
Assessment of Risk Factors for Acute Kidney Injury with Machine Learning Tools in Children Undergoing Hematopoietic Stem Cell Transplantation

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Characteristics
2.2. Serum Creatinine and eGFR Values
2.3. AKI Diagnosis
2.4. Classical Statistical Analysis
2.5. Machine Learning Methods
2.5.1. Machine Learning Is a Domain of Artificial Intelligence Aimed at Imitating the Decision-Making Process Carried out by Humans
2.5.2. Model Performance Measures Are Classically Described as the Ratio of True Matches to Both Domains: Positives and Negatives
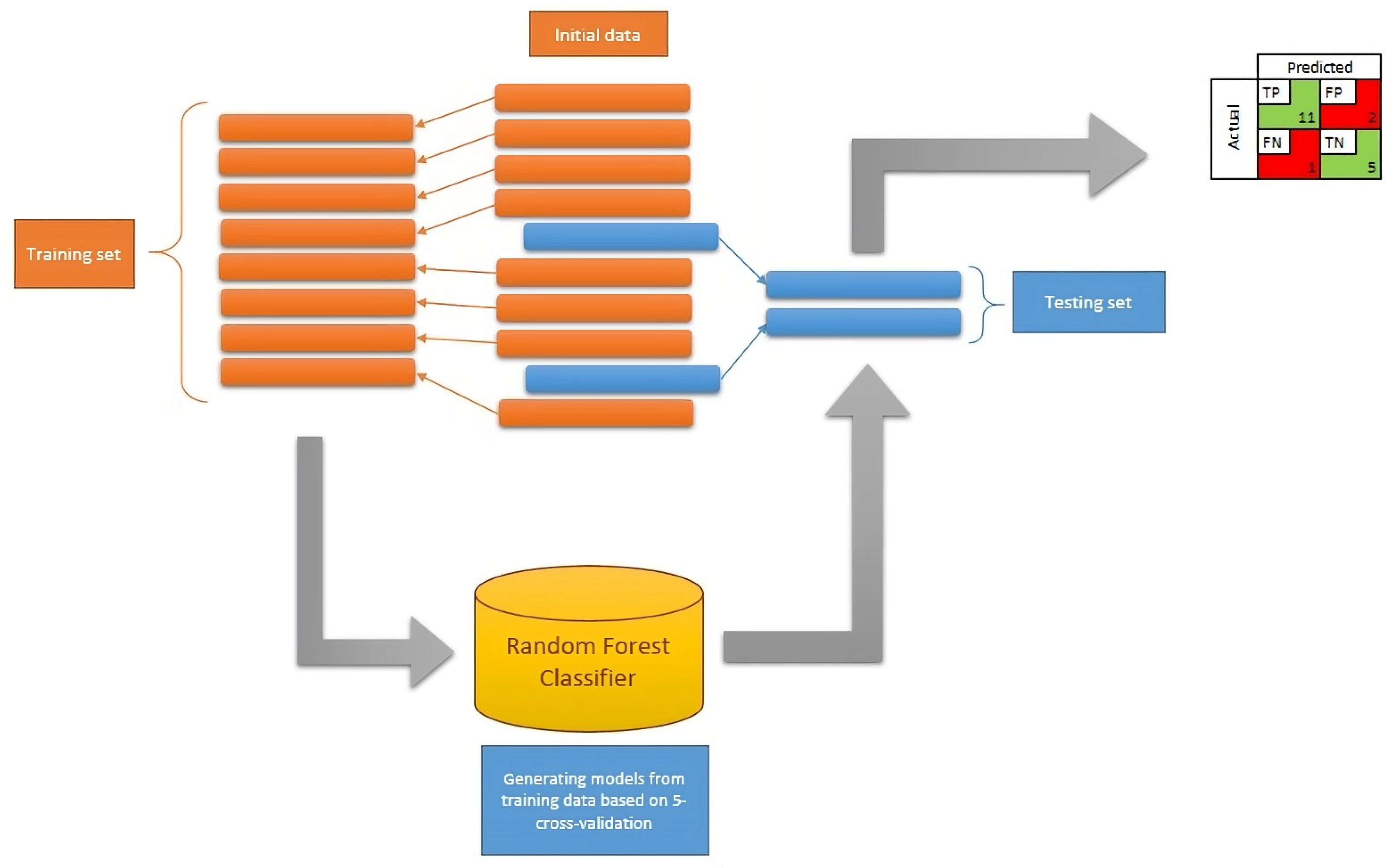
2.5.3. Selection of Input Data and Development of the Model
2.5.4. Feature Importance
3. Results
3.1. Clinical Data Concerning the HSCT Patients
3.2. Serum Creatinine and eGFR Values
3.3. The Incidence of AKI
3.4. Preparing the Dataset to Build the Model
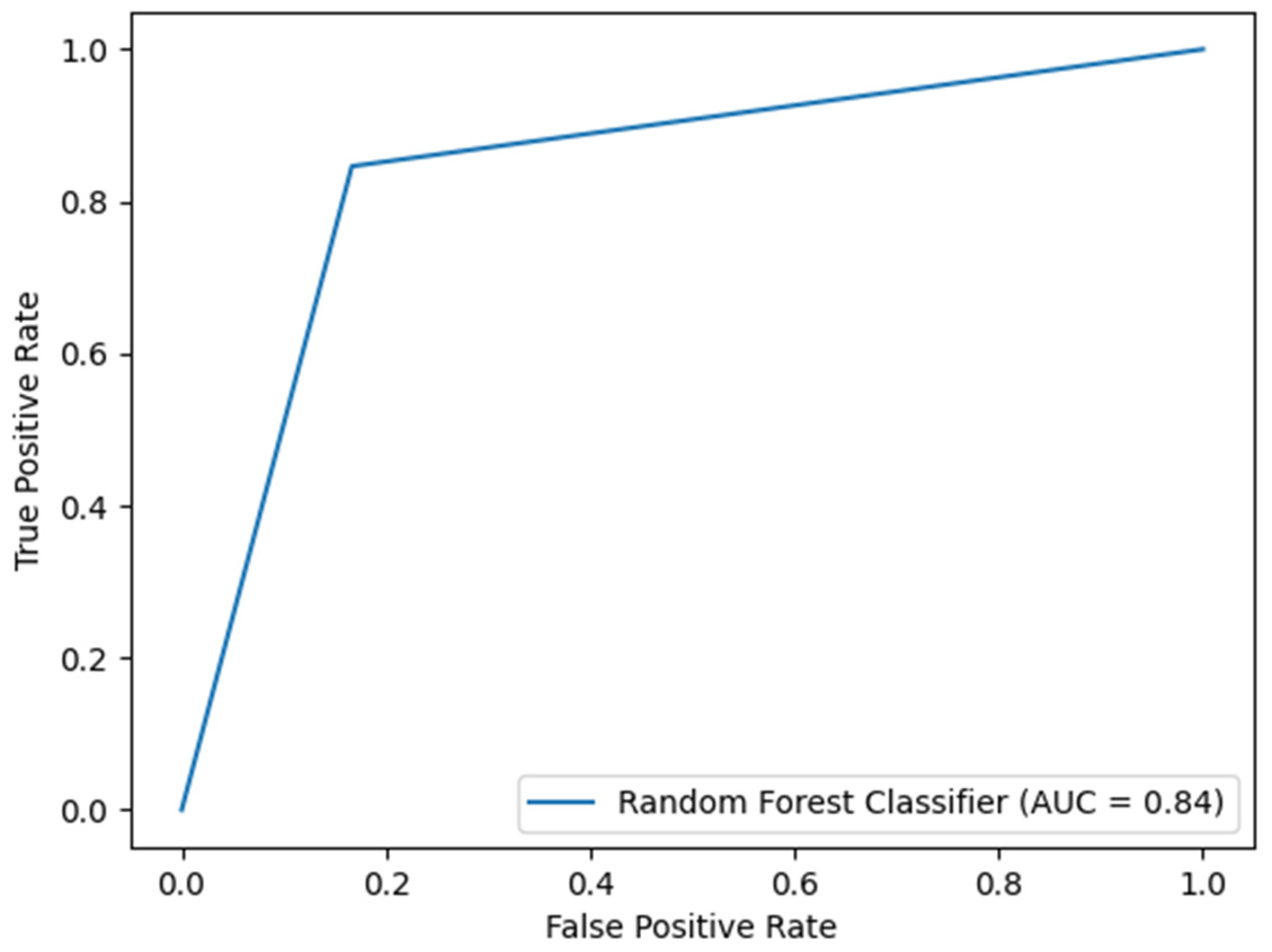
3.5. Model Predicting AKI Incidence during the Observation Period
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Raina, R.; Abu-Arja, R.; Sethi, S.K.; Dua, R.; Chakraborty, R.; Dibb, J.T.; Basu, R.K.; Bissler, J.; Felix, M.B.; Brophy, P.; et al. Acute kidney injury in pediatric hematopoietic stem cell transplantation: Critical appraisal and consensus. Pediatr. Nephrol. 2023, 37, 1179–1203. [Google Scholar] [CrossRef] [PubMed]
- Koh, K.N.; Sunkara, A.; Kang, G.; Sooter, A.; Mulrooney, D.A.; Triplett, B.; Onder, A.M.; Bissler, J.; Cunningham, L.C. Acute Kidney Injury in Pediatric Patients Receiving Allogeneic Hematopoietic Cell Transplantation: Incidence, Risk Factors, and Outcomes. Biol. Blood Marrow Transplant. 2018, 24, 758–764. [Google Scholar] [CrossRef] [PubMed]
- Kizilbash, S.J.; Kashtan, C.E.; Chavers, B.M.; Cao, Q.; Smith, A.R. Acute kidney injury and the risk of mortality in children undergoing hematopoietic stem cell transplantation. Biol. Blood Marrow Transplant. 2016, 22, 1264–1270. [Google Scholar] [CrossRef] [PubMed]
