Okoshi, M.P.; Okoshi, K. Rutin administration attenuates myocardial dysfunction in diabetic rats. Cardiovasc. Diabetol. 2015, 14, 90. [Google Scholar]
- Gimenes, R.; Gimenes, C.; Rosa, C.M.; Xavier, N.P.; Campos, D.H.S.; Fernandes, A.A.H.; Cezar, M.D.M.; Guirado, G.N.; Pagan, L.U.; Chaer, I.D.; et al. Influence of apocynin on cardiac remodeling in rats with streptozotocin-induced diabetes mellitus. Cardiovasc. Diabetol. 2018, 17, 15. [Google Scholar]
- Oliveira Junior, S.A.; Dal Pai-Silva, M.; Martinez, P.F.; Lima-Leopoldo, A.P.; Campos, D.H.S.; Leopoldo, A.S.; Okoshi, M.P.; Okoshi, K.; Padovani, C.R.; Cicogna, A.C. Diet-induced obesity causes metabolic, endocrine and cardiac alterations in spontaneously hypertensive rats. Med. Sci. Monit. 2010, 16, BR367–BR373. [Google Scholar]
- Cezar, M.D.; Damatto, R.L.; Martinez, P.F.; Lima, A.R.R.; Campos, D.H.S.; Rosa, C.M.; Guizoni, D.M.; Bonomo, C.; Cicogna, A.C.; Gimenes, R.; et al. Aldosterone blockade reduces mortality without changing cardiac remodeling in spontaneously hypertensive rats. Cell. Physiol. Biochem. 2013, 32, 1275–1287. [Google Scholar]
- Lima, A.R.; Martinez, P.F.; Damatto, R.L.; Cezar, M.D.; Guizoni, D.M.; Bonomo, C.; Oliveira, S.A., Jr.; Dal-Pai Silva, M.; Zornoff, L.A.; Okoshi, K.; et al. Heart failure-induced diaphragm myopathy. Cell. Physiol. Biochem. 2014, 34, 333–345. [Google Scholar]
- Cicogna, A.C.; Padovani, C.R.; Okoshi, K.; Aragon, F.F.; Okoshi, M.P. Myocardial function during chronic food restriction in isolated hypertrophied cardiac muscle. Am. J. Med. Sci. 2000, 320, 244–248. [Google Scholar]
- Minicucci, M.F.; Azevedo, P.S.; Martinez, P.F.; Lima, A.R.R.; Bonomo, C.; Guizoni, D.M.; Polegato, B.F.; Okoshi, M.P.; Okoshi, K.; Matsubara, B.B.; et al. Critical infarct size to induce ventricular remodeling, cardiac dysfunction and heart failure in rats. Int. J. Cardiol. 2011, 151, 242–243. [Google Scholar]
- Okoshi, K.; Fioretto, J.R.; Okoshi, M.P.; Cicogna, A.C.; Aragon, F.F.; Matsubara, L.S.; Matsubara, B.B. Food restriction induces in vivo ventricular dysfunction in spontaneously hypertensive rats without impairment of in vitro myocardial contractility. Braz. J. Med. Biol. Res. 2004, 37, 607–613. [Google Scholar]
- Gomes, N.J.; Pagan, L.U.; Lima, A.R.R.; Reyes, D.R.A.; Martinez, P.F.; Damatto, F.C.; Pontes, T.H.D.; Rodrigues, E.A.; Souza, L.M.; Tosta, I.F.; et al. Effects of aerobic and resistance exercise on cardiac remodelling and skeletal muscle oxidative stress of infarcted rats. J. Cell. Mol. Med. 2020, 24, 5352–5362. [Google Scholar]
