
Incidence, Treatment and Clinical Impact of Iron Deficiency in Chronic Heart Failure: A Longitudinal Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Iron Deficiency Parameters’ Assessment and Definitions
2.2. Intravenous Iron Treatment
2.3. Endpoints
2.4. Statistical Analysis
3. Results
3.1. Longitudinal Cohort Characteristics
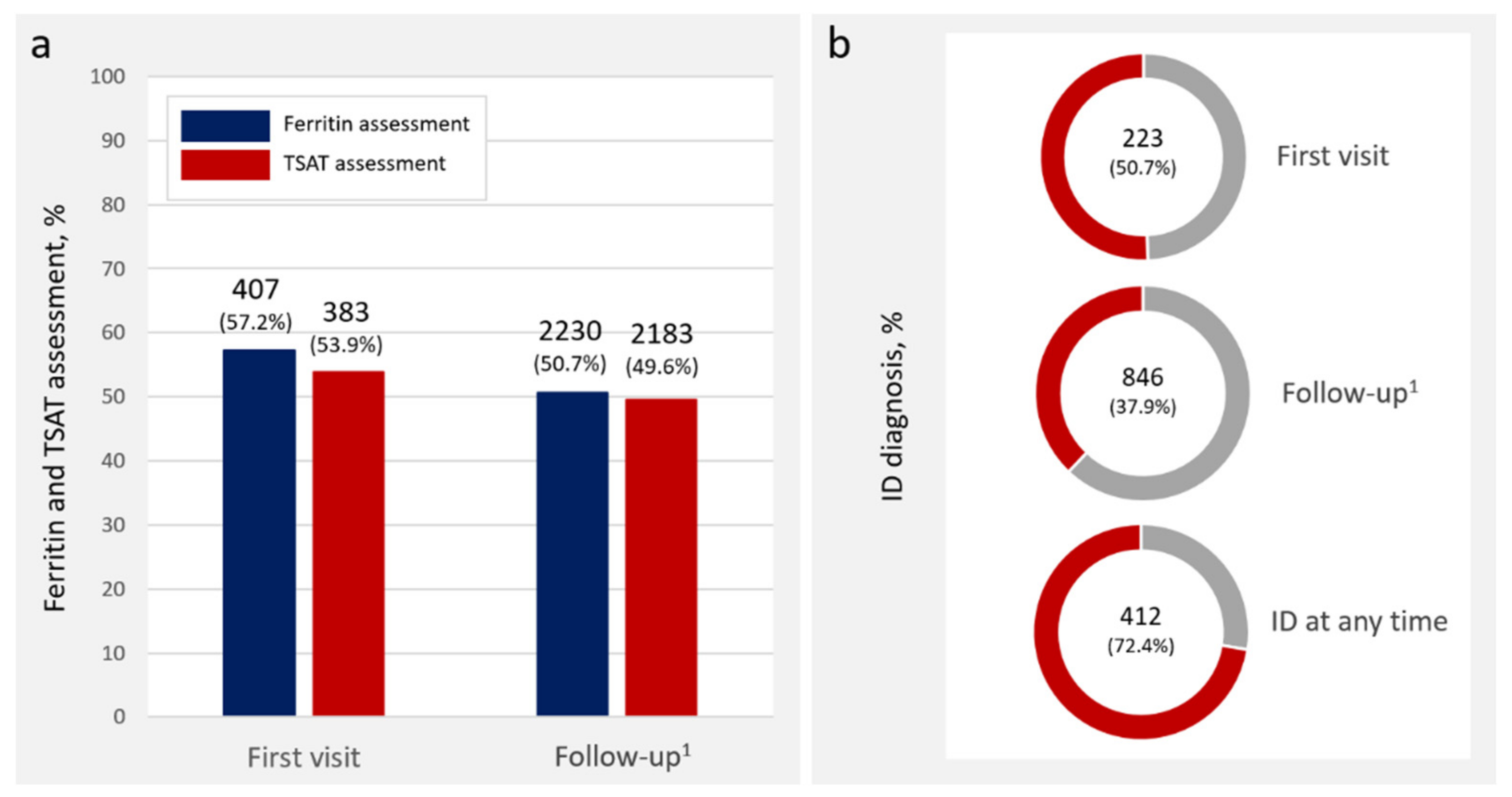
3.2. Iron Deficiency Assessment and Diagnosis
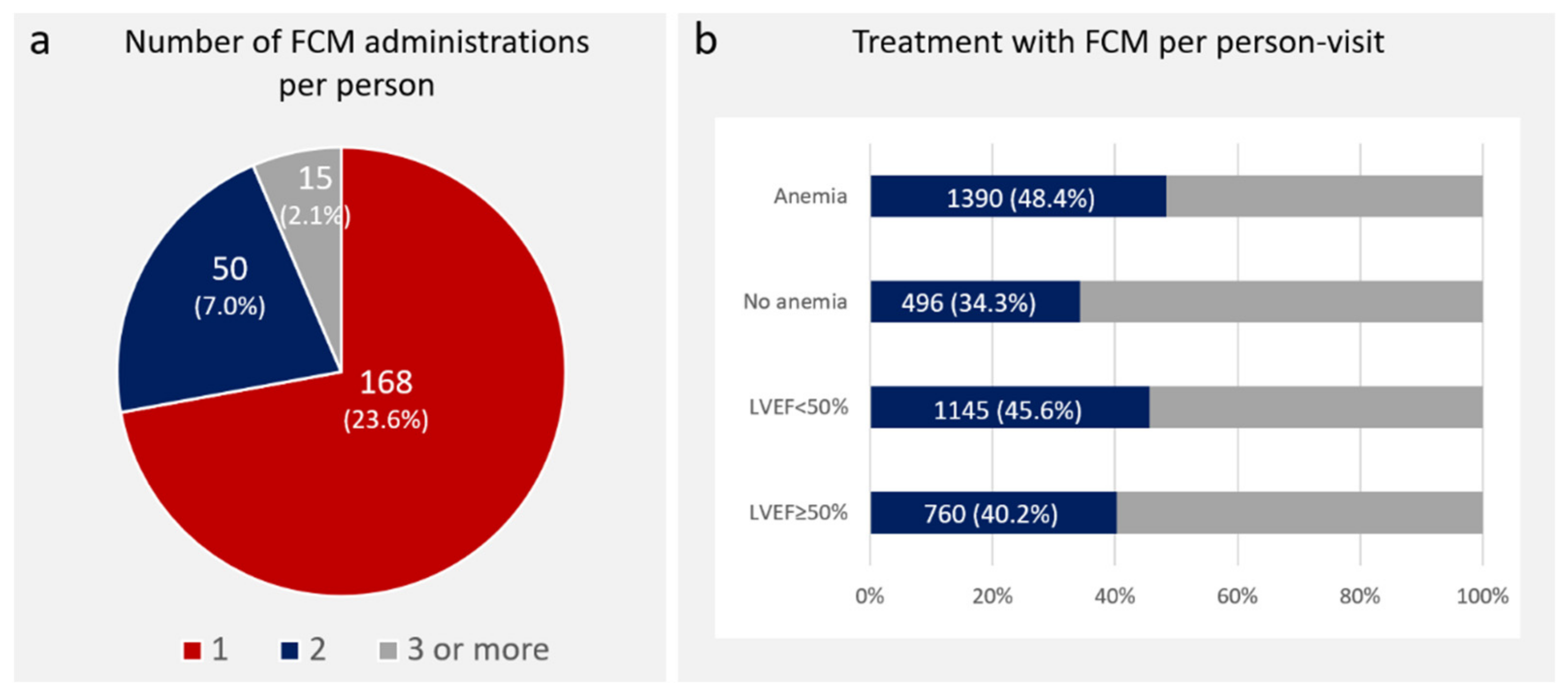
3.3. Intravenous Iron Treatment
3.4. Adverse Clinical Events
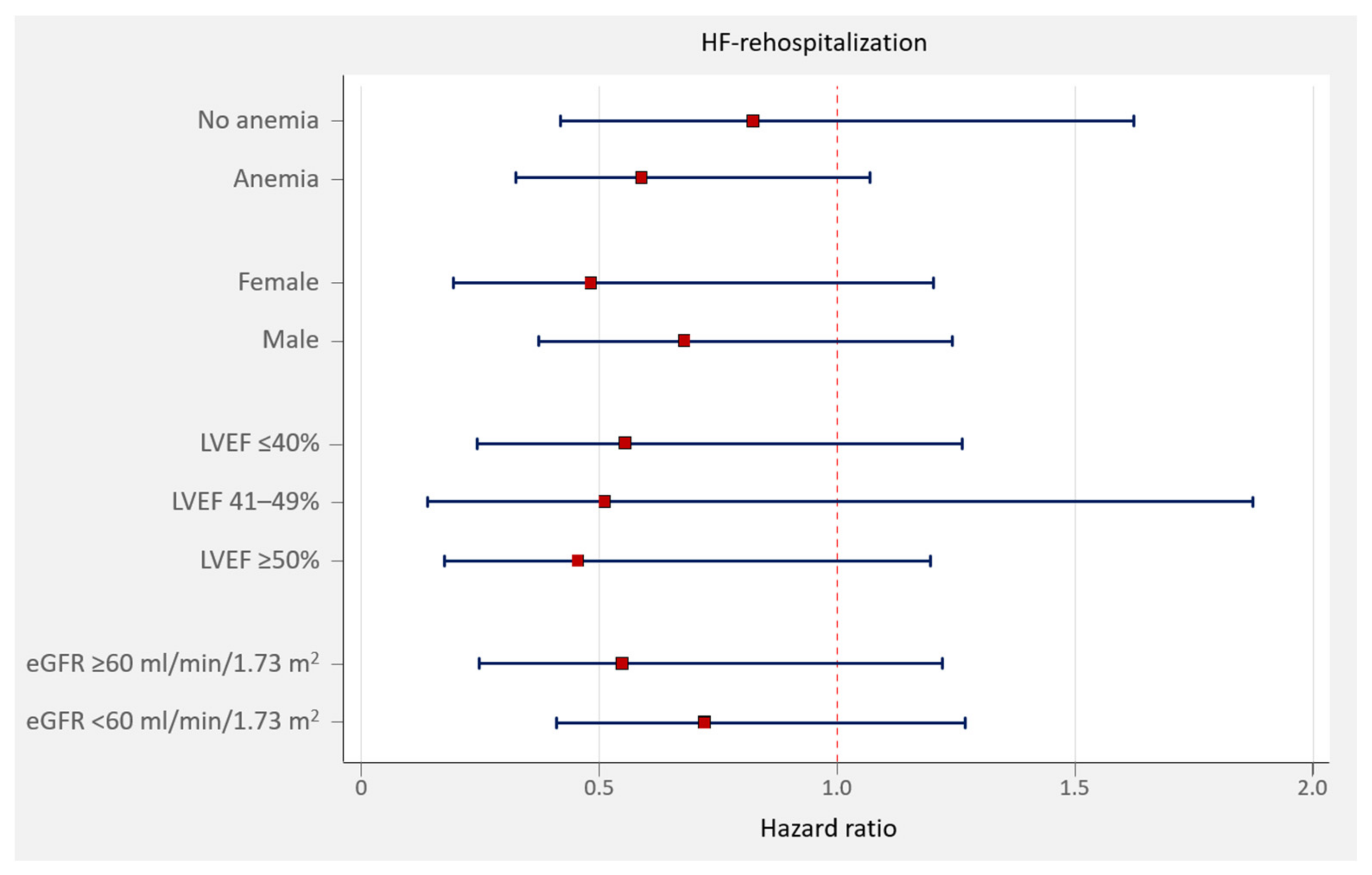
3.5. Iron Deficiency and HF Rehospitalizations
3.6. Intravenous Iron and Adverse Clinical Events
4. Discussion
4.1. ID Testing and Treatment in Daily Clinical Practice
4.2. ID and Its Treatment and Adverse Clinical Events: Evidence from Real-World Data
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Anand, I.S.; Gupta, P. Anemia and iron deficiency in heart failure: Current concepts and emerging therapies. Circulation 2018, 138, 80–98. [Google Scholar] [CrossRef] [PubMed]
- Cohen-Solal, A.; Damy, T.; Terbah, M.; Kerebel, S.; Baguet, J.P.; Hanon, O.; Zannad, F.; Laperche, T.; Leclercq, C.; Concas, V.; et al. High prevalence of iron deficiency in patients with acute decompensated heart failure. Eur. J. Heart Fail. 2014, 16, 984–991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rocha, B.M.L.; Cunha, G.J.L.; Menezes Falcão, L.F. The burden of iron deficiency in heart failure: Therapeutic approach. J. Am. Coll. Cardiol. 