
The Impact of Whole-Body Cryotherapy on Endothelium Parameters in Patients with Ankylosing Spondylitis

 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
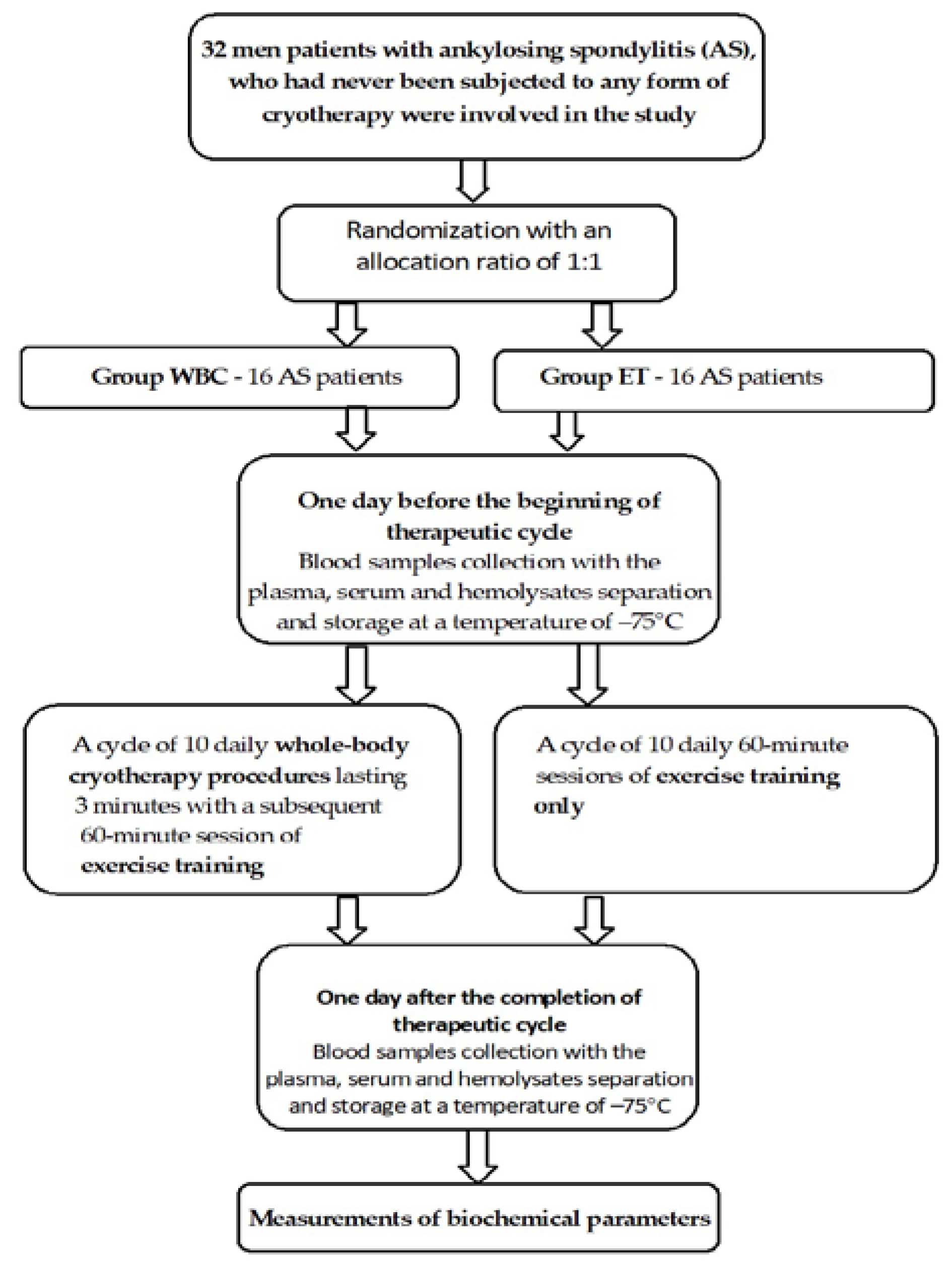
2.1. Patients
2.2. Whole-Body Cryotherapy and Exercise Training Protocol
2.3. Biochemical analysis
2.3.1. Endothelium Function Parameters
2.3.2. Oxidative Stress Parameters
2.4. Statistical analyses
3. Results
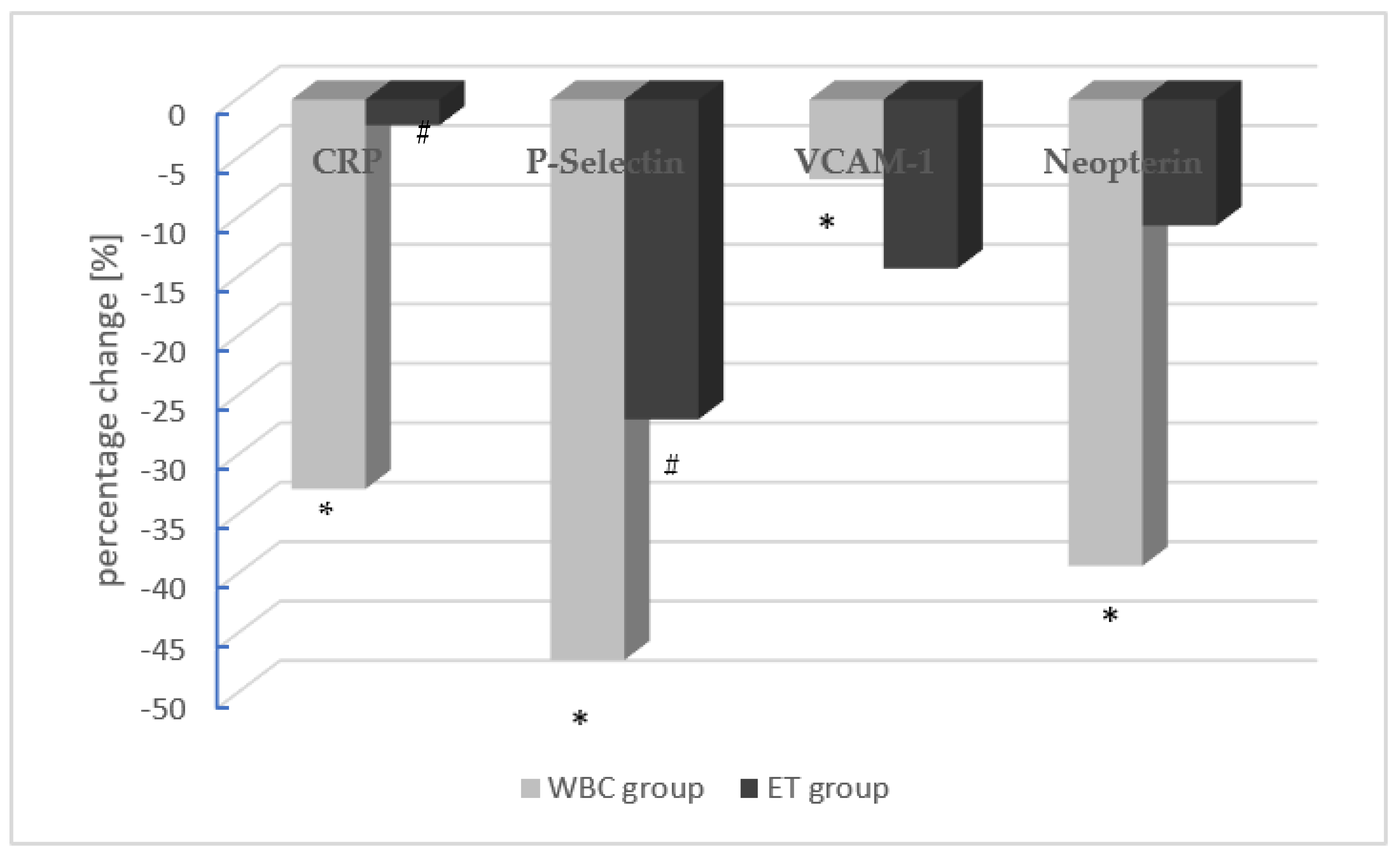
3.1. Endothelium Parameters
3.2. Oxidative Stress Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sieper, J.; Braun, J.; Rudwaleit, M.; Boonen, A.; Zink, A. Ankylosing spondylitis: An overview. Ann. Rheum. Dis. 2002, 61, iii8–iii18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, W.; He, X.; Cheng, K.; Zhang, L.; Chen, D.; Wang, X.; Qiu, G.; Cao, X.; Weng, X. Ankylosing spondylitis: Etiology, pathogenesis, and treatments. Bone Res. 2019, 7, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Heijde, D.; Braun, J.; Deodhar, A.; Baraliakos, X.; Landewé, R.; Richards, H.B.; Porter, B.; Readie, A. Modified stoke ankylosing spondylitis spinal score as an outcome measure to assess the impact of treatment on structural progression in ankylosing spondylitis. Rheumatology 2019, 58, 388–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, J.; Sieper, J. Ankylosing spondylitis. Lancet 2007, 369, 1379–1390. [Google Scholar] [CrossRef] [PubMed]
- Exarchou, S.; Lindstrom, U.; Askling, J.; Eriksson, J.K.; Forsblad-d’Elia, H.; Neovius, M.; Turesson, C.; Kristensen, L.E.; Jacobsson, L.T. The prevalence of clinically diagnosed ankylosing spondylitis and its clinical manifestations: A nationwide register study. Arthritis Res. Ther. 2015, 17, 118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.H.; Chen, Y.M.; Lai, K.L.; Hsieh, T.Y.; Hung, W.T.; Lin, C.T.; Tseng, C.W.; Tang, K.T.; Chou, Y.Y.; Wu, Y.D.; et al. Gender difference in ASAS HI among patients with ankylosing spondylitis. PLoS ONE 2020, 15, e0235678. [Google Scholar] [CrossRef]
- Atzeni, F.; Nucera, V.; Galloway, J.; Zoltán, S.; Nurmohamed, M. Cardiovascular risk in ankylosing spondylitis and the effect of anti-TNF drugs: A narrative review. Expert Opin. Biol. Ther. 2020, 20, 517–524. [Google Scholar] [CrossRef]
- Mathieu, S.; Gossec, L.; Dougados, M.; Soubrier, M. Cardiovascular profile in ankylosing spondylitis: A systematic review and meta-analysis. Arthritis Care Res. 2011, 63, 557–563. [Google Scholar] [CrossRef]
- Verma, I.; Krishan, P.; Syngle, A. Predictors of Atherosclerosis in Ankylosing Spondylitis. Rheumatol. Ther. 2015, 2, 173–182. [Google Scholar] [CrossRef] [Green Version]
