
Non-Renal Risk Factors for Chronic Kidney Disease in Liver Recipients with Functionally Intact Kidneys at 1 Month

 , , , , , , , , , , , and
on behalf of The Korean Organ Transplantation Registry Study Groupadd
Show full author list
, , , , , , , , , , , and
on behalf of The Korean Organ Transplantation Registry Study Groupadd
Show full author list
Abstract
:1. Introduction
2. Material and Methods
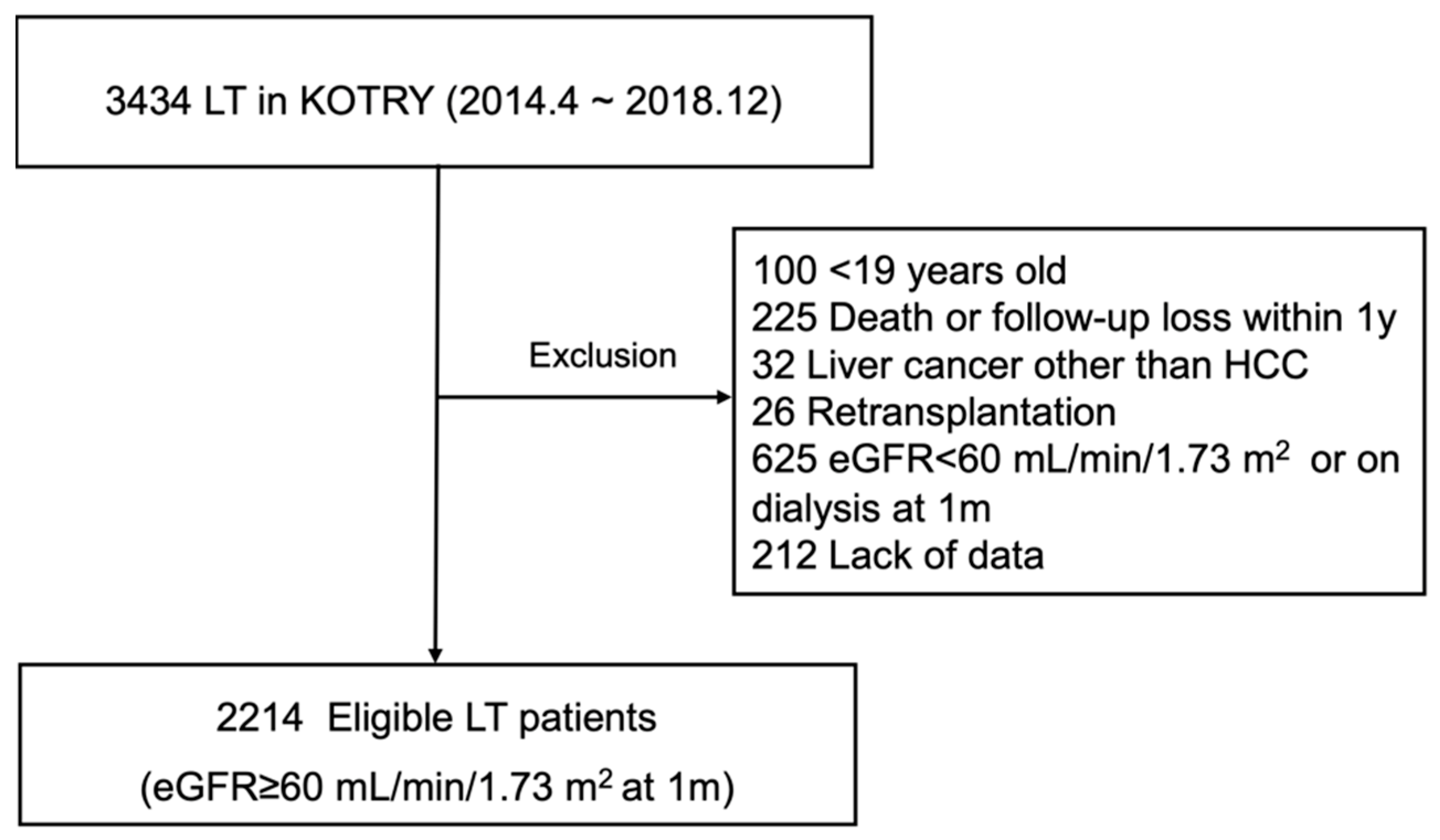
2.1. Selection of Study Population
2.2. Data Collection
2.3. Definition
2.4. Statistical Analyses
2.5. Ethics Approval
3. Results
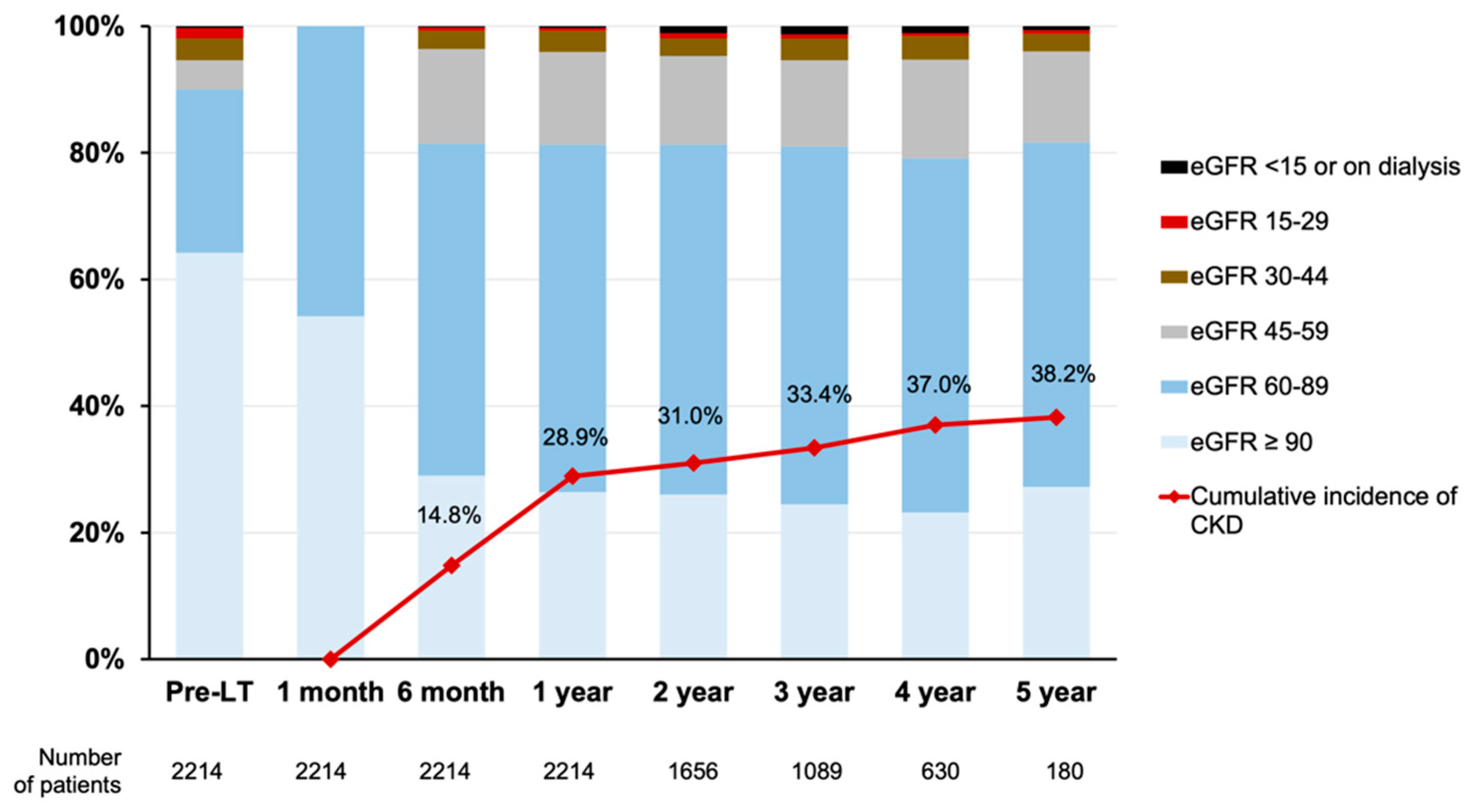
3.1. Distributions of eGFR and CKD
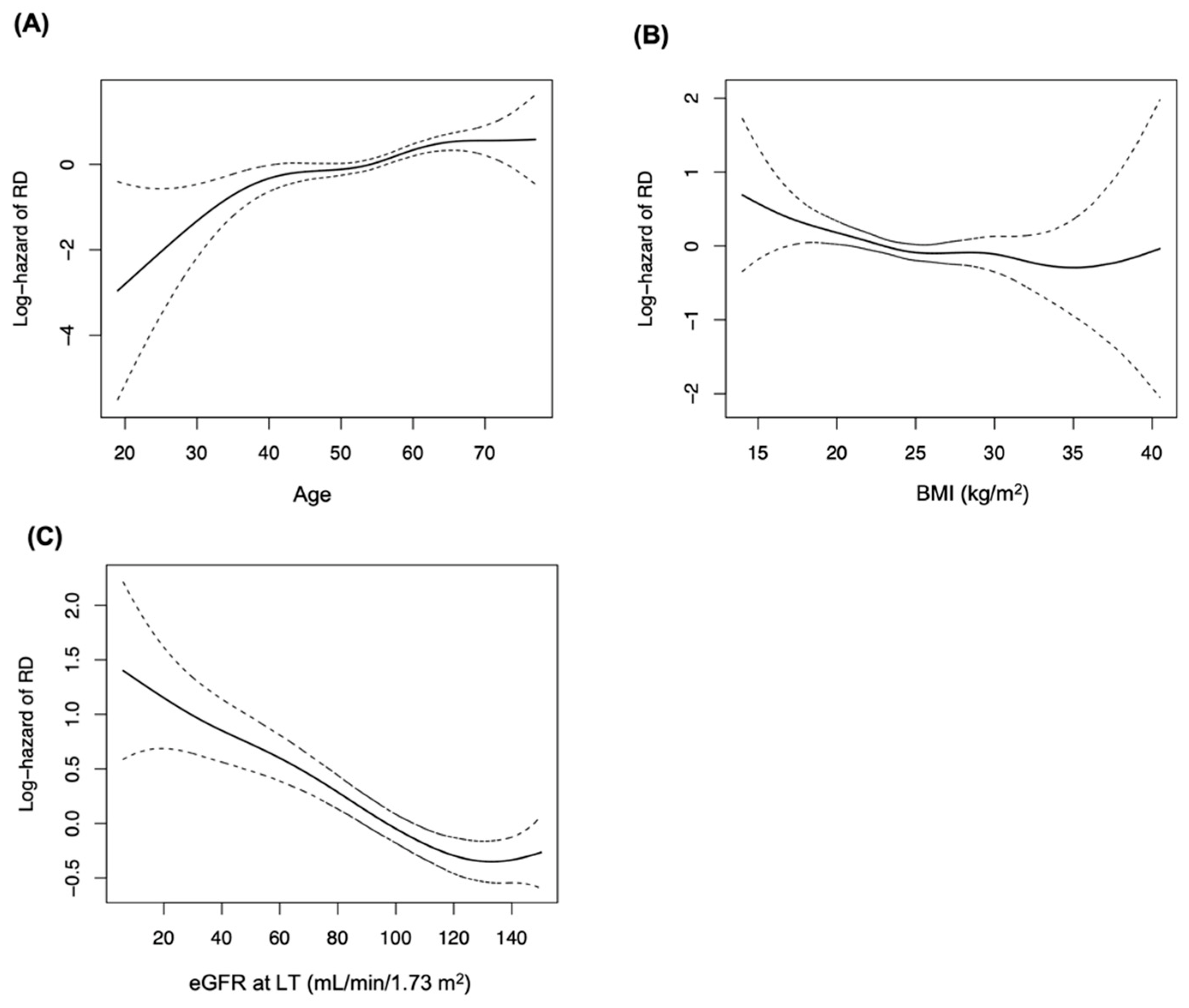
3.2. Baseline Risk Factors for CKD
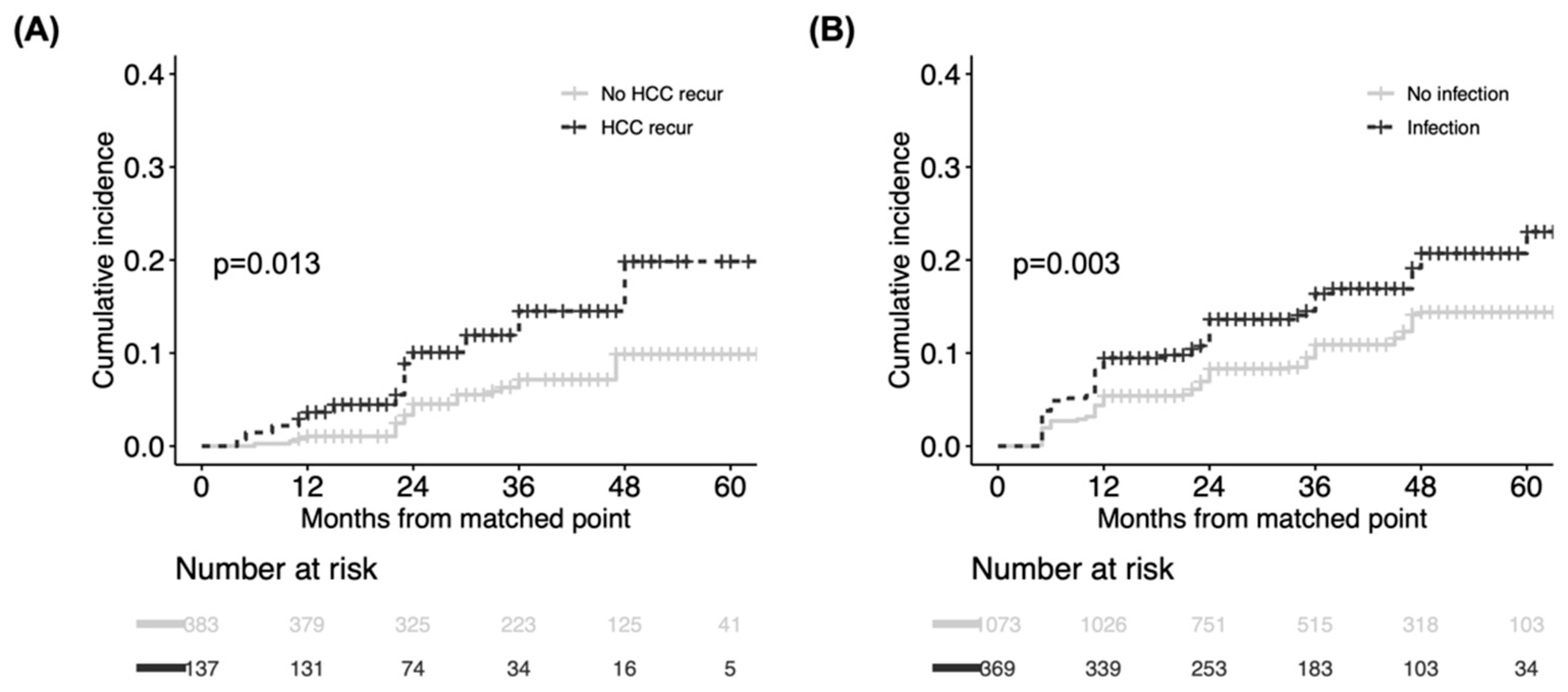
3.3. Post-Transplant Risk Factors for CKD
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kwong, A.; Kim, W.R.; Lake, J.R.; Smith, J.M.; Schladt, D.P.; Skeans, M.A.; Noreen, S.M.; Foutz, J.; Miller, E.; Snyder, J.J.; et al. OPTN/SRTR 2018 Annual Data Report: Liver. Am. J. Transplant. 2020, 20 (Suppl. S1), 193–299. [Google Scholar] [CrossRef]
- VanWagner, L.B.; Montag, S.; Zhao, L.; Allen, N.B.; Lloyd-Jones, D.M.; Das, A.; Skaro, A.I.; Hohmann, S.; Friedewald, J.J.; Levitsky, J. Cardiovascular Disease Outcomes Related to Early Stage Renal Impairment After Liver Transplantation. Transplantation 2018, 102, 1096–1107. [Google Scholar] [CrossRef] [PubMed]
- Allen, A.M.; Kim, W.R.; Therneau, T.M.; Larson, J.J.; Heimbach, J.K.; Rule, A.D. Chronic kidney disease and associated mortality after liver transplantation--a time-dependent analysis using measured glomerular filtration rate. J. Hepatol. 2014, 61, 286–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weber, M.L.; Ibrahim, H.N.; Lake, J.R. Renal dysfunction in liver transplant recipients: Evaluation of the critical issues. Liver Transpl. 2012, 18, 1290–1301. [Google Scholar] [CrossRef] [PubMed]
- Durand, F.; Francoz, C.; Asrani, S.K.; Khemichian, S.; Pham, T.A.; Sung, R.S.; Genyk, Y.S.; Nadim, M.K. Acute Kidney Injury After Liver Transplantation. Transplantation 2018, 102, 1636–1649. [Google Scholar] [CrossRef]
