
Exhaled Hydrogen as a Marker of Intestinal Fermentation Is Associated with Diarrhea in Kidney Transplant Recipients

 , , , ,
, , , ,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
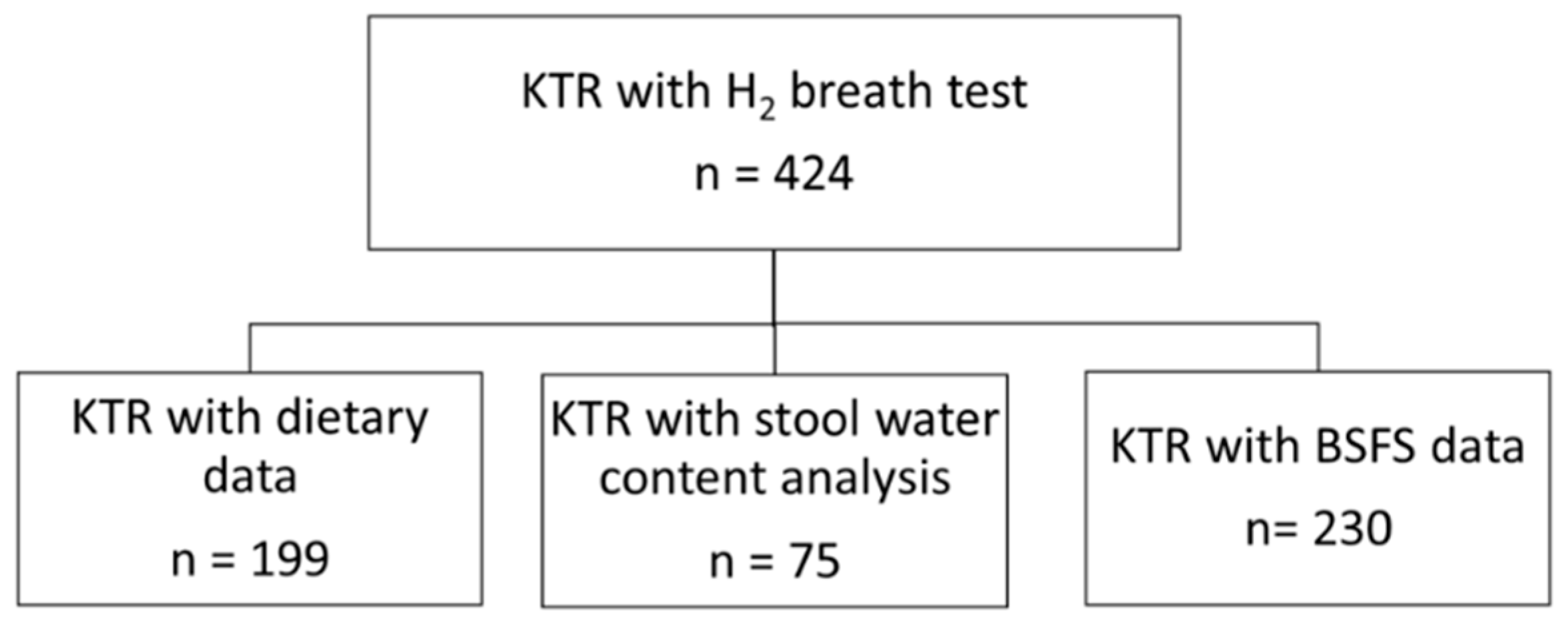
2.1. Clinical Data
2.2. Breath H2 Measurement
2.3. Stool Water Content Measurement
2.4. Diarrhea Classification
2.5. Dietary Assessment
2.6. Statistical Analyses
3. Results
3.1. Clinical Parameters
3.2. Determinants of Exhaled H2
3.3. H2 and Diarrhea
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| BMI | Body Mass Index |
| BSFS | Bristol Stool Form Scale |
| CH4 | Methane |
| CKD | Chronic Kidney Disease |
| eGFR | Estimated glomerular filtration rate |
| FFQ | Food Frequency Questionnaire |
| GI | Gastrointestinal |
| H2 | Hydrogen |
| IBS | Irritable bowel syndrome |
| KTR | Kidney Transplant Recipients |
| MMF | Mycophenolate mofetil |
| PPI | Proton-pump inhibitors |
| RS | Resistant starch |
| SCFA | Short-chain Fatty Acids |
| SIBO | Small Intestinal Bacterial Overgrowth |
References
- Eisenga, M.F.; Gomes-Neto, A.W.; Van Londen, M.; Ziengs, A.L.; Douwes, R.M.; Stam, S.P.; Osté, M.C.J.; Knobbe, T.J.; Hessels, N.R.; Buunk, A.M.; et al. Rationale and design of TransplantLines: A prospective cohort study and biobank of solid organ transplant recipients. BMJ Open 2018, 8, e024502. [Google Scholar] [CrossRef] [PubMed]
- U.S. National Library Medicine. TransplantLines: The Transplantation Biobank. 2015. Available online: https://clinicaltrials.gov/ct2/show?term=transplantlines&rank=1 (accessed on 20 April 2021).
