Bioavailability of Epigallocatechin Gallate Administered with Different Nutritional Strategies in Healthy Volunteers

 ,
,  , , and
, , and 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Participants and Selection Criteria
2.2. Reagents and EGCG Preparations
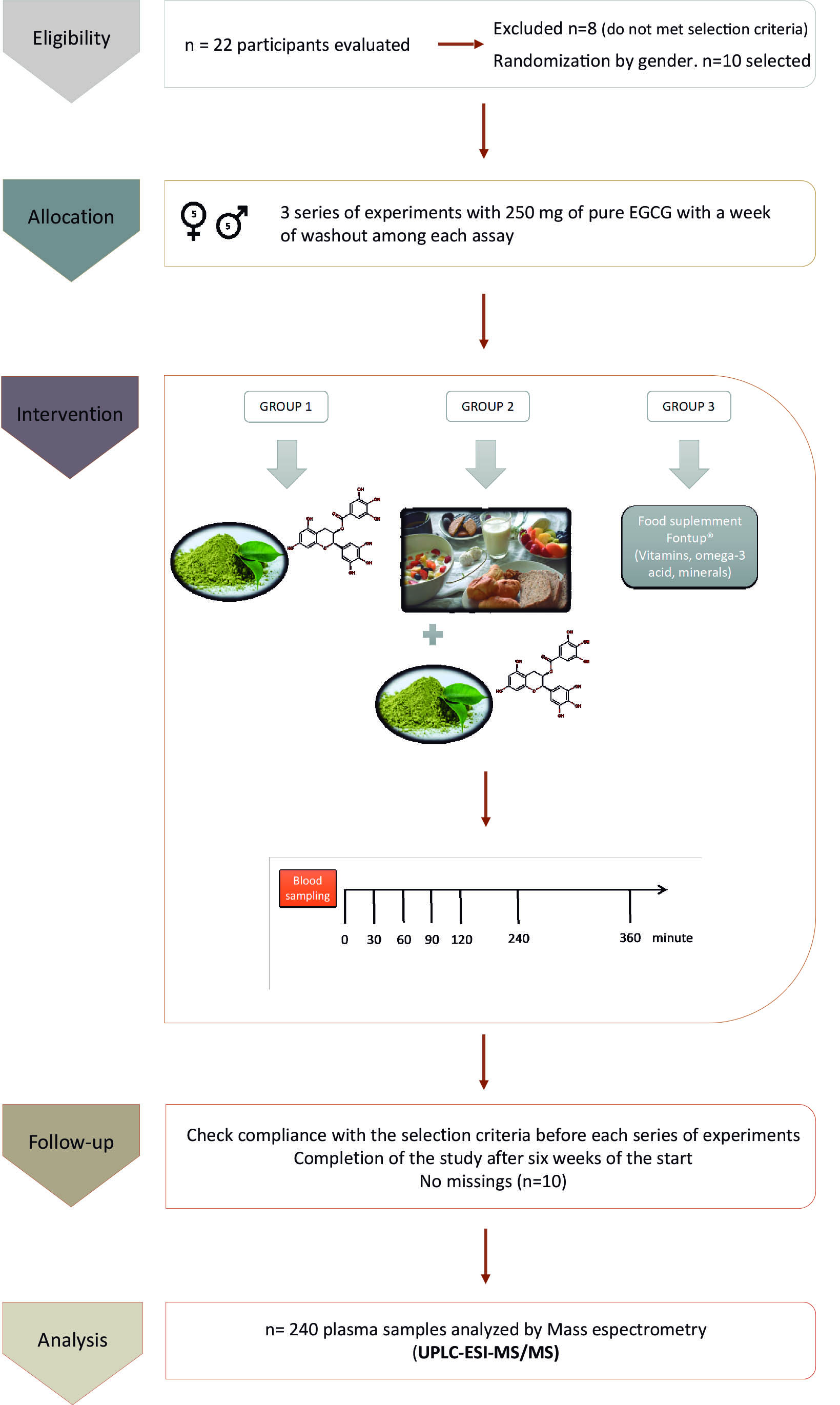
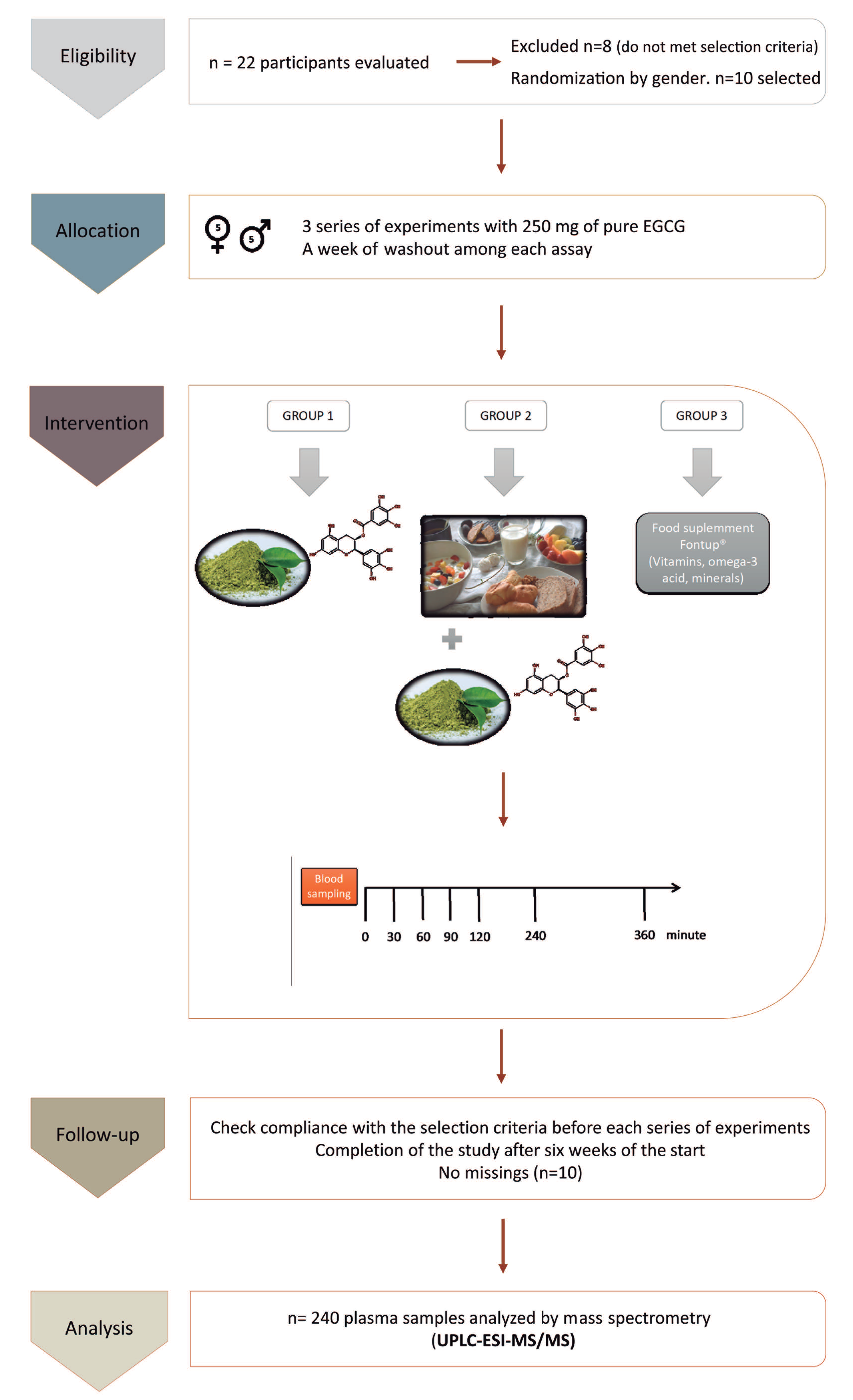
2.3. Interventions
2.4. Blood Collection, Processing, and Plasma Storage Protocol
2.5. Determination of Free EGCG in Plasma Samples
2.5.1. Preparation of Standard Solutions
2.5.2. Sample Preparation
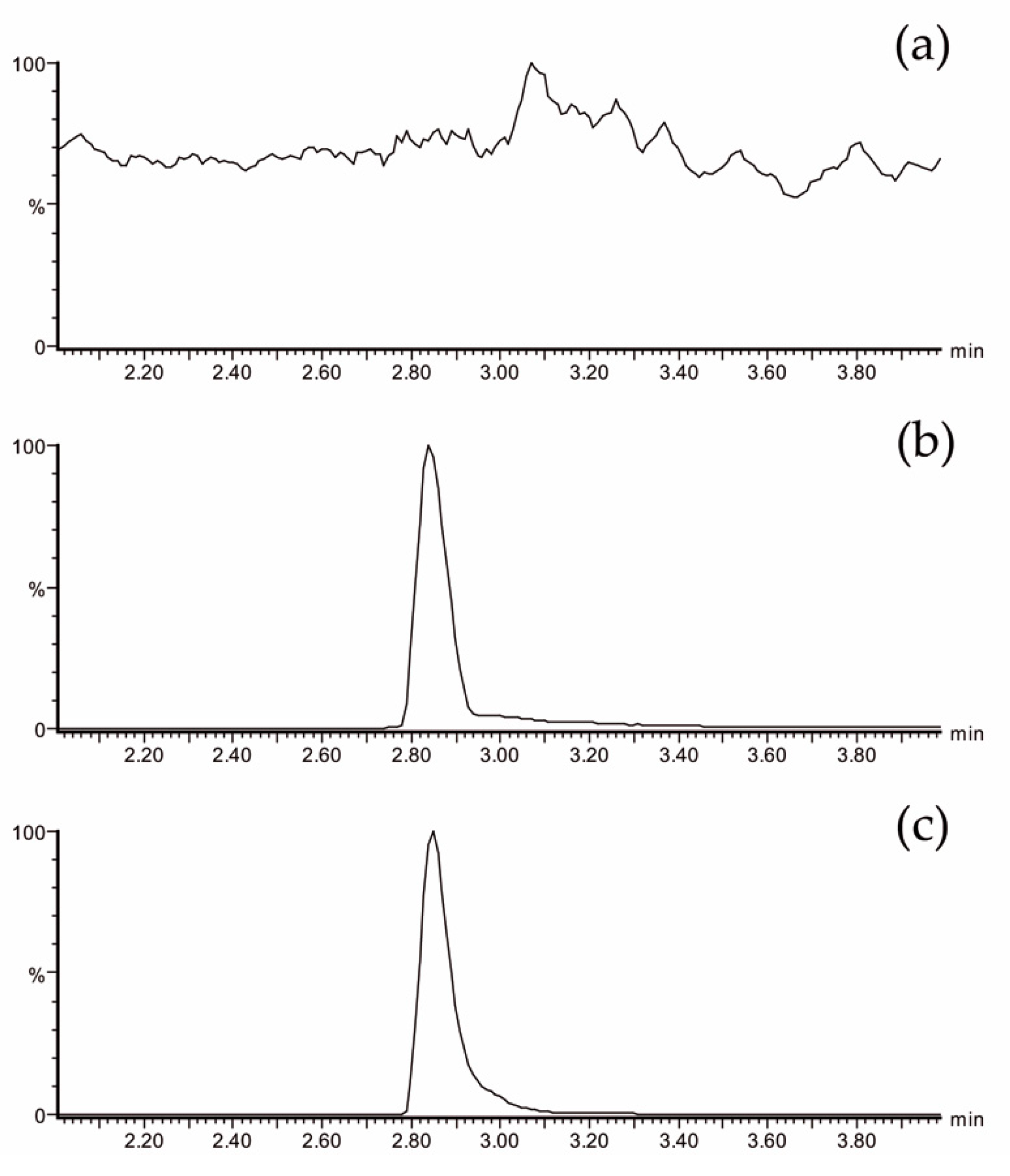
2.5.3. UPLC-ESI-MS/MS
2.6. Statistical Analysis
3. Results
3.1. Anthropometric Data of Participants and EGCG Administration
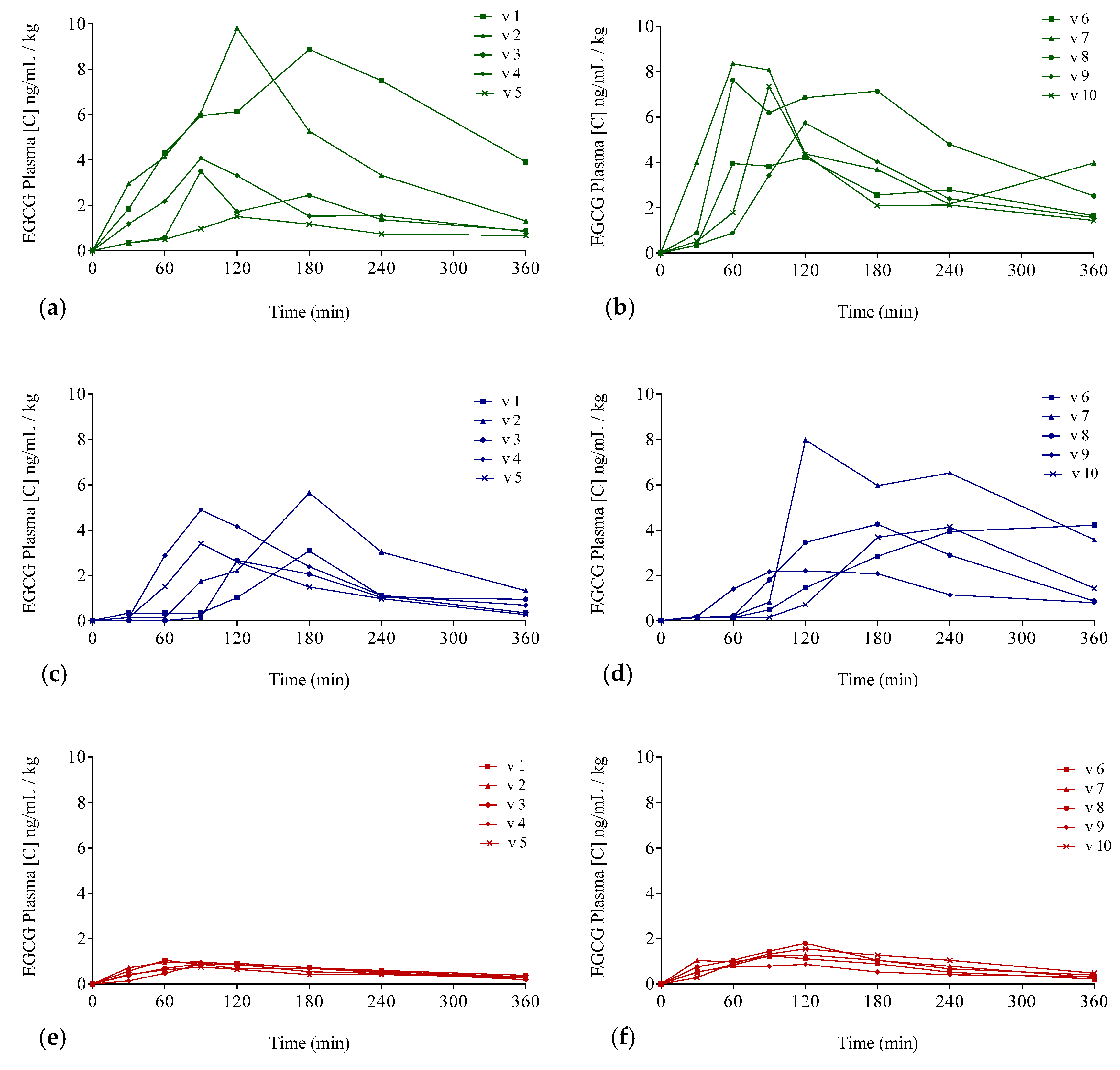
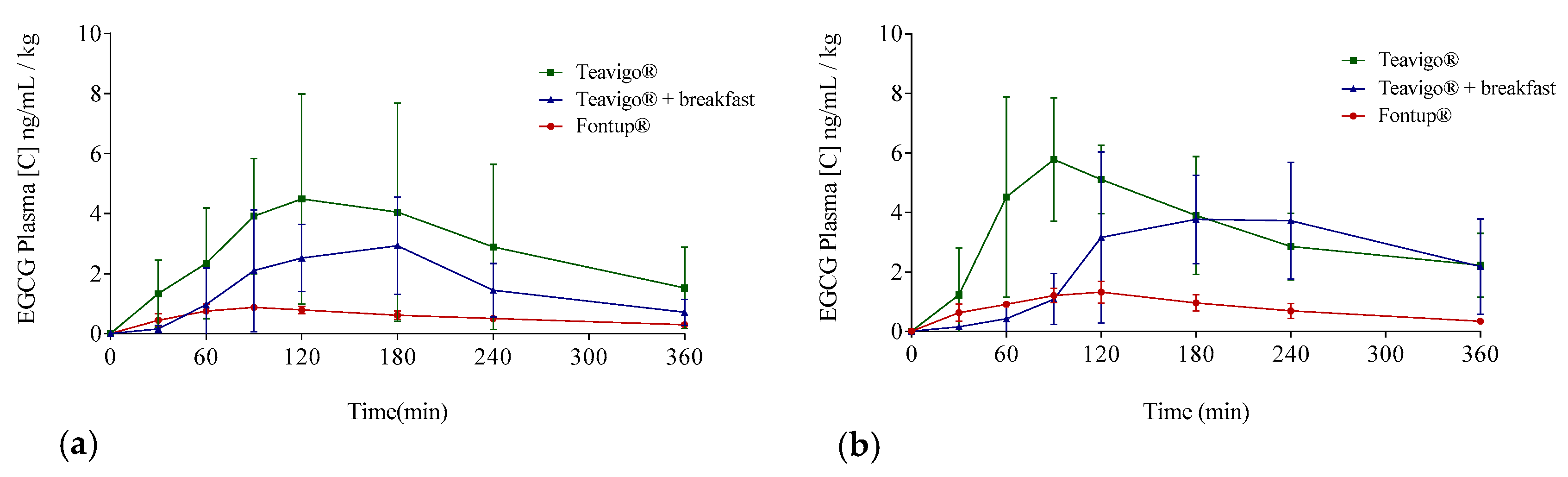
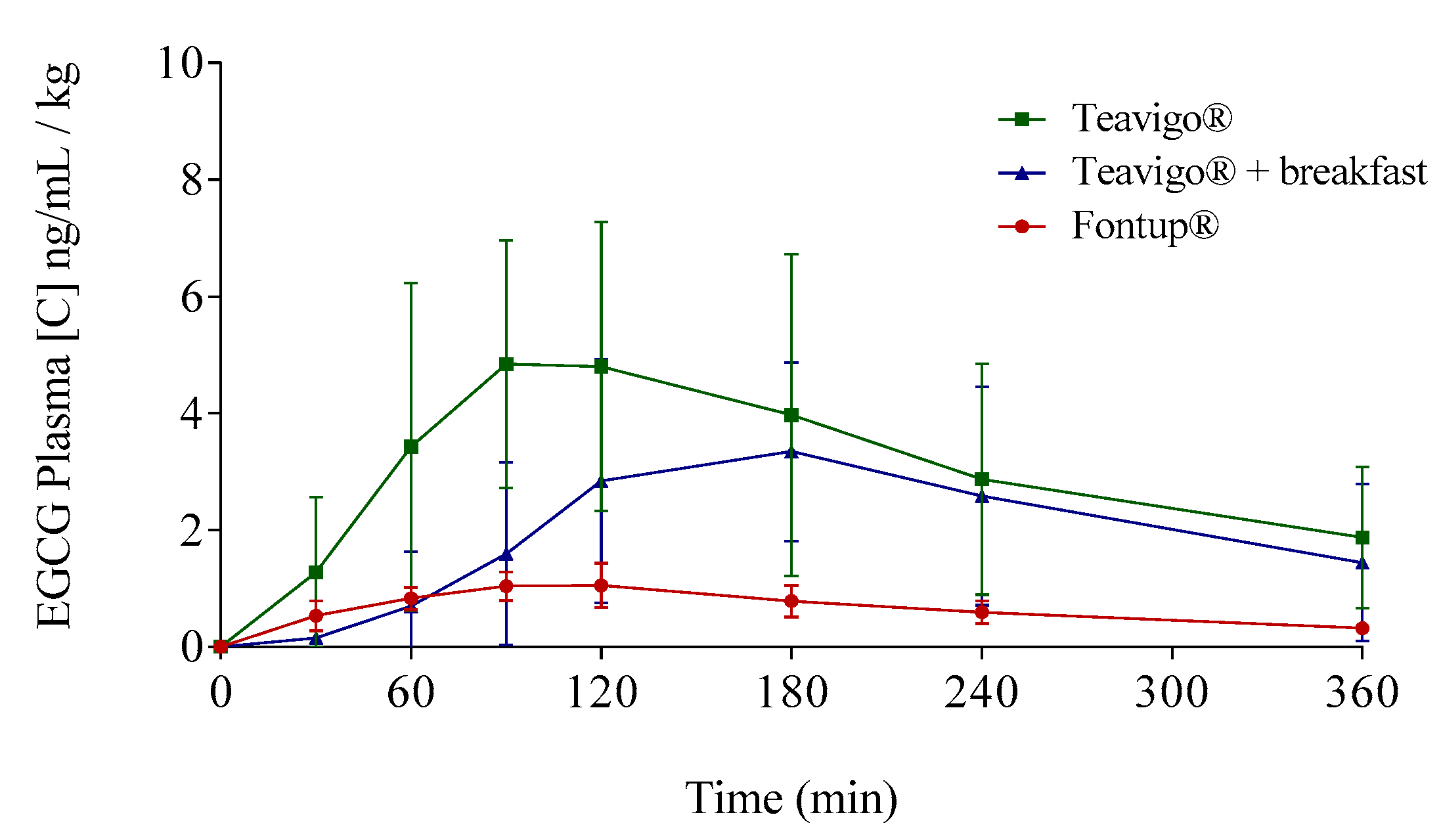
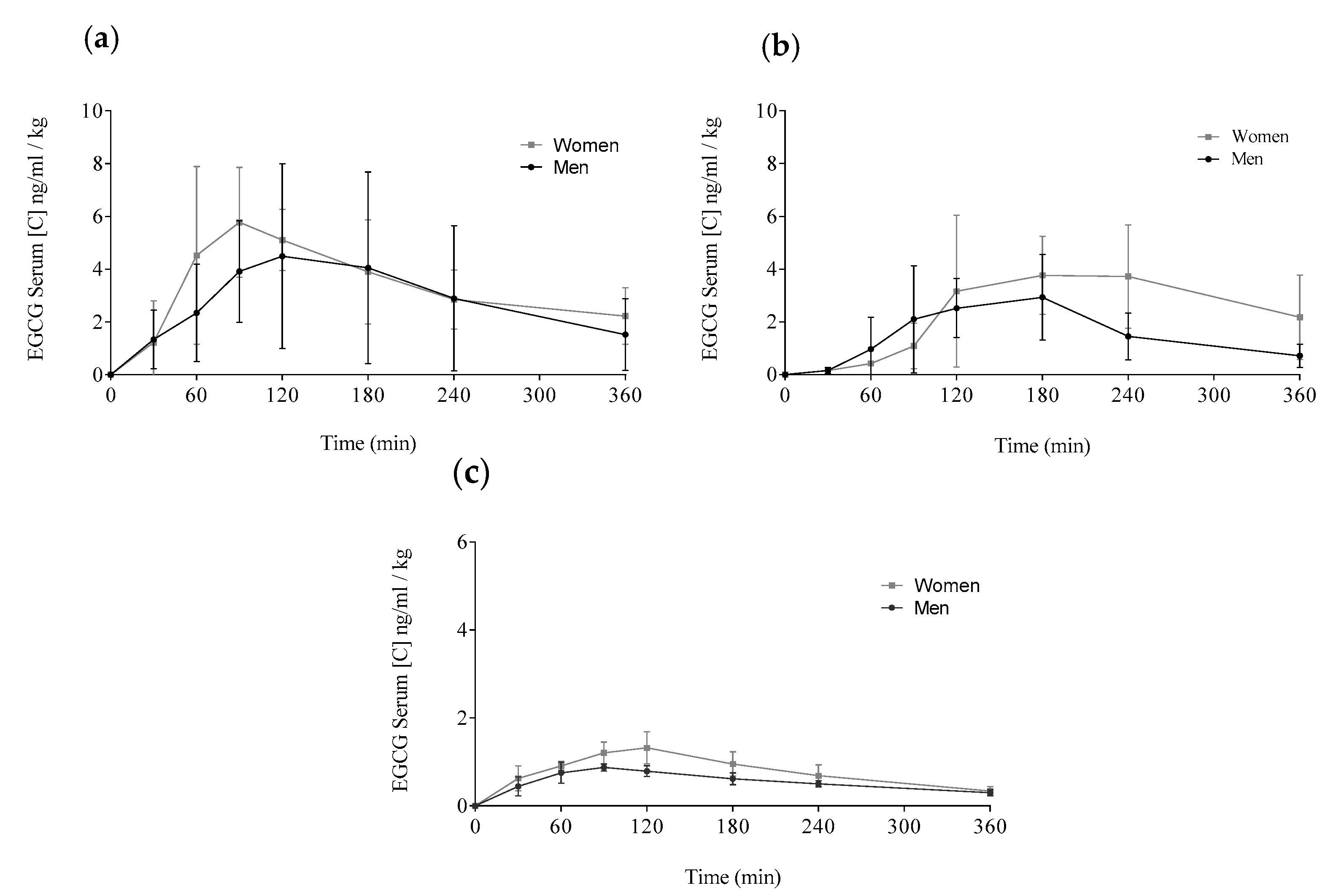
3.2. EGCG Concentration–Time Profiles in Plasma
3.3. Pharmacokinetic Parameters of EGCG in Plasma
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Average Analysis | Per 100 mL | Per Ration | |
|---|---|---|---|
| Energetic value (kJ/kcal) | 1606/383 | 787/188 | |
| Fats (g) | 11 | 5.4 | |
| Saturated (g) | 4.4 | 2.2 | |
| Monounsaturated (g) | 4.4 | 2.2 | |
| Polyunsaturated (g) | 2.2 | 1.1 | |
| Docosahexaenoic acid (DHA, mg) | 5.4 | 2.6 | |
| Carbohydrates (g) | 47 | 23 | |
| Dietary fiber (g) | 16 | 7.9 | |
| Fructo-oligosaccharides (g) | 3.1 | 1.5 | |
| Proteins (g) | 16 | 8 | |
| Salt (g) | 0.52 | 0.3 | |
| Minerals | |||
| Na (mg) | 206 | 101 | |
| K (mg) | 606 | 297 | |
| Cl (mg) | 395 | 194 | |
| Ca (mg) | 221 | 108 | |
| P (mg) | 209 | 102 | |
| Mg (mg) | 106 | 52 | |
| Fe (mg) | 4.6 | 2.3 | |
| Zn (mg) | 3.1 | 1.5 | |
| Cu (μg) | 0.5 | 0.2 | |
| Mn (mg) | 0.5 | 0.2 | |
| F (μg) | 0.1 | 0.05 | |
| Se (μg) | 10 | 4.9 | |
| Cr (μg) | 16 | 7.8 | |
| Mo (μg) | 10 | 4.9 | |
| I (μg) | 21 | 10 | |
| Vitamins | |||
| Vitamin A (μg) | 251 | 123 | |
| Vitamin D (μg) | 1.9 | 0.9 | |
| Vitamin E (mg) | 4.2 | 2.1 | |
| Vitamin K (μg) | 15.0 | 7.4 | |
| Vitamin C (mg) | 25 | 12 | |
| Thiamine (B1) (mg) | 0.3 | 0.1 | |
| Riboflavin (B2) (mg) | 0.4 | 0.2 | |
| Niacin (B3/PP) (mg) | 4.0 | 2.0 | |
| Vitamin B6 (mg) | 0.4 | 0.2 | |
| Folic acid (B9) (μg) | 80.0 | 39 | |
| Vitamin B12 (μg) | 0.5 | 0.2 | |
| Biotin (μg) | 58.0 | 28 | |
| Pantothenic acid (B5) (mg) | 1.9 | 0.9 | |
| Others | |||
| Green tea extract (mg) (minimum 250 mg EGCG) | 543 | 266 | |
| Osmolarity (mOsm/L) | 635 | ||