- Giusto, M.; Berenguer, M.; Merkel, C.; Aguilera, V.; Rubin, A.; Ginanni Corradini, S.; Mennini, G.; Rossi, M.; Prieto, M.; Merli, M. Chronic kidney disease after liver transplantation: Pretransplantation risk factors and predictors during follow-up. Transplantation 2013, 95, 1148–1153. [Google Scholar] [CrossRef]
- Sharma, P.; Schaubel, D.E.; Guidinger, M.K.; Goodrich, N.P.; Ojo, A.O.; Merion, R.M. Impact of MELD-based allocation on end-stage renal disease after liver transplantation. Am. J. Transplant. 2011, 11, 2372–2378. [Google Scholar] [CrossRef] [Green Version]
- Sharma, P.; Welch, K.; Eikstadt, R.; Marrero, J.A.; Fontana, R.J.; Lok, A.S. Renal outcomes after liver transplantation in the model for end-stage liver disease era. Liver Transpl. 2009, 15, 1142–1148. [Google Scholar] [CrossRef] [Green Version]
- Ojo, A.O.; Held, P.J.; Port, F.K.; Wolfe, R.A.; Leichtman, A.B.; Young, E.W.; Arndorfer, J.; Christensen, L.; Merion, R.M. Chronic renal failure after transplantation of a nonrenal organ. N. Engl. J. Med. 2003, 349, 931–940. [Google Scholar] [CrossRef]
- Kim, J.M.; Kim, D.G.; Kim, J.; Lee, K.; Lee, K.W.; Ryu, J.H.; Kim, B.-W.; Choi, D.L.; You, Y.K.; Kim, D.-S.; et al. Outcomes after Liver Transplantation in Korea: Incidence and Risk Factors from Korean Transplantation Registry. Clin. Mol. Hepatol. 2021, 27, 451–462. [Google Scholar] [CrossRef]
- Kalisvaart, M.; Schlegel, A.; Trivedi, P.J.; Roberts, K.; Mirza, D.F.; Perera, T.; Isaac, J.I.; Ferguson, J.; De Jonge, J.; Muiesan, P. Chronic Kidney Disease After Liver Transplantation: Impact of Extended Criteria Grafts. Liver Transpl. 2019, 25, 922–933. [Google Scholar] [CrossRef]
- Levitsky, J.; O’Leary, J.G.; Asrani, S.; Sharma, P.; Fung, J.; Wiseman, A.; Niemann, C.U. Protecting the Kidney in Liver Transplant Recipients: Practice-Based Recommendations From the American Society of Transplantation Liver and Intestine Community of Practice. Am. J. Transplant. 2016, 16, 2532–2544. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.; Jeong, J.C.; Lee, J.; Kim, Y.H.; Paik, H.C.; Kim, J.J.; Park, H.-Y.; Kim, M.S.; Ahn, C. Design and Methods of the Korean Organ Transplantation Registry. Transplant. Direct. 2017, 3, e191. [Google Scholar] [CrossRef]