- Stanek, A.; Cieślar, G.; Romuk, E.; Kasperczyk, S.; Sieroń-Stołtny, K.; Birkner, E.; Sieroń, A. Decrease in antioxidant status of plasma and erythrocytes from patients with ankylosing spondylitis. Clin. Biochem. 2010, 43, 566–570. [Google Scholar] [CrossRef]
- Stanek, A.; Cholewka, A.; Wielkoszyński, T.; Romuk, E.; Sieroń, K.; Sieroń, A. Increased Levels of Oxidative Stress Markers, Soluble CD40 Ligand, and Carotid Intima-Media Thickness Reflect Acceleration of Atherosclerosis in Male Patients with Ankylosing Spondylitis in Active Phase and without the Classical Cardiovascular Risk Factors. Oxidative Med. Cell. Longev. 2017, 2017, 9712536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perrotta, F.M.; Scarno, A.; Carboni, A.; Bernardo, V.; Montepaone, M.; Lubrano, E.; Spadaro, A. Assessment of subclinical atherosclerosis in ankylosing spondylitis: Correlations with disease activity indices. Reumatismo 2013, 65, 105–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Heijde, D.; Ramiro, S.; Landewé, R.; Baraliakos, X.; Van den Bosch, F.; Sepriano, A.; Regel, A.; Ciurea, A.; Dagfinrud, H.; Dougados, M.; et al. 2016 update of the ASAS-EULAR management recommendations for axial spondyloarthritis. Ann. Rheum. Dis. 2017, 76, 978–991. [Google Scholar] [CrossRef] [PubMed]
- Giannotti, E.; Trainito, S.; Arioli, G.; Rucco, V.; Masiero, S. Effects of physical therapy for the management of patients with ankylosing spondylitis in the biological era. Clin. Rheumatol. 2014, 33, 1217–1230. [Google Scholar] [CrossRef]
- Gravaldi, L.P.; Bonetti, F.; Lezzerini, S.; De Maio, F. Effectiveness of Physiotherapy in Patients with Ankylosing Spondylitis: A Systematic Review and Meta-Analysis. Healthcare 2022, 10, 132. [Google Scholar] [CrossRef]
- Zao, A.; Cantista, P. The role of land and aquatic exercise in ankylosing spondylitis: A systematic review. Rheumatol. Int. 2017, 37, 1979–1990. [Google Scholar] [CrossRef]
- Guillot, X.; Tordi, N.; Mourot, L.; Demougeot, C.; Dugué, B.; Prati, C.; Wendling, D. Cryotherapy in inflammatory rheumatic diseases: A systematic review. Expert Rev. Clin. Immunol. 2014, 10, 281–294. [Google Scholar] [CrossRef]
- Cholewka, A.; Stanek, A.; Wójcik, M.; Sieroń-Stołtny, K.; Drzazga, Z. Does local cryotherapy improve thermal diagnosis similar to whole-body cryotherapy in spinal diseases? J. Therm. Anal. Calorim. 2017, 127, 1155–1162. [Google Scholar] [CrossRef] [Green Version]