| Parameters | N | Teavigo® | Teavigo® with Breakfast | FontUp® |
|---|---|---|---|---|
| AUC0–360 (μg/mL/6 h) | ♂ ♀ | 270.4 ± 288.2 233.2 ± 76.1 | 108.6 ± 40.7 171.8 ± 77.7 | 38.5 ± 5.8 ** 54.7 ± 12.3 ** |
| Cmax (ng/mL) | ♂ ♀ | 528.6 ± 472.3 466.1 ± 116.3 | 275.3 ± 89.1 318.7 ± 147.0 | 63.7 ± 7.7 ** 94.5 ± 24.5 ** |
| Cav (ng/mL) | ♂ ♀ | 271.4 ± 299.2 256.0 ± 162.4 | 108.4 ± 102.3 144.8 ± 143.2 | 42.8 ± 16.6 ** 60.4 ± 27.4 ** |
| Cmin (ng/mL) | ♂ ♀ | 148.7 ± 188.1 155.8 ± 74.7 | 50.1 ± 30.6 152.4 ± 112.0 | 20.9 ± 4.8 * 23.8 ± 6.8 * |
| T1/2 (min) | ♂ ♀ | 154.2 ± 27.9 117.2 ± 53.5 | 93.1 ± 36.2 * 111.4 ± 39.1 | 191.7 ± 66.4 132.9 ± 27.8 |
| Tmax (min) | ♂ ♀ | 120 (90–180) 90 (60–120) | 120 (90–180) 180 (120–360) | 90 (60–90) 120 (90–120) |

References
- Saito, S.; Gosmann, G.; Pungartnik, C.; Brendel, M. Green Tea Extract-Patents and Diversity of Uses. Recent Patents Food, Nutr. Agric. 2009, 1, 203–215. [Google Scholar] [CrossRef] [PubMed]
- Chakrawarti, L.; Agrawal, R.; Dang, S.; Gupta, S.; Gabrani, R. Therapeutic effects of EGCG: A patent review. Expert Opin. Ther. Patents 2016, 26, 907–916. [Google Scholar] [CrossRef] [PubMed]
- Yang, C. Tea and health. Nutrition 1999, 15, 946–949. [Google Scholar] [CrossRef]
- Zaveri, N.T. Green tea and its polyphenolic catechins: Medicinal uses in cancer and noncancer applications. Life Sci. 2006, 78, 2073–2080. [Google Scholar] [CrossRef] [PubMed]
- Du, G.-J.; Zhang, Z.; Wen, X.-D.; Yu, C.; Calway, T.; Yuan, C.-S.; Wang, C.-Z. Epigallocatechin Gallate (EGCG) Is the Most Effective Cancer Chemopreventive Polyphenol in Green Tea. Nutrition 2012, 4, 1679–1691. [Google Scholar] [CrossRef] [PubMed]
- Williams, R.; Spencer, J.P. Flavonoids, cognition, and dementia: Actions, mechanisms, and potential therapeutic utility for Alzheimer disease. Free. Radic. Boil. Med. 2012, 52, 35–45. [Google Scholar] [CrossRef]
- Xicota, L.; Rodríguez-Morató, J.; Dierssen, M.; De La Torre, R. Potential Role of (−)-epigallocatechin-3-gallate (EGCG) in the Secondary Prevention of Alzheimer Disease. Curr. Drug Targets 2015, 18, 174–195. [Google Scholar] [CrossRef]
- Khan, N.; Mukhtar, H. Tea polyphenols for health promotion. Life Sci. 2007, 81, 519–533. [Google Scholar] [CrossRef] [Green Version]
- Moyers, S.B.; Kumar, N.B. Green tea polyphenols and cancer chemoprevention: Multiple mechanisms and endpoints for phase II trials. Nutr. Rev. 2004, 62, 204–211. [Google Scholar] [CrossRef]
- Higdon, J.V.; Frei, B. Tea catechins and polyphenols: Health effects, metabolism, and antioxidant functions. Crit. Rev. Food Sci. Nutr. 2003, 43, 89–143. [Google Scholar] [CrossRef]