- Didsbury, M.S.; Mackie, F.E.; Kennedy, S.E. A systematic review of acute kidney injury in pediatric allogeneic hematopoietic stem cell recipients. Pediatr. Transplant. 2015, 19, 460–470. [Google Scholar] [CrossRef] [PubMed]
- Huang, B.; Shan, J.; Yi, L.; Xin, Y.; Zhong, Z.; Xu, H. Risk factors for acute kidney injury in pediatric patients after hematopoietic stem cell transplantation: A systematic review and meta-analysis. Pediatr. Nephrol. 2024, 39, 397–408. [Google Scholar] [CrossRef] [PubMed]
- Hirano, D.; Kakegawa, D.; Miwa, S.; Umeda, C.; Takemasa, Y.; Tokunaga, A.; Kawakami, Y.; Ito, A. Independent risk factors and long-term outcomes for acute kidney injury in pediatric patients undergoing hematopoietic stem cell transplantation: A retrospective cohort study. BMC Nephrol. 2020, 21, 373. [Google Scholar] [CrossRef] [PubMed]
- Sahin, U.; Toprak, S.K.; Atilla, P.A.; Atilla, E.; Demirer, T. An overview of infectious complications after allogeneic hematopoietic stem cell transplantation. J. Infect. Chemother. 2016, 22, 505–514. [Google Scholar] [CrossRef]
- Hierlmeier, S.; Eyrich, M.; Wölfl, M.; Schlegel, P.-G.; Wiegering, V. Early and late complications following hematopoietic stem cell transplantation in pediatric patients—A retrospective analysis over 11 years. PLoS ONE 2018, 13, e0204914. [Google Scholar] [CrossRef]
- Gurbanov, A.; Gülhan, B.; Kuşkonmaz, B.; Okur, F.V.; Ozaltin, F.; Düzova, A.; Çetinkaya, D.U.; Topaloglu, R. Predictors of kidney complications and analysis of hypertension in children with allogeneic hematopoietic stem cell transplantation. Pediatr. Nephrol. 2023, 38, 461–469. [Google Scholar] [CrossRef]
- Avci, B.; Bilir, Ö.A.; Özlü, S.G.; Kanbur, Ş.M.; Gökçebay, D.G.; Bozkaya, I.O.; Bayrakçi, U.S.; Özbek, N.Y. Acute kidney injury and risk factors in pediatric patients undergoing hematopoietic stem cell transplantation. Pediatr. Nephrol. 2024. [Google Scholar] [CrossRef]