- Stanek, A.; Cholewka, A.; Gadula, J.; Drzazga, Z.; Sieron, A.; Sieron-Stoltny, K. Can Whole-Body Cryotherapy with Subsequent Kinesiotherapy Procedures in Closed Type Cryogenic Chamber Improve BASDAI, BASFI, and Some Spine Mobility Parameters and Decrease Pain Intensity in Patients with Ankylosing Spondylitis? BioMed Res. Int. 2015, 2015, 404259. [Google Scholar] [CrossRef] [Green Version]
- Romanowski, M.W.; Straburzyńska-Lupa, A. Is the whole-body cryotherapy a beneficial supplement to exercise therapy for patients with ankylosing spondylitis? J. Back Musculoskelet. Rehabil. 2020, 33, 185–192. [Google Scholar] [CrossRef]
- Stanek, A.; Cholewka, A.; Wielkoszyński, T.; Romuk, E.; Sieroń, A. Whole-Body Cryotherapy Decreases the Levels of Inflammatory, Oxidative Stress, and Atherosclerosis Plaque Markers in Male Patients with Active-Phase Ankylosing Spondylitis in the Absence of Classical Cardiovascular Risk Factors. Mediat. Inflamm. 2018, 2018, 8592532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanek, A.; Cholewka, A.; Wielkoszyński, T.; Romuk, E.; Sieroń, A. Decreased Oxidative Stress in Male Patients with Active Phase Ankylosing Spondylitis Who Underwent Whole-Body Cryotherapy in Closed Cryochamber. Oxidative Med. Cell. Longev. 2018, 2018, 7365490. [Google Scholar] [CrossRef] [PubMed]
- Straburzyńska-Lupa, A.; Kasprzak, M.P.; Romanowski, M.W.; Kwaśniewska, A.; Romanowski, W.; Iskra, M.; Rutkowski, R. The Effect of Whole-Body Cryotherapy at Different Temperatures on Proinflammatory Cytokines, Oxidative Stress Parameters, and Disease Activity in Patients with Ankylosing Spondylitis. Oxidative Med. Cell. Longev. 2018, 2018, 2157496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanek, A.; Wielkoszyński, T.; Bartuś, S.; Cholewka, A. Whole-Body Cryostimulation Improves Inflammatory Endothelium Parameters and Decreases Oxidative Stress in Healthy Subjects. Antioxidants 2020, 9, 1308. [Google Scholar] [CrossRef] [PubMed]
- van der Linden, S.; Valkenburg, H.A.; Cats, A. Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria. Arthritis Rheum. 1984, 27, 361–368. [Google Scholar] [CrossRef]
- Södergren, E.; Nourooz-Zadeh, J.; Berglund, L.; Vessby, B. Re-evaluation of the ferrous oxidation in xylenol orange assay for the measurement of plasma lipid hydroperoxides. J. Biochem. Biophys. Methods 1998, 37, 137–146. [Google Scholar] [CrossRef]
- Jain, S.K. In vivo externalization of phosphatidylserine and phosphatidylethanolamine in the membrane bilayer and hypercoagulability by the lipid peroxidation of erythrocytes in rats. J. Clin. Investig. 1985, 76, 281–286. [Google Scholar] [CrossRef]