- Fujiki, H.; Watanabe, T.; Sueoka, E.; Rawangkan, A.; Suganuma, M. Cancer Prevention with Green Tea and Its Principal Constituent, EGCG: From Early Investigations to Current Focus on Human Cancer Stem Cells. Mol. Cells 2018, 41, 73–82. [Google Scholar]
- Chen, D.; Wan, S.B.; Yang, H.; Yuan, J.; Chan, T.H.; Dou, Q.P. EGCG, green tea polyphenols and their synthetic analogs and prodrugs for human cancer prevention and treatment. Adv. Clin. Chem. 2011, 53, 155–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zamora-Ros, R.; Forouhi, N.G.; Sharp, S.J.; Gonzalez, C.A.; Buijsse, B.; Guevara, M.; Van Der Schouw, Y.T.; Amiano, P.; Boeing, H.; Bredsdorff, L.; et al. Dietary intakes of individual flavanols and flavonols are inversely associated with incident type 2 diabetes in European populations. J. Nutr. 2013, 144, 335–343. [Google Scholar] [CrossRef]
- Zhao, X.; Li, R.; Jin, H.; Jin, H.; Wang, Y.; Zhang, W.; Wang, H.; Chen, W. Epigallocatechin-3-gallate confers protection against corticosterone-induced neuron injuries via restoring extracellular signal-regulated kinase 1/2 and phosphatidylinositol-3 kinase/protein kinase B signaling pathways. PLoS ONE 2018, 13, e0192083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De La Torre, R.; De Sola, S.; Hernandez, G.; Farré, M.; Pujol, J.; Rodriguez, J.; Espadaler, J.M.; Langohr, K.; Cuenca-Royo, A.; Principe, A.; et al. Safety and efficacy of cognitive training plus epigallocatechin-3-gallate in young adults with Down’s syndrome (TESDAD): A double-blind, randomised, placebo-controlled, phase 2 trial. Lancet Neurol. 2016, 15, 801–810. [Google Scholar] [CrossRef]
- Arbones, M.L.; Thomazeau, A.; Nakano-Kobayashi, A.; Hagiwara, M.; Arbones, M.L. DYRK1A and cognition: A lifelong relationship. Pharmacol. Ther. 2019, 194, 199–221. [Google Scholar] [CrossRef]
- Lee, M.-J.; Maliakal, P.; Chen, L.; Meng, X.; Bondoc, F.Y.; Prabhu, S.; Lambert, G.; Mohr, S.; Yang, C.S. Pharmacokinetics of tea catechins after ingestion of green tea and (−)-epigallocatechin-3-gallate by humans: Formation of different metabolites and individual variability. Cancer Epidemiol. Biomark. Prev. 2002, 11, 1025–1032. [Google Scholar]
- Zeng, L.; Ma, M.; Li, C.; Luo, L. Stability of Tea Polyphenols Solution with Different pH at Different Temperatures. Int. J. Food Prop. 2016, 20, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Pervin, M.; Unno, K.; Takagaki, A.; Isemura, M.; Nakamura, Y. Function of Green Tea Catechins in the Brain: Epigallocatechin Gallate and its Metabolites. Int. J. Mol. Sci. 2019, 20, 3630. [Google Scholar] [CrossRef] [Green Version]