- Reyes, D.R.A.; Gomes, M.J.; Rosa, C.M.; Pagan, L.U.; Damatto, F.C.; Damatto, R.L.; Depra, I.; Campos, D.H.S.; Fernandez, A.A.H.; Martinez, P.F.; et al. N-acetylcysteine influence on oxidative stress and cardiac remodeling in rats during transition from compensated left ventricular hypertrophy to heart failure. Cell. Physiol. Biochem. 2017, 44, 2310–2321. [Google Scholar]
- Okoshi, M.P.; Matsubara, L.S.; Franco, M.; Cicogna, A.C.; Matsubara, B.B. Myocyte necrosis is the basis for fibrosis in renovascular hypertensive rats. Braz. J. Med. Biol. Res. 1997, 30, 1135–1144. [Google Scholar]
- Guizoni, D.M.; Oliveira-Junior, S.A.; Noor, S.L.; Pagan, L.U.; Martinez, P.F.; Lima, A.R.R.; Gomes, M.J.; Damatto, R.L.; Cezar, M.D.; Bonomo, C.; et al. Effects of late exercise on cardiac remodeling and myocardial calcium handling proteins in rats with moderate and large size myocardial infarction. Int. J. Cardiol. 2016, 221, 406–412. [Google Scholar]
- Matsubara, L.S.; Matsubara, B.B.; Okoshi, M.P.; Franco, M.; Cicogna, A.C. Myocardial fibrosis rather than hypertrophy induces diastolic dysfunction in renovascular hypertensive rats. Can. J. Physiol. Pharmacol. 1997, 75, 1328–1334. [Google Scholar]
- Damatto, R.L.; Lima, A.R.R.; Martinez, P.F.; Cezar, M.D.M.; Okoshi, K.; Okoshi, M.P. Myocardial myostatin in spontaneously hypertensive rats with heart failure. Int. J. Cardiol. 2016, 215, 384–387. [Google Scholar]
- Martinez, P.F.; Bonomo, C.; Guizoni, D.M.; Oliveira Junior, S.A.; Damatto, R.L.; Cezar, M.D.M.; Lima, A.R.R.; Pagan, L.U.; Seiva, F.R.; Bueno, R.T.; et al. Modulation of MAPK and NF-KB signaling pathways by antioxidant therapy in skeletal muscle of heart failure rats. Cell. Physiol. Biochem. 2016, 39, 371–384. [Google Scholar]
- Martinez, P.F.; Bonomo, C.; Guizoni, D.M.; Oliveira Junior, S.A.; Damatto, R.L.; Cezar, M.D.M.; Lima, A.R.R.; Pagan, L.U.; Seiva, F.R.; Fernandes, D.C.; et al. Influence of N-acetylcysteine on oxidative stress in slow-twitch soleus muscle of heart failure rats. Cell. Physiol. Biochem. 2015, 35, 148–159. [Google Scholar]
- Reyes, D.R.A.; Gomes, M.J.; Rosa, C.M.; Pagan, L.U.; Zanati, S.G.; Damatto, R.L.; Rodrigues, E.A.; Carvalho, R.F.; Fernandes, A.A.H.; Martinez, P.F.; et al. Exercise during transition from compensated left ventricular hypertrophy to heart failure in aortic stenosis rats. J. Cell. Mol. Med. 2019, 23, 1235–1245. [Google Scholar]
- Paulson, D.J.; Shug, A.L.; Zhao, J. Protection of the ischemic diabetic heart by L-propionylcarnitine therapy. Mol. Cell. Biochem. 1992, 116, 131–137. [Google Scholar]