- Corpa, M.V.N.; Soares, V. Systemic hypertension in patients with glomerulonephritis. Renal. Fail. 2002, 24, 347–352. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 2003, 26 (Suppl. 1), S5–S20. [Google Scholar] [CrossRef] [Green Version]
- Du Bois, D.; Du Bois, E.F. A formula to estimate the approximate surface area if height and weight be known. 1916. Nutrition 1989, 5, 303. [Google Scholar] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gómez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.-C.; Pirlich, M.; et al. Bioelectrical impedance analysis—part II: Utilization in clinical practice. Clin. Nutr. 2004, 23, 1430–1453. [Google Scholar] [CrossRef]
- Sabaté, J.-M.; Jouët, P.; Harnois, F.; Mechler, C.; Msika, S.; Grossin, M.; Coffin, B. High Prevalence of Small Intestinal Bacterial Overgrowth in Patients with Morbid Obesity: A Contributor to Severe Hepatic Steatosis. Obes. Surg. 2008, 18, 371–377. [Google Scholar] [CrossRef]
- Saad, R.J.; Chey, W.D. Breath Testing for Small Intestinal Bacterial Overgrowth: Maximizing Test Accuracy. Clin. Gastroenterol. Hepatol. 2014, 12, 1964–1972. [Google Scholar] [CrossRef]
- Romagnuolo, J.; Schiller, D.; Bailey, R.J. Using breath tests wisely in a gastroenterology practice: An evidence-based review of indications and pitfalls in interpretation. Am. J. Gastroenterol. 2002, 97, 1113–1126. [Google Scholar] [CrossRef]
- Kerckhoffs, A.P.M.; Visser, M.R.; Samsom, M.; Van Der Rest, M.E.; De Vogel, J.; Harmsen, W.; Akkermans, L.M.A. Critical Evaluation of Diagnosing Bacterial Overgrowth in the Proximal Small Intestine. J. Clin. Gastroenterol. 2008, 42, 1095–1102. [Google Scholar] [CrossRef]
- Levitt, M.; Hirsh, P.; Fetzer, C.; Sheahan, M.; Levine, A. H2 excretion after ingestion of complex carbohydrates. Gastroenterology 1987, 92, 383–389. [Google Scholar] [CrossRef]
- Ohno, H.; Murakami, H.; Tanisawa, K.; Konishi, K.; Miyachi, M. Validity of an observational assessment tool for multifaceted evaluation of faecal condition. Sci. Rep. 2019, 9, 3760. [Google Scholar] [CrossRef] [PubMed]
- Hinnant, R.T.; Kothmann, M.M. Collecting, Drying, and Preserving Feces for Chemical and Microhistological Analysis. J. Range Manag. 1988, 41, 168. [Google Scholar] [CrossRef]
- Heaton, K.W.; Radvan, J.; Cripps, H.; Mountford, R.A.; Braddon, F.E.; Hughes, A.O. Defecation frequency and timing, and stool form in the general population: A prospective study. Gut 1992, 33, 818–824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van den Berg, E.; Engberink, M.F.; Brink, E.J.; van Baak, M.; Gans, R.; Navis, G.; Bakker, S.J.L. Dietary protein, blood pressure and renal function in renal transplant recipients. Br. J. Nutr. 2012, 109, 1463–1470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Netherlands Nutrition Center. Dutch Food Composition Table 2006 NEVO-Tabel. 2006. Available online: https://www.rivm.nl/nederlands-voedingsstoffenbestand (accessed on 23 April 2021).