- Min, S.I.; Ahn, C.; Han, D.J.; Kim, S.I.; Chung, S.Y.; Lee, S.K.; Kim, S.J.; Kwon, O.J.; Cho, H.R.; Hwang, S.; et al. To achieve national self-sufficiency: Recent progresses in deceased donation in Korea. Transplantation 2015, 99, 765–770. [Google Scholar] [CrossRef]
- Mazzaferro, V.; Regalia, E.; Doci, R.; Andreola, S.; Pulvirenti, A.; Bozzetti, F.; Montalto, F.; Ammatuna, M.; Morabito, A.; Gennari, L. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N. Engl. J. Med. 1996, 334, 693–699. [Google Scholar] [CrossRef]
- Levey, A.S.; Coresh, J.; Greene, T.; Stevens, L.A.; Zhang, Y.L.; Hendriksen, S.; Kusek, J.W.; Van Lente, F.; Chronic Kidney Disease Epidemiology Collaboration. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann. Intern. Med. 2006, 145, 247–254. [Google Scholar] [CrossRef]
- Levin, A.; Stevens, P.E. Summary of KDIGO 2012 CKD Guideline: Behind the scenes, need for guidance, and a framework for moving forward. Kidney Int. 2014, 85, 49–61. [Google Scholar] [CrossRef] [Green Version]
- Thuluvath, P.J.; Thuluvath, A.J.; Savva, Y. Karnofsky performance status before and after liver transplantation predicts graft and patient survival. J. Hepatol. 2018, 69, 818–825. [Google Scholar] [CrossRef]
- Hastie, T.; Tibshirani, R. Exploring the nature of covariate effects in the proportional hazards model. Biometrics 1990, 46, 1005–1016. [Google Scholar] [CrossRef]
- Zhang, Z.; Reinikainen, J.; Adeleke, K.A.; Pieterse, M.E.; Groothuis-Oudshoorn, C.G.M. Time-varying covariates and coefficients in Cox regression models. Ann. Transl. Med. 2018, 6, 121. [Google Scholar] [CrossRef] [Green Version]
- Lu, B. Propensity score matching with time-dependent covariates. Biometrics 2005, 61, 721–728. [Google Scholar] [CrossRef]