- Daraskevicius, J.; Azukaitis, K.; Dziugeviciute-Tupko, J.; Peciulyte, M.; Planciunaite, R.; Vaitkeviciene, G.; Rascon, J.; Jankauskiene, J. Phenotypes and baseline risk factors of acute kidney injury in children after allogeneic hematopoietic stem cell transplantation. Front. Pediatr. 2020, 8, 499. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Ji, Y.; Huang, M.; Feng, Z. Machine learning for acute kidney injury: Changing the traditional disease prediction model. Front. Med. 2023, 10, 1050255. [Google Scholar] [CrossRef] [PubMed]
- Thongprayoon, C.; Pattharanitima, P.; Kattah, A.G.; Mao, M.A.; Keddis, M.T.; Dillon, J.J.; Kaewput, W.; Tangpanithandee, S.; Krisanapan, P.; Qureshi, F.; et al. Explainable preoperative automated machine learning prediction model for cardiac surgery-associated acute kidney injury. J. Clin. Med. 2022, 11, 6264. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Lu, Y.; Li, S.; Guo, F.; Xue, H.; Jiang, L.; Wang, Z.; Zhang, C.; Xie, W.; Zhu, F. Predicting renal function recovery and short-term reversibility among acute kidney injury patients in the ICU: Comparison of machine learning methods and conventional regression. Ren. Fail. 2022, 44, 1327–1338. [Google Scholar] [CrossRef] [PubMed]
- Raina, R.; Nada, A.; Shah, R.; Aly, H.; Kadatane, S.; Abitbol, C.; Aggarwal, M.; Koyner, J.; Neyra, J.; Sethi, S.K. Artificial intelligence in early detection and prediction of pediatric/neonatal acute kidney injury: Current status and future directions. Pediatr. Nephrol. 2023. [Google Scholar] [CrossRef] [PubMed]
- Musiał, K.; Stojanowski, J.; Miśkiewicz-Bujna, J.; Kałwak, K.; Ussowicz, M. KIM-1, IL-18, and NGAL, in the machine learning prediction of kidney injury among children undergoing hematopoietic stem cell transplantation—A pilot study. Int. J. Mol. Sci. 2023, 24, 15791. [Google Scholar] [CrossRef]
- Schwartz, G.J.; Muñoz, A.; Schneider, M.F.; Mak, R.H.; Kaskel, F.; Warady, B.A.; Furth, S.L. New equations to estimate GFR in children with CKD. J. Am. Soc. Nephrol. 2009, 20, 629–637. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, S.M.; Byrnes, J.J.; Kothari, M.; Longhurst, C.A.; Dutta, S.; Garcia, P.; Goldstein, S.L. AKI in hospitalized children: Comparing the pRIFLE, AKIN, and KDIGO definitions. Clin. J. Am. Soc. Nephrol. 2015, 10, 554–561. [Google Scholar] [CrossRef] [PubMed]