- Willett, W.C.; Howe, G.R.; Kushi, L.H. Adjustment for total energy intake in epidemiologic studies. Am. J. Clin. Nutr. 1997, 65 (Suppl. 4), 1220S–1228S. [Google Scholar] [CrossRef] [PubMed]
- Bunnapradist, S.; Neri, L.; Wong, W.; Lentine, K.L.; Burroughs, T.E.; Pinsky, B.W.; Takemoto, S.K.; Schnitzler, M.A. Incidence and Risk Factors for Diarrhea Following Kidney Transplantation and Association With Graft Loss and Mortality. Am. J. Kidney Dis. 2008, 51, 478–486. [Google Scholar] [CrossRef] [Green Version]
- Aulagnon, F.; Scemla, A.; DeWolf, S.; Legendre, C.; Zuber, J. Diarrhea After Kidney Transplantation: A new look at a frequent symptom. Transplantation 2014, 98, 806–816. [Google Scholar] [CrossRef]
- Ekberg, H.; Kyllonen, L.; Madsen, S.; Grave, G.; Solbu, D.; Holdaas, H. Increased prevalence of gastrointestinal symptoms associated with impaired quality of life in renal transplant recipients. Transplantation 2007, 83, 282–289. [Google Scholar] [CrossRef]
- Shin, H.S.; Chandraker, A. Causes and management of postrenal transplant diarrhea: An underappreciated cause of transplant-associated morbidity. Curr. Opin. Nephrol. Hypertens. 2017, 26, 484–493. [Google Scholar] [CrossRef]
- Lee, J.R.; Magruder, M.; Zhang, L.; Westblade, L.F.; Satlin, M.J.; Robertson, A.; Edusei, E.; Crawford, C.; Ling, L.; Taur, Y.; et al. Gut microbiota dysbiosis and diarrhea in kidney transplant recipients. Am. J. Transplant. 2019, 19, 488–500. [Google Scholar] [CrossRef] [Green Version]
- Zinsmeister, A.R.; Herrick, L.M.; Saito Loftus, Y.A.; Schleck, C.D.; Talley, N.J. Identification and validation of functional gastrointestinal disorder subtypes using latent class analysis: A population-based study. Scand. J. Gastroenterol. 2017, 53, 549–558. [Google Scholar] [CrossRef]
- Scallan, E.; Majowicz, S.; Hall, G.; Banerjee, A.; Bowman, C.; Daly, L.; Jones, T.F.; Kirk, M.D.; Fitzgerald, M.; Angulo, F.J. Prevalence of diarrhoea in the community in Australia, Canada, Ireland, and the United States. Int. J. Epidemiol. 2005, 34, 454–460. [Google Scholar] [CrossRef]
- Knight, S.R.; Russell, N.K.; Barcena, L.; Morris, P.J. Mycophenolate Mofetil Decreases Acute Rejection and may Improve Graft Survival in Renal Transplant Recipients When Compared with Azathioprine: A Systematic Review. Transplantation 2009, 87, 785–794. [Google Scholar] [CrossRef] [Green Version]
- Ghoshal, U.C. How to Interpret Hydrogen Breath Tests. J. Neurogastroenterol. Motil. 2011, 17, 312–317. [Google Scholar] [CrossRef] [Green Version]