- Austin, P.C. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat. Med. 2009, 28, 3083–3107. [Google Scholar] [CrossRef] [Green Version]
- Man Kim, J.; Hwang, S.; Lee, K.W.; Lee, J.G.; Ryu, J.H.; Kim, B.W.; Choi, D.L.; You, Y.K.; Kim, D.S.; Nah, Y.W.; et al. New-onset diabetes after adult liver transplantation in the Korean Organ Transplantation Registry (KOTRY) study. Hepatobiliary Surg. Nutr. 2020, 9, 425–439. [Google Scholar] [CrossRef]
- Braun, H.J.; Ascher, N.L. The Impact of Renal Insufficiency After Liver Transplantation. Transplantation 2018, 102, 1033–1034. [Google Scholar] [CrossRef]
- Sharma, P.; Goodrich, N.P.; Zhang, M.; Guidinger, M.K.; Schaubel, D.E.; Merion, R.M. Short-term pretransplant renal replacement therapy and renal nonrecovery after liver transplantation alone. Clin. J. Am. Soc. Nephrol. 2013, 8, 1135–1142. [Google Scholar] [CrossRef] [Green Version]
- Parvathaneni, K.; Surapaneni, A.; Ballew, S.H.; Palta, P.; Rebholz, C.M.; Selvin, E.; Coresh, J.; Grams, M.E. Association Between Midlife Physical Activity and Incident Kidney Disease: The Atherosclerosis Risk in Communities (ARIC) Study. Am. J. Kidney Dis. 2021, 77, 74–81. [Google Scholar] [CrossRef]
- Harhay, M.N.; Rao, M.K.; Woodside, K.J.; Johansen, K.L.; Lentine, K.L.; Tullius, S.G.; Parsons, R.F.; Alhamad, T.; Berger, J.; Cheng, X.S.; et al. An overview of frailty in kidney transplantation: Measurement, management and future considerations. Nephrol. Dial.Transplant. 2020, 35, 1099–1112. [Google Scholar] [CrossRef] [Green Version]
- Pongrac Barlovic, D.; Tikkanen-Dolenc, H.; Groop, P.H. Physical Activity in the Prevention of Development and Progression of Kidney Disease in Type 1 Diabetes. Curr. Diab. Rep. 2019, 19, 41. [Google Scholar] [CrossRef] [Green Version]
- Lee, B.C.; Liu, K.L.; Lin, C.L.; Kao, C.H. Risk of acute kidney injury after transarterial chemoembolisation in hepatocellular carcinoma patients: A nationwide population-based cohort study. Eur. Radiol. 2017, 27, 4482–4489. [Google Scholar] [CrossRef]