2018, 71, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Palau, P.; Llàcer, P.; Domínguez, E.; Tormo, J.P.; Zakarne, R.; Mollar, A.; Martínez, A.; Miñana, G.; Santas, E.; Almenar, L.; et al. Iron deficiency and short-term adverse events in patients with decompensated heart failure. Clin. Res. Cardiol. 2021, 110, 1292–1298. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2016, 18, 891–975. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Kirwan, B.A.; Anker, S.D.; McDonagh, T.; Dorobantu, M.; Drozdz, J.; Fabien, V.; Filippatos, G.; Göhring, U.M.; Keren, A.; et al. Ferric carboxymaltose for iron deficiency at discharge after acute heart failure: A multicentre, double-blind, randomised, controlled trial. Lancet 2020, 396, 1895–1904. [Google Scholar] [CrossRef]
- Becher, P.M.; Schrage, B.; Benson, L.; Fudim, M.; Corovic Cabrera, C.; Dahlström, U.; Rosano, G.M.C.; Jankowska, E.A.; Anker, S.D.; Lund, L.H.; et al. Phenotyping heart failure patients for iron deficiency and use of intravenous iron therapy: Data from the Swedish Heart Failure Registry. Eur. J. Heart Fail. 2021, 23, 1844–1854. [Google Scholar] [CrossRef] [PubMed]
- Miñana, G.; Bayés-Genís, A.; Núñez, J. Iron deficiency testing and treatment in heart failure: The eyes are useless when the mind is blind. Eur. J. Heart Fail. 2021, 23, 1855–1857. [Google Scholar] [CrossRef] [PubMed]
- Miñana, G.; Lorenzo, M.; Llàcer, P.; Núñez, E.; Palau, P.; Núñez, J. Iron deficiency testing in acute heart failure. Much to do. REC CardioClinics 2021, in press. [Google Scholar] [CrossRef]