- Hatch, G.M.; Cao, S.G.; Angel, A. Decrease in cardiac phosphatidylglycerol in streptozotocin-induced diabetic rats does not affect cardiolipin biosynthesis: Evidence for distinct pools of phosphatidylglycerol in the heart. Biochem. J. 1995, 306, 759–764. [Google Scholar]
- Tosaki, A.; Pali, T.; Droy-Lefaix, M.T. Effects of Ginkgo biloba extract and preconditioning on the diabetic rat myocardium. Diabetologia 1996, 39, 1255–1262. [Google Scholar]
- Hadova, K.; Mesarosova, L.; Kralova, E.; Doka, G.; Krenek, P.; Klimas, J. The tyrosine kinase inhibitor crizotinib influences blood glucose and mRNA expression of GLUT4 and PPARs in the heart of rats with experimental diabetes. Can. J. Physiol. Pharmacol. 2021, 99, 635–643. [Google Scholar]
- Badole, S.L.; Chaudhari, S.M.; Jangam, G.B.; Kandhare, A.D.; Bodhankar, S.L. Cardioprotective activity of Pongamia pinnata in streptozotocin-nicotinamide induced diabetic rats. Biomed. Res. Int. 2015, 2015, 403291. [Google Scholar]
- Tosaki, A.; Engelman, D.T.; Engelman, R.M.; Das, D.K. Diabetes and ATP-sensitive potassium channel openers and blockers in isolated ischemic/reperfused hearts. J. Pharmacol. Exp. Ther. 1995, 275, 1115–1123. [Google Scholar]
- Ewis, S.A.; Abdel-Rahman, M.S. Effect of metformin on glutathione and magnesium in normal and streptozotocin-induced diabetic rats. J. Appl. Toxicol. 1995, 15, 387–390. [Google Scholar]
- Rosa, C.M.; Xavier, N.P.; Campos, D.H.; Fernandes, A.A.; Cezar, M.D.; Martinez, P.F.; Cicogna, A.C.; Gimenes, C.; Gimenes, R.; Okoshi, M.P.; et al. Diabetes mellitus activated fetal gene program and intensifies cardiac remodeling and oxidative stress in aged spontaneously hypertensive rats. Cardiovasc. Diabetol. 2013, 12, 152. [Google Scholar]
- Cunha, J.M.; Funez, M.I.; Cunha, F.Q.; Parada, C.A.; Ferreira, S.H. Streptozotocin-induced mechanical hypernociception is not dependent on hyperglycemia. Braz. J. Med. Biol. Res. 2009, 42, 197–206. [Google Scholar]
- Koh, P.-O. Streptozotocin-induced diabetes increases apoptosis through JNK phosphorylation and Bax activation in rat testes. J. Vet. Med. Sci. 2007, 69, 969–971. [Google Scholar]
- Seufert, J.; Lanzinger, S.; Danne, T.; Bramlage, P.; Schmid, S.M.; Kopp, F.; Kress, S.; Fasching, P.; Schafer, C.; Holl, R.W.; et al. Real-world data of 12-month adjunct sodium-glucose co-transporter-2 inhibitor treatment in type 1 diabetes from the German/Austrian DPV Registry: Improved HbA1c without diabetic ketoacidosis. Diabetes Obes. Metab. 2022, 24, 742–746. [Google Scholar]
- Gillard, P.; Schnell, O.; Groop, P.-H. The nephrological perspective on SGLT-2 inhibitors in type 1 diabetes. Diabetes Res. Clin. Pract. 2020, 170, 108462. [Google Scholar]