- Yeh, H.; Chiang, C.C.; Yen, T.H. Hepatocellular carcinoma in patients with renal dysfunction: Pathophysiology, prognosis, and treatment challenges. World J. Gastroenterol. 2021, 27, 4104–4142. [Google Scholar] [CrossRef]
- Persson, P.B.; Hansell, P.; Liss, P. Pathophysiology of contrast medium-induced nephropathy. Kidney Int. 2005, 68, 14–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, C.H.; Hsieh, S.Y.; Lin, J.L.; Liu, M.S.; Yen, T.H. Hepatocellular carcinoma in patients with chronic kidney disease. World J. Gastroenterol. 2013, 19, 2466–2472. [Google Scholar] [CrossRef] [PubMed]
- Weng, P.H.; Hung, K.Y.; Huang, H.L.; Chen, J.H.; Sung, P.K.; Huang, K.C. Cancer-specific mortality in chronic kidney disease: Longitudinal follow-up of a large cohort. Clin. J. Am. Soc. Nephrol. 2011, 6, 1121–1128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiecek, A.; Zeier, M.; Ritz, E. Role of infection in the genesis of acute renal failure. Nephrol. Dial. Transplant. 1994, 9 (Suppl. S4), 40–44. [Google Scholar]
- Morales-Alvarez, M.C. Nephrotoxicity of Antimicrobials and Antibiotics. Adv. Chronic. Kidney Dis. 2020, 27, 31–37. [Google Scholar] [CrossRef]
- Rodriguez-Peralvarez, M.; Germani, G.; Darius, T.; Lerut, J.; Tsochatzis, E.; Burroughs, A.K. Tacrolimus trough levels, rejection and renal impairment in liver transplantation: A systematic review and meta-analysis. Am. J. Transplant. 2012, 12, 2797–2814. [Google Scholar] [CrossRef] [Green Version]
- Saliba, F.; Duvoux, C.; Dharancy, S.; Dumortier, J.; Calmus, Y.; Gugenheim, J.; Parsons, R.F.; Alhamad, T.; Berger, J.; Cheng, X.S.; et al. Early Switch From Tacrolimus to Everolimus After Liver Transplantation: Outcomes at 2 Years. Liver Transpl. 2019, 25, 1822–1832. [Google Scholar] [CrossRef] [Green Version]
- Jeng, L.B.; Lee, S.G.; Soin, A.S.; Lee, W.C.; Suh, K.S.; Joo, D.J.; Uemoto, S.; Joh, J.; Yoshizumi, T.; Yang, H.-R.; et al. Efficacy and safety of everolimus with reduced tacrolimus in living-donor liver transplant recipients: 12-month results of a randomized multicenter study. Am. J. Transplant. 2018, 18, 1435–1446. [Google Scholar] [CrossRef] [Green Version]