- Lu, H.; Meng, X.; Yang, C.S. Enzymology of methylation of tea catechins and inhibition of catechol-O-methyltransferase by (−)-epigallocatechin gallate. Drug Metab. Dispos. 2003, 31, 572–579. [Google Scholar] [CrossRef] [Green Version]
- Scholl, C.; Lepper, A.; Lehr, T.; Hanke, N.; Schneider, K.L.; Brockmöller, J.; Seufferlein, T.; Stingl, J. Population nutrikinetics of green tea extract. PLoS ONE 2018, 13, e0193074. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Taylor, L.S.; Mauer, L.J. Degradation Kinetics of Catechins in Green Tea Powder: Effects of Temperature and Relative Humidity. J. Agric. Food Chem. 2011, 59, 6082–6090. [Google Scholar] [CrossRef] [PubMed]
- Naumovski, N.; Blades, B.L.; Roach, P. Food Inhibits the Oral Bioavailability of the Major Green Tea Antioxidant Epigallocatechin Gallate in Humans. Antioxidants 2015, 4, 373–393. [Google Scholar] [CrossRef] [PubMed]
- Shirai, N.; Suzuki, H. Effects of Simultaneous Intakes of Fish Oil and Green Tea Extracts on Plasma, Glucose, Insulin, C-Peptide, and Adiponectin and on Liver Lipid Concentrations in Mice Fed Low- and High-Fat Diets. Ann. Nutr. Metab. 2008, 52, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Peters, C.M.; Green, R.J.; Janle, E.M.; Ferruzzi, M.G. Formulation with ascorbic acid and sucrose modulates catechin bioavailability from green tea. Food Res. Int. 2010, 43, 95–102. [Google Scholar] [CrossRef] [Green Version]
- Giunta, B.; Hou, H.; Zhu, Y.; Salemi, J.; Ruscin, A.; Shytle, R.D.; Tan, J. Fish oil enhances anti-amyloidogenic properties of green tea EGCG in Tg2576 mice. Neurosci. Lett. 2010, 471, 134–138. [Google Scholar] [CrossRef] [Green Version]
- Zhong, Y.; Shahidi, F. Lipophilized Epigallocatechin Gallate (EGCG) Derivatives as Novel Antioxidants. J. Agric. Food Chem. 2011, 59, 6526–6533. [Google Scholar] [CrossRef]
- Zhong, Y.; Ma, C.-M.; Shahidi, F. Antioxidant and antiviral activities of lipophilic epigallocatechin gallate (EGCG) derivatives. J. Funct. Foods 2012, 4, 87–93. [Google Scholar] [CrossRef]
- Zhong, Y.; Shahidi, F. Lipophilised epigallocatechin gallate (EGCG) derivatives and their antioxidant potential in food and biological systems. Food Chem. 2012, 131, 22–30. [Google Scholar] [CrossRef]