- Iduoriyekemwen, N.J.; Ibadin, M.O.; Aikhionbare, H.A.; Idogun, S.E.; Abiodun, M.T. Glomerular hyperfiltration in excess weight adolescents. Niger. J. Clin. Pract. 2019, 22, 842–848. [Google Scholar] [CrossRef]
- Cachat, F.; Combescure, C.; Cauderay, M.; Girardin, E.; Chehade, H. A systematic review of glomerular hyperfiltration assessment and definition in the medical literature. Clin. J. Am. Soc. Nephrol. 2015, 10, 382–389. [Google Scholar] [CrossRef]
- Chicco, D.; Jurman, G. The advantages of the Matthews correlation coefficient (MCC) over F1 score and accuracy in binary classification evaluation. BMC Genom. 2020, 21, 6. [Google Scholar] [CrossRef] [PubMed]
- Kong, Y.; Yu, T. A Deep Neural Network Model using Random Forest to Extract Feature Representation for Gene Expression Data Classification. Sci. Rep. 2018, 8, 16477. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.C.; Dewi, C.; Huang, S.W.; Caraka, R.E. Selecting critical features for data classification based on machine learning methods. J. Big Data 2020, 7, 52. [Google Scholar] [CrossRef]
- Jaiswal, J.K.; Samikannu, R. Application of random forest algorithm on feature subset selection and classification and regression. In Proceedings of the 2017 World Congress on Computing and Communication Technologies (WCCCT), Tiruchirappalli, India, 2–4 February 2017; IEEE: New York, NY, USA, 2017; pp. 65–68. [Google Scholar]
- Gholamy, A.; Kreinovich, V.; Kosheleva, O. Why 70/30 or 80/20 Relation Between Training and Testing Sets: A Pedagogical Explanation. Departmental. Technical. Reports. (CS) 2018, 1209. Available online: https://scholarworks.utep.edu/cs_techrep/1209 (accessed on 9 April 2024).
- Menze, B.H.; Kelm, B.M.; Masuch, R.; Himmelreich, U.; Bachert, P.; Petrich, W.; Hamprecht, F.A. A comparison of random forest and its Gini importance with standard chemometric methods for the feature selection and classification of spectral data. BMC Bioinform. 2009, 10, 213. [Google Scholar] [CrossRef]