- Ghoshal, U.C.; Srivastava, D.; Ghoshal, U.; Misra, A. Breath tests in the diagnosis of small intestinal bacterial overgrowth in patients with irritable bowel syndrome in comparison with quantitative upper gut aspirate culture. Eur. J. Gastroenterol. Hepatol. 2014, 26, 753–760. [Google Scholar] [CrossRef] [PubMed]
- Pyleris, E.; Giamarellos-Bourboulis, E.J.; Tzivras, D.; Koussoulas, V.; Barbatzas, C.; Pimentel, M. The Prevalence of Overgrowth by Aerobic Bacteria in the Small Intestine by Small Bowel Culture: Relationship with Irritable Bowel Syndrome. Dig. Dis. Sci. 2012, 57, 1321–1329. [Google Scholar] [CrossRef] [PubMed]
- Sahakian, A.B.; Jee, S.-R.; Pimentel, M. Methane and the Gastrointestinal Tract. Dig. Dis. Sci. 2009, 55, 2135–2143. [Google Scholar] [CrossRef]
- Corazza, G.R.; Strocchi, A.; Gasbarrini, G. Fasting breath hydrogen in celiac disease. Gastroenterology 1987, 93, 53–58. [Google Scholar] [CrossRef]
- Perman, J.A.; Modler, S.; Barr, R.G.; Rosenthal, P. Fasting breath hydrogen concentration: Normal values and clinical application. Gastroenterology 1984, 87, 1358–1363. [Google Scholar] [CrossRef]
- Jahng, J.; Jung, I.S.; Choi, E.J.; Conklin, J.L.; Park, H. The effects of methane and hydrogen gases produced by enteric bacteria on ileal motility and colonic transit time. Neurogastroenterol. Motil. 2011, 24, 185-e92. [Google Scholar] [CrossRef]
- Su, T.; Lai, S.; Lee, A.; He, X.; Chen, S. Meta-analysis: Proton pump inhibitors moderately increase the risk of small intestinal bacterial overgrowth. J. Gastroenterol. 2017, 53, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Laine, L.; Ahnen, D.; McClain, C.; Solcia, E.; Walsh, J.H. Review article: Potential gastrointestinal effects of long-term acid suppression with proton pump inhibitors. Aliment. Pharmacol. Ther. 2000, 14, 651–668. [Google Scholar] [CrossRef] [PubMed]
- Kashyap, P.C.; Marcobal, A.; Ursell, L.K.; Larauche, M.; Duboc, H.; Earle, K.A.; Sonnenburg, E.D.; Ferreyra, J.A.; Higginbottom, S.K.; Million, M.; et al. Complex Interactions Among Diet, Gastrointestinal Transit, and Gut Microbiota in Humanized Mice. Gastroenterology 2013, 144, 967–977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slavin, J.L. Carbohydrates, Dietary Fiber, and Resistant Starch in White Vegetables: Links to Health Outcomes. Adv. Nutr. 2013, 4, 351S–355S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saffouri, G.B.; Shields-Cutler, R.R.; Chen, J.; Yang, Y.; Lekatz, H.R.; Hale, V.L.; Cho, J.M.; Battaglioli, E.J.; Bhattarai, Y.; Thompson, K.J.; et al. Small intestinal microbial dysbiosis underlies symptoms associated with functional gastrointestinal disorders. Nat. Commun. 2019, 10, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levitt, M.D. Malabsorption of starch: A normal phenomenon. Gastroenterology 1983, 85, 769–770. [Google Scholar] [CrossRef]