- Chao, J.; Lau, W.K.-W.; Huie, M.J.; Ho, Y.-S.; Yu, M.-S.; Lai, C.S.-W.; Wang, M.; Yuen, W.-H.; Lam, W.H.; Chan, T.H. A pro-drug of the green tea polyphenol (−)-epigallocatechin-3-gallate (EGCG) prevents differentiated SH-SY5Y cells from toxicity induced by 6-hydroxydopamine. Neurosci. Lett. 2010, 469, 360–364. [Google Scholar] [CrossRef] [Green Version]
- Mereles, D.; Hunstein, W. Epigallocatechin-3-gallate (EGCG) for Clinical Trials: More Pitfalls than Promises? Int. J. Mol. Sci. 2011, 12, 5592–5603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chow, H.H.; Cai, Y.; Alberts, D.S.; Hakim, I.; Dorr, R.; Shahi, F.; A Crowell, J.; Yang, C.S.; Hara, Y. Phase I pharmacokinetic study of tea polyphenols following single-dose administration of epigallocatechin gallate and polyphenon E. Cancer Epidemiol. Biomark. Prev. 2001, 10, 53–58. [Google Scholar] [PubMed]
- Kim, H.-S.; Quon, M.; Kim, J. New insights into the mechanisms of polyphenols beyond antioxidant properties; lessons from the green tea polyphenol, epigallocatechin 3-gallate. Redox Boil. 2014, 2, 187–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagle, D.G.; Ferreira, D.; Zhou, Y.-D. Epigallocatechin-3-gallate (EGCG): Chemical and biomedical perspectives. Phytochemistry 2006, 67, 1849–1855. [Google Scholar] [CrossRef] [Green Version]
- Lorenz, M.; Stangl, K.; Stangl, V. Addition of milk prevents vascular protective effects of tea: Reply. Eur. Hear. J. 2007, 28, 1266–1267. [Google Scholar] [CrossRef] [Green Version]
- Chow, H.-H.S.; Cai, Y.; Hakim, I.A.; A Crowell, J.; Shahi, F.; A Brooks, C.; Dorr, R.T.; Hara, Y.; Alberts, D.S. Pharmacokinetics and safety of green tea polyphenols after multiple-dose administration of epigallocatechin gallate and polyphenon E in healthy individuals. Clin. Cancer Res. 2003, 9, 3312–3319. [Google Scholar]
- Lambert, J.D.; Kennett, M.J.; Sang, S.; Reuhl, K.R.; Ju, J.; Yang, C.S. Hepatotoxicity of high oral dose (−)-epigallocatechin-3-gallate in mice. Food Chem. Toxicol. 2010, 48, 409–416. [Google Scholar] [CrossRef] [Green Version]
- EFSA Panel on Food Additives and Nutrient Sources added to Food (ANS); Younes, M.; Aggett, P.; Aguilar, F.; Crebelli, R.; Dusemund, B.; Filipič, M.; Frutos, M.J.; Galtier, P.; Gott, D.; et al. Scientific opinion on the safety of green tea catechins. EFSA J. 2018, 16, 05239. [Google Scholar] [CrossRef] [Green Version]
- Chow, H.-H.S.; Hakim, I.A.; Vining, D.R.; Crowell, J.A.; Ranger-Moore, J.; Chew, W.M.; Celaya, C.A.; Rodney, S.R.; Hara, Y.; Alberts, D.S. Effects of Dosing Condition on the Oral Bioavailability of Green Tea Catechins after Single-Dose Administration of Polyphenon E in Healthy Individuals. Clin. Cancer Res. 2005, 11, 4627–4633. [Google Scholar] [CrossRef] [Green Version]