- Renaghan, A.D.M.; Jaimes, E.A.; Małyszko, J.; Perazella, M.A.; Sprangers, B.; Rosner, M.H. Acute kidney injury and CKD associated with hematopoietic stem cell transplantation. CJASN 2020, 15, 289–297. [Google Scholar] [CrossRef]
- Lopes, J.A.; Jorge, A.; Neves, M. Acute kidney injury in HCT: An update. Bone Marrow Transplant. 2016, 51, 755–762. [Google Scholar] [CrossRef]
- Krishnappa, V.; Gupta, M.; Manu, G.; Kwatra, S.; Owusu, O.T.; Raina, R. Acute kidney injury in hematopoietic stem cell transplantation: A review. Int. J. Nephrol. 2016, 2016, 5163789. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.H.; Chen, J.-J.; Cheng, C.-T.; Chang, C.-H. Does artificial intelligence make clinical decision better? A review of artificial intelligence and machine learning in acute kidney injury prediction. Healthcare 2021, 9, 1662. [Google Scholar] [CrossRef] [PubMed]
- Kellum, J.A.; Bihorac, A. Artificial intelligence to predict AKI: Is it a breakthrough? Nat. Rev. Nephrol. 2019, 15, 663–664. [Google Scholar] [CrossRef]
- Filler, G.; Lee, M. Measurement of GFR in special populations. Pediatr. Nephrol. 2018, 33, 2037–2046. [Google Scholar] [CrossRef]
- Kwatra, N.S.; Meany, H.J.; Ghelani, S.J.; Zahavi, D.; Pandya, N.; Majd, M. Glomerular hyperfiltration in children with cancer: Prevalence and a hypothesis. Pediatr. Radiol. 2016, 47, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Cortinovis, M.; Perico, R.; Ruggenenti, P.; Remuzzi, A.; Remuzzi, G. Glomerular hyperfiltration. Nat. Rev. Nephrol. 2022, 18, 435–451. [Google Scholar] [CrossRef] [PubMed]
- Fuhrman, D.Y. The role of renal functional reserve in predicting acute kidney injury. Crit. Care Clin. 2021, 37, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Musiał, K. Current concepts of pediatric acute kidney injury—Are we ready to translate them into everyday practice? J. Clin. Med. 2021, 10, 3113. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Mucino, M.J.; Ronco, C. Renal functional reserve and renal recovery after acute kidney injury. Nephron Clin. Pract. 2014, 127, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Mueller, T.F.; Luyckx, V.A. Potential utility of renal functional reserve testing in clinical nephrology. Curr. Opin. Nephrol. Hypertens. 2024, 33, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Mancianti, N.; Guarnieri, A.; Lenoci, M.; Toraldo, F.; Salvo, D.P.; Belluardo, M.; Iadanza, E.; Ferretti, F.; Marotta, G.; Garosi, G. Rationale for the evaluation of renal functional reserve in allogeneic stem cell transplantation candidates: A pilot study. Clin. Kidney J. 2023, 16, 996–1004. [Google Scholar] [CrossRef] [PubMed]
- Grams, M.E.; Sang, Y.; Ballew, S.H.; Gansevoort, R.T.; Kimm, H.; Kovesdy, C.P.; Naimark, D.; Oien, C.; Smith, D.H.; Coresh, J.; et al. A meta-analysis of the association of estimated GFR, albuminuria, age, race, and sex with acute kidney injury. Am. J. Kidney Dis. 2015, 66, 591–601. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.J.; Go, A.S.; Parikh, R.; Leong, T.K.; Tan, T.C.; Walia, S.; Hsu, R.K.; Liu, K.D.; Hsu, C. Pre-admission proteinuria impacts risk of non-recovery after dialysis-requiring acute kidney injury. Kidney Int. 2018, 93, 968–976. [Google Scholar] [CrossRef]
- Flammia, R.S.; Tufano, A.; Proietti, F.; Gerolimetto, C.; De Nunzio, C.; Franco, G.; Leonardo, C. Renal surgery for kidney cancer: Is preoperative proteinuria a predictor of functional and survival outcomes after surgery? A systematic review of the literature. Minerva Urol. Nephrol. 2022, 74, 255–264. [Google Scholar] [CrossRef]
- Ando, M. An overview of kidney disease following hematopoietic cell transplantation. Intern. Med. 2018, 57, 1503–1508. [Google Scholar] [CrossRef] [PubMed]
- James, V.; Angelo, J.; Elbahlawan, L. Kidney injury in children after hematopoietic stem cell transplant. Curr. Oncol. 2023, 30, 3329–3343. [Google Scholar] [CrossRef] [PubMed]