- Hammer, H.F.; Hammer, J. Diarrhea Caused By Carbohydrate Malabsorption. Gastroenterol. Clin. N. Am. 2012, 41, 611–627. [Google Scholar] [CrossRef]
- Bello-Perez, L.A.; Flores-Silva, P.C.; Agama-Acevedo, E.; Tovar, J. Starch digestibility: Past, present, and future. J. Sci. Food Agric. 2018, 100, 5009–5016. [Google Scholar] [CrossRef]
- Ho Do, M.; Seo, Y.S.; Park, H.-Y. Polysaccharides: Bowel health and gut microbiota. Crit. Rev. Food Sci. Nutr. 2021, 61, 1212–1224. [Google Scholar] [CrossRef]
- DeMartino, P.; Cockburn, D.W. Resistant starch: Impact on the gut microbiome and health. Curr. Opin. Biotechnol. 2020, 61, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Swarte, J.C.; Douwes, R.M.; Hu, S.; Vila, A.V.; Eisenga, M.F.; Van Londen, M.; Gomes-Neto, A.W.; Weersma, R.K.; Harmsen, H.J.; Bakker, S.J. Characteristics and Dysbiosis of the Gut Microbiome in Renal Transplant Recipients. J. Clin. Med. 2020, 9, 386. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.R.; Muthukumar, T.; Dadhania, D.; Toussaint, N.C.; Ling, L.; Pamer, E.; Suthanthiran, M. Gut Microbial Community Structure and Complications After Kidney Transplantation. Transplantation 2014, 98, 697–705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, H.C. Small intestinal bacterial overgrowth: A framework for understanding irritable bowel syndrome. JAMA 2004, 292, 852–858. [Google Scholar] [CrossRef] [PubMed]
- Knobbe, T.J.; Douwes, R.M.; Kremer, D.; Swarte, J.C.; Eisenga, M.F.; Gomes-Neto, A.W.; Van Londen, M.; Peters, F.T.M.; Blokzijl, H.; Nolte, I.M.; et al. Altered Gut Microbial Fermentation and Colonization with Methanobrevibacter smithii in Renal Transplant Recipients. J. Clin. Med. 2020, 9, 518. [Google Scholar] [CrossRef] [Green Version]
- Rezaie, A.; Buresi, M.; Lembo, A.; Lin, H.; McCallum, R.; Rao, S.; Schmulson, M.; Valdovinos, M.; Zakko, S.; Pimentel, M. Hydrogen and Methane-Based Breath Testing in Gastrointestinal Disorders: The North American Consensus. Am. J. Gastroenterol. 2017, 112, 775–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Baseline Characteristics | Total (n = 424) | Exhaled H2, per Group | ||
|---|---|---|---|---|
| 1.0–6.9 ppm (n = 151) | 7.0–19.9 ppm (n = 139) | ≥20.0 ppm (n = 134) | ||
| Fermentation Parameter | ||||
| H2, ppm | 11 (5.0–25.0) | 4.0 (2.0–5.0) | 11.0 (8.0–15.0) b | 33.5 (26.0–49.0) ab |
| Demographics | ||||
| Age, years | 55.4 ± 13.2 | 55.4 ± 13.7 | 57.2 ± 12.1 | 53.7 ± 13.5 |
| Sex (male), n (%) | 258 (60.8) | 86 (57.0) | 84 (62.7) | 88 (63.3) |