- McMurray, J.J.; Adamopoulos, S.; Anker, S.D.; Auricchio, A.; Böhm, M.; Dickstein, K.; Falk, V.; Filippatos, G.; Fonseca, C.; Gomez-Sanchez, M.A.; et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2012, 33, 1787–1847. [Google Scholar] [CrossRef] [PubMed]
- Crowther, M.J. Merlin—A unified modeling framework for data analysis and methods development in Stata. Stata J. 2020, 20, 763–784. [Google Scholar] [CrossRef]
- Pezel, T.; Audureau, E.; Mansourati, J.; Baudry, G.; Ben Driss, A.; Durup, F.; Fertin, M.; Godreuil, C.; Jeanneteau, J.; Kloeckner, M.; et al. Diagnosis and treatment of iron deficiency in heart Failure: OFICSel study by the French Heart Failure Working Group. ESC Heart Fail. 2021, 8, 1509–1521. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; van Veldhuisen, D.J.; Comin-Colet, J.; Ertl, G.; Komajda, M.; Mareev, V.; McDonagh, T.; Parkhomenko, A.; Tavazzi, L.; Levesque, V.; et al. Beneficial effects of long-term intravenous iron therapy with ferric carboxymaltose in patients with symptomatic heart failure and iron deficiency. Eur. Heart J. 2015, 36, 657–668. [Google Scholar] [CrossRef] [PubMed]
- Graham, F.J.; Pellicori, P.; Ford, I.; Petrie, M.C.; Kalra, P.R.; Cleland, J.G.F. Intravenous iron for heart failure with evidence of iron deficiency: A meta-analysis of randomised trials. Clin. Res. Cardiol. 2021, 110, 1299–1307. [Google Scholar] [CrossRef] [PubMed]