- Koster, J.F.; Biemond, P.; Swaak, A.J. Intracellular and extracellular sulphydryl levels in rheumatoid arthritis. Ann. Rheum. Dis. 1986, 45, 44–46. [Google Scholar] [CrossRef] [Green Version]
- Mackness, M.I.; Harty, D.; Bhatnagar, D.; Winocour, P.H.; Arrol, S.; Ishola, M.; Durrington, P.N. Serum paraoxonase activity in familial hypercholesterolemia and insulin-dependent diabetes mellitus. Atherosclerosis 1991, 86, 193–199. [Google Scholar] [CrossRef]
- Rajendran, P.; Rengarajan, T.; Thangavel, J.; Nishigaki, Y.; Sakthisekaran, D.; Sethi, G.; Nishigaki, I. The vascular endothelium and human diseases. Int. J. Biol. Sci. 2013, 9, 1057–1069. [Google Scholar] [CrossRef] [Green Version]
- Serdaroglu Beyazal, M.; Erdogan, T.; Turkyilmaz, A.K.; Devrimsel, G.; Cure, M.C.; Beyazal, M.; Sahin, I. Relationship of serum osteoprotegerin with arterial stiffness, preclinical atherosclerosis, and disease activity in patients with ankylosing spondylitis. Clin. Rheumatol. 2016, 35, 2235–2241. [Google Scholar] [CrossRef] [PubMed]
- Pasceri, V.; Willerson, J.T.; Yeh, E.T. Direct proinflammatory effect of C-reactive protein on human endothelial cells. Circulation 2000, 102, 2165–2168. [Google Scholar] [CrossRef]
- Cook-Mills, J.M.; Marchese, M.E.; Abdala-Valencia, H. Vascular cell adhesion molecule-1 expression and signaling during disease: Regulation by reactive oxygen species and antioxidants. Antioxid. Redox Signal. 2011, 15, 1607–1638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruparelia, N.; Choudhury, R. Inflammation and atherosclerosis: What is on the horizon? Heart 2020, 106, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Woollard, K.J.; Chin-Dusting, J. Therapeutic targeting of p-selectin in atherosclerosis. Inflamm. Allergy-Drug Targets 2007, 6, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Iiyama, K.; Hajra, L.; Iiyama, M.; Li, H.; DiChiara, M.; Medoff, B.D.; Cybulsky, M.I. Patterns of vascular cell adhesion molecule-1 and intercellular adhesion molecule-1 expression in rabbit and mouse atherosclerotic lesions and at sites predisposed to lesion formation. Circ. Res. 1999, 85, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Konstantopoulos, K.; Kukreti, S.; Smith, C.W.; McIntire, L.V. Endothelial P-selectin and VCAM-1 each can function as primary adhesive mechanisms for T cells under conditions of flow. J. Leukoc. Biol. 1997, 61, 179–187. [Google Scholar] [CrossRef]
- Landmesser, U.; Hornig, B.; Drexler, H. Endothelial function: A critical determinant in atherosclerosis? Circulation 2004, 109, II27–II33. [Google Scholar] [CrossRef] [Green Version]