- Roowi, S.; Stalmach, A.; Mullen, W.; Lean, M.E.J.; Edwards, C.A.; Crozier, A. Green Tea Flavan-3-ols: Colonic Degradation and Urinary Excretion of Catabolites by Humans. J. Agric. Food Chem. 2010, 58, 1296–1304. [Google Scholar] [CrossRef]
- Stalmach, A.; Troufflard, S.; Serafini, M.; Crozier, A. Absorption, metabolism and excretion of Choladi green tea flavan-3-ols by humans. Mol. Nutr. Food Res. 2008, 53, S44–S53. [Google Scholar] [CrossRef] [PubMed]
- Martí, M.-P.; Pantaleón, A.; Rózek, A.; Soler, A.; Fonayet, J.V.; Macià, A.; Romero, M.-P.; Motilva, M.J.; Romero-Fabregat, M.-P. Rapid analysis of procyanidins and anthocyanins in plasma by microelution SPE and ultra-HPLC. J. Sep. Sci. 2010, 33, 2841–2853. [Google Scholar] [CrossRef]
- Sauter, R.; Steinijans, V.W.; Diletti, E.; Böhm, A.; Schulz, H.U. Presentation of results from bioequivalence studies. Int. J. Clin. Pharmacol. Ther. Toxicol. 1992, 30, 233–256. [Google Scholar] [PubMed]
- Chen, M.; Shah, V.; Patnaik, R.; Adams, W.; Hussain, A.; Conner, D.; Mehta, M.; Malinowski, H.; Lazor, J.; Huang, S.; et al. Bioavailability and bioequivalence: An FDA regulatory overview. Pharm. Res. 2001, 18, 1645–1650. [Google Scholar] [CrossRef] [PubMed]
- De la Torre, R.; De Sola, S.; Pons, M.; Duchon, A.; de Lagran, M.M.; Farré, M.; Fitó, M.; Benejam, B.; Langohr, K.; Rodriguez, J. Epigallocatechin-3-gallate, a DYRK1A inhibitor, rescues cognitive deficits in D own syndrome mouse models and in humans. Mol. Nutr. Food Res. 2014, 58, 278–288. [Google Scholar] [CrossRef] [PubMed]
- Widlansky, M.E.; Hamburg, N.M.; Anter, E.; Holbrook, M.; Kahn, D.F.; Elliott, J.G.; Keaney, J.; Vita, J.A. Acute EGCG supplementation reverses endothelial dysfunction in patients with coronary artery disease. J. Am. Coll. Nutr. 2007, 26, 95–102. [Google Scholar] [CrossRef]
- Dostal, A.; Samavat, H.; Bedell, S.; Torkelson, C.J.; Wang, R.; Swenson, K.; Le, C.T.; Wu, A.H.; Ursin, G.; Yuan, J.-M.; et al. The safety of green tea extract supplementation in postmenopausal women at risk for breast cancer: Results of the Minnesota Green Tea Trial. Food Chem. Toxicol. 2015, 83, 26–35. [Google Scholar] [CrossRef] [Green Version]
- Kumar, N.B.; Pow-Sang, J.; Egan, K.M.; Spiess, P.E.; Dickinson, S.; Salup, R.; Helal, M.; McLarty, J.; Williams, C.R.; Schreiber, F.; et al. Randomized, Placebo-Controlled Trial of Green Tea Catechins for Prostate Cancer Prevention. Cancer Prev. Res. 2015, 8, 879–887. [Google Scholar] [CrossRef] [Green Version]
