

Conservative Therapies for TMJ Closed Lock: A Randomized Controlled Trial
 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
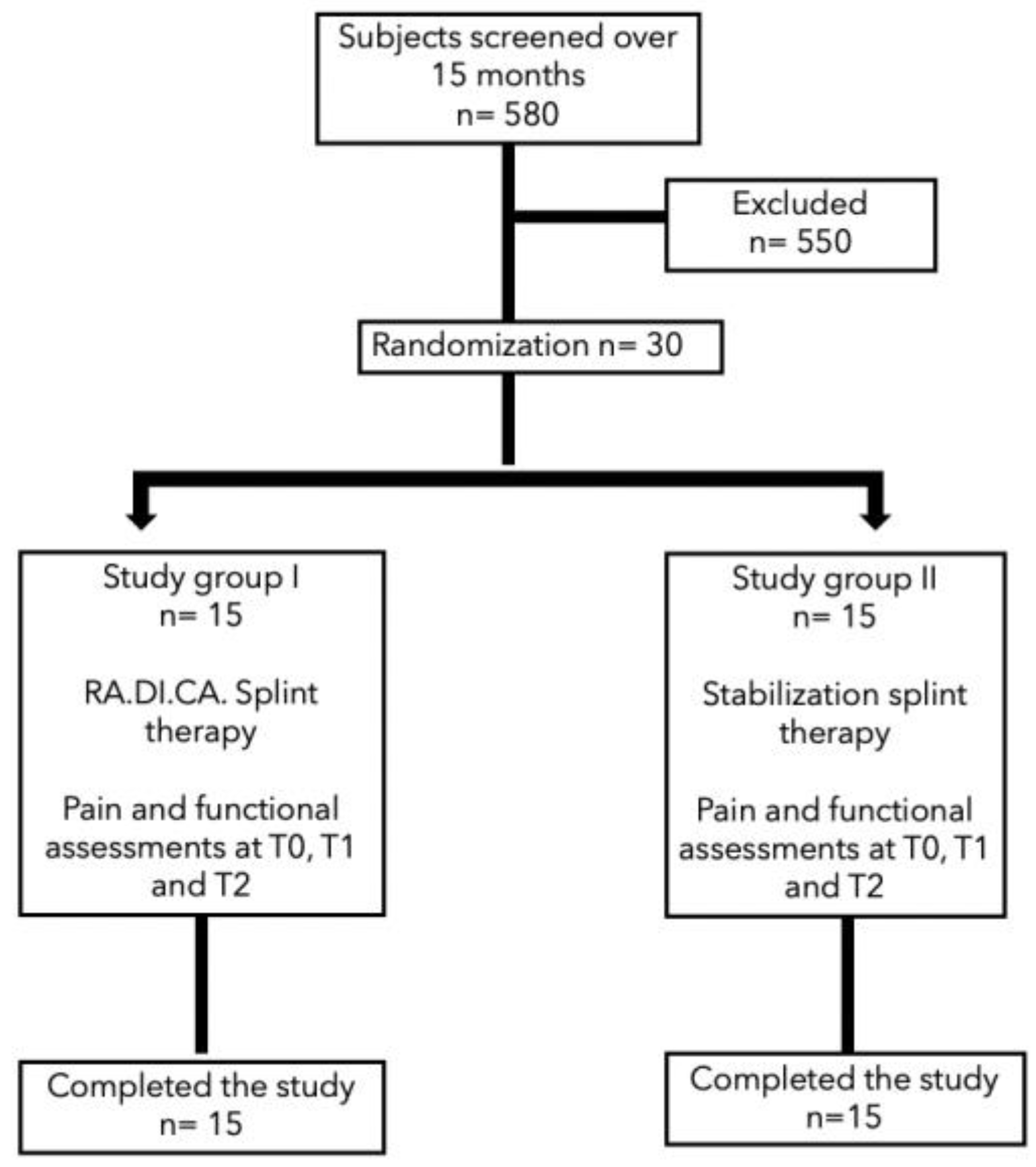
2.1. Participants and Sampling
2.2. Study Design
- A heat-cured acrylic resin upper plate (1),
- A heat-cured acrylic resin lower plate (2),
- An anterior hinge (3),
- Two vestibular springs made with orthodontic wire (4),
- Two or more Adams clasps and/or two ball clasps (5),
- A vestibular steel arch (6).