- Bamba, R.; Okamura, T.; Hashimoto, Y.; Majima, S.; Senmaru, T.; Ushigome, E.; Nakanishi, N.; Asano, M.; Yamazaki, M.; Takakuwa, H.; et al. Extracellular lipidome change by an SGLT2 inhibitor, luseogliflozin, contributes to prevent skeletal muscle atrophy in db/db mice. J. Cachexia Sarcopenia Muscle 2022, 13, 574–588. [Google Scholar]
- Briasoulis, A.; Dhaybi, O.A.; Bakris, G.L. SGLT2 inhibitors and mechanisms of hypertension. Curr. Cardiol. Rep. 2018, 20, 1. [Google Scholar]
- Kawasoe, S.; Maruguchi, Y.; Kajiya, S.; Uenomachi, H.; Miyata, M.; Kawasoe, M.; Kubozono, T.; Ohishi, M. Mechanism of the blood pressure-lowering effect of sodium-glucose cotransporter 2 inhibitors in obese patients with type 2 diabetes. BMC Pharmacol. Toxicol. 2017, 18, 23. [Google Scholar]
- Durante, W.; Behnammanesh, G.; Peyton, K.J. Effects of sodium-glucose co-transporter 2 inhibitors on vascular cell function and arterial remodeling. Int. J. Mol. Sci. 2021, 22, 8786. [Google Scholar]
- Arow, M.; Waldman, M.; Yadin, D.; Nudelman, V.; Shainberg, A.; Abraham, N.G.; Freimark, D.; Kornowski, R.; Aravot, D.; Hochhauser, E.; et al. Sodium-glucose cotransporter 2 inhibitor dapagliflozin attenuates diabetic cardiomyopathy. Cardiovasc. Diabetol. 2020, 19, 7. [Google Scholar]
- Joshi, S.S.; Singh, T.; Newby, D.E.; Singh, J. Sodium-glucose co-transporter 2 inhibitor therapy: Mechanisms of action in heart failure. Heart 2021, 107, 1032–1038. [Google Scholar]
- Marchini, G.S.; Cestari, I.N.; Salemi, V.M.C.; Irigoyen, M.C.; Arnold, A.; Kakoi, A.; Rocon, C.; Aiello, V.D.; Cestari, I.A. Early changes in myocyte contractility and cardiac function in streptozotocin-induced type 1 diabetes in rats. PLoS ONE 2020, 15, e0237305. [Google Scholar]
- Kusaka, H.; Koibuchi, N.; Hasegawa, Y.; Ogawa, H.; Kim-Mitsuyama, S. Empagliflozin lessened cardiac injury and reduced visceral adipocyte hypertrophy in prediabetic rats with metabolic syndrome. Cardiovasc. Diabetol. 2016, 15, 157. [Google Scholar]
- Fan, D.; Takawale, A.; Lee, J.; Kassiri, Z. Cardiac fibroblasts, fibrosis and extracellular matrix remodeling in heart disease. Fibrogenesis Tissue Repair 2012, 5, 5–15. [Google Scholar]
- Pagan, L.U.; Damatto, R.L.; Gomes, M.J.; Lima, A.R.R.; Cezar, M.D.M.; Damatto, F.C.; Reyes, D.R.A.; Caldonazo, T.M.M.; Polegato, B.F.; Okoshi, M.P.; et al. Low-intensity aerobic exercise improves cardiac remodelling of adult spontaneously hypertensive rats. J. Cell. Mol. Med. 2019, 23, 6504–6507. [Google Scholar]
- Quagliariello, V.; De Laurentiis, M.; Rea, D.; Barbieri, A.; Monti, M.G.; Carbone, A.; Paccone, A.; Altucci, L.; Conte, M.; Canale, M.L.; et al. The SGLT-2 inhibitor empagliflozin improves myocardial strain, reduces cardiac fibrosis and pro-inflammatory cytokines in non-diabetic mice treated with doxorubicin. Cardiovasc. Diabetol. 2021, 20, 150. [Google Scholar]