- Murr, C.; Widner, B.; Wirleitner, B.; Fuchs, D. Neopterin as a marker for immune system activation. Curr. Drug Metab. 2002, 3, 175–187. [Google Scholar] [CrossRef]
- Yavuz, F.; Kesikburun, B.; Öztürk, Ö.; Güzelküçük, Ü. Serum chitotriosidase and neopterin levels in patients with ankylosing spondylitis. Ther. Adv. Musculoskelet. Dis. 2019, 11, 1759720X19832321. [Google Scholar] [CrossRef] [Green Version]
- Farghaly, H.S.; Metwalley, K.A.; Raafat, D.M.; Saied, G.M.; Gabri, M.F.; Algowhary, M. Association between vascular endothelial dysfunction and the inflammatory marker neopterin in patients with classic congenital adrenal hyperplasia. Atherosclerosis 2021, 328, 38–43. [Google Scholar] [CrossRef]
- Zhang, Y.Y.; Tong, X.Z.; Xia, W.H.; Xie, W.L.; Yu, B.B.; Zhang, B.; Chen, L.; Tao, J. Increased plasma neopterin levels are associated with reduced endothelial function and arterial elasticity in hypertension. J. Hum. Hypertens. 2016, 30, 436–441. [Google Scholar] [CrossRef]
- Watanabe, T. Neopterin derivatives—A novel therapeutic target rather than biomarker for atherosclerosis and related diseases. Vasa 2021, 50, 165–173. [Google Scholar] [CrossRef]
- Shirai, R.; Sato, K.; Yamashita, T.; Yamaguchi, M.; Okano, T.; Watanabe-Kominato, K.; Watanabe, R.; Matsuyama, T.A.; Ishibashi-Ueda, H.; Koba, S.; et al. Neopterin Counters Vascular Inflammation and Atherosclerosis. J. Am. Heart Assoc. 2018, 7, e007359. [Google Scholar] [CrossRef] [Green Version]
- Aziz, N.; Detels, R.; Quint, J.J.; Gjertson, D.; Ryner, T.; Butch, A.W. Biological variation of immunological blood biomarkers in healthy individuals and quality goals for biomarker tests. BMC Immunol. 2019, 20, 33. [Google Scholar] [CrossRef] [Green Version]
- Wiecek, M.; Szygula, Z.; Gradek, J.; Kusmierczyk, J.; Szymura, J. Whole-Body Cryotherapy Increases the Activity of Nitric Oxide Synthase in Older Men. Biomolecules 2021, 11, 1041. [Google Scholar] [CrossRef]
- Mackness, M.I.; Arrol, S.; Abbott, C.; Durrington, P.N. Protection of low-density lipoprotein against oxidative modification by high-density lipoprotein associated paraoxonase. Atherosclerosis 1993, 104, 129–135. [Google Scholar] [CrossRef]