- Jaguś, D.; Lis, K.; Niemczyk, L.; Basak, G.W. Kidney dysfunction after hematopoietic cell transplantation—Etiology, management, and perspectives. Hematol. Oncol. Stem Cell Ther. 2018, 11, 195–205. [Google Scholar] [CrossRef] [PubMed]
- Miyata, M.; Ichikawa, K.; Matsuki, E.; Watanabe, M.; Peltier, D.; Toubai, T. Recent advances of acute kidney injury in hematopoietic cell transplantation. Front. Immunol. 2022, 12, 779881. [Google Scholar] [CrossRef]
- Mima, A.; Tansho, K.; Nagahara, D.; Tsubaki, K. Incidence of acute kidney disease after receiving hematopoietic stem cell transplantation: A single-center retrospective study. PeerJ 2019, 7, e6467. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Number of Children | Percentage |
|---|---|---|
| Boys/girls | 78/57 | 58/42 |
| 1 eGFR < 90 mL/min/1.73 m2 | 11 | 8 |
| eGFR > 140 mL/min/1.73 m2 | 55 | 40 |
| Unrelated donors | 98 | 72 |
| Matching 10/10 | 86 | 63 |
| Peripheral blood stem cells | 114 | 84 |
| Conditioning therapy | ||
| Fludarabine | 119 | 88 |
| Thiotepa | 86 | 63 |
| Treosulfan | 69 | 51 |
| Cyclophosphamide | 31 | 22 |
| 2 GvHD prophylaxis | ||
| Cyclosporin A | 132 | 98 |
| Anti-thymoglobulin | 108 | 80 |
| Methotrexate | 105 | 77 |
| Mycophenolate mofetil | 20 | 15 |
| Infectious complications | ||
| BK virus | 86 | 63 |
| Cytomegalovirus | 47 | 35 |
| Adenovirus | 38 | 28 |
| Epstein–Barr virus | 35 | 26 |
| Bacterial | 23 | 17 |
| Fungal | 2 | 1 |
| Acute GvHD | 77 | 57 |
| Chronic GvHD | 21 | 15 |
| Time Point | Serum Creatinine [mg/dL] Mean Value ± SD | eGFR [ml/min/1.73 m2] Mean Value ± SD | Risk Incidence [Number of Patients/%] | Injury Incidence [Number of Patients/%] |
|---|---|---|---|---|
| Before HSCT | 0.58 ± 0.19 | 141 ± 44 | 0 | 0 |
| 24 h after HSCT | 0.49 ± 0.15 a | 164 ± 51 b | 1/0.7 | 2/1.4 |
| 1 week after HSCT | 0.49 ± 0.17 a | 166 ± 55 b | 1/0.7 | 0 |
| 2 weeks after HSCT | 0.53 ± 0.18 a | 156 ± 55 b | 11/8 | 1/0.7 |
| 3 weeks after HSCT | 0.58 ± 0.17 | 141 ± 50 | 16/12 | 1/0.7 |
| 4 weeks after HSCT | 0.61 ± 0.18 a | 133 ± 43 b | 25/18 | 0 |