| Transplant vintage, years | 1.8 (1.0–7.1) | 2.0 (1.0–8.1) | 1.0 (0.6–5.0) | 1.1 (0.8–7.8) |
| History of allograft rejection, n (%) | 69 (16.3) | 27 (17.8) | 19 (14.2) | 23 (16.5) |
| Body Composition | ||||
| Body mass index, kg/m2 | 27.7 ± 4.8 | 28.2 ± 5.6 | 28.1 ± 4.6 | 26.8 ± 3.9 a |
| Waist circumference, cm | 99.5 ± 13.2 | 100.8 ± 13.6 | 100.8 ± 13.4 | 96.9 ± 12.1 ab |
| Body fat percentage, % | 31.1 ± 9.8 | 32.3 ± 10.3 | 31.6 ± 9.8 | 29.3 ± 9.0 a |
| Immunosuppressive Drug Use | ||||
| MMF, n (%) | 311 (73.3) | 113 (74.8) | 100 (74.6) | 98 (70.5) |
| Tacrolimus, n (%) | 333 (78.5) | 111 (73.5) | 112 (83.5) | 110 (79.1) |
| Cyclosporine, n (%) | 38 (9.0) | 17 (11.3) | 12 (8.9) | 9 (6.5) |
| Everolimus, n (%) | 10 (2.4) | 5 (3.3) | 3 (2.2) | 2 (1.4) |
| Prednisolone, n (%) | 396 (93.4) | 141 (93.4) | 124 (92.5) | 131 (94.2) |
| Azathioprine, n (%) | 24 (5.7) | 8 (5.3) | 6 (4.5) | 10 (7.2) |
| Immunosuppressive Drug Trough Levels | ||||
| MMF, ug/L | 2.3 ± 1.6 | 2.2 ± 1.7 | 2.2 ±1.4 | 2.5 ± 1.8 |
| Tacrolimus, ug/L | 6.3 ± 2.5 | 5.9 ± 2.3 | 6.1 ± 2.2 | 6.8 ± 2.4 a |
| Lifestyle | ||||
| Current smoker, n (%) | 13 (3.1) | 7 (4.6) | 4 (3.0) | 2 (1.4) |
| Alcohol consumption, g/day | 1.5 (0.0–7.9) | 1.7 (0.0–7.3) | 1.0 (0.2–9.2) | 1.6 (0.0–7.6) |
| Glucose Homeostasis | ||||
| Diabetes mellitus, n (%) | 82 (19.3) | 28 (18.5) | 32 (23.0) | 22 (16.4) |
| Plasma glucose, mmol/L | 6.1 ± 1.7 | 6.2 ± 1.6 | 6.1 ± 1.8 | 6.0 ± 1.8 |
| HbA1c, % | 6.0 ± 1.7 | 6.0 ± 0.9 | 6.0 ± 0.8 | 5.9 ± 0.9 |
| Lipids | ||||
| Total cholesterol, mmol/L | 4.6 ± 1.0 | 4.7 ± 1.0 | 4.7 ± 1.0 | 4.4 ± 1.1 |
| HDL-cholesterol, mmol/L | 1.3 ± 0.4 | 1.4 ± 0.4 | 1.4 ± 0.4 | 1.3 ± 0.4 |
| LDL-cholesterol, mmol/L | 2.9 ± 0.9 | 2.9 ± 0.9 | 3.0 ± 0.9 | 2.7 ± 0.9 |
| Triglycerides, mmol/L | 1.8 ± 0.8 | 1.9 ± 0.9 | 1.9 ± 0.8 | 1.8 ± 0.9 |
| Cardiovascular | ||||
| SBP, mmHg | 137.4 ± 16.9 | 137.9 ± 16.2 | 137.2 ± 16.6 | 137.1 ± 16.6 |
| DBP, mmHg | 79.9 ± 11.1 | 79.8 ± 10.7 | 80.2 ± 11.1 | 79.6 ± 11.4 |
| Kidney Function | ||||
| eGFR, mL/min/1.73 m2 | 49.8 ± 19.1 | 49.3 ± 18.9 | 49.5 ± 18.2 | 50.4 ± 5.9 |
| Creatinine, µmol/L | 155.3 ± 124.3 | 149.9 ± 92.2 | 152.4 ± 110.9 | 163.9 ± 161.6 |
| Urinary protein excretion, g/24 h | 0.1 ± 0.2 | 0.2 ± 0.3 | 0.1 ± 0.1 | 0.1 ± 0.2 |
| Medication | ||||
| Proton pump inhibitors, n (%) | 306 (72.2) | 96 (63.5) | 105 (78.4) a | 105 (75.5) a |
| Statins, n (%) | 220 (51.9) | 80 (53.0) | 72 (53.7) | 68 (48.9) |
| Antihypertensive, n (%) | 311 (73.3) | 106 (70.2) | 105 (78.4) | 100 (71.9) |
| Diarrhea according to BSFS, n (%) * | 76 (33.0) | 24 (27.9) | 25 (36.2) | 27 (36.0) |
| Evacuation episodes, n/day * | 2.1 ± 1.3 | 2.2 ± 1.3 | 2.2 ± 1.3 | 2.1 ± 1.3 |