- Núñez, J.; Comín-Colet, J.; Miñana, G.; Núñez, E.; Santas, E.; Mollar, A.; Valero, E.; García-Blas, S.; Cardells, I.; Bodí, V.; et al. Iron deficiency and risk of early readmission following a hospitalization for acute heart failure. Eur. J. Heart Fail. 2016, 18, 798–802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- López-Vilella, R.; Lozano-Edo, S.; Arenas Martín, P.; Jover-Pastor, P.; Ezzitouny, M.; Sorolla Romero, J.; Calvo Asensio, M.; Martínez-Solé, J.; Guerrero Cervera, B.; Sánchez Martínez, J.C.; et al. Impact of intravenous ferric carboxymaltose on heart failure with preserved and reduced ejection fraction. ESC Heart Fail. 2021, 9, 133–145. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 711) | |
|---|---|
| Demographics and medical history | |
| Age, years | 72 ± 12 |
| Male, n (%) | 445 (62.6) |
| Hypertension, n (%) | 554 (77.9) |
| Dyslipidaemia, n (%) | 444 (62.4) |
| Diabetes, n (%) | 266 (37.4) |
| Insulin-dependent diabetes, n (%) | 86 (12.1) |
| Active smoker, n (%) | 98 (13.7) |
| Previous smoker, n (%) | 207 (29.1) |
| Alcohol abuse, n (%) | 27 (3.8) |
| Ischaemic heart disease, n (%) | 318 (44.7) |
| Valve heart disease, n (%) | 199 (28.0) |
| Pacemaker, n (%) | 36 (5.0) |
| Implantable cardioverter-defibrillator, n (%) | 41 (5.8) |
| Prior stroke, n (%) | 56 (7.9) |
| Chronic obstructive pulmonary disease, n (%) | 115 (16.2) |
| History of chronic renal disease, n (%) | 149 (20.9) |
| History of peripheral artery disease, n (%) | 52 (7.3) |
| Prior heart failure hospitalization in the last year, n (%) | 315 (44.3) |
| Physical examination | |
| Heart rate, bpm | 77 ± 17 |
| Systolic blood pressure, mmHg | 129 ± 23 |
| Diastolic blood pressure, mmHg | 68 ± 13 |
| Pleural effusion, n (%) | 100 (14.0) |