- Stanek, A.; Sieroń-Stołtny, K.; Romuk, E.; Cholewka, A.; Wielkoszyński, T.; Cieślar, G.; Kwiatek, S.; Sieroń, A.; Kawczyk-Krupka, A. Whole-body cryostimulation as an effective method of reducing oxidative stress in healthy men. Adv. Clin. Exp. Med. 2016, 25, 1281–1291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsirpanlis, G.; Bagos, P.; Ioannou, D.; Bleta, A.; Marinou, I.; Lagouranis, A.; Chatzipanagiotou, S.; Nicolaou, C.; Nascimento, M.M.D.; Stenvinkel, P.; et al. Serum albumin: A late-reacting negative acute-phase protein in clinically evident inflammation in dialysis patients. Nephrol. Dial. Transplant. 2005, 20, 658–659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eckart, A.; Struja, T.; Kutz, A.; Baumgartner, A.; Baumgartner, T.; Zurfluh, S.; Neeser, O.; Huber, A.; Stanga, Z.; Mueller, B.; et al. Relationship of Nutritional Status, Inflammation, and Serum Albumin Levels During Acute Illness: A Prospective Study. Am. J. Med. 2020, 133, 713–722.e7. [Google Scholar] [CrossRef] [PubMed]
- Klemm, P.; Becker, J.; Aykara, I.; Asendorf, T.; Dischereit, G.; Neumann, E.; Müller-Ladner, U.; Lange, U. Serial whole-body cryotherapy in fibromyalgia is effective and alters cytokine profiles. Adv. Rheumatol. 2021, 61, 3. [Google Scholar] [CrossRef] [PubMed]
- Lubkowska, A.; Szyguła, Z.; Chlubek, D.; Banfi, G. The effect of prolonged whole-body cryostimulation treatment with different amounts of sessions on chosen pro- and anti-inflammatory cytokines levels in healthy men. Scand J. Clin. Lab. Investig. 2011, 71, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Miller, E.; Mrowicka, M.; Malinowska, K.; Mrowicki, J.; Saluk-Juszczak, J.; Kędziora, J. Effects of whole-body cryotherapy on a total antioxidative status and activities of antioxidative enzymes in blood of depressive multiple sclerosis patients. World J. Biol. Psychiatry 2011, 12, 223–227. [Google Scholar] [CrossRef]
- Pilch, W.; Wyrostek, J.; Piotrowska, A.; Czerwińska-Ledwig, O.; Zuziak, R.; Sadowska-Krępa, E.; Maciejczyk, M.; Żychowska, M. Blood pro-oxidant/antioxidant balance in young men with class II obesity after 20 sessions of whole body cryostimulation: A preliminary study. Redox Rep. 2021, 26, 10–17. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | WBC Group (n = 16) | Exercise Training (ET) Group (n = 16) | p-Value |
|---|---|---|---|
| Age, years, mean (SD) | 46.63 ± 1.5 | 45.94 ± 1.24 | 0.114 |
| Sex M/F | 16/0 | 16/0 | - |
| BMI, kg/m2, mean (SD) | 24.24 ± 4.4 | 23.76 ± 6.8 | 0.880 |
| BASDAI index | 5.43 ±1.61 | 5.28 ± 1.71 | 0.720 |
| BASFI index | 5.20 ± 2.29 | 5.01 ± 2.06 | 1.00 |
| Smoking (yes/no) | 0/16 | 0/16 | - |
| Medication | |||
| NSAID (yes/no) | 16/0 | 16/0 | - |
| DMARD (yes/no) | 0/16 | 0/16 | - |
| Biological agents (yes/no) | 0/16 | 0/16 | - |
| Parameters | WBC Group | ET Group | p | |