2.3. Statistical Analysis
3. Results
3.1. Descriptive Statistics
3.2. Inferential Statistics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Miernik, M.; Więckiewicz, W. The Basic Conservative Treatment of Temporomandibular Joint Anterior Disc Displacement Without Reduction—Review. Adv. Clin. Exp. Med. 2015, 24, 731–735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dworkin, S.F.; LeResche, L. Research diagnostic criteria for temporomandibular disorders: Review, criteria, examinations and specifications, critique. J. Craniomandib. Disord. 1992, 6, 301–355. [Google Scholar] [PubMed]
- McNeill, C. Management of temporomandibular disorders: Concepts and controversies. J. Prosthet. Dent. 1997, 77, 510–522. [Google Scholar] [CrossRef] [PubMed]
- Dimitroulis, G. The prevalence of osteoarthrosis in cases of advanced internal derangement of the Temporomandibular Joint: A clinical, surgical and histological study. Int. J. Oral Maxillofac. Surg. 2005, 34, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Cascone, P.; Di Paolo, C. Patologia dell’Articolazione Temporomandibolare: Dall’eziopatogenesi Alla Terapia; UTET: Torino, Italy, 2004; pp. 31–181. [Google Scholar]
- Schmitter, M.; Zahran, M.; Duc, J.-M.P.; Henschel, V.; Rammelsberg, P. Conservative Therapy in Patients with Anterior Disc Displacement Without Reduction Using 2 Common Splints: A Randomized Clinical Trial. J. Oral Maxillofac. Surg. 2005, 63, 1295–1303. [Google Scholar] [CrossRef]
- Zotti, F.; Albanese, M.; Rodella, L.F.; Nocini, P.F. Platelet-Rich Plasma in Treatment of Temporomandibular Joint Dysfunctions: Narrative Review. Int. J. Mol. Sci. 2019, 20, 277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurita, H.; Kurashina, K.; Ohtsuka, A. Efficacy of a mandibular manipulation technique in reducing the permanently displaced temporomandibular joint disc. J. Oral Maxillofac. Surg. 1999, 57, 784–787. [Google Scholar] [CrossRef]
- Dimitroulis, G. Management of temporomandibular joint disorders: A surgeon’s perspective. Aust. Dent. J. 2018, 63, S79–S90. [Google Scholar] [CrossRef] [PubMed]
- Stiesch-Scholz, M.; Kempert, J.; Wolter, S.; Tschernitschek, H.; Rossbach, A. Comparative prospective study on splint therapy of anterior disc displacement without reduction. J. Oral Rehabil. 2005, 32, 474–479. [Google Scholar] [CrossRef] [PubMed]
- Ohnuki, T.; Fukuda, M.; Nakata, A.; Nagai, H.; Takahashi, T.; Sasano, T.; Miyamoto, Y. Evaluation of the position, mobility, and morphology of the disc by MRI before and after four different treatments for temporomandibular joint disorders. Dentomaxill. Radiol. 2006, 35, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Ramfjord, S.; Ash, M.M. Reflections on the Michigan occlusal splint. J. Oral Rehabil. 1994, 21, 491–500. [Google Scholar] [CrossRef]
- Ekberg, E.; Vallon, D.; Nilner, M. Occlusal appliance therapy in patients with temporomandibular disorders: A double-blind controlled study in a short-term perspective. Acta Odontol. Scand. 1998, 56, 122–128. [Google Scholar] [CrossRef]
- Kreiner, M.; Betancor, E.; Clark, G.T. Occlusal stabilization appliances. J. Am. Dent. Assoc. 2001, 132, 770–777. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Paolo, C.; Falisi, G.; Panti, F.; Di Giacomo, P.; Rampello, A. “RA.DI.CA.” Splint for the Management of the Mandibular Functional Limitation: A Retrospective Study on Patients with Anterior Disc Displacement without Reduction. Int. J. Environ. Res. Public Health 2020, 17, 9057. [Google Scholar] [CrossRef] [PubMed]