| Peripheral oedema, n (%) | 210 (29.5) |
| NYHA class, n (%) | |
| I | 55 (7.8) |
| II | 615 (86.5) |
| III | 40 (5.6) |
| IV | 1 (0.1) |
| ECG and echocardiography | |
| Left bundle branch block, n (%) | 190 (26.7) |
| Atrial fibrillation, n (%) | 297 (41.8) |
| Left ventricle ejection fraction, % | 47 ± 16 |
| LVEF ≤40%, n (%) | 268 (37.7) |
| LVEF 41–49%, n (%) | 104 (14.6) |
| LVEF ≥50%, n (%) | 339 (47.7) |
| Mitral insufficiency, n (%) | 90 (12.6) |
| III/IV Tricuspid insufficiency, n (%) | 58 (8.2) |
| TAPSE, mm | 18.5 ± 4.2 |
| Laboratory data | |
| Haemoglobin, g/dL 1 | 12.9 ± 2.0 |
| Haematocrit, % 1 | 40.1 (6.8) |
| Anemia (WHO criteria), n (%) 1 | 272 (41.2) |
| Ferritin, μg/L 2 | 213.8 ± 249.7 |
| TSAT, % 3 | 23.1 ± 18.8 |
| Iron deficiency (combined criteria), n (%) 4 | 223 (57.0) |
| Absolute iron deficiency, n (%) 4 | 155 (39.7) |
| Functional iron deficiency, n (%) 4 | 68 (17.4) |
| Urea, mg/dL 1 | 71.3 ± 76.8 |
| Creatinine, mg/dL 1 | 1.31 ± 0.68 |
| eGFR (MDRD formula), mL/min/1.73 m2 4 | 63.7 ± 27.6 |
| eGFR <60 mL/min/1.73 m2, n (%) 1 | 323 (48.9) |
| Sodium, mEq/L 1 | 140 ± 3 |
| Potassium, mEq/L 1 | 4.4 ± 0.6 |
| NT-proBNP, pg/mL, median (IQR) 5,6 | 1848 (646–4637) |
| Carbohydrate antigen 125, U/mL, median (IQR) 5,6 | 23 (12–75) |
| Treatment | |
| Loop diuretics, n (%) | 587 (82.6) |
| ACEI or ARB, n (%) | 463 (51.3) |
| ARNI, n (%) | 112 (15.8) |
| Betablockers, n (%) | 552 (77.6) |
| MRA, n (%) | 365 (51.3) |
| SGLT2i, n (%) | 85 (11.9) |
| Oral anticoagulants, n (%) | 274 (38.5) |
| Antiplatelet, n (%) | 206 (29.0) |