- Berletch, J.B.; Liu, C.; Love, W.K.; Andrews, L.G.; Katiyar, S.K.; Tollefsbol, T.O. Epigenetic and genetic mechanisms contribute to telomerase inhibition by EGCG. J. Cell. Biochem. 2008, 103, 509–519. [Google Scholar] [CrossRef] [Green Version]
- Cano, A.; Ettcheto, M.; Chang, J.-H.; Barroso, E.; Espina, M.; Kühne, B.A.; Barenys, M.; Auladell, C.; Folch, J.; Souto, E.B. Dual-drug loaded nanoparticles of Epigallocatechin-3-gallate (EGCG)/Ascorbic acid enhance therapeutic efficacy of EGCG in a APPswe/PS1dE9 Alzheimer’s disease mice model. J. Control. Release 2019, 301, 62–75. [Google Scholar] [CrossRef]
- McElyea, S.D.; Starbuck, J.M.; Tumbleson-Brink, D.M.; Harrington, E.; Blazek, J.D.; Ghoneima, A.; Kula, K.; Roper, R.J. Influence of prenatal EGCG treatment and Dyrk1a dosage reduction on craniofacial features associated with Down syndrome. Hum. Mol. Genet. 2016, 25, 4856–4869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.-K.; Cheung, C.; Reuhl, K.R.; Liu, A.B.; Lee, M.-J.; Lu, Y.-P.; Yang, C.S. Effects of green tea polyphenol (−)-epigallocatechin-3-gallate on newly developed high-fat/Western-style diet-induced obesity and metabolic syndrome in mice. J. Agric. Food Chem. 2011, 59, 11862–11871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borutinskaitė, V.; Virkšaitė, A.; Gudelytė, G.; Navakauskienė, R. Green tea polyphenol EGCG causes anti-cancerous epigenetic modulations in acute promyelocytic leukemia cells. Leuk. Lymphoma 2017, 59, 469–478. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, E.; Liu, D. Flavonoids influence epigenetic-modifying enzyme activity: Structure - function relationships and the therapeutic potential for cancer. Curr. Med. Chem. 2010, 17, 1756–1768. [Google Scholar] [CrossRef] [PubMed]
- Ullmann; Haller; Decourt; Girault; Spitzer; Weber Plasma-Kinetic Characteristics of Purified and Isolated Green Tea Catechin Epigallocatechin Gallate (EGCG) after 10 Days Repeated Dosing in Healthy Volunteers. Int. J. Vitam. Nutr. Res. 2004, 74, 269–278. [CrossRef]
- Chen, L.; Lee, M.J.; Li, H.; Yang, C.S. Absorption, distribution, elimination of tea polyphenols in rats. Drug Metab. Dispos. 1997, 25, 1045–1050. [Google Scholar]
- Altland, K.; Schreiner, R.; Hunstein, W. Of Green Tea, Black Pepper, and Amyloidoses. 2009. Available online: http://www.ukgm.de/ugm_2/deu/ugi_hum/EGCG_Piperin_engl.pdf (accessed on 5 February 2009).