|---|---|---|---|---|
| hsCRP (s) (mg/dL) | before | 17.4 ±15.8 | 13.9 ± 15.2 | 0.532 |
| after | 11.7 ± 15.0 | 13.6 ± 16.2 | 0.730 | |
| P* | 0.013 | 0.623 | ||
| sP-Selectin (p) (ng/mL) | before | 171 ± 85.4 | 197 ± 92.1 | 0.405 |
| after | 90.4 ± 42.4 | 144 ± 103 | 0.067 | |
| P* | 0.011 | 0.044 | ||
| sVCAM-1 (p) (ng/mL) | before | 923 ± 135 | 922 ± 349 | 0.843 |
| after | 861 ± 102 | 791 ± 344 | 0.611 | |
| P* | 0.001 | 0.215 | ||
| Neopterin (s) (ng/mL) | before | 9.05 ± 6.37 | 5.47 ± 3.39 | 0.063 |
| after | 5.50 ± 3.31 | 4.89 ± 2.70 | 0.223 | |
| P* | 0.039 | 0.600 | ||
| Parameters | WBC Group | ET Group | p | |
|---|---|---|---|---|
| LHP (s) (μmol/L) | Before | 19.9 ± 23.7 | 14.3 ± 6.8 | 0.957 |
| After | 9.47 ± 17.0 | 13.8 ± 21.9 | 0.537 | |
| P* | 0.001 | 0.008 | ||
| Lipofuscin (e) (RF/gHb) | Before | 225 ± 43.6 | 201 ± 36.9 | 0.101 |
| After | 41.9 ± 16.5 | 46.4 ± 31.8 | 0.623 | |
| P* | <0.001 | <0.001 | ||
| PON-1 (s) (IU/L) | Before | 163.3 ± 74.9 | 185.5 ± 85.6 | 0.441 |
| After | 132.2 ± 71.0 | 166 ± 82.8 | 0.224 | |
| P* | 0.015 | 0.03 | ||
| PSH (s) (μmol/L) | Before | 402.6 ± 91.7 | 393.2 ± 90.0 | 0.872 |
| After | 616.5 ± 279.1 | 364.7 ± 28.4 | 0.339 | |
| P* | 0. 921 | 0.017 | ||
| Albumin (s) (g/L) | Before | 38.93 ± 2.29 | 40.59 ± 2.32 | 0.060 |
| After | 42.98 ± 2.13 | 41.26 ± 2.38 | <0.001 | |
| P* | 0.044 | 0.756 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stanek, A.; Romuk, E.; Wielkoszyński, T.; Brożyna-Tkaczyk, K.; Wziątek-Kuczmik, D.; Cholewka, A. The Impact of Whole-Body Cryotherapy on Endothelium Parameters in Patients with Ankylosing Spondylitis. Antioxidants 2023, 12, 521. https://doi.org/10.3390/antiox12020521
Stanek A, Romuk E, Wielkoszyński T, Brożyna-Tkaczyk K, Wziątek-Kuczmik D, Cholewka A. The Impact of Whole-Body Cryotherapy on Endothelium Parameters in Patients with Ankylosing Spondylitis. Antioxidants. 2023; 12(2):521. https://doi.org/10.3390/antiox12020521
Chicago/Turabian StyleStanek, Agata, Ewa Romuk, Tomasz Wielkoszyński, Klaudia Brożyna-Tkaczyk, Daria Wziątek-Kuczmik, and Armand Cholewka. 2023. "The Impact of Whole-Body Cryotherapy on Endothelium Parameters in Patients with Ankylosing Spondylitis" Antioxidants 12, no. 2: 521. https://doi.org/10.3390/antiox12020521
APA StyleStanek, A., Romuk, E., Wielkoszyński, T., Brożyna-Tkaczyk, K., Wziątek-Kuczmik, D., & Cholewka, A. (2023). The Impact of Whole-Body Cryotherapy on Endothelium Parameters in Patients with Ankylosing Spondylitis. Antioxidants, 12(2), 521. https://doi.org/10.3390/antiox12020521