| Statins, n (%) | 429 (60.3) |
| ICD, n (%) | 41 (5.8) |
| CRT, n (%) | 35 (4.9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miñana, G.; Lorenzo, M.; Ramirez de Arellano, A.; Wächter, S.; de la Espriella, R.; Sastre, C.; Mollar, A.; Núñez, E.; Bodí, V.; Sanchis, J.; et al. Incidence, Treatment and Clinical Impact of Iron Deficiency in Chronic Heart Failure: A Longitudinal Analysis. J. Clin. Med. 2022, 11, 2559. https://doi.org/10.3390/jcm11092559
Miñana G, Lorenzo M, Ramirez de Arellano A, Wächter S, de la Espriella R, Sastre C, Mollar A, Núñez E, Bodí V, Sanchis J, et al. Incidence, Treatment and Clinical Impact of Iron Deficiency in Chronic Heart Failure: A Longitudinal Analysis. Journal of Clinical Medicine. 2022; 11(9):2559. https://doi.org/10.3390/jcm11092559
Chicago/Turabian StyleMiñana, Gema, Miguel Lorenzo, Antonio Ramirez de Arellano, Sandra Wächter, Rafael de la Espriella, Clara Sastre, Anna Mollar, Eduardo Núñez, Vicent Bodí, Juan Sanchis, and et al. 2022. "Incidence, Treatment and Clinical Impact of Iron Deficiency in Chronic Heart Failure: A Longitudinal Analysis" Journal of Clinical Medicine 11, no. 9: 2559. https://doi.org/10.3390/jcm11092559
APA StyleMiñana, G., Lorenzo, M., Ramirez de Arellano, A., Wächter, S., de la Espriella, R., Sastre, C., Mollar, A., Núñez, E., Bodí, V., Sanchis, J., Bayés-Genís, A., & Núñez, J. (2022). Incidence, Treatment and Clinical Impact of Iron Deficiency in Chronic Heart Failure: A Longitudinal Analysis. Journal of Clinical Medicine, 11(9), 2559. https://doi.org/10.3390/jcm11092559