- Saliba, F.; Duvoux, C.; Gugenheim, J.; Kamar, N.; Dharancy, S.; Salamé, E.; Neau-Cransac, M.; Durand, F.; Houssel-Debry, P.; Vanlemmens, C.; et al. Efficacy and Safety of Everolimus and Mycophenolic Acid With Early Tacrolimus Withdrawal After Liver Transplantation: A Multicenter Randomized Trial. Am. J. Transplant. 2017, 17, 1843–1852. [Google Scholar] [CrossRef] [Green Version]
- Asrani, S.K.; Jennings, L.W.; Trotter, J.F.; Levitsky, J.; Nadim, M.K.; Kim, W.R.; Gonzalez, S.A.; Fischbach, B.; Bahirwani, R.; Emmett, M.; et al. A Model for Glomerular Filtration Rate Assessment in Liver Disease (GRAIL) in the Presence of Renal Dysfunction. Hepatology 2019, 69, 1219–1230. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All (n = 2214) | No CKD (n = 1720) | CKD (n = 494) | p |
|---|---|---|---|---|
| Age, years | 53.4 ± 8.9 | 52.6 ± 9.0 | 56.5 ± 7.7 | <0.001 |
| Sex, female | 588 (26.6) | 416 (24.2) | 172 (34.8) | <0.001 |
| BMI, kg/m2 | 24.2 ± 4.2 | 24.2 ± 3.4 | 23.9 ± 3.6 | 0.152 |
| Year of LT | 0.013 | |||
| 2014–2016 | 1153 (52.1) | 871 (50.6) | 282 (57.1) | |
| 2017–2018 | 1061 (47.9) | 849 (49.4) | 212 (42.9) | |
| Donor type | <0.001 | |||
| Living | 1848 (83.5) | 1467 (85.3) | 381 (77.1) | |
| Deceased | 366 (16.5) | 253 (14.7) | 113 (22.9) | |
| Donor age, years | 34.3 ± 13.4 | 33.9 ± 13.4 | 35.7 ± 13.4 | 0.006 |
| Donor sex, female | 799 (36.1) | 627 (36.5) | 172 (34.8) | 0.539 |
| ABO incompatibility | 415 (18.7) | 345 (20.1) | 70 (14.2) | 0.004 |
| Hypertension | 356 (16.1) | 269 (15.6) | 87 (17.6) | 0.326 |
| Pre-transplant DM | 524 (23.7) | 269 (15.6) | 87 (17.6) | 0.326 |
| Underlying liver disease | <0.001 | |||
| Hepatitis B | 1265 (57.2) | 1015 (59.0) | 250 (50.6) | |
| Hepatitis C | 118 (5.3) | 87 (5.1) | 31 (6.3) | |
| Alcoholic | 550 (24.8) | 414 (24.1) | 136 (27.5) | |
| Cryptogenic | 118 (5.3) | 76 (4.4) | 42 (8.5) | |
| Autoimmune | 48 (2.2) | 35 (2.0) | 13 (2.6) | |
| Others | 115 (5.2) | 93 (5.4) | 22 (4.5) | |
| KONOS Status 1 | 28 (1.3) | 20 (1.2) | 8 (1.6) | 0.620 |