- Ash, M.M.; Bernhardt, O. Schienentherapie; Urban und Schwarzenberg: Munich, Germany, 1995. [Google Scholar]
- Nitzan, D.; Benoliel, R.; Heir, G.; Dolwick, F. Chapter 8—Pain and dysfunction of the temporomandibular joint. In Orofacial Pain and Headache; Mosby: Maryland Heights, MO, USA, 2008; pp. 149–192. [Google Scholar]
- Mazza, D.; Stasolla, A.; Kharrub, Z.; Maccioni, F.; Marini, M. MRI evaluation of morpho-structural alterations of the retrodiscal tissue in condylo-meniscal incoordination of the TMJ: Usefulness of individualised T2-weighted TSE sequences. Radiol. Med. 2004, 107, 261–268. [Google Scholar] [PubMed]
- Haketa, T.; Kino, K.; Sugisaki, M.; Takaoka, M.; Ohta, T. Randomized Clinical Trial of Treatment for TMJ Disc Displacement. J. Dent. Res. 2010, 89, 1259–1263. [Google Scholar] [CrossRef] [PubMed]
- Shoji, Y.-N. Nonsurgical Treatment of Anterior Disk Displacement Without Reduction of the Temporomandibular Joint: A Case Report on the Relationship between Condylar Rotation and Translation. CRANIO® 1995, 13, 270–273. [Google Scholar] [CrossRef] [PubMed]
- Stiesch-Scholz, M.; Tschernitschek, H.; Rossbach, A. Early begin of splint therapy improves treatment outcome in patients with temporomandibular joint disk displacement without reduction. Clin. Oral Investig. 2002, 6, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Lundh, H.; Westesson, P.-L. Long-term follow-up after occlusal treatment to correct abnormal temporomandibular joint disk position. Oral Surg. Oral Med. Oral Pathol. 1989, 67, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Sears, V.H. Occlusal pivots. J. Prosthet. Dent. 1956, 6, 332–336. [Google Scholar] [CrossRef]
- Martini, G.; Martini, M.; Carano, A. MRI Study of a Physiotherapeutic Protocol in Anterior Disk Displacement without Reduction. CRANIO® 1996, 14, 216–224. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter Assessed | Stabilization Splint | RA.DI.CA Splint | p-Value Student’s | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Arthralgia | 68.00 | 24.85 | 69.00 | 17.28 | 0.89 |
| Headache | 75.00 | 13.54 | 83.00 | 13.37 | 0.11 |
| Neck pain | 53.00 | 20.02 | 57.00 | 24.51 | 0.62 |
| Mouth opening | 31.30 (mm) | 2.66 | 30.40 (mm) | 3.47 | 0.43 |
| Parameter Assessed at T1 | RADICA EMM ± SD | 95% CI for Mean Difference | Stabilization Splint Mean ± SD | 95% CI for Mean Difference | ||||
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | Lower | Upper | |||||
| Arthralgia | 39.333 | 4.842 | 29.843 | 48.823 | 52.667 | 4.842 | 43.177 | 62.157 |
| Headache | 46.000 | 3.695 | 38.759 | 53.241 | 65.333 | 3.695 | 58.092 | 72.575 |
| Neck pain | 37.333 | 5.711 | 26.139 | 48.527 | 46.667 | 5.711 | 35.473 | 57.861 |
| Mouth opening | 43.133 | 0.842 | 41.484 | 44.783 | 35.800 | 0.842 | 34.150 | 37.450 |
| Parameter assessed at T2 | ||||||||
| Arthralgia | 14.800 | 3.727 | 7.496 | 22.104 | 44.000 | 3.727 | 36.696 | 51.304 |
| Headache | 14.667 | 3.469 | 7.868 | 21.465 | 50.000 | 3.469 | 43.202 | 56.798 |
| Neck pain | 24.000 | x5.080 | 14.043 | 33.957 | 42.667 | 5.080 | 32.709 | 52.624 |
| Mouth opening | 44.667 | 0.791 | 43.116 | 46.217 | 36.800 | 0.791 | 35.249 | 38.351 |