- Cieluch, A.; Uruska, A.; Zozulinska-Ziolkiewicz, D. Can we prevent mitochondrial dysfunction and diabetic cardiomyopathy in type 1 diabetes mellitus? Pathophysiology and treatment options. Int. J. Mol. Sci. 2020, 21, 2852. [Google Scholar]
- Singh, R.M.; Waqar, T.; Howarth, F.C.; Adeghate, E.; Bidasee, K.; Singh, J. Hyperglycemia-induced cardiac contractile dysfunction in the diabetic heart. Heart Fail. Rev. 2018, 23, 37–54. [Google Scholar]
- Rukavina-Mikusic, I.A.; Rey, M.; Martinefski, M.; Tripodi, V.; Valdez, L.B. Temporal evolution of cardiac mitochondrial dysfunction in a type 1 diabetes model. Mitochondrial complex I impairment, and H2O2 and NO productions as early subcellular events. Free Radic. Biol. Med. 2021, 162, 129–140. [Google Scholar]
- Hatanaka, T.; Ogawa, D.; Tachibana, H.; Eguchi, J.; Inoue, T.; Yamada, H.; Takei, K.; Makino, H.; Wada, J. Inhibition of SGLT2 alleviates diabetic nephropathy by suppressing high glucose-induced oxidative stress in type 1 diabetic mice. Pharmacol. Res. Perspect. 2016, 4, e00239. [Google Scholar]
- Sayed, N.; Abdalla, O.; Kilany, O.; Dessouki, A.; Yoshida, T.; Sasaki, K.; Shimoda, M. Effect of dapagliflozin alone and in combination with insulin in a rat model of type 1 diabetes. J. Vet. Med. Sci. 2020, 82, 467–474. [Google Scholar]
- Vlassara, H.; Uribarri, J. Advanced glycation end products (AGE) and diabetes: Cause, effect, or both? Curr. Diab. Rep. 2014, 14, 453. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| C (n = 14) | C + DAPA (n = 14) | DM (n = 20) | DM + DAPA (n = 20) | |
|---|---|---|---|---|
| Initial BW (g) | 448 ± 44 | 449 ± 44 | 450 ± 42 | 448 ± 39 |
| Final BW (g) | 507 ± 52 | 474 ± 50 | 381 ± 52 * | 430 ± 48 #§ |
| Final BP (mmHg) | 124 (122–127) | 123 (120–126) | 140 (136–144) * | 133 (130–138) #§ |
| Initial blood glucose (mg/dL) | 111 (106–115) | 103 (99–111) | 111 (104–114) | 105 (103–114) |
| Blood glucose before DAPA | 110 (102–113) | 108 (104–119) | 573 (443–600) * | 560 (439–600) # |
| Final blood glucose (mg/dL) | 101 (95–105) | 99 (90–109) | 494 (422–546) * | 145 (131–188) #§ |
| C (n = 14) | C + DAPA (n = 14) | DM (n = 20) | DM + DAPA (n = 20) | |
|---|---|---|---|---|
| HR (bpm) | 273 ± 35 | 251 ± 43 | 248 ± 33 | 254 ± 39 |
| LVDD (mm) | 7.78 (7.64–7.83) | 7.69 (7.46–8.03) | 7.88 (7.56–8.37) | 8.09 (7.56–8.34) |
| LVSD (mm) | 3.68 ± 0.40 | 3.88 ± 0.35 | 4.36 ± 0.53 * | 4.30 ± 0.56 # |