| 8 weeks after HSCT | 0.69 ± 0.30 a | 123 ± 42 b | 39/29 | 3/2 |
| 3 months after HSCT | 0.69 ± 0.26 a | 122 ± 41 b | 29/21 | 7/5 |
| 6 months after HSCT | 0.64 ± 0.18 a | 127 ± 38 b | 23/17 | 0 |
| Predicted | ||||
|---|---|---|---|---|
| Actual | TP | FP | ||
| 11 | 2 | |||
| FN | TN | |||
| 1 | 5 | |||
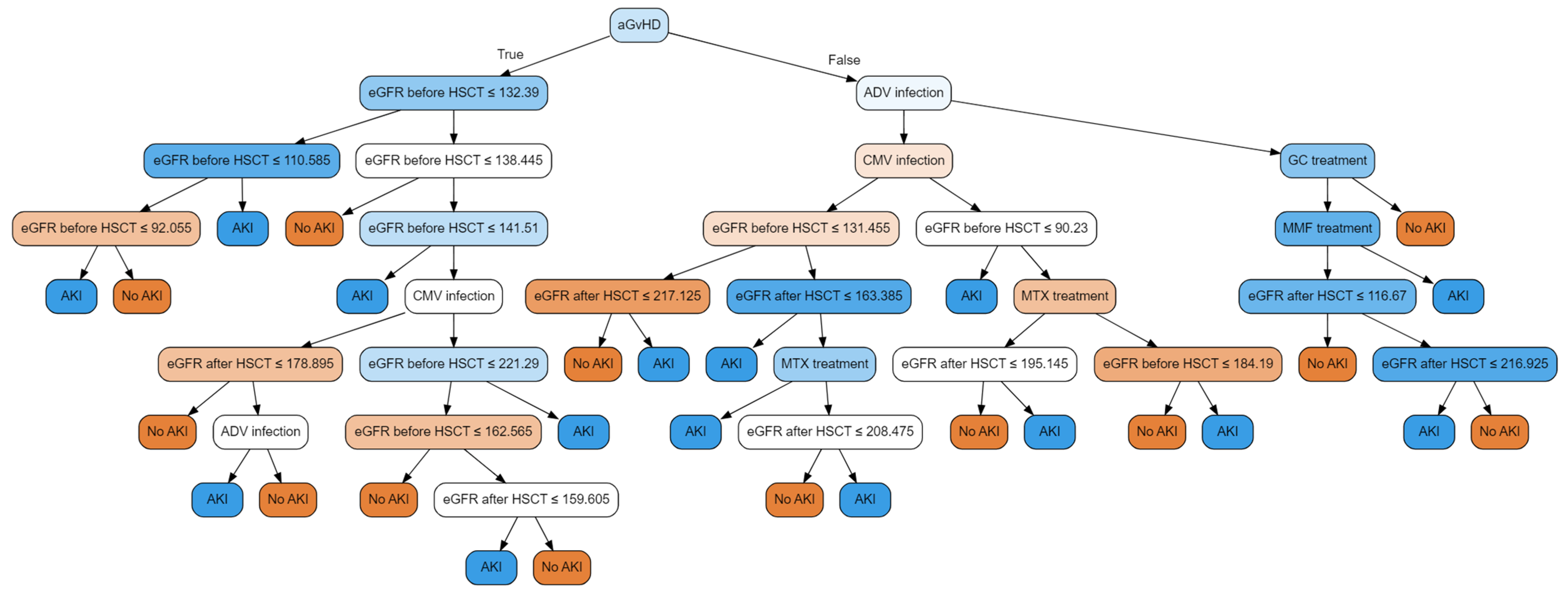
| Feature | Feature Importance |
|---|---|
| eGFR after HSCT b | 37.04% |
| eGFR before HSCT b | 35.78% |
| Methotrexate a | 8.54% |
| Cytomegalovirus a | 5.99% |
| Adenovirus a | 4.99% |
| Acute GvHD a | 4.04% |
| Mycophenolate mofetil a | 2.63% |
| Glucocorticoids a | 0.98% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Musiał, K.; Stojanowski, J.; Augustynowicz, M.; Miśkiewicz-Migoń, I.; Kałwak, K.; Ussowicz, M. Assessment of Risk Factors for Acute Kidney Injury with Machine Learning Tools in Children Undergoing Hematopoietic Stem Cell Transplantation. J. Clin. Med. 2024, 13, 2266. https://doi.org/10.3390/jcm13082266
Musiał K, Stojanowski J, Augustynowicz M, Miśkiewicz-Migoń I, Kałwak K, Ussowicz M. Assessment of Risk Factors for Acute Kidney Injury with Machine Learning Tools in Children Undergoing Hematopoietic Stem Cell Transplantation. Journal of Clinical Medicine. 2024; 13(8):2266. https://doi.org/10.3390/jcm13082266
Chicago/Turabian StyleMusiał, Kinga, Jakub Stojanowski, Monika Augustynowicz, Izabella Miśkiewicz-Migoń, Krzysztof Kałwak, and Marek Ussowicz. 2024. "Assessment of Risk Factors for Acute Kidney Injury with Machine Learning Tools in Children Undergoing Hematopoietic Stem Cell Transplantation" Journal of Clinical Medicine 13, no. 8: 2266. https://doi.org/10.3390/jcm13082266
APA StyleMusiał, K., Stojanowski, J., Augustynowicz, M., Miśkiewicz-Migoń, I., Kałwak, K., & Ussowicz, M. (2024). Assessment of Risk Factors for Acute Kidney Injury with Machine Learning Tools in Children Undergoing Hematopoietic Stem Cell Transplantation. Journal of Clinical Medicine, 13(8), 2266. https://doi.org/10.3390/jcm13082266