| MELD | 16.0 ± 9.2 | 15.5 ± 8.8 | 18.0 ± 10.3 | <0.001 |
| Pre-transplant HCC | <0.001 | |||
| No HCC | 1063 (48.0) | 788 (45.8) | 275 (55.7) | |
| Within-Milan | 869 (39.3) | 700 (40.7) | 169 (34.2) | |
| Above-Milan | 282 (12.7) | 232 (13.5) | 50 (10.1) | |
| KPS at 1 month | <0.001 | |||
| High (80–100%) | 823 (37.1) | 665 (38.7) | 158 (32.0) | |
| Intermediate (50–70%) | 1175 (53.1) | 922 (53.6) | 253 (51.2) | |
| Low (0–40%) | 216 (9.8) | 133 (7.7) | 83 (16.8) | |
| eGFR at LT, mL/min/1.73 m2 (categorized) | <0.001 | |||
| ≥90 | 1422 (64.3) | 1221 (71.0) | 201 (40.7) | |
| 60–89 | 571 (25.8) | 392 (22.8) | 179 (36.2) | |
| 30–59 | 178 (8.0) | 89 (5.2) | 89 (18.0) | |
| 15–29 | 36 (1.6) | 16 (0.9) | 20 (4.0) | |
| <15 or on dialysis | 7 (0.3) | 2 (0.1) | 5 (1.0) | |
| eGFR at 1 month, mL/min/1.73 m2 (numerical) | 97.5 ± 25.1 | 101.3 ± 24.9 | 84.4 ± 21.4 | <0.001 |
| Univariable † | Multivariable † | |||
|---|---|---|---|---|
| Variables | HR (95% CI) | p | HR (95% CI) | p |
| Age, per 5 years | 1.08 (1.01–1.16) | 0.033 | 1.21 (1.14–1.29) | <0.001 |
| Sex, female | 1.71 (1.33–2.20) | <0.001 | 1.43 (1.17–1.75) | <0.001 |
| Body mass index, per 1 kg/m2 | 0.91 (0.88–0.95) | <0.001 | 0.96 (0.94–0.99) | <0.001 |
| Pre-transplant DM | 1.38 (1.06–1.81) | 0.018 | 1.58 (1.30–1.93) | <0.001 |
| KPS at 1 month | ||||
| High (80–100%) | Reference | <0.001 | Reference | |
| Intermediate (50–70%) | 2.26 (1.63–3.14) | <0.001 | 1.12 (0.91–1.37) | 0.312 |
| Low (0–40%) | 3.25 (1.32–6.05) | <0.001 | 2.01 (1.52–2.65) | <0.001 |
| eGFR at LT, mL/min/1.73 m2 | 0.97 (0.96–0.98) | <0.001 | 0.97 (0.96–0.98) | <0.001 |
| eGFR at 1 month, mL/min/1.73 m2 | 0.98 (0.97–0.99) | <0.001 | 0.98 (0.97–0.99) | <0.001 |
| Variables | HR † | 95% CI | p |
|---|---|---|---|
| Biopsy-proven rejection | 0.96 | 0.59–1.55 | 0.871 |
| Bile duct complication | 1.21 | 0.91–1.62 | 0.188 |
| Vascular complication | 0.81 | 0.51–1.30 | 0.390 |
| HCC recurrence | 1.93 | 1.06–3.53 | 0.032 |
| Infection | 1.44 | 1.12–1.60 | 0.048 |
| NODAT ‡ | 1.17 | 0.81–1.69 | 0.420 |
| AST, U/L | 0.99 | 0.99–1.00 | 0.756 |