| LVPWT (mm) | 1.30 (1.27–1.37) | 1.33 (1.30–1.37) | 1.33 (1.29–1.39) | 1.37 (1.33–1.40) |
| LVSWT (mm) | 1.30 (1.27–1.37) | 1.33 (1.30–1.37) | 1.35 (1.30–1.39) | 1.37 (1.33–1.40) |
| AO (mm) | 4.01 (4.01–4.16) | 4.01 (3.83–4.10) | 3.83 (3.83–3.89) * | 4.01 (3.83–4.01) |
| LA (mm) | 5.62 ± 0.34 | 5.52 ± 0.44 | 5.99 ± 0.42 * | 5.34 ± 0.44 § |
| LA/AO | 1.39 ± 0.08 | 1.39 ± 0.06 | 1.55 ± 0.10 * | 1.37 ± 0.09 § |
| LVDD/BW (mm/kg) | 15.4 (15.0–15.8) | 15.9 (15.3–18.1) | 21.4 (19.7–23.0) * | 19.5 (17.0–20.3) #§ |
| LA/BW (mm/kg) | 11.2 ± 1.41 | 11.7 ± 1.18 | 15.9 ± 1.93 * | 12.6 ± 1.36 § |
| LV mass (g) | 0.69 ± 0.07 | 0.68 ± 0.07 | 0.72 ± 0.10 | 0.75 ± 0.09 # |
| LV mass/BW (g/kg) | 1.36 (1.31–1.42) | 1.47 (1.30–1.50) | 1.95 (1.73–2.11) * | 1.79 (1.52–2.03) # |
| RWT | 0.34 ± 0.01 | 0.35 ± 0.02 | 0.34 ± 0.02 | 0.34 ± 0.02 |
| C (n = 14) | C + DAPA (n = 14) | DM (n = 20) | DM + DAPA (n = 20) | |
|---|---|---|---|---|
| EFS (%) | 52.9 ± 4.51 | 49.5 ± 3.64 | 44.9 ± 4.73 * | 46.5 ± 4.99 |
| Ejection fraction | 0.89 ± 0.03 | 0.87 ± 0.03 | 0.83 ± 0.04 * | 0.84 ± 0.04 # |
| PWSV (mm/s) | 39.9 ± 4.23 | 36.3 ± 4.58 * | 30.1 ± 3.83 * | 33.6 ± 4.85 § |
| Tei Index | 0.48 ± 0.06 | 0.50 ± 0.06 | 0.55 ± 0.08 * | 0.49 ± 0.07 § |
| Lateral TDI-S’ (cm/s) | 3.50 (3.30–4.00) | 3.65 (3.40–4.00) | 3.30 (3.10–3.40) * | 3.45 (3.10–3.70) |
| Septal TDI-S’ (cm/s) | 3.63 ± 0.50 | 3.41 ± 0.36 | 3.22 ± 0.39 * | 3.29 ± 0.35 |
| Mean TDI-S’ (cm/s) | 3.58 (3.45–3.80) | 3.48 (3.35–3.70) | 3.20 (3.10–3.40) * | 3.35 (3.08–3.68) |
| C (n = 14) | C + DAPA (n = 14) | DM (n = 20) | DM + DAPA (n = 20) | |
|---|---|---|---|---|
| E-wave (cm/s) | 76.1 ± 7.75 | 71.5 ± 3.33 | 70.5 ± 6.29 * | 72.8 ± 6.09 |
| A-wave (cm/s) | 46.4 ± 13.7 | 39.2 ± 6.58 | 48.5 ± 12.6 | 44.1 ± 11.9 |
| E/A | 1.70 (1.38–1.91) | 1.75 (1.67–2.05) | 1.48 (1.22–1.74) | 1.71 (1.54–2.02) |
| IVRT (ms) | 26.0 ± 2.72 | 28.5 ± 3.13 | 38.7 ± 5.67 * | 31.1 ± 5.77 § |
| IVRT/R-R | 52.4 (51.4–57.8) | 59.4 (57.3–62.3) | 80.9 (68.5–87.9) * | 61.7 (56.4–66.9) § |
| EDT (ms) | 52.0 ± 8.64 | 54.5 ± 7.20 | 54.8 ± 8.57 | 53.1 ± 7.84 |
| Lateral TDI-E’ | 4.43 ± 0.65 | 4.16 ± 0.46 | 4.30 ± 0.66 | 4.19 ± 0.62 |
| Septal TDI-E’ | 4.26 ± 0.69 | 4.13 ± 0.54 | 4.22 ± 0.66 | 4.31 ± 0.78 |
| Average TDI-E’ | 4.33 (3.85–4.70) | 4.10 (3.90–4.40) | 4.53 (3.65–4.75) | 4.45 (3.78–4.69) |
| Lateral TDI-A’ | 3.50 (2.80–4.90) | 2.60 (2.30–3.60) | 3.85 (3.10–4.30) | 3.20 (2.85–3.93) |
| Septal TDI-A’ | 3.00 (2.70–4.20) | 2.60 (2.10–3.40) | 3.50 (2.90–4.60) | 2.90 (2.80–4.35) |
| Average TDI-A’ | 3.35 (2.80–4.00) | 3.20 (2.96–3.99) | 3.63 (3.05–4.45) | 3.20 (2.96–3.99) |
| E/average E’ | 17.7 ± 2.39 | 17.7 ± 1.57 | 16.7 ± 2.56 | 17.2 ± 2.33 |