- Record, I.R.; Lane, J.M. Simulated intestinal digestion of green and black teas. Food Chem. 2001, 73, 481–486. [Google Scholar] [CrossRef]
- Wang, R.; Zhou, W.; Jiang, X. Reaction Kinetics of Degradation and Epimerization of Epigallocatechin Gallate (EGCG) in Aqueous System over a Wide Temperature Range. J. Agric. Food Chem. 2008, 56, 2694–2701. [Google Scholar] [CrossRef]
- Proniuk, S.; Liederer, B.M.; Blanchard, J. Preformulation study of epigallocatechin gallate, a promising antioxidant for topical skin cancer prevention. J. Pharm. Sci. 2002, 91, 111–116. [Google Scholar] [CrossRef]
- Hunstein, W. AL-Amyloidosis and Epigallocatechin-3-Gallate: 4 Years and 5 Months Later. 2020. Available online: http://hunstein-egcg.de/en/al-egcg.html (accessed on 13 July 2011).
- Bose, M.; Hao, X.; Ju, J.; Park, S.; Husain, A.; Yang, C.S. Inhibition of intestinal tumorigenesis in ApcMin/+ mice by a combination of (−)-epigallocatechin-3-gallate (EGCG) with fish oil or calcium. Cancer Res. 2006, 66, 533–534. [Google Scholar]
- Warden, B.A.; Smith, L.S.; Beecher, G.R.; Balentine, D.A.; Clevidence, B.A. Catechins are bioavailable in men and women drinking black tea throughout the day. J. Nutr. 2001, 131, 1731–1737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakagawa, K.; Miyazawa, T. Chemiluminescence–High-Performance Liquid Chromatographic Determination of Tea Catechin, (−)-Epigallocatechin 3-Gallate, at Picomole Levels in Rat and Human Plasma. Anal. Biochem. 1997, 248, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.; Moroy, G.; Paul, J.-L.; Rebillat, A.-S.; Dierssen, M.; De La Torre, R.; Cieuta-Walti, C.; Dairou, J.; Janel, N. Molecular Rescue of Dyrk1A Overexpression Alterations in Mice with Fontup® Dietary Supplement: Role of Green Tea Catechins. Int. J. Mol. Sci. 2020, 21, 1404. [Google Scholar] [CrossRef] [PubMed] [Green Version]





| Nutrient | Weight (g) | % (w/w) 1 | kcal |
|---|---|---|---|
| Semi-skimmed milk + Soluble cocoa | 200 | 78.4 | 200 |
| Breakfast cereals | 30 | 11.8 | 120 |
| 2 bread toasts + 5 mL Olive oil | 25 | 9.8 | 160 |
| Total | 255 | 100 | 480 |
| Demographic Parameters | Total | Men | Women |
|---|---|---|---|
| Nº of participants | 10 | 5 | 5 |
| Age mean (years) | 29.7 ± 4.3 | 30.6 ± 5.2 | 28.8 ± 3.6 |
| Height (cm) | 169 ± 8.8 | 176 ± 5.0 | 163 ± 6.0 |
| Weight (kg) | 63.2 ± 14.4 | 73.8 ± 11.6 | 52.8 ± 7.0 |
| BMI 1 (kg/m2) | 21.8 ± 3.1 | 23.7 ± 2.8 | 19.9 ± 2.1 |
| Parameters | G | Teavigo® | Teavigo® with Breakfast | FontUp® |
|---|---|---|---|---|
| AUC0–360 (μg/mL/kg/6 h) | ♂ ♀ | 3.9 ± 4.1 3.3 ± 1.1 | 1.5 ± 0.6 2.4 ± 1.1 | 0.6 ± 0.1 ** 0.8 ± 0.2 ** |
| Cmax (ng/mL/kg) | ♂ ♀ | 5.9 ± 4.1 6.7 ± 1.7 | 3.9 ± 1.3 4.5 ± 2.1 | 0.9 ± 0.1 ** 1.3 ± 0.3 ** |
| Cav (ng/mL/kg) | ♂ ♀ | 3.0 ± 2.6 3.7 ± 2.3 | 1.5 ± 1.5 2.1 ± 2.0 | 0.6 ± 0.2 ** 0.9 ± 0.4 ** |
| Cmin (ng/mL/kg) | ♂ ♀ | 1.5 ± 1.4 2.2 ± 1.1 | 0.7 ± 0.4 2.2 ± 1.6 | 0.3 ± 0.1 * 0.3 ± 0.0 * |
| T1/2 (min) | ♂ ♀ | 154.2 ± 27.9 117.2 ± 53.5 | 93.1 ± 36.2 * 111.4 ± 39.1 | 191.7 ± 66.4 132.9 ± 27.9 |
| Tmax (min) | ♂ ♀ | 120 (90–180) 90 (60–120) | 120 (90–180) 180 (120–360) | 90 (60–90) 120 (90–120) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andreu Fernández, V.; Almeida Toledano, L.; Pizarro Lozano, N.; Navarro Tapia, E.; Gómez Roig, M.D.; De la Torre Fornell, R.; García Algar, Ó. Bioavailability of Epigallocatechin Gallate Administered with Different Nutritional Strategies in Healthy Volunteers. Antioxidants 2020, 9, 440. https://doi.org/10.3390/antiox9050440
Andreu Fernández V, Almeida Toledano L, Pizarro Lozano N, Navarro Tapia E, Gómez Roig MD, De la Torre Fornell R, García Algar Ó. Bioavailability of Epigallocatechin Gallate Administered with Different Nutritional Strategies in Healthy Volunteers. Antioxidants. 2020; 9(5):440. https://doi.org/10.3390/antiox9050440
Chicago/Turabian StyleAndreu Fernández, Vicente, Laura Almeida Toledano, Nieves Pizarro Lozano, Elisabet Navarro Tapia, María Dolores Gómez Roig, Rafael De la Torre Fornell, and Óscar García Algar. 2020. "Bioavailability of Epigallocatechin Gallate Administered with Different Nutritional Strategies in Healthy Volunteers" Antioxidants 9, no. 5: 440. https://doi.org/10.3390/antiox9050440
APA StyleAndreu Fernández, V., Almeida Toledano, L., Pizarro Lozano, N., Navarro Tapia, E., Gómez Roig, M. D., De la Torre Fornell, R., & García Algar, Ó. (2020). Bioavailability of Epigallocatechin Gallate Administered with Different Nutritional Strategies in Healthy Volunteers. Antioxidants, 9(5), 440. https://doi.org/10.3390/antiox9050440