| Parameter Assessed | Within-Subjects Factor (Time T0→T1) | Between-Subjects Factor (Type of Treatment) | Interaction between Treatment and Time | |||
| Chi-Square value | p value | Chi-Square value | p value | Chi-Square value | p value | |
| Arthralgia | 44.510 | <0.001 | 1.320 | 0.251 | 8.028 | 0.005 |
| Headache | 54.449 | <0.001 | 2.046 | 0.153 | 34.575 | <0.001 |
| Neck Pain | 17.307 | <0.001 | 0.267 | 0.605 | 17.307 | <0.001 |
| Mouth opening | 68.096 | <0.001 | 13.964 | <0.001 | 18.242 | <0.001 |
| Parameter assessed | Within-subjects factor (time T1→T2) | Between-subjects factor (type of treatment) | Interaction between treatment and time | |||
| Chi-Square value | p value | Chi-Square value | p value | Chi-Square value | p value | |
| Arthralgia | 45.856 | <0.001 | 14.929 | <0.001 | 18.045 | <0.001 |
| Headache | 41.713 | <0.001 | 28.075 | <0.001 | 8.648 | 0.003 |
| Neck Pain | 14.289 | <0.001 | 4.147 | 0.042 | 4.886 | 0.027 |
| Mouth opening | 13.391 | <0.001 | 30.742 | <0.001 | 0.773 | 0.379 |
| ANOVA Summary | Within subjects factor (time T0→T2) | Between-subjects factor (type of treatment) | Interaction between treatment and time | |||
| F | p value | F | p value | F | p value | |
| Artralgia | 170.163 | <0.001 | 6.244 | 0.019 | 23.379 | <0.001 |
| Headache | 219.299 | <0.001 | 21.928 | <0.001 | 131.403 | <0.001 |
| Neck Pain | 23,748 | <0.001 | 1660 | 0.208 | 13,206 | <0.001 |
| Mouth opening | 157.609 | <0.001 | 37.791 | <0.001 | 24.227 | <0.001 |
| Parameters | T0 → T1 | T0 → T2 | ||
|---|---|---|---|---|
| F | p-Value | F | p-Value | |
| Arthralgia | 66.741 | <0.001 | 87.227 | <0.001 |
| 95% CI for Mean Difference | ||||
| Mean difference between T0 and T2 | Lower | Upper | ptukey | |
| −27.337 | −31.728 | 22.946 | <0.001 | |
| Headache | 54.712 | <0.001 | 289.605 | <0.001 |
| 95% CI for Mean Difference | ||||
| Mean difference between T0 and T2 | Lower | Upper | ptukey | |
| −52.500 | −58.830 | −46.170 | <0.001 | |
| Neck pain | 22.164 | <0.001 | 66.982 | <0.001 |
| 95% CI for Mean Difference | ||||
| Mean difference between T0 and T2 | Lower | Upper | ptukey | |
| −20.876 | −28.041 | −13.711 | <0.001 | |
| Mouth opening | 0.419 | 0.523 | 0.190 | <0.666 |
| 95% CI for Mean Difference | ||||
| Mean difference between T0 and T2 | Lower | Upper | ptukey | |
| 7.871 | 5.871 | 9.871 | <0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Giacomo, P.; Di Paolo, C.; Qorri, E.; Gatto, R.; Manes Gravina, G.; Falisi, G. Conservative Therapies for TMJ Closed Lock: A Randomized Controlled Trial. J. Clin. Med. 2022, 11, 7037. https://doi.org/10.3390/jcm11237037
Di Giacomo P, Di Paolo C, Qorri E, Gatto R, Manes Gravina G, Falisi G. Conservative Therapies for TMJ Closed Lock: A Randomized Controlled Trial. Journal of Clinical Medicine. 2022; 11(23):7037. https://doi.org/10.3390/jcm11237037
Chicago/Turabian StyleDi Giacomo, Paola, Carlo Di Paolo, Erda Qorri, Roberto Gatto, Giovanni Manes Gravina, and Giovanni Falisi. 2022. "Conservative Therapies for TMJ Closed Lock: A Randomized Controlled Trial" Journal of Clinical Medicine 11, no. 23: 7037. https://doi.org/10.3390/jcm11237037
APA StyleDi Giacomo, P., Di Paolo, C., Qorri, E., Gatto, R., Manes Gravina, G., & Falisi, G. (2022). Conservative Therapies for TMJ Closed Lock: A Randomized Controlled Trial. Journal of Clinical Medicine, 11(23), 7037. https://doi.org/10.3390/jcm11237037