| Mean E’/average A’ | 1.29 ± 0.40 | 1.48 ± 0.42 | 1.20 ± 0.38 | 1.30 ± 0.35 |
| C (n = 14) | C + DAPA (n = 14) | DM (n = 20) | DM + DAPA (n = 20) | |
|---|---|---|---|---|
| BW (g) | 460 ± 43 | 449 ± 55 | 343 ± 52 * | 389 ± 46 #§ |
| LV (g) | 0.79 ± 0.14 | 0.79 ± 0.09 | 0.68 ± 0.11 * | 0.72 ± 0.10 |
| LV/BW (g/kg) | 1.72 ± 0.32 | 1.80 ± 0.22 | 2.01 ± 0.32 * | 1.86 ± 0.28 |
| RV (g) | 0.24 ± 0.05 | 0.21 ± 0.03 | 0.22 ± 0.04 | 0.20 ± 0.04 |
| RV/BW (g/kg) | 0.51 (0.46–0.53) | 0.47 (0.41–0.53) | 0.62 (0.54–0.67) * | 0.52 (0.47–0.57) § |
| Atria (g) | 00.10 ± 0.03 | 0.08 ± 0.02 | 0.08 ± 0.02 | 0.08 ± 0.02 |
| Atria/BW (g/kg) | 0.22 ± 0.06 | 0.19 ± 0.04 | 0.23 ± 0.06 | 0.22 ± 0.05 |
| C (n = 10) | C + DAPA (n = 10) | DM (n = 10) | DM + DAPA (n = 10) | |
|---|---|---|---|---|
| HOP (mg/g tissue) | 1.43 ± 0.35 | 1.56 ± 0.54 | 1.48 ± 0.28 | 1.50 ± 0.28 |
| ICF (%) | 9.41 ± 0.02 | 8.30 ± 0.02 | 8.85 ± 0.02 | 9.88 ± 0.02 |
| Diameter (μm) | 17.6 (16.7–18.3) | 15.5 (15.1–16.3) * | 17.1 (15.6–17.8) | 17.6 (15.8–18.1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosa, C.M.; Campos, D.H.S.; Reyes, D.R.A.; Damatto, F.C.; Kurosaki, L.Y.; Pagan, L.U.; Gomes, M.J.; Corrêa, C.R.; Fernandes, A.A.H.; Okoshi, M.P.; et al. Effects of the SGLT2 Inhibition on Cardiac Remodeling in Streptozotocin-Induced Diabetic Rats, a Model of Type 1 Diabetes Mellitus. Antioxidants 2022, 11, 982. https://doi.org/10.3390/antiox11050982
Rosa CM, Campos DHS, Reyes DRA, Damatto FC, Kurosaki LY, Pagan LU, Gomes MJ, Corrêa CR, Fernandes AAH, Okoshi MP, et al. Effects of the SGLT2 Inhibition on Cardiac Remodeling in Streptozotocin-Induced Diabetic Rats, a Model of Type 1 Diabetes Mellitus. Antioxidants. 2022; 11(5):982. https://doi.org/10.3390/antiox11050982
Chicago/Turabian StyleRosa, Camila Moreno, Dijon Henrique Salome Campos, David Rafael Abreu Reyes, Felipe Cesar Damatto, Lucas Yamada Kurosaki, Luana Urbano Pagan, Mariana Janini Gomes, Camila Renata Corrêa, Ana Angelica Henrique Fernandes, Marina Politi Okoshi, and et al. 2022. "Effects of the SGLT2 Inhibition on Cardiac Remodeling in Streptozotocin-Induced Diabetic Rats, a Model of Type 1 Diabetes Mellitus" Antioxidants 11, no. 5: 982. https://doi.org/10.3390/antiox11050982
APA StyleRosa, C. M., Campos, D. H. S., Reyes, D. R. A., Damatto, F. C., Kurosaki, L. Y., Pagan, L. U., Gomes, M. J., Corrêa, C. R., Fernandes, A. A. H., Okoshi, M. P., & Okoshi, K. (2022). Effects of the SGLT2 Inhibition on Cardiac Remodeling in Streptozotocin-Induced Diabetic Rats, a Model of Type 1 Diabetes Mellitus. Antioxidants, 11(5), 982. https://doi.org/10.3390/antiox11050982