| ALT, U/L | 1.00 | 0.99–1.00 | 0.718 |
| Total bilirubin, mg/dL | 1.02 | 0.97–1.08 | 0.485 |
| Immunosuppressants (with or without steroid) | |||
| Tacrolimus + Mycophenolate mofetil | Reference | ||
| Tacrolimus | 1.34 | 0.65–1.41 | 0.745 |
| Others | 1.22 | 0.89–2.30 | 0.096 |
| Tacrolimus trough level § | |||
| 5–8 (ng/mL) | Reference | ||
| 0–5 (ng/mL) | 0.97 | 0.77–1.21 | 0.857 |
| 8–12 (ng/mL) | 1.04 | 0.81–1.36 | 0.701 |
| >12 (ng/mL) | 0.95 | 0.62–1.46 | 0.864 |
| eGFR, mL/min/1.73 m2 | 0.98 | 0.97–0.99 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.-G.; Hwang, S.; Kim, J.M.; Ryu, J.H.; You, Y.K.; Choi, D.; Kim, B.-W.; Kim, D.-S.; Nah, Y.W.; Kim, T.-S.; et al. Non-Renal Risk Factors for Chronic Kidney Disease in Liver Recipients with Functionally Intact Kidneys at 1 Month. J. Clin. Med. 2022, 11, 4203. https://doi.org/10.3390/jcm11144203
Kim D-G, Hwang S, Kim JM, Ryu JH, You YK, Choi D, Kim B-W, Kim D-S, Nah YW, Kim T-S, et al. Non-Renal Risk Factors for Chronic Kidney Disease in Liver Recipients with Functionally Intact Kidneys at 1 Month. Journal of Clinical Medicine. 2022; 11(14):4203. https://doi.org/10.3390/jcm11144203
Chicago/Turabian StyleKim, Deok-Gie, Shin Hwang, Jong Man Kim, Je Ho Ryu, Young Kyoung You, Donglak Choi, Bong-Wan Kim, Dong-Sik Kim, Yang Won Nah, Tae-Seok Kim, and et al. 2022. "Non-Renal Risk Factors for Chronic Kidney Disease in Liver Recipients with Functionally Intact Kidneys at 1 Month" Journal of Clinical Medicine 11, no. 14: 4203. https://doi.org/10.3390/jcm11144203
APA StyleKim, D. -G., Hwang, S., Kim, J. M., Ryu, J. H., You, Y. K., Choi, D., Kim, B. -W., Kim, D. -S., Nah, Y. W., Kim, T. -S., Cho, J. Y., Hong, G., Yang, J. D., Han, J., Suh, S. -W., Kim, K. W., Jung, Y. K., Moon, J. I., Lee, J. Y., ... Joo, D. J., on behalf of The Korean Organ Transplantation Registry Study Group. (2022). Non-Renal Risk Factors for Chronic Kidney Disease in Liver Recipients with Functionally Intact Kidneys at 1 Month. Journal of Clinical Medicine, 11(14), 4203. https://doi.org/10.3390/jcm11144203