| Stool water content, % ** | 75.4 ± 6.3 | 73.8 ± 6.0 | 75.8 ± 7.0 | 77.7 ± 5.5 c |
| Potential Determinants | Univariate | Multivariate * | ||
|---|---|---|---|---|
| Std. β | p | Std. β | p | |
| Polysaccharides intake, g | 0.266 | <0.001 | 0.243 | 0.01 |
| Proton pump inhibitor use | 0.160 | <0.01 | 0.164 | 0.05 |
| Mono and disaccharides intake, g | −0.188 | 0.01 | ||
| Tacrolimus trough levels, ug/L | 0.133 | 0.02 | ||
| Vitamin C intake, mg | −0.162 | 0.02 | ||
| Total cholesterol, mmol/L | −0.106 | 0.03 | ||
| LDL-cholesterol, mmol/L | −0.101 | 0.04 | ||
| Waist circumference, cm | −0.098 | 0.05 | ||
| Variable | OR (95% CI) | p |
|---|---|---|
| Log2 exhaled H2, ppm | 1.51 (1.07–2.14) | 0.02 |
| Sex (male) | 1.10 (0.41–2.99) | 0.85 |
| eGFR, mL/min/1.73 m2 | 0.95 (0.92–0.99) | 0.01 |
| Transplant vintage, years | 0.99 (0.99–1.01) | 0.08 |
| MMF use | 4.71 (1.24–17.77) | 0.02 |
| Tacrolimus use | 0.25 (0.05–1.22) | 0.09 |
| PPI, use | 1.09 (0.37–3.30) | 0.86 |
| Polysaccharides intake, g | 0.99 (0.98–1.01) | 0.12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodrigues, F.G.; Swarte, J.C.; Douwes, R.M.; Knobbe, T.J.; Sotomayor, C.G.; Blokzijl, H.; Weersma, R.K.; Heilberg, I.P.; Bakker, S.J.L.; de Borst, M.H.; et al. Exhaled Hydrogen as a Marker of Intestinal Fermentation Is Associated with Diarrhea in Kidney Transplant Recipients. J. Clin. Med. 2021, 10, 2854. https://doi.org/10.3390/jcm10132854
Rodrigues FG, Swarte JC, Douwes RM, Knobbe TJ, Sotomayor CG, Blokzijl H, Weersma RK, Heilberg IP, Bakker SJL, de Borst MH, et al. Exhaled Hydrogen as a Marker of Intestinal Fermentation Is Associated with Diarrhea in Kidney Transplant Recipients. Journal of Clinical Medicine. 2021; 10(13):2854. https://doi.org/10.3390/jcm10132854
Chicago/Turabian StyleRodrigues, Fernanda Guedes, J. Casper Swarte, Rianne M. Douwes, Tim J. Knobbe, Camilo G. Sotomayor, Hans Blokzijl, Rinse K. Weersma, Ita P. Heilberg, Stephan J. L. Bakker, Martin H. de Borst, and et al. 2021. "Exhaled Hydrogen as a Marker of Intestinal Fermentation Is Associated with Diarrhea in Kidney Transplant Recipients" Journal of Clinical Medicine 10, no. 13: 2854. https://doi.org/10.3390/jcm10132854
APA StyleRodrigues, F. G., Swarte, J. C., Douwes, R. M., Knobbe, T. J., Sotomayor, C. G., Blokzijl, H., Weersma, R. K., Heilberg, I. P., Bakker, S. J. L., de Borst, M. H., & TransplantLines Investigators. (2021). Exhaled Hydrogen as a Marker of Intestinal Fermentation Is Associated with Diarrhea in Kidney Transplant Recipients. Journal of Clinical Medicine, 10(13), 2854. https://doi.org/10.3390